Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
VectorLift: Anatomically Guided Thread-Lifting Technique With Reduced Pain and Downtime — Results from a Real-World Non-Randomized Comparative Study
Authors Leguina-Ruzzi A ![]() , Rawshani N, Brito S, Bin BH, Abbas Z, Zhao Q
, Rawshani N, Brito S, Bin BH, Abbas Z, Zhao Q ![]()
Received 5 April 2026
Accepted for publication 26 May 2026
Published 10 June 2026 Volume 2026:19 613245
DOI https://doi.org/10.2147/CCID.S613245
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Alberto Leguina-Ruzzi,1,2,* Nina Rawshani,3 Sofia Brito,4,5 Bum-Ho Bin,4,5 Zafar Abbas,6,7 Qiaofeng Zhao8,*
1Faculty of Medicine, Universidad Andrés Bello, Santiago, Chile; 2TotalSkin Studio Clinic, Santiago, Chile; 3Rawsh Clinic, Göteborg, Sweden; 4Department of Biological Sciences, Ajou University, Suwon, Republic of Korea; 5The Anti Aging Lab, Co. Ltd, Suwon, Republic of Korea; 6Royal Academy of Facial Aesthetic, Karachi, Pakistan; 7International Dental College, Dow University of Health Science, Karachi, Pakistan; 8Juntendo Itch Research Center (JIRC), Institute for Environmental and Gender-Specific Medicine, Juntendo University Graduate School of Medicine, Chiba, Japan
*These authors contributed equally to this work
Correspondence: Alberto Leguina-Ruzzi, Universidad Andrés Bello, Faculty of Medicine, Sazié 2320, piso 3, Santiago, Región Metropolitana, 7591538, Chile, Email [email protected] Qiaofeng Zhao, Juntendo Itch Research Center (JIRC), institute for Environmental and Gender-Specific Medicine, Juntendo University Graduate School of Medicine, 2-1-1 Tomioka Urayasu-shi, Chiba, Japan, Email [email protected]
Background: Thread lifting has emerged as a minimally invasive alternative to surgical facial rejuvenation, providing mechanical tissue repositioning with shorter recovery times. Advances in biomaterials and thread design have improved safety and lifting capacity; however, variability in clinical outcomes persists due to differences in vector design, thread type, tissue manipulation, and anesthesia techniques. These factors may influence complication rates, procedural tolerance, and postoperative downtime, contributing to ongoing concerns regarding the predictability and reproducibility of thread-lifting procedures.
Objective: To describe the development of a vector-optimized thread-lifting technique (VectorLift) and to compare its clinical performance in an exploratory, real-world, non-randomized comparative study with two commonly used thread-lifting approaches employing different biomaterials and insertion methods.
Methods: The VectorLift protocol was developed using anatomically guided vector placement, ligament-oriented reinforcement, and optimized local anesthetic infiltration. Over a three-year period, 44 female patients (mean age 47 years) underwent facial thread-lifting procedures. Eighteen patients were treated using the proposed technique with cannulated polydioxanone (PDO) threads, while the remaining patients were treated with either double-needle poly-L-lactic acid (PLA) plus poly(L-lactide-co-glycolide) (PLGA) cone threads or cannulated PLA/polycaprolactone (PCL) threads. Clinical outcomes included recovery time (days of downtime), intraoperative pain levels, patient satisfaction measured using the FACE-Q scale before treatment and two weeks post-procedure, and complication rates including dimpling, bruising, edema, and transient asymmetry. Standardized clinical photographs were obtained before and immediately after treatment.
Results: VectorLift was associated with lower reported intraoperative pain, shorter recovery time and lower rates of early postoperative complications compared with the other techniques, while patient satisfaction scores were comparable among groups. Immediate photographic assessment confirmed visible aesthetic improvement without overcorrection.
Conclusion: VectorLift is an anatomically guided thread-lifting technique that, in this real-world non-randomized comparative study, was associated with improved procedural tolerance and shorter postoperative downtime while maintaining high patient satisfaction and effective aesthetic outcomes. Further controlled studies with larger patient populations and longer follow-up periods are warranted to confirm these findings.
Keywords: facial rejuvenation, polydioxanone threads, minimally invasive aesthetic procedures, vector-based lifting technique
Introduction
Thread lifting has emerged over the past two decades as a minimally invasive alternative to surgical facial rejuvenation.1 Initially introduced using nonabsorbable sutures for soft-tissue suspension, early thread-lifting techniques generated considerable interest but were also associated with high complication and revision rates, leading to skepticism regarding their clinical utility.2 Subsequent technological advances led to the development of absorbable barbed sutures, which improved safety profiles and procedural predictability. The introduction of biodegradable materials such as polydioxanone (PDO), poly-L-lactic acid (PLLA or PLA), and polycaprolactone (PCL) marked an evolution of thread lifting by combining mechanical lifting with a biostimulatory effect through collagen induction during the degradation process.3–5
The primary objective of thread lifting is the repositioning of ptotic facial tissues through mechanical suspension and reinforcement of weakened retaining ligaments, which progressively lose structural integrity during the aging process.6 Age-related changes in facial anatomy include ligament laxity, descent of superficial fat compartments, and progressive skin laxity, all of which contribute to the characteristic features of facial aging.7 Thread lifting aims to counteract these changes by providing structural support along vector-oriented trajectories that reposition superficial fat pads and improve skin contour without the morbidity associated with surgical rhytidectomy.8
Currently, several absorbable materials are used in thread-lifting procedures. PDO threads are still employed due to their long history of use in surgical suturing, favorable safety profile, and predictable biodegradation over several months.9 PLA threads plus poly(L-lactide-co-glycolide) (PLGA) provide a longer-lasting collagen-stimulating effect but may involve greater tissue reaction due to their slower degradation kinetics.10 PCL-based threads and hybrid combinations of PLA/PCL have also been introduced to extend durability while maintaining biocompatibility.11 In addition to material composition, thread-lifting techniques vary according to insertion methods, including cannulated approaches that minimize tissue trauma and double-needle systems designed to achieve suspension through bidirectional anchoring mechanisms.12
Despite technological improvements and increasing procedural standardization, the popularity and demand for thread lifting have fluctuated over time. Early enthusiasm for the technique was tempered by reports of complications such as dimpling, bruising, edema, asymmetry, thread extrusion, and patient discomfort.13 Furthermore, concerns regarding the durability of results, postoperative downtime, and procedural tolerability have contributed to ongoing debate regarding the true efficacy of thread lifting compared with other minimally invasive facial rejuvenation modalities.14 In addition, variability in technique, practitioner experience, and product selection has contributed to inconsistent outcomes and a perceived lack of robust clinical evidence supporting some applications of thread lifting.15
Nevertheless, thread lifting remains a valid procedure within aesthetic medicine. Large multicenter analyses have demonstrated that thread-lifting procedures are still incorporated into multimodal facial rejuvenation strategies.16 When performed in properly selected patients with mild to moderate facial laxity, thread lifting can provide improvements in facial contour with minimal invasiveness and high patient satisfaction.17 Appropriate patient selection, realistic expectations, careful product choice, and optimized procedural technique are therefore essential factors in achieving predictable outcomes and minimizing complications.
Based on these considerations, we designed an optimized thread-lifting approach termed VectorLift, which utilizes cannulated PDO threads placed along anatomically guided vectors to reinforce key facial retaining ligaments and reposition superficial fat compartments. In addition to vector optimization, this technique incorporates a targeted extraoral anesthetic infiltration protocol designed to achieve effective neural blockade while minimizing anesthetic volume and reducing postoperative edema. This approach aims to improve procedural tolerability, reduce tissue trauma, and shorten recovery time while maintaining effective lifting outcomes.
To evaluate the clinical performance of this technique, we conducted a comparative analysis of patients treated with the VectorLift method and patients undergoing thread lifting using two others widely used thread systems and insertion techniques, namely cannulated PLA/PCL threads and double-needle PLA cone threads.
Materials and Methods
Study Population and Design
Over a 3 years period period, a total of 44 female patients presenting for aesthetic consultation due to mid- and lower-face ptosis were included in this observational comparative study. The mean age of the study population was 47 ± 6 years.
This study was designed as a single-center prospective real-world non-randomized comparative study conducted in a private practice setting. Patients seeking minimally invasive facial rejuvenation were consecutively evaluated and treated according to routine clinical practice, and outcomes were prospectively collected using standardized clinical and patient-reported assessments. The study design aimed to reflect real-world decision-making and treatment selection while allowing comparative evaluation of different thread-lifting approaches under daily clinical conditions.
The most common aesthetic concerns included mid- and lower-face sagging, increased prominence of nasolabial folds, and the presence of early jowling.
Clinical evaluation demonstrated that all patients presented mild-to-moderate skin laxity without evidence of marked hyperelastosis. Mild cutaneous atrophy was observed; however, patients did not present significant volume loss in the upper (temporal), midface (zygomatic), or lower face (mandibular border) compartments. All patients expressed a personal interest in minimally invasive facial rejuvenation with thread lifting and had no prior history of thread-lifting procedures.
Following clinical assessment, patients were considered appropriate candidates for thread lifting when manual upward vectorial repositioning of the facial skin resulted in visible improvement of facial contour and tissue support. In addition, none of the patients presented significant excess skin in the periauricular region that would have made them better candidates for surgical rhytidectomy.
Three different thread-lifting modalities were proposed and discussed with the patients during the consultation. The characteristics of each technique, including expected benefits, potential complications, recovery time, invasiveness, and estimated durability, were thoroughly explained. Patients independently selected the treatment modality considered most appropriate for their individual expectations and preferences. No allocation or influence toward a specific technique was applied by the treating physicians, even when our retrospective study has non-randomized allocation, we minimize the selection bias by presenting the three techniques and products as clear treatment options.
All procedures were performed by trained physicians with more than three years of experience in thread-lifting techniques and with prior successful clinical experience using the three thread modalities evaluated in this study. The procedures were conducted following the protocols and technical recommendations established by the respective manufacturers and their medical advisory teams.
Prior to the implementation of the VectorLift technique, a pilot application was performed in two patients to evaluate procedural feasibility, safety, and preliminary clinical outcomes. The favorable results observed in these initial cases supported the incorporation of the technique into routine clinical practice and its subsequent offering to patients during consultation. Data obtained from the pilot cases were included in the present study.
Standard post-procedural care instructions were provided to all patients. Clinical follow-up was performed two weeks after the procedure, during which patient satisfaction, recovery parameters, and potential complications were evaluated and documented.
Our study excluded participants who had chronic diseases such as diabetes, obesity, hypertension, autoimmune diseases, coagulopathies, intercurrent inflammatory or infectious disorders. Smokers and users of recreational or non-recreational drugs (mainly statins, antibiotics, isotretinoin and anti-inflammatory drugs) were also eliminated. Patients suffering from other skin disorders such as acne, psoriasis or dermatitis were ruled out as well. Patients who were pregnant, trying to get pregnant or breastfeeding were also excluded. People with known allergies to anesthetics or PDO were removed from the study too.
Each subject signed a comprehensive written informed consent that included permission to obtain and publish their photographs. This work was conducted according to the principles stated in the Declaration of Helsinki.
Threads and Techniques
For the PLA/PCL cannulated thread technique, the product Aptos ® Excellence Visage (Aptos LLC, Tbilisi, Georgia) was used. A total of 10 threads per patient were implanted following the manufacturer’s recommended protocol. These threads are absorbable cannulated threads composed of a PLA/PCL. The threads are supplied preloaded within a blunt-tip cannula, facilitating subcutaneous placement through a single-entry point. The thread structure incorporates bidirectional barbs (cogs) designed to anchor within the subdermal tissue and provide mechanical lifting through tissue engagement and redistribution of tension vectors. The threads typically correspond to USP 2–0 caliber and have an approximate length of 190 mm, allowing placement along extended lifting vectors in the mid- and lower face. The barbed design promotes tissue fixation and repositioning while the PLA/PCL copolymer gradually undergoes hydrolytic degradation over time.
For the PLA cone-based thread technique, the product Silhouette Soft ® (Sinclair Pharma, London, United Kingdom) was used. A total of 4 threads per patient were inserted according to the recommended treatment protocol. Silhouette Soft threads consist of absorbable PLA sutures equipped with bidirectional resorbable cones that function as anchoring elements within the subcutaneous tissues. The system is designed as a double-needle thread, with each end of the thread attached to a straight needle that allows symmetric placement along preplanned vectors. The threads are typically USP 3–0 PLA sutures with resorbable PLGA cones and absorbable spacers, which create mechanical fixation by compressing tissue between opposing cones. This configuration allows tissue repositioning and suspension of facial soft tissues through mechanical anchorage combined with subsequent collagen stimulation induced by PLA degradation.
For both, the procedures were performed using the standardized techniques established by the respective companies and their medical training teams. All physicians performing these procedures were trained and experienced in thread-lifting techniques and followed the technical recommendations, compliance guidelines, and clinical protocols provided by the manufacturers during certified training programs.
For the VectorLift technique, a total of 12 cannulated PDO threads were used per patient, consisting of 8 Mint ® Fine threads and 4 Petite threads (HansBiomed Co., Ltd., Seoul, South Korea).
Both thread types are composed of PDO, an absorbable polymer widely used in surgical sutures that undergoes hydrolytic degradation over several months while promoting localized collagen stimulation and tissue support.
Mint Fine threads are barbed PDO threads preloaded within a blunt-tip cannula, designed for lifting and repositioning of superficial facial soft tissues. These threads correspond approximately to USP 2–0 caliber and have an approximate length of 160 mm, with bidirectional molded barbs distributed along the thread body to provide multidirectional tissue engagement and lifting capability.
Mint Petite threads are shorter cannulated PDO threads intended for localized lifting and reinforcement of specific vector points, particularly in areas requiring more precise tissue repositioning. These threads typically correspond to USP 3–0 caliber, with an approximate length of 90 mm, and incorporate bidirectional barbed engagement structures that allow effective anchoring within the superficial subcutaneous plane.
No financial support or sponsorship was received from the manufacturers of the thread systems used in this study.
Anesthesia
For the VectorLift technique, a standardized protocol of optimized local anesthesia was established, as illustrated in Figure 1. This protocol was designed to achieve effective regional neural blockade while minimizing the total volume of anesthetic infiltration and reducing tissue edema during the procedure. The anesthetic approach focused on targeted extraoral infiltration at key anatomical points corresponding to sensory nerve pathways involved in the mid- and lower-face treatment areas.
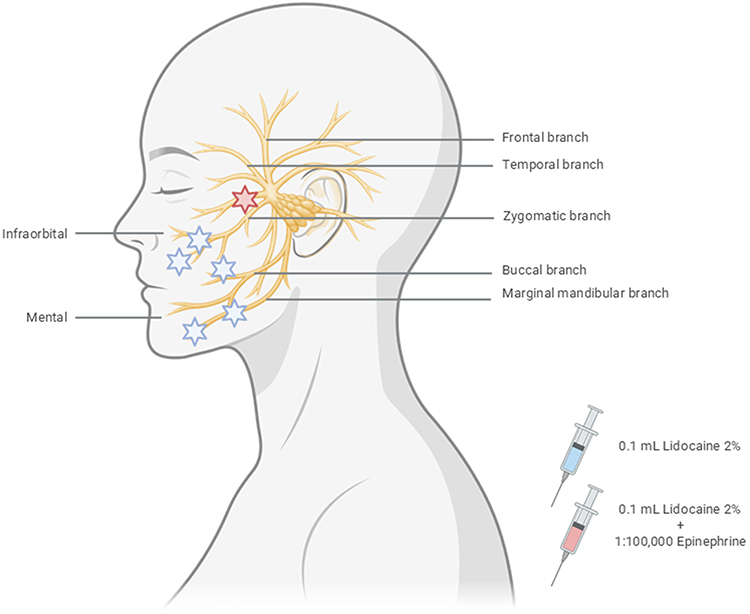 |
Figure 1 Optimized local anesthesia protocol for the VectorLift technique. This figure illustrates the standardized anesthesia protocol used for the VectorLift procedure. The approach was designed to achieve effective regional neural blockade while minimizing the total volume of anesthetic infiltration and reducing procedure-related tissue edema. The technique involves targeted extraoral infiltration at specific anatomical points corresponding to sensory nerve pathways of the mid- and lower-face treatment areas, allowing improved procedural comfort while limiting tissue distortion during thread placement. |
The injections were performed using 32-gauge, 4-mm needles at the subcutaneous level. Small boluses of 0.1 mL were administered at predefined anatomical points with the objective of temporarily modulating the motor conduction of the zygomatic, buccal, and marginal mandibular branches of the facial nerve, as well as the mental and infraorbital nerves. This targeted micro-bolus approach allows diffusion of the anesthetic solution within the superficial subcutaneous layer, producing a regional nerve block effect across the treatment vectors. In addition, lidocaine combined with epinephrine was infiltrated at the entry points to induce local vasoconstriction, thereby reducing the risk of intraoperative bleeding and postoperative bruising. The infiltration pattern also provides partial anesthetic coverage of adjacent neural branches, including areas corresponding to the temporal and upper cervical branches, further improving procedural tolerance. The controlled diffusion of these small anesthetic boluses facilitates effective neural blockade while avoiding the need for cannula-based hydro dissection or large infiltration volumes, which may otherwise contribute to increased tissue distension and postoperative edema.
For the other two thread-lifting techniques evaluated in this study, anesthesia was administered according to the protocols recommended by the respective manufacturers and their medical advisory teams for the specific thread systems used.
Local anesthetic solutions included 2% lidocaine (Fresenius Kabi, Germany) and 2% lidocaine with epinephrine 1:100,000 (Novocol, Canada). Depending on the procedural technique and anatomical location, anesthetic solutions were used either undiluted or diluted at a 1:10 ratio with sodium chloride 0.9% (Fresenius Kabi, Germany) in order to achieve appropriate anesthetic diffusion while minimizing local tissue distension. The dilution and infiltration strategy followed the recommendations established for each technique and thread system employed in the study.
Pain Assessment
Intraoperative pain was assessed during the thread-lifting procedure following local anesthetic infiltration. Pain perception was measured using the Numeric Rating Scale (NRS), a validated patient-reported outcome measure widely used for clinical pain assessment. The NRS is based on an 11-point scale ranging from 0 to 10, where 0 represents no pain and 10 represents the worst imaginable pain. This method allows rapid and reliable quantification of subjective pain intensity and has been extensively validated for use in both clinical practice and research settings.18
During each procedure, patients were asked to report their pain level using the NRS at five predefined time points throughout the intervention, beginning after the completion of the anesthetic infiltration and continuing during key stages of thread placement. Patients verbally reported their perceived pain intensity each time the assessment was requested.
The final intraoperative pain score for each patient was calculated as the mean value of the five NRS measurements obtained during the procedure, providing an overall estimate of pain experienced throughout the treatment. This approach allowed a more representative assessment of procedural tolerance by accounting for variations in discomfort that may occur during different stages of thread insertion and manipulation.
The Numeric Rating Scale has been shown to provide a reliable and sensitive measure of pain intensity and is commonly used in clinical research due to its simplicity, reproducibility, and ease of administration in real-time procedural settings.19
Satisfaction Rate
Patient satisfaction with facial appearance was evaluated using the FACE-Q Appearance Scale, a validated patient-reported outcome instrument specifically developed to assess outcomes in facial aesthetic procedures. The FACE-Q is a modular questionnaire designed to measure patient perceptions of facial appearance, quality of life, and treatment satisfaction following cosmetic interventions. It has been widely used in aesthetic medicine and plastic surgery research due to its strong psychometric properties, including reliability, validity, and sensitivity to clinical changes after aesthetic treatments.20
In the present study, the FACE-Q Facial Appearance Scale was used to assess patient-reported satisfaction with overall facial appearance. This scale evaluates patients’ perceptions of their facial attractiveness, harmony, and overall aesthetic satisfaction using a standardized questionnaire. Responses are converted into a Rasch-transformed score ranging from 0 to 100, where higher scores indicate greater satisfaction with facial appearance.
The questionnaire was administered before treatment and again two weeks after the thread-lifting procedure to evaluate early improvements in facial appearance following the intervention. The use of the FACE-Q instrument allowed standardized comparison of satisfaction outcomes among the different thread-lifting techniques evaluated in this study.
By measuring patient-reported outcomes using a validated scale, this assessment provided an objective method to evaluate perceived aesthetic improvement and the overall effectiveness of the treatment from the patient’s perspective.
After Procedure and Indications
All patients received standardized verbal and written post-procedure instructions immediately after treatment.
After completion of the thread-lifting procedure (for any of the three treatment modalities), a sterile patch applied over a thin film of topical antibiotic-corticosteroid cream was placed at all thread entry points. The cream used was Fucidin® H (fusidic acid 20 mg/g and hydrocortisone acetate 10 mg/g; LEO Laboratories Limited, Ireland). Patients were instructed to maintain the sterile patch in place for approximately 12 hours following the procedure. After removal, patients were advised to keep the entry areas clean and avoid the application of cosmetics or topical products on the treated sites for at least 48 hours to reduce the risk of local irritation or contamination during the early healing phase.
These recommendations were intended to minimize complications, optimize tissue healing, and maintain the stability of the inserted lifting threads during the early integration phase.
Patients were advised to limit excessive facial movements and avoid manipulation of the treated areas, including rubbing or massaging the face, for at least the first two weeks. They were instructed to avoid strenuous physical activity, heavy lifting, and intense exercise for approximately 1–2 weeks, as increased facial tension or blood flow may contribute to swelling, bruising, or thread displacement. Patients were also recommended to sleep in a supine position with the head slightly elevated, avoid excessive chewing or exaggerated facial expressions, and refrain from aesthetic facial treatments or massages during the early recovery period. In addition, patients were advised to avoid alcohol consumption, smoking, and medications that may increase bleeding risk during the first postoperative days, and to minimize direct sun exposure during the initial healing phase. When mild swelling or discomfort occurred, intermittent application of cold compresses was recommended.
These postoperative recommendations are consistent with commonly reported clinical guidance for absorbable thread-lifting procedures to support thread stabilization and reduce the risk of early complications.
Photo Documentation
High-resolution digital photographs were taken and collected using a digital portable camera, maintaining the angle, distance, background, and illumination as constant as possible.
Statistical Analysis
Statistical analyses were performed using GraphPad Prism version 10.4.2 (GraphPad Software, San Diego, CA, USA). Continuous variables are presented as mean ± standard error of the mean (SEM). Given the exploratory real-world comparative design of the study and the relatively limited sample size per treatment group, the statistical analysis was primarily focused on identifying overall trends and group-associated differences rather than establishing definitive causal superiority between techniques. Comparative analyses for continuous variables, including intraoperative pain scores, recovery time, and FACE-Q outcomes, were performed using two-way analysis of variance (ANOVA) followed by Tukey’s multiple-comparison post hoc test to account for intergroup variability and multiple pairwise comparisons or Welch’s t-test, as appropriate. Exact p-values were calculated whenever applicable. Categorical complication data were analyzed according to incidence and percentage within each treatment group using Fisher’s exact test, which was selected due to the relatively small sample size and the low expected frequencies observed in several complication categories. This statistical approach was considered the most appropriate and robust method for analyzing binary categorical outcomes under the present study conditions. Due to the exploratory nature of the study and the limited number of patients included per arm, confidence intervals and formal power calculations were not considered statistically robust or clinically informative for interpretation of the present dataset. A p-value <0.05 was considered statistically significant.
Results
VectorLift Technique: Procedural Design and Anatomical Rationale
The VectorLift technique is based on a standardized vectorial placement of cannulated PDO threads designed to reinforce key ligamentous structures and reposition superficial facial fat compartments. As illustrated in Figure 2A, the technique utilizes four Fine threads and two Petite threads per facial side, for a total of 12 threads per patient. The threads are inserted through three entry points per side following the anesthesia protocol described in the Materials and Methods section.
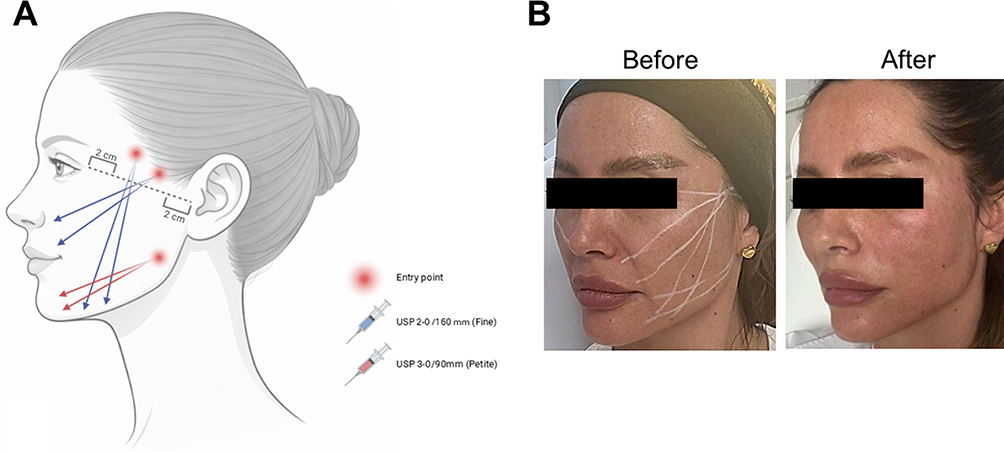 |
Figure 2 VectorLift thread placement design and clinical marking. (A) Schematic representation of the VectorLift technique showing the standardized vectorial placement of cannulated PDO threads. Four Fine (blue arrows) and two Petite threads (red arrows) are inserted per facial side, for a total of 12 threads per patient, using three entry points per side following the anesthesia protocol described in the Materials and Methods section. (B) Clinical example of the vectorial marking performed on a patient prior to the procedure, illustrating thread trajectories and entry points used for implantation. The panel also shows the immediate post-treatment result, highlighting the lifting effect achieved directly after the procedure. |
Figure 2B shows the clinical marking performed on a patient prior to the procedure, illustrating the vectorial orientation and entry points used for thread placement. The figure also demonstrates the immediate post-treatment result, highlighting the lifting effect achieved directly after the procedure.
The anatomical rationale of the VectorLift approach is illustrated in Figure 3A. The technique focuses on vectorial reinforcement of key facial retaining ligaments, allowing mechanical elevation of the overlying soft tissues. Specifically, the thread trajectories are designed to provide lifting support through interaction with the zygomatic ligament (A), masseteric ligament, mandibular ligament, and the platysma-auricular fascia complex (B). The proximal anchoring of the threads occurs in a stable support region located between the inferior temporal septum and the posterior region of the orbitomalar ligament (C), providing a strong fixation point that enhances lifting stability. Distally, the convergence of thread trajectories creates a high-density support area between the mandibular ligament and the mandibular septum (D), contributing to effective repositioning of the lower facial tissues.
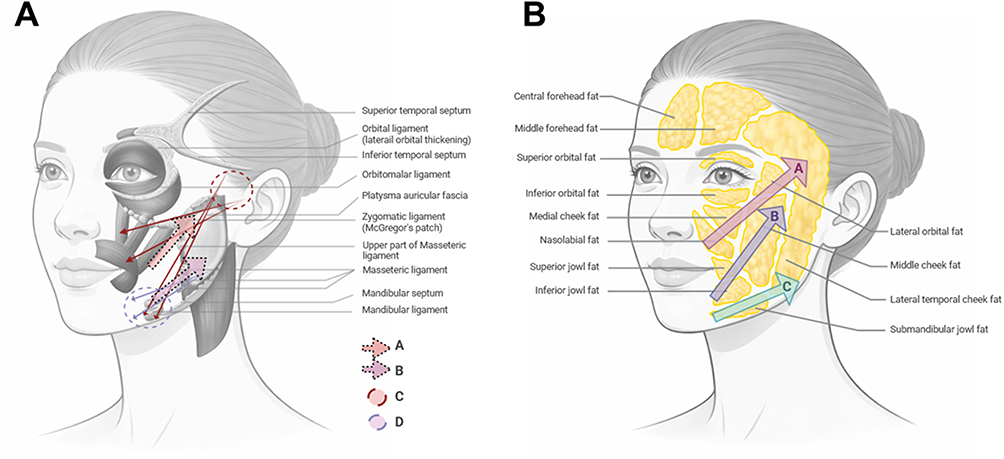 |
Figure 3 Anatomical rationale and lifting mechanism of the VectorLift technique. (A) Schematic illustration of the ligament-based vector reinforcement strategy used in the VectorLift approach. Red arrows represent Fine threads, while blue arrows represent Petite threads. Thread trajectories are designed to interact with key facial retaining ligaments, including the zygomatic ligament [A] masseteric ligament, mandibular ligament, and the platysma-auricular fascia complex [B]. Proximal anchoring occurs in a stable support region between the inferior temporal septum and the posterior region of the orbitomalar ligament [C] while distal thread convergence creates a high-density support zone between the mandibular ligament and the mandibular septum [D]. (B) Diagram illustrating the lifting effect on superficial facial fat compartments. Vectorial traction elevates the lateral orbital, medial cheek, and nasolabial fat compartments [A], as well as the superior and inferior jowl and middle cheek fat pads [B] and contributes to repositioning of the submandibular jowl and lateral temporal-cheek fat pad [C]. Together, these anatomical targets allow balanced tissue repositioning and immediate lifting with natural-appearing facial contours. |
The lifting effect on superficial fat compartments is schematically illustrated in Figure 3B. The vectorial traction generated by the threads is designed to elevate multiple facial fat pads in a coordinated manner. The primary lifting targets include the lateral orbital, medial cheek, and nasolabial fat compartments (A), followed by the superior and inferior jowl fat pads and the middle cheek compartment (B). Additionally, the technique contributes to repositioning of the submandibular jowl and the lateral temporal-cheek fat pad (C).
These anatomical targets were selected because they represent critical structural components involved in the development of facial ptosis during aging. By reinforcing ligamentous support structures and repositioning key superficial fat compartments, the VectorLift technique aims to generate a balanced and natural-appearing lifting effect, with high tissue retention capacity and immediate visible improvement following the procedure.
Representative Clinical Outcomes Following VectorLift Treatment
Figure 4 presents a representative panel of patients treated with the VectorLift technique. The figure includes standardized frontal and lateral photographs obtained before and immediately after treatment, illustrating the immediate clinical outcomes achieved with this approach. The patients shown represent four cases selected from the complete pool of treated individuals, chosen to illustrate typical results observed with the technique.
 |
Figure 4 Representative clinical outcomes following the VectorLift technique. Standardized frontal and lateral photographs of representative patients treated with the VectorLift technique. Images show pre-treatment and immediate post-treatment results demonstrating visible elevation and repositioning of mid- and lower-face tissues. Improvements include enhanced cheek projection, reduction in nasolabial fold prominence, and repositioning of the jowl region. Immediate post-procedure images show minimal signs of treatment-related trauma, with limited erythema and edema and, no clinically significant petechiae, dimpling, hematomas, or visible bruising. Representative patients include (A) a 57-year-old female with Fitzpatrick phototype II, (B) a 46-year-old female with phototype I, (C) a 52-year-old female with phototype III, and (D) a 41-year-old female with phototype IV, illustrating the applicability of the technique across different ages and skin phototypes. |
In all patients, an immediate improvement in tissue elevation and repositioning of the mid- and lower-face structures can be observed. The images demonstrate enhanced definition of facial contours, including improvement in the cheek projection, reduction in the prominence of the nasolabial folds, and repositioning of the jowl region. Importantly, the immediate post-procedure photographs show minimal signs of treatment-related trauma, including limited erythema and edema, and an absence of clinically significant petechiae, dimpling, skin irregularities, hematomas, or visible bruising. These clinical manifestations were quantified as “complications”.
Figure 4 includes a representative set of female patients treated with the VectorLift technique: (A) a 57-year-old patient with Fitzpatrick phototype II, (B) a 46-year-old patient with phototype I, (C) a 52-year-old patient with phototype III, and (D) a 41-year-old patient with phototype IV. The inclusion of patients across a range of ages and skin phototypes illustrates the applicability of the technique in diverse patient profiles.
Overall, the clinical images demonstrate that the VectorLift technique provides effective lifting and tissue repositioning while maintaining a minimally invasive profile, allowing visible aesthetic improvement immediately after the procedure with minimal signs of procedural trauma.
Procedural Tolerance, Recovery Time, and Patient Satisfaction Outcomes
The VectorLift technique demonstrated improved procedural tolerance and recovery characteristics compared with the other thread-lifting approaches evaluated in this study. As shown in Figure 5A, patients treated with the VectorLift technique reported significantly lower intraoperative pain levels, as measured using the Numeric Rating Scale (NRS), when compared with patients treated with the other two techniques. This finding suggests that the optimized anesthesia protocol and reduced tissue manipulation associated with the VectorLift approach contribute to improved patient comfort during the procedure.
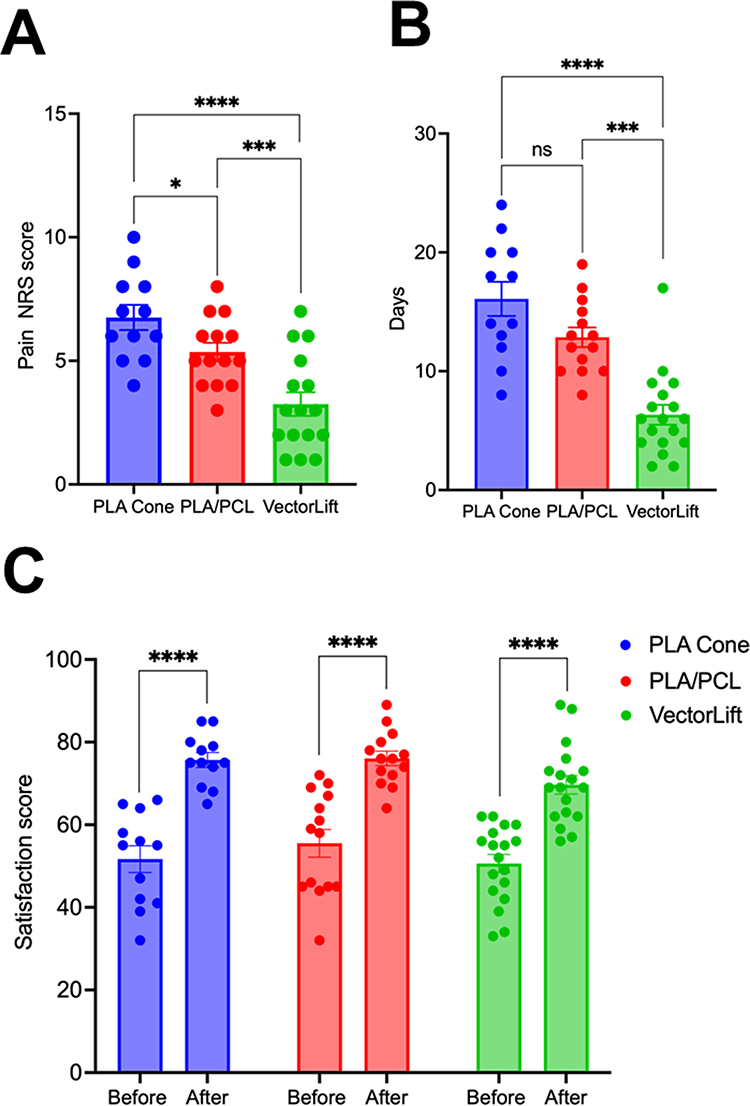 |
Figure 5 Procedural tolerance, recovery time, and patient satisfaction. (A) Intraoperative pain levels measured using the Numeric Rating Scale (NRS), demonstrating significantly lower pain scores in patients treated with the VectorLift technique compared with the other thread-lifting approaches evaluated. Data are presented as mean ± SEM, PLA Cone 6.750 ± 0.5094 (n = 12); PLA/PCL: 5.357 ± 0.3722 (n = 14); VectorLift: 3.250 ± 0.4787 (n = 16). PLA Cone vs PLA/PCL: mean difference = 1.655, 95% CI: 0.2382–3.071, *p < 0.05; PLA Cone vs VectorLift: mean difference = 4.012, 95% CI: 2.595–5.428, ****p < 0.0001; PLA/PCL vs VectorLift: mean difference = 2.357, 95% CI: 1.022–3.693, ***p < 0.001. (B) Recovery time expressed as days required for resolution of procedure-related signs and symptoms, including pain, edema, bruising, and skin irregularities, allowing return to normal daily activities. Patients treated with the VectorLift technique exhibited significantly shorter recovery periods. Data are presented as mean ± SEM, PLA Cone: 16.08 ± 1.438 (n=12); PLA/PCL: 12.86 ± 0.8245 (n=14); VectorLift:6.333 ± 0.8363 (n=18). PLA Cone vs PLA/PCL: mean difference =3.274, 95% CI: −0.8470–7.395, ns; PLA Cone vs VectorLift: mean difference = 10.06, 95% CI 5.939–14.18, ****p < 0.0001; PLA/PCL vs VectorLift: mean difference = 6.786, 95% CI: 2.901–10.67, ***p < 0.001. (C) Patient satisfaction measured using the FACE-Q Facial Appearance Scale before treatment and two weeks post-procedure. Satisfaction scores were comparable across the VectorLift treatment, indicating similar aesthetic outcomes despite differences in procedural tolerance and recovery. Data are presented as mean ± SEM, before: 50.61 ± 2.183 (n=18); after: 69.67 ± 2.232 (n=18). VectorLift: mean difference = 19.06, 95% CI: 12.71–25.40, ****p < 0.0001. Statistical analysis was performed using two-way ANOVA followed by Tukey’s multiple-comparison test or Welch’s t-test, as appropriate. |
In addition, the VectorLift technique showed a significant reduction in recovery time, quantified as the number of days required for patients to return to their baseline condition following treatment (Figure 5B). In the context of minimally invasive aesthetic procedures, recovery time is generally defined as the period required for the complete resolution of procedure-related signs and symptoms, including pain, edema, bruising, and visible skin irregularities, allowing patients to resume normal daily activities without noticeable treatment effects.
Despite the reduced procedural invasiveness and faster recovery profile, the VectorLift technique demonstrated significant improvement in facial appearance, as measured by the FACE-Q Facial Appearance Scale. Importantly, no statistically significant differences in satisfaction scores were observed among the three treatment modalities, indicating that the aesthetic outcomes achieved with VectorLift were comparable to those obtained with the other thread systems (Figure 5C).
These findings are particularly relevant considering that the comparator techniques involve widely used and previously reported effective thread-lifting approaches, including PLA/PCL cannulated threads and double-needle PLA cone-based systems. The ability of the VectorLift technique to achieve comparable patient satisfaction while providing lower intraoperative pain and faster recovery highlights its potential as a less invasive yet effective alternative for mid- and lower-face rejuvenation.
Post-Procedure Complications and Safety Outcomes
The incidence of treatment-related complications observed in the study population is summarized in Table 1. Overall, patients treated with the VectorLift technique demonstrated lower rates of immediate post-procedural complications, including dimpling or skin irregularities, bruising, edema, and immediate facial asymmetry, when compared with the other thread-lifting techniques evaluated in this study. These findings are consistent with the less invasive nature of the VectorLift approach, and the optimized anesthesia and vectorial placement strategy employed during the procedure.
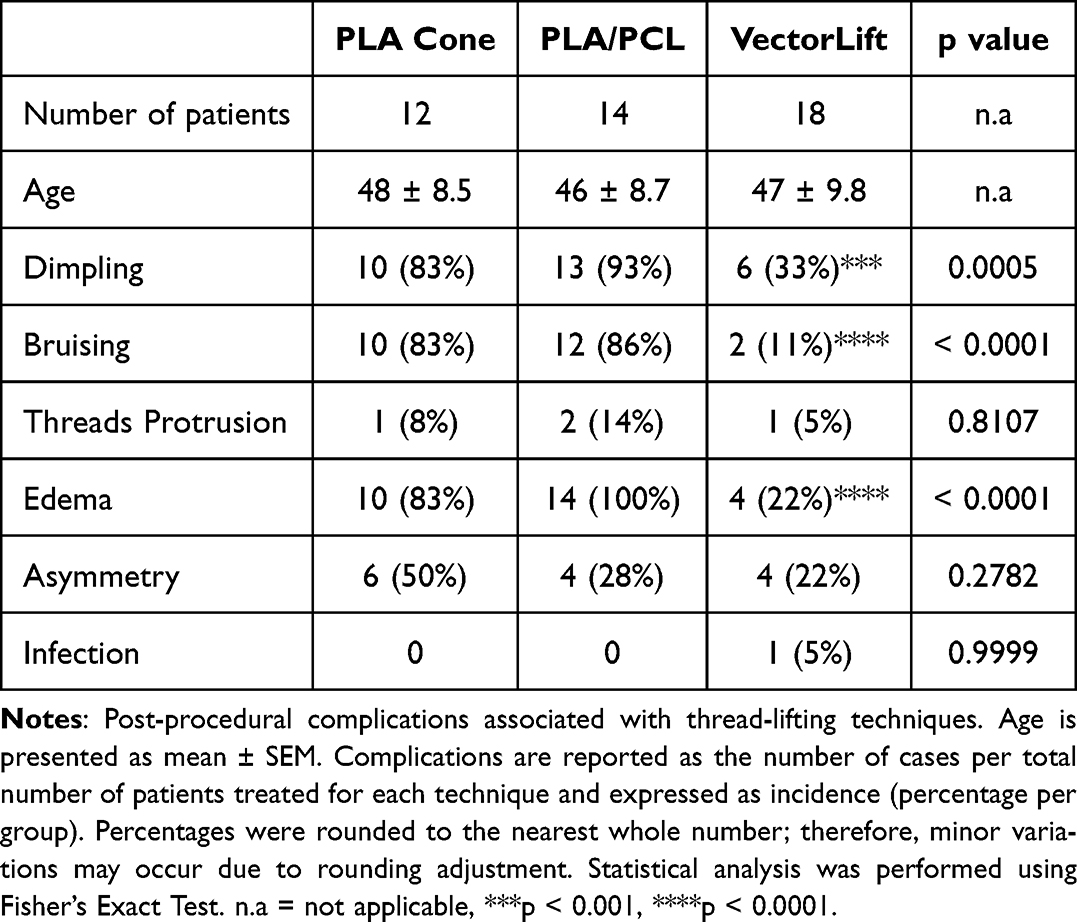 |
Table 1 Complication Incidences |
The incidence of thread protrusion was low and not significantly different among the three treatment groups. In most cases, thread protrusion was associated with excessive facial movement or premature return to physical exercise, often related to incomplete adherence to the post-procedure recommendations provided to the patients. These events were easily managed within the first 24 hours by trimming the exposed thread segment and covering the entry point with a sterile patch and topical antibiotic-corticosteroid cream.
One case of localized infection was reported in a patient treated with the VectorLift technique. The patient reported removal of the protective patch and the use of makeup and alcohol immediately after the procedure, despite having received detailed post-procedure care instructions. The complication was successfully resolved with oral doxycycline 200 mg/day for 7 days, combined with removal of the thread three days after the procedure, without further sequelae.
Importantly, no patients experienced dysesthesia, facial nerve injury, fasciculation, Stensen duct rupture (sialocele), post-inflammatory hyperpigmentation, visible threads, granuloma formation, or allergic reactions during or after the procedures. All complications reported in this study were temporary and mild, resolving either spontaneously or with simple supportive measures such as nonsteroidal anti-inflammatory medication, topical arnica preparations, or intermittent cold compresses. None of the complications resulted in permanent functional or aesthetic damage, and no patients required additional corrective procedures beyond the minor management measures described above.
Management of Post-Procedural Dimpling and Skin Irregularities
Post procedure dimpling was observed in a subset of patients, although at lower frequency in the VectorLift group compared with the other techniques shown in Table 1.
Although the incidence of dimpling in our study was lower with the VectorLift protocol compared with the other techniques evaluated, cases were still observed during the immediate post-procedural period. To manage this complication effectively and provide immediate correction, we developed a manual correction maneuver referred to as the “Compass Massage”, illustrated in Figure 6A.
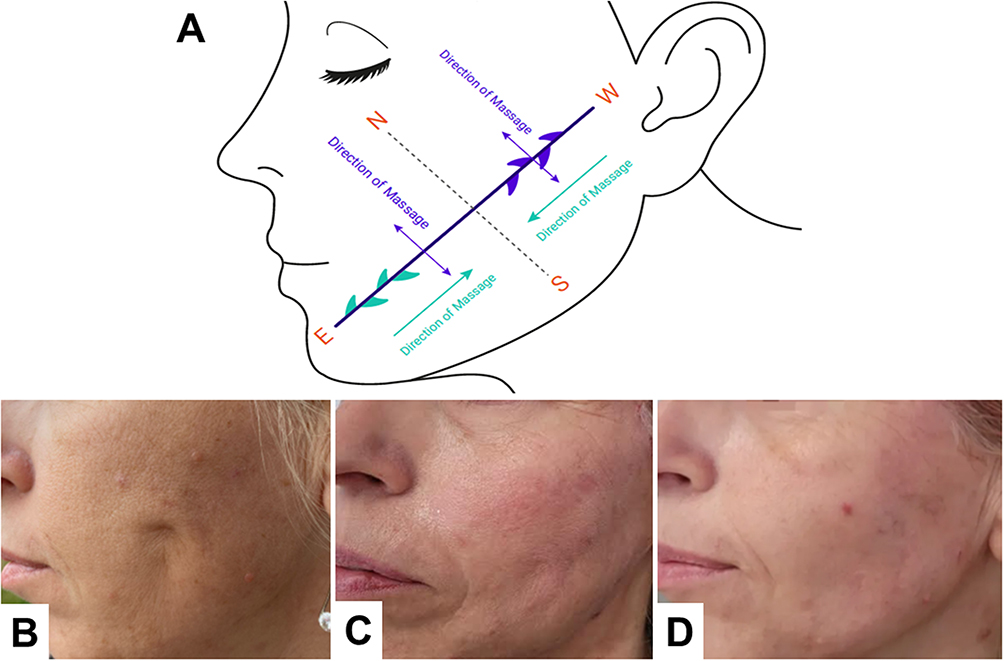 |
Figure 6 Compass Massage technique for the management of post-procedural dimpling. (A) Schematic representation of the Compass Massage maneuver developed to correct post-procedural dimpling or puckering associated with thread-lifting procedures. Directional massage movements are applied according to the position of the skin irregularity relative to the thread trajectory in order to release excessive tension between the barbed cogs and surrounding tissues. (B) Clinical example of dimpling observed immediately after thread insertion. (C) Immediate correction following application of the Compass Massage technique. (D) Appearance of the treated area 48 hours after the procedure, showing complete resolution of the skin irregularity. This minimally invasive maneuver allows rapid correction of dimpling, improving patient comfort and satisfaction while preserving the lifting effect of the threads. |
This technique is based on understanding the directional anatomy and engagement pattern of the barbed threads. Depending on the position of the puckering relative to the thread pathway, specific directional massage movements can be used to temporarily release the engagement of the cogs with the surrounding tissue. When puckering occurs in the distal portion of the thread, an upward massage along the vector direction (east-to-west) can be applied, optionally following local anesthetic infiltration, to release the engaged cogs and restore smooth tissue positioning. Conversely, when the dimpling occurs in the proximal segment of the thread, massage should be applied in the opposite direction (west-to-east) along the thread trajectory to reduce excessive tissue tension. Finally, a perpendicular massage from the mandibular angle toward the midline (north-to-south) can be performed to redistribute tension across the treated area and further smooth the skin surface.
The underlying causes are multifactorial and may include incorrect implantation depth, excessive traction applied during thread tightening, anatomical variations in superficial fat compartments, thin or atrophic skin, and localized tethering between the thread barbs and surrounding tissues. Changes in the distribution or mobility of facial fat pads can also contribute to uneven tension across the thread pathway, resulting in visible dimpling. This complication has been widely reported in the literature as a common but generally transient event associated with thread-lifting procedures.21
The effectiveness of this maneuver is illustrated in Figure 6B–D. Figure 6B shows a typical example of puckering observed after thread insertion. Figure 6C demonstrates the immediate correction of the dimpling following the Compass Massage maneuver, while Figure 6D illustrates the appearance of the treated skin 48 hours after the procedure, showing complete resolution without residual irregularities in a 54 years old patient that underwent the VectorLift technique.
This maneuver represents a simple, safe, and minimally invasive technique that allows immediate correction of post-procedural dimpling, thereby improving patient comfort and satisfaction. The effectiveness of this approach is facilitated by the 360-degree three-dimensional molded cog technology of the threads used in the VectorLift technique, which allows controlled disengagement and repositioning of the threads when directional pressure is applied.
Immediate correction of dimpling is clinically important because visible skin irregularities can generate significant patient concern and psychological stress during the recovery period, potentially increasing perceived downtime and reducing satisfaction with the procedure. Furthermore, persistent tissue tethering may theoretically increase the risk of localized nodules or fibrotic reactions if not properly addressed. For these reasons, the Compass Massage technique provides a valuable adjunct to the VectorLift protocol, allowing rapid resolution of skin irregularities while maintaining the lifting effect of the threads.
Discussion
The present study describes the development and clinical evaluation of the VectorLift technique, an optimized cannulated PDO thread-lifting approach designed to improve procedural tolerance and reduce downtime while maintaining aesthetic outcomes comparable to widely used thread-lifting systems. Our findings demonstrate that this technique provides significantly reduced intraoperative pain and shorter recovery time, while achieving similar patient satisfaction rates compared with PLA/PCL cannulated threads and double-needle PLA cone-based threads. In addition, the VectorLift protocol was associated with lower rates of common early complications, including edema, bruising, dimpling, and transient facial asymmetry. These findings suggest that a vector-optimized anatomical approach combined with targeted anesthesia infiltration may improve patient experience without compromising clinical effectiveness.
A key element underlying the effectiveness of thread lifting is the reinforcement of facial retaining ligaments, which play a critical role in maintaining soft-tissue support during aging.22 Facial aging is strongly associated with attenuation of ligamentous structures such as the zygomatic, masseteric, and mandibular ligaments, resulting in descent of superficial fat compartments and loss of facial contour.23 Mechanical repositioning of these structures through thread engagement can restore support and elevate ptotic tissues, producing a lifting effect that mimics certain aspects of surgical repositioning but with significantly lower invasiveness. Anatomical studies have demonstrated that successful thread-lifting outcomes depend largely on appropriate vector orientation and anchoring within stable ligamentous zones, which allow redistribution of mechanical tension across facial soft tissues.24
The use of PDO threads in aesthetic medicine has increased substantially in recent years due to their favorable safety profile and predictable biodegradation characteristics. PDO is a synthetic absorbable polymer widely used in surgical sutures since the 1980s and has demonstrated excellent biocompatibility, minimal inflammatory response, and gradual hydrolytic degradation within approximately 6–8 months.25 In addition to providing immediate mechanical lifting, PDO threads can stimulate mild collagen deposition around the thread pathway, contributing to tissue support during the resorption process.26 Clinical studies have reported that PDO-based thread lifting can provide effective short-term facial rejuvenation with a relatively low complication profile, particularly when performed by trained practitioners using appropriate patient selection and technique optimization.27
From an anatomical perspective, the VectorLift technique was designed to target specific ligamentous and fat-pad structures involved in mid- and lower-face aging. The vectorial orientation used in this protocol emphasizes engagement near the inferior temporal septum and orbitomalar region, while creating support convergence between the mandibular ligament and mandibular septum. This configuration facilitates elevation of multiple superficial fat compartments, including the nasolabial, cheek, and jowl fat pads, which play an important role in facial contour and perceived aging. Similar anatomical targets are commonly addressed in surgical lifting procedures, although surgical approaches typically involve extensive tissue dissection and longer recovery times. In contrast, minimally invasive procedures such as dermal fillers and biostimulator injectables, including poly-L-lactic acid and calcium hydroxyapatite, aim to restore facial structure through volume and collagen stimulation rather than mechanical repositioning. While these treatments can improve facial appearance, their mechanism differs from thread lifting, which provides a direct lifting effect through tissue anchoring.28–30
Appropriate patient selection remains a critical determinant of success in thread-lifting procedures. Ideal candidates typically present mild-to-moderate skin laxity with preserved facial volume and limited skin redundancy, allowing mechanical repositioning of tissues without the need for surgical excision. In our study, the technique demonstrated effectiveness across a range of ages and Fitzpatrick skin phototypes, suggesting that this approach may be suitable for diverse patient populations when anatomical indications are respected. Importantly, the technique should not be viewed as a replacement for surgical lifting in patients with advanced laxity but rather as a minimally invasive alternative for individuals seeking moderate improvement with reduced downtime.31,32
Patient tolerance is another important factor influencing acceptance of aesthetic procedures. Pain perception during minimally invasive treatments can significantly affect patient satisfaction and willingness to undergo future procedures. In the present real-world exploratory setting, the VectorLift protocol was associated with lower reported intraoperative pain scores, which may be related to the combination of targeted neural blockade and reduced tissue infiltration used in this approach. In contrast, some thread-lifting techniques may require larger anesthetic volumes or cannula-based hydrodissection, factors that could contribute to greater tissue distension, edema, or procedural discomfort. Additionally, the use of double-needle thread systems or higher numbers of threads may involve increased tissue manipulation, which could potentially influence the occurrence of hematomas or postoperative swelling. Importantly, despite the observed differences in procedural tolerance and recovery characteristics, patient satisfaction rates remained comparable among the evaluated techniques, suggesting that all approaches were capable of achieving clinically meaningful aesthetic improvement within the context of their respective indications and procedural characteristics.
The complication profile observed in this study is consistent with previously reported literature describing mostly mild and transient adverse events associated with thread lifting, such as bruising, swelling, dimpling, and temporary asymmetry.33 Notably, although the VectorLift technique showed lower complication rates, the other techniques evaluated in this study also demonstrated acceptable safety profiles and did not result in severe or permanent complications. Therefore, our findings should not be interpreted as suggesting that other thread-lifting systems are inferior or of lower quality. Instead, the results indicate that the VectorLift technique may represent an alternative option for patients seeking a less invasive approach with faster recovery, while the other techniques remain valuable tools that may provide advantages such as stronger lifting force, greater collagen stimulation, or longer durability.
Our findings are in accordance with previous studies evaluating PDO thread-lifting techniques using ultrasonographic follow-up. The authors demonstrated that PDO threads promote effective tissue repositioning and collagen formation with measurable improvement in facial sagging through ultrasound analysis.34 Interestingly, while their study confirmed the effectiveness of PDO-based lifting, our VectorLift approach additionally demonstrated improved procedural tolerance and reduced downtime, highlighting the potential clinical benefit of anatomically guided vector optimization and reduced tissue manipulation.
An important aspect addressed in this study is the management of post-procedural dimpling, a relatively common early complication reported after thread-lifting procedures. Dimpling may occur when excessive tension or superficial thread engagement produces localized tethering of the skin along the thread trajectory. In our clinical setting, we descriptively observed the potential usefulness of a manual maneuver referred to as the Compass Massage, which was developed as a practical adjunctive technique intended to reduce localized tissue tension through directional massage following thread placement. Manual massage has previously been suggested as a conservative management approach for thread-related irregularities, as controlled pressure may help redistribute tissue tension and facilitate relaxation without invasive intervention.35 The Compass Massage maneuver expands on this concept by incorporating directional manipulation according to thread orientation and the location of the irregularity. Although this approach was observed to be useful for immediate correction of dimpling in our experience, it should be interpreted as a descriptive technical adjunct rather than a formally validated therapeutic strategy. Immediate management of visible skin irregularities may nevertheless be clinically relevant, as these alterations can generate patient concern and negatively influence perceived recovery time and overall satisfaction during the early postoperative period.
This study has several limitations. First, the follow-up period was relatively short, which limits evaluation of the long-term durability of the treatment. However, long-term assessment was not the primary objective of this study, as many patients undergo maintenance aesthetic procedures that may influence perceived longevity of thread-lifting outcomes. Second, the study design was non-randomized and non-blinded, reflecting the ethical considerations inherent to aesthetic medicine, where treatment allocation based solely on experimental design may not align with patient preferences or clinical indications. Third, the sample size was relatively small, although since the establishment of the VectorLift protocol, more than 200 patients have been treated using this approach, indicating broader clinical applicability beyond the study population. Finally, male patients were not included, as anatomical differences and beard distribution may require adjustments to the technique; further research is ongoing to evaluate modifications of the protocol for male facial anatomy.
Despite the increasing popularity of thread-lifting procedures, some controversy remains regarding their scientific validation. A portion of the medical community has questioned the strength of the available evidence supporting these techniques and has highlighted the presence of a “significant theoretical and methodological gap in the subject of procedures for facial rejuvenation”.36 These concerns emphasize the need for well-designed clinical studies and rigorous scientific evaluation to better define the indications, effectiveness, and safety of thread-based lifting procedures. As authors, we strongly support the advancement of evidence-based aesthetic medicine and believe that continued investigation is essential to clarify the role of minimally invasive lifting techniques within the broader spectrum of facial rejuvenation strategies. We hope that the present study represents a modest but meaningful contribution toward strengthening the scientific foundation of this field.
Conclusion
The VectorLift technique represents an exploratory anatomically guided PDO thread-lifting approach developed within a real-world clinical setting with the aim of optimizing procedural tolerance and early recovery while achieving clinically meaningful aesthetic outcomes. The observational findings of this study suggest that the combination of vector-oriented thread placement, targeted anesthesia infiltration, and conservative management of common early complications may be associated with favorable short-term procedural characteristics and high patient satisfaction. However, given the non-randomized design, limited sample size, and short follow-up period, these findings should be interpreted cautiously. Further controlled studies with larger populations and longer-term follow-up are required to determine the reproducibility, durability, and comparative effectiveness of this approach.
Ethical Statement
The study was set in a private practice setting and an internal board of consultant physicians as Ethics Committee/Institutional Review Board (Comité de Ética para la Investigación Clínica) approved and supported the study under the code #ALR052023 by Total Skin Studio clinic as host institution. The data of the pilot study was approved and included in the analysis and data of this study.
Consent Statement
Each subject signed a comprehensive written informed consent that included granting permission for the acquisition and publication of photographs. This work was conducted according to the principles stated in the Declaration of Helsinki.
Acknowledgments
We thank all the patients for their participation and support during the study.
Disclosure
A Leguina-Ruzzi is a Key Opinion Leader for Hyalual, MAD Skincare, Hansbiomed, Armesso and Tlab and has received stipends as a speaker unrelated to this study.
The rest of authors have nothing to disclose.
The authors declare that the manufacturer had no role in the study design, data collection, data analysis, interpretation of results, figure preparation, or manuscript writing. Furthermore, no products were provided free of charge or at a discounted rate by the manufacturer, and the study was conducted independently without any form of industry involvement or influence.
References
1. Hong GW, Kim SB, Park SY, Wan J, Yi KH. Thread lifting materials: a review of its difference in terms of technical and mechanical perspective. Clin Cosmet Invest Dermatol. 2024;17:999–17. PMID: 38737945; PMCID: PMC11086642. doi:10.2147/CCID.S457352
2. Adam A, Karypidis D, Ghanem A. Thread lifts: a critical analysis of treatment modalities. J Drugs Dermatol. 2020;19(4):413–417. PMID: 32272519. doi:10.36849/JDD.2020.3646
3. Sulamanidze M, Sulamanidze G. Facial lifting with aptos methods. J Cutan Aesthet Surg. 2008;1(1):7–11. PMID: 20300331; PMCID: PMC2840891. doi:10.4103/0974-2077.41149
4. Lee H, Yoon K, Lee M. Outcome of facial rejuvenation with polydioxanone thread for Asians. J Cosmet Laser Ther. 2018;20(3):189–192. PMID: 29271683. doi:10.1080/14764172.2017.1400167
5. Wong V. The science of absorbable Poly(L-Lactide-Co-ε-Caprolactone) threads for soft tissue repositioning of the face: an evidence-based evaluation of their physical properties and clinical application. Clin Cosmet Invest Dermatol. 2021;14:45–54. PMID: 33469333; PMCID: PMC7812524. doi:10.2147/CCID.S274160
6. Hong GW, Kim SB, Park SY, Wan J, Yi KH. Basic concepts in facial and neck thread lifting procedures. Skin Res Technol. 2024;30(4):e13673. PMID: 38584590; PMCID: PMC10999942. doi:10.1111/srt.13673
7. Wong C-H, Mendelson BC. Facial anatomy and ageing. In: Farhadieh RD, Bulstrode NW, Cugno S, eds. Plastic and Reconstructive Surgery. 2015. doi:10.1002/9781118655412.ch65
8. Garvey PB, Ricciardelli EJ, Gampper T. Outcomes in threadlift for facial rejuvenation. Ann Plast Surg. 2009;62(5):482–485. PMID: 19387145. doi:10.1097/SAP.0b013e31818c18ed
9. Unal M, Islamoğlu GK, Ürün Unal G, Köylü N. Experiences of barbed polydioxanone (PDO) cog thread for facial rejuvenation and our technique to prevent thread migration. J DermatolTreat. 2021;32(2):227–230. PMID: 31267809. doi:10.1080/09546634.2019.1640347
10. Saray A. Brow lifting with Poly-L-Lactic Acid (PLLA) and Polylactide/Glycolide (PGA), resorbable and coned threads. Aesthetic Plast Surg. 2025;49(23):6383–6392. PMID: 40855019. doi:10.1007/s00266-025-05117-y
11. Sulamanidze G, Nikishin D, Kajaia A. Benefits of P(LA/CL)-Hyaluronic acid threads with innovative hyaluronic acid coating technology (NAMICA)-Preclinical test results. J Cosmet Dermatol. 2025;24(10):e70502. PMID: 41098145; PMCID: PMC12529244. doi:10.1111/jocd.70502
12. Cao L, Qiu H, Yu D, Shuo L, Wang H. Comparison of different thread products for facial rejuvenation: materials and barb designs. J Cosmet Dermatol. 2023;22(7):1988–1994. PMID: 36994594. doi:10.1111/jocd.15691
13. Pham CT, Chu S, Foulad DP, Mesinkovska NA. Safety profile of thread lifts on the face and neck: an evidence-based systematic review. Dermatol Surg. 2021;47(11):1460–1465. doi:10.1097/DSS.0000000000003189
14. Bertossi D, Botti G, Gualdi A, et al. Effectiveness, longevity, and complications of facelift by barbed suture insertion. Aesthet Surg J. 2019;39(3):241–247. PMID: 29474522. doi:10.1093/asj/sjy042
15. Hong G-W, Hu H, Park S-Y, Wan J, Yi K-H. What are the factors that enable thread lifting to last longer? Cosmetics. 2024;11:42. doi:10.3390/cosmetics11020042
16. Tamura T, Okumura K, Funakoshi Y, Teranishi H. Multicenter review of more than 110,000 facial thread lifting cases from a cosmetic surgery group. Plast Reconstr Surg Glob Open. 2025;13(12):e7335. PMID: 41346928; PMCID: PMC12674162. doi:10.1097/GOX.0000000000007335
17. Suh DH, Jang HW, Lee SJ, Lee WS, Ryu HJ. Outcomes of polydioxanone knotless thread lifting for facial rejuvenation. Dermatol Surg. 2015;41(6):720–725. PMID: 25993611. doi:10.1097/DSS.0000000000000368
18. Choi S, Yoon SH, Lee HJ. Beyond measurement: a deep dive into the commonly used pain scales for postoperative pain assessment. Korean J Pain. 2024;37(3):188–200. PMID: 38769013; PMCID: PMC11220383. doi:10.3344/kjp.24069
19. Johnson C. Measuring pain. visual analog scale versus numeric pain scale: what is the difference? J Chiropr Med. 2005;4:43–44. doi:10.1016/S0899-3467(07)60112-8
20. Pusic AL, Klassen AF, Scott AM, Cano SJ. Development and psychometric evaluation of the FACE-Q satisfaction with appearance scale: a new patient-reported outcome instrument for facial aesthetics patients. Clin Plast Surg. 2013;40(2):249–260. PMID: 23506765. doi:10.1016/j.cps.2012.12.001
21. Yi KH, Park SY. Facial thread lifting complications. J Cosmet Dermatol. 2025;24(1):e16745. PMID: 39760325; PMCID: PMC11702150. doi:10.1111/jocd.16745
22. Mendelson B, Wong CH. Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesthetic Plast Surg. 2012;36(4):753–760. PMID: 22580543; PMCID: PMC3404279. doi:10.1007/s00266-012-9904-3
23. Furnas DW. The retaining ligaments of the cheek. Plast Reconstr Surg. 1989;83(1):11–16. PMID: 2909050. doi:10.1097/00006534-198901000-00003
24. Mendelson BC, Muzaffar AR, Adams WP. Surgical anatomy of the midcheek and malar mounds. Plast Reconstr Surg. 2002. 110(3):885–896. 10.1097/00006534-200209010-00026. discussion 897-911. PMID: 12172155.
25. Matarasso A, Ruff GL. The history of barbed sutures. Aesthetic Surgery Journal. 2013;33(3_Supplement):12S–16S. doi:10.1177/1090820X13498505
26. Ruff G. Technique and uses for absorbable barbed sutures. Aesthet Surg J. 2006;26(5):620–628. PMID: 19338953. doi:10.1016/j.asj.2006.08.011
27. Kochhar A, Kumar P, Karimi K. Minimally invasive techniques for facial rejuvenation utilizing polydioxanone threads. Clin Plast Surg. 2023;50(3):465–477. PMID: 37169412. doi:10.1016/j.cps.2022.12.011
28. Fitzgerald R, Carqueville J, Yang PT. An approach to structural facial rejuvenation with fillers in women. Int J Womens Dermatol. 2018;5(1):52–67. PMID: 30809580; PMCID: PMC6374711. doi:10.1016/j.ijwd.2018.08.011
29. Kontis TC, Rivkin A. The history of injectable facial fillers. Facial Plast Surg. 2009;25(2):67–72. PMID: 19415573. doi:10.1055/s-0029-1220645
30. Sundaram H, Liew S, Signorini M, et al; Global Aesthetics Consensus Group. Global aesthetics consensus: hyaluronic acid fillers and botulinum toxin type a-recommendations for combined treatment and optimizing outcomes in diverse patient populations. Plast Reconstr Surg. 2016;137(5):1410–1423. PMID: 27119917; PMCID: PMC5242215. doi:10.1097/PRS.0000000000002119
31. Maas CS, Bapna S. Pins and needles: minimally invasive office techniques for facial rejuvenation. Facial Plast Surg. 2009;25(4):260–269. PMID: 19924599. doi:10.1055/s-0029-1242038
32. Gallo L, Churchill I, Kim P, et al. Patient factors that impact FACE-Q aesthetics outcomes: an exploratory cross-sectional regression analysis. Aesthet Surg J. 2025;45(6):543–551. PMID: 39930866; PMCID: PMC12080882. doi:10.1093/asj/sjaf027
33. Brummund D, Puebla B, Ruiz S, Mir H, Morejon O. Review of outpatient aesthetic surgery complications. Plast Reconstr Surg Glob Open. 2022;10(10 Suppl):151–152. PMCID: PMC9592380. doi:10.1097/01.GOX.0000899116.49172.08
34. Lots TCC. Effect of pdo facelift threads on facial skin tissues: an ultrasonographic analysis. J Cosmet Dermatol. 2023;22(9):2534–2541. doi:10.1111/jocd.15761
35. Wang CK. Complications of thread lift about skin dimpling and thread extrusion. Dermatol Ther. 2020;33(4):e13446. PMID: 32323425; PMCID: PMC7507174. doi:10.1111/dth.13446
36. Contreras C, Ariza-Donado A, Ariza-Fontalvo A. Using PDO threads: a scarcely studied rejuvenation technique. Case report and systematic review. J Cosmet Dermatol. 2023;22:2158–2165.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.