Back to Journals » Open Access Journal of Contraception » Volume 7
Varying family planning strategies across age categories: differences in factors associated with current modern contraceptive use among youth and adult women in Luanda, Angola
Authors Prata N ![]() , Bell S, Weidert K, Nieto-Andrade B, Carvahlo A, Neves I
, Bell S, Weidert K, Nieto-Andrade B, Carvahlo A, Neves I
Received 5 August 2015
Accepted for publication 21 October 2015
Published 28 January 2016 Volume 2016:7 Pages 1—9
DOI https://doi.org/10.2147/OAJC.S93794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Ndola Prata,1 Suzanne Bell,1 Karen Weidert,1 Benjamin Nieto-Andrade,2 Adelaide Carvalho,3 Isilda Neves3
1Bixby Center for Population, Health and Sustainability, School of Public Health, University of California at Berkeley, Berkeley, CA, USA; 2Population Services International Angola, 3National Directorate of Public Health, Ministry of Health, Luanda, Angola
Background: The objective of this study is to identify factors associated with current modern contraceptive use among Angolan women. By differentiating according to age groups (15–24 and 25–49 years), this study aimed to help family planning program planners better tailor interventions to improve utilization of modern contraception.
Methods: A household survey was used to collect data from 1,545 women of reproductive age living in Luanda Province, Angola. Data on sociodemographic characteristics, reproductive behavior and intentions, contraceptive knowledge and use, and attitudes and beliefs regarding contraception and abortion were collected. The analyses were stratified based on age: 15–24 years (youth) and 25–49 years (adult). Multivariate logistic regression models were built for each age group, adding different subsets of variables in groups to see how relationships changed across the models.
Results: Common factors associated with modern contraceptive use among all ages include education level, perceived contraceptive accessibility, contraceptive knowledge, communication with partner about family planning in last year, and self-efficacy. Exposure to family planning information in the media in the last few months, perceived partner approval of family planning, and marital status were all positively associated with current modern contraceptive use among women aged 15–24 years. Meanwhile, receiving information about family planning from a pharmacy in the last year was uniquely associated with current modern contraceptive use among women aged 25–49 years.
Conclusion: Young women in Luanda, Angola seem to have a unique set of factors affecting their contraceptive use. These findings highlight the need for family planning programs to cater services and messages toward specific age groups.
Keywords: contraceptive uptake, contraceptive access, contraceptive self-efficacy, partner communication
Introduction
The critical role that family planning plays in improving maternal and child health outcomes has become widely recognized among governments and donors alike in the last decade. Additionally, many policy makers acknowledge the importance of expanding family planning programs in order to improve overall socioeconomic development in low-resource countries.1–3 In order to tailor programs to best meet the growing needs of women, studying factors associated with modern contraceptive uptake is necessary. Previous research conducted in Sub-Saharan Africa has demonstrated that individual factors such as household socioeconomic status, age, education, parity, sociocultural beliefs, and spousal communication affect family planning use.4–9 Though research typically generalizes contraceptive use among all women with age as a covariate, more recent studies have highlighted the need to differentiate by age when studying factors affecting contraception use, with many studies providing evidence that young women in particular need special attention in order to increase contraceptive prevalence, recognizing that improving availability, affordability, and youth-friendliness may not fully address the psycho-social barriers to contraceptive use among them.7,10–12
The objective of this paper is to explore differences in factors associated with modern contraceptive use between young and adult women of reproductive age in Luanda, Angola. As the government and the private sector work to improve reproductive health in Angola, results from this study can help identify unique factors upon which family planning programs can intervene to improve utilization of modern contraception.
Background
In part due to the protracted nearly 30-year civil war that ended in 2002, there are limited data regarding the reproductive health status of women in Angola. Additionally, fertility levels and aspirations in Angola changed both as a result of the conflict and migration associated with the civil war. In an analysis of war-related differences in reproductive preferences using data from a 1996 survey (a few years after a major outbreak of war), Agadjanian and Prata13 found a wartime drop and a postwar rebound in fertility. In a study of war, migration, and fertility in Angola, Avogo and Agadjanian14 found that in a given year, migration related to the war was associated with a lower probability of birth than war-related migration.
Over a decade of peace may have had an effect on fertility preferences in Angola. Although the country has made substantial economic and political progress in recent years, women’s health has continued to suffer. Estimates indicate that the maternal mortality ratio is 450 per 100,000 live births,15 and recent estimates of modern contraceptive prevalence in the country is ~12%.16 With an estimated national population of over 24 million people in 2015,17 the current and very high total fertility rate of 6.3 children per woman is reflected in the country’s rapid population growth rate of 3.1% per year.18 Total fertility rates are highest among the poorest and least educated (8.0) and lowest among those with secondary education or higher (3.3) and in the highest wealth quintile (4.5). In Luanda, the capital and largest city in Angola, the total fertility rate is 4.4.19
Existing data clearly indicate that a concerted effort is necessary to increase contraceptive prevalence throughout the country. In a more recent study, Decker and Constantine20 used data from 2002 and found women’s educational level, wealth, and area of residence influence contraceptive use. Women in urban areas had three times the contraceptive prevalence rates as compared with their counterparts in rural areas (9.4% vs 3.0%). They also found age to be associated with contraceptive use, with an especially low level of contraceptive use among adolescents, concluding that young women needed special attention with regards to family services in Angola.20 Policy makers in Angola would be remiss to not take young women’s needs into consideration when developing family planning strategies, given that 48% of the country is less than 15 years old16 and fertility rates are high at 191 and 261 births per 1,000 women aged 15–19 and 20–24 years, respectively.19 Fortunately, the National Strategic Plan for Reproductive Health21 has made a reduction in sex disparities and an increase in family planning coverage and options key objectives, with an overall intention of improving women’s health. Understanding the factors associated with women’s use of modern contraception methods will play an important role in reaching this goal.
Methods
Setting and sample
Luanda province includes the capital city of Angola and, at the time of the survey, the province included nine municipalities (Cacuaco, Viana, Cazenga, Maianga, Imgombota, Kilamba Kiaxi, Rangel, Samba, and Sabizamga). Only two of the municipalities had rural communities (Cacuaco and Viana), the remaining were urban. A more recent geopolitical division shows Luanda province with only seven municipalities: several urban municipalities were joined to make the municipality of Luanda and three new municipalities were added, each of which includes rural communities.
The study population is women aged 15–49 years who resided in the Luanda Province at the time of the survey, October through November of 2012. SINFIC (Sistemas de Informação Industriais e Consultoria), a local marketing firm, carried out the data collection on behalf of the University of California, Berkeley Bixby Center for Population, Health, and Sustainability (Bixby Center) and Population Services International (PSI) Angola. A representative sample of women of reproductive age from all municipalities in Luanda Province was captured using a multistage random sampling design. The sample was distributed proportionally across the nine municipalities of Luanda Province. Within each municipality, interviewers randomly selected a number of “sampling points” (eg, churches, hospitals, gas stations, etc) from a sampling framework created for that purpose. A fixed number of participants were randomly selected from each sampling point and one woman from each household was asked to participate in the interview. In total, 1,825 women of reproductive age living in Luanda were selected to be interviewed. Eighty-five percent completed the survey, 8% started but did not complete the survey, 6% refused to participate, and 2% did not participate due to other reasons. All women provided verbal consent before taking part in the interview, and the interviewers signed to confirm that consent was given for each interviewee. Ethical approval for this study was provided by the University of California, Berkeley Center for Protection of Human Subjects (CPHS # 2011-08-3521). Approval was also provided by the Ethical Committee at the Instituto de Saude Publica in Luanda, Angola.
Data source
The study uses data collected with a survey instrument that was developed by researchers from the Bixby Center. The instrument was modeled on the Women’s Questionnaire of the Demographic and Health Surveys22 and Angola’s Malaria Indicator Survey,19 with additional standardized questions included from the PSI Tracking Results Continuously survey tools. It was designed to assess women’s knowledge, attitudes, and practices, as well as opportunities, ability, and motivation, related to childbearing and family planning. The survey also collected information regarding women’s experiences with reproductive health services and their preferences related to the delivery of family planning services. All items and response options in the survey instrument were initially developed in English and later translated into Portuguese by the research team, with feedback from PSI Angola. Once a final version was decided upon, the survey instrument was pilot tested among 30 women of reproductive age in Luanda, Angola. Feedback from this phase was incorporated and the final version was then back translated into English to ensure accuracy.
Variables
The dependent variable was current use of a modern method of family planning. It was dichotomous (yes/no) with no as reference group, which encompassed both nonusers of any form of contraception and users of traditional methods. Given the small number of users of traditional (n=35, 2.6%) methods, its users were combined with those using no method at all for this analysis.
Independent variables of interest included sociodemographic and individual factors that were found to influence modern contraceptive uptake in literature. Sociodemographic variables included age, marital status, education, and wealth quintile derived from a principal components analysis of household assets, including building materials and household amenities, following the methodology used by Demographic and Health Surveys.
To determine contraceptive knowledge, respondents were asked to list contraceptive methods they had heard of, both spontaneously and with probing (0–12 methods). Knowledge of specific contraceptive methods was determined by the number of correct answers in response to questions surrounding correct use and side effects. Accessibility of contraception and receipt of information on family planning from a pharmacy were both dichotomously coded (yes/no) in response to the questions: 1) Are contraceptives accessible to you? 2) In the last 12 months, have you received any information or counseling on family planning/contraception while visiting a pharmacy? Exposure to family planning information in the last few months was dichotomously coded (yes/no) in response to whether they had heard about family planning on radio, television, or in newspaper/magazine in last few months.
Recent couple communication was determined by measuring the number of times surveyed women had discussed family planning with her husband/partner in the last year (none, once or twice, more often). The contraceptive self-efficacy index was developed using principal components analysis of variables included in the survey which measure self-efficacy, including: capability of using contraceptives; ability to use methods correctly and consistently to space births; communicate about preventing pregnancy; and negotiate contraceptive use and use contraception in the face of husband/partner opposition. “Perceived approval of family planning” was captured by the question: Do you think your husband/partner/boyfriend approves of couples using family planning? Responses were categorized dichotomously (yes/no or do not know), with no or do not know as the reference group.
Statistical analyses
Descriptive statistics were analyzed to explore dependent and independent variables of interest. At the multivariate level, the relationship between select variables of interest and the dependent variable (current use of modern contraception) was estimated using a multiple logistic regression model. A one-way analysis of variance analysis was used to determine the average value of each variable in the logistic model among contraceptive users compared with noncontraceptive users.
It was hypothesized a priori that factors associated with current modern contraceptive use would differ by age, thus, we stratified the analyses into two categories: women aged 15–24 years and women aged 25–49 years. Additional analyses included all women of reproductive age. We were unable to stratify further due to limited sample size and power. Focusing on factors upon which family planning programs could intervene, we selected a number of variables from the data that we hypothesized could be related to current modern contraceptive use based on review of the literature. Bivariate analyses were used to investigate the association between each variable and the current modern contraceptive use. After identifying variables that were significantly associated at the P<0.10 level with the dependent variable, we engaged in a model building process wherein we built a series of multivariate models for each age group, gradually adding different subsets of variables to see how relationships changed across the models. Only significant variables were retained in the progression to later models.
In Model 1, we tested the significance of sociodemographic variables with current modern contraceptive use. Significant variables were retained and a question about perceived contraceptive accessibility was added to create Model 2. In Model 3, questions regarding contraceptive knowledge/exposure were added; in Model 4, questions regarding sex dynamics/social norms were added; and in Model 5, the self-efficacy scale was added. Each model contained only the significant variables from the previous models and the additional variable(s) of interest. Researchers used P-values and 95% confidence intervals (CIs) to determine significance.
Results
The analytical sample was derived from a larger study sample of 1,825 women of reproductive age living in Luanda and was restricted to fecund women of reproductive age who completed the survey (n=1,342). Over half of the population was less than 25 years old (57%) and had at least secondary education (56%), while nearly three-quarters were not married or cohabiting (data not shown). Fifty-five percent of women in the subsample of this analysis reported current use of a modern contraceptive method. Half of the users were using condoms (55.5%) followed by injectable contraceptives (21.5%) and pills (18.5%). A much smaller percentage of women were using implants (2.8%), intrauterine devices (1.5%), or other modern contraceptives (0.6%) (data not shown).
As seen in Table 1, overall contraceptive prevalence was 55%, but women aged 25–49 years (66%) were more likely to be currently using modern contraceptives than women aged 15–24 years (48%). This trend was seen across many of the sociodemographic and other variables. There were some variables that did not adhere to this trend, most notably marital status, where married women aged 15–24 years (76%) were more likely than married women aged 25–49 years (68%) to currently be using modern contraceptives. Among single women, the opposite was true: 45% of 15–24-year-olds and 63% of 25–49-year-olds were using modern contraception. Younger women with no exposure to family planning information in the media in the last few months had a low prevalence of modern contraceptive use (35%) compared with those who were exposed (58%); exposure to family planning messages did not appear to be associated with contraceptive use in older women.
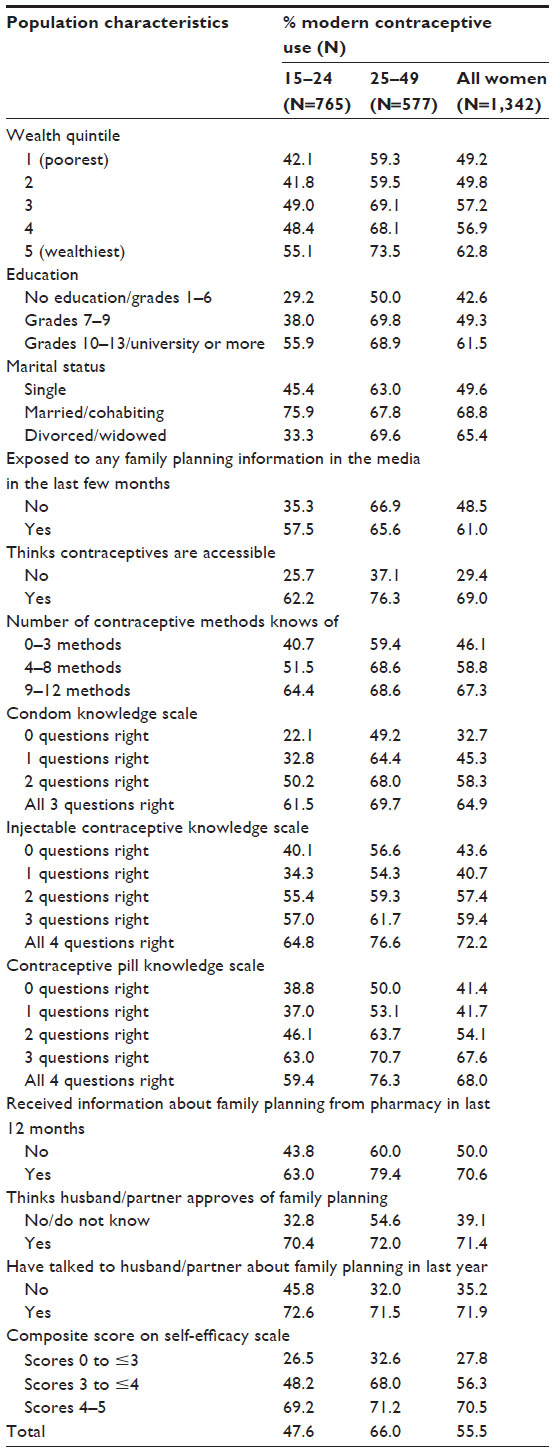 | Table 1 Percent modern contraceptive use across covariates from final models by age group among women of reproductive age in Luanda, Angola |
The multivariate analysis assessed distinct differences in factors associated with current modern contraceptive use between women aged 15–24 years (Table 2) and 25–49 years (Table 3), while also indicating which factors influenced contraceptive use among all women of reproductive age (Table 4). Factors associated with current modern contraceptive use in the final models among all three analysis groups included education level, perceived contraceptive accessibility, contraceptive knowledge, whether respondent had talked to her husband/partner about family planning in the last year, and self-efficacy. For young women, only condom knowledge positively influenced contraceptive use (odds ratio [OR] =1.44, 95% CI 1.18–1.75), whereas contraceptive use among older women was positively associated with injectable contraceptive knowledge (OR =1.31, 95% CI 1.11–1.53) and contraceptive pill knowledge (OR =1.26, 95% CI 1.05–1.50). Additionally, exposure to family planning information in the media in the last few months was positively associated with current modern contraceptive use uniquely among women aged 15–24 years (OR =1.98, 95% CI 1.39–2.82), as was perceived husband/partner approval of family planning (OR =2.39, 95% CI 1.63–3.51). Meanwhile, receiving information about family planning from a pharmacy in the last year was uniquely associated with current modern contraceptive use among women aged 25–49 years (OR =2.51, 95% CI 1.40–4.51).
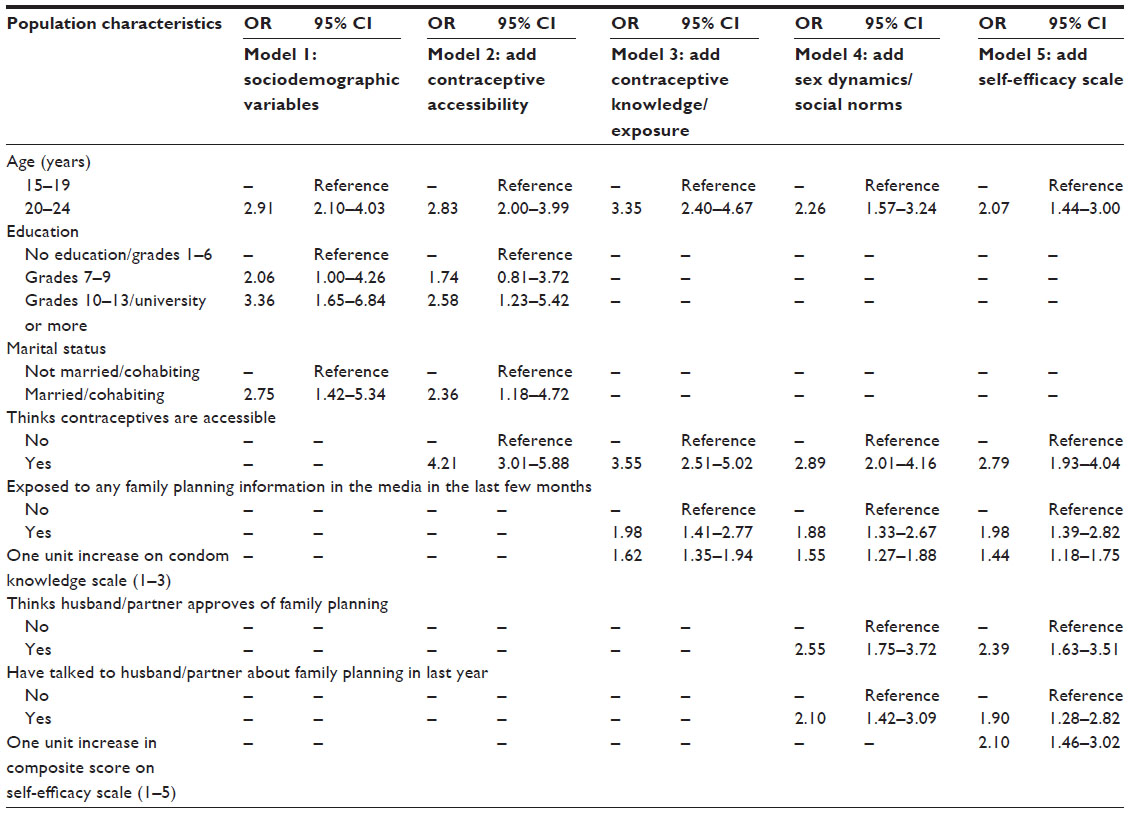 | Table 2 Model building for factors significantly associated with current modern contraceptive use among women aged 15–24 years in Luanda, Angola* |
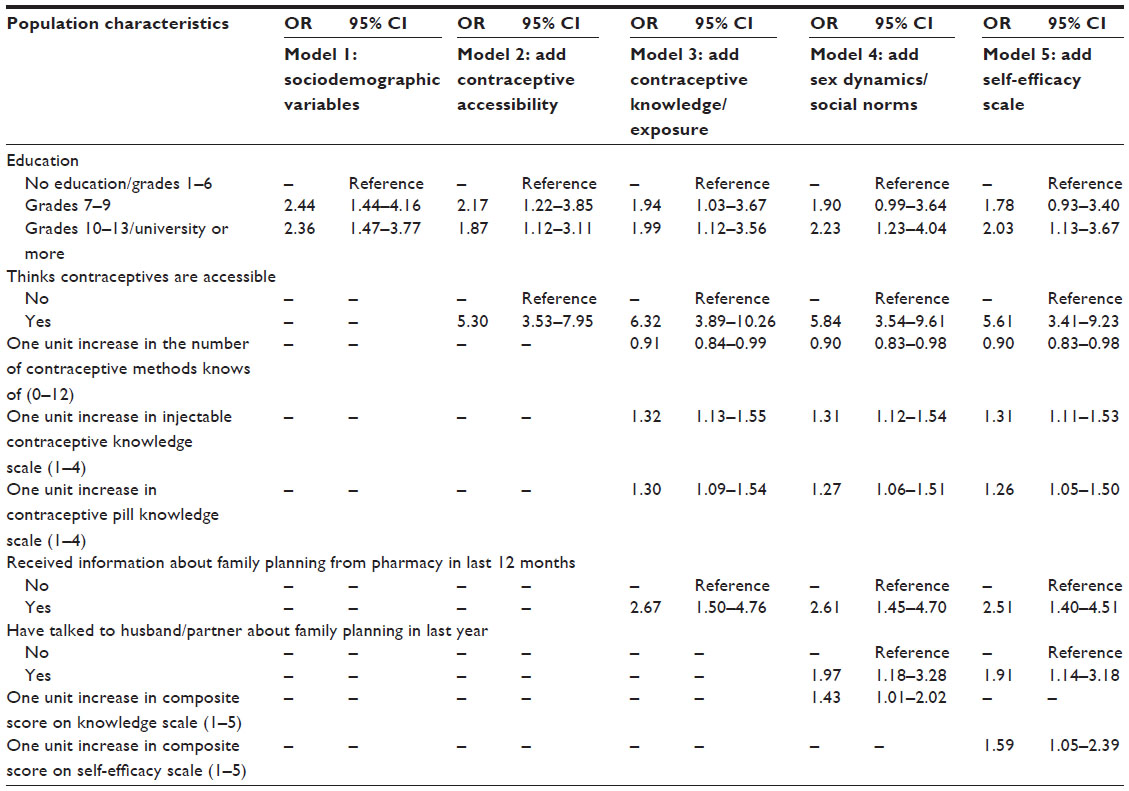 | Table 3 Model building for factors significantly associated with current modern contraceptive use among women aged 25–49 years in Luanda, Angola* |
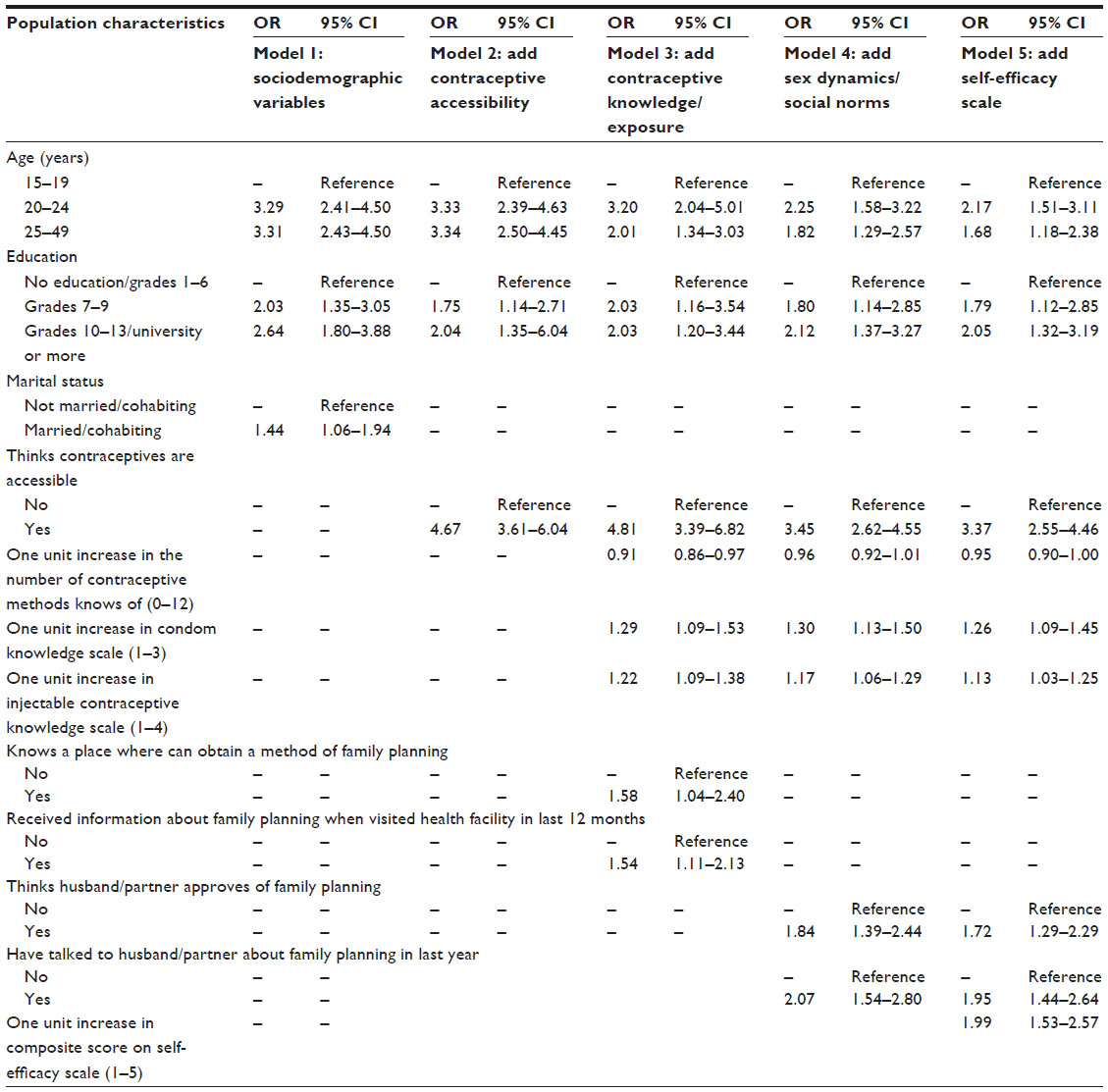 | Table 4 Model building for factors significantly associated with current modern contraceptive use among all women of reproductive age in Luanda, Angola* |
Discussion
In this study, we analyzed the factors associated with contraceptive use among women of reproductive age in Luanda, Angola, comparing findings among young women (aged 15–24 years) and older women (aged 25–49 years). The factors that were associated with current contraceptive use among all women were not unusual; education, perceived accessibility, and contraceptive knowledge were significant predictors in many studies of contraceptive use in other studies from the region.6–8,23,24 Condom knowledge was the only method to have a positive impact on contraceptive use among young women. This may suggest the importance of condoms as the preferred method and/or mostly used form of contraception among young women. However, ~40% of young women could only name up to three contraceptive methods. The same percentage of young women could not get any questions correct surrounding knowledge of injectable and oral contraceptives. This indicates that information, education, and communication efforts targeting youth should focus on increasing knowledge of other methods beyond the condom. The limited knowledge of other modern methods besides male condoms could also be a reason why male condoms are the most used contraceptive. Another reason could be that because some of these young women have not started sexual activity, they do not actively seek information. In fact, it is important to note that some (~10%) of the nonusers in the sample reported not being sexually active.
Other factors that came up as important enablers of contraceptive use may require more creativity. For example, social cognitive theory suggests developing self-efficacy is a key part of the process to adopt new health behaviors.25 The findings from this study confirmed previous research that found an association between self-efficacy and contraceptive use among both older and younger women.26–28 At the same time, the role of men in women’s use of contraception in Luanda should also be highlighted. Confirming the literature that highlights the influence of male partners on women’s contraceptive use in low-resource settings,29–32 women of all ages who recently communicated with their husband about family planning had increased odds of current contraceptive use. Suggestions from other researchers that public health promotion efforts seeking to increase contraceptive use include men and target both males and females may apply to the Angolan context.32–34
Meanwhile, for younger women, even the perception that their husband/partner supports family planning had a positive influence on their contraceptive use. Thus, it is not only important to increase young women’s self-efficacy to use contraception but also vital to address barriers to partner communication and approval. We believe that this variable captures partnership dynamics in contraceptive use better then marital status. In this study, most women reported “single” as their civil status, which is likely a result of matching their response to their national identity card that does not recognize cohabitation. This is a limitation of the survey, as women were asked their civil status rather than relationship status, which may have yielded a different response. Based on findings from young female students in Vietnam, Bui et al35 recommended that sexual promotion strategies aimed at young women address the influence of relationships on young women’s self-efficacy to communicate about safe sex given its impact on contraceptive use.35 Tailoring family planning messages for young women through media outlets may be important in Luanda, given that women aged 15–24 years with exposure to media messages on family planning in recent months were twice as likely to be using contraception.
Finally, as efforts are made to expand family planning services in Angola, the private sector should not be overlooked. Findings from women aged 24–49 years indicated the important role pharmacies can play in family planning counseling and services. This finding is supported by evidence from across Sub-Saharan Africa.36,37
Given the cross-sectional nature of data, there are some limitations in interpretation of these results. We created two groups of women of reproductive age to capture factors associated with modern contraceptive use among adolescents and young adults (15–24 years) and other adults (25–49 years). We hypothesized that women aged 25–34 years could differ significantly from those 35 years and older. However, when we conducted the analysis at the end of model building, we found they were very similar. Given that further grouping reduces the sample size of each group, we decided to keep the adult group (25–49 years). However, future studies with larger sample size should assess associations for the 25–34-year-olds as they might be significantly different from women aged 35 years and older. Additionally, some variables may reflect issues of availability and supply, rather than decision-making or other factors that independently affect use of modern methods. In addition, half of the women using modern methods reported condom use, which was the method women knew best, and also the most available and affordable at the time of the survey.
Conclusion
Findings highlight the need for family planning programming and information campaigns to cater services and messages toward specific age groups, for whom differing factors are associated with current modern contraceptive use. Different strategies may be more effective for increasing contraceptive prevalence among different age groups of women in Angola and elsewhere.
Acknowledgments
This secondary analysis was conducted with data collected through the “Ouakula: Integrated Health Social Marketing Program”, a program implemented by PSI Angola and funded by the United States Agency for International Development. Special thanks to Jorge Rivas, Research Director at PSI Angola at the time of data collection, who wrote the study design and Elsa Caveya and Venceslau Pelenda, both research coordinators at PSI Angola, who supervised the fieldwork. The points of view in this study are solely those of the authors and do not necessarily reflect the views of United States Agency for International Development.
Disclosure
The authors report no conflicts of interest in this work.
References
Cates W Jr. Family planning: the essential link to achieving all eight Millennium Development Goals. Contraception. 2010;81(6):460–461. | |
Brown W, Ahmed S, Roche N, Sonneveldt E, Darmstadt GL. Impact of family planning programs in reducing high-risk births due to younger and older maternal age, short birth intervals, and high parity. Semin Perinatol. 2015;39(5):338–344. | |
Cleland J, Bernstein S, Ezeh A, Faundes A, Glasier A, Innis J. Family planning: the unfinished agenda. Lancet. 2006;368(9549):1810–1827. | |
Schwitters A, Lederer P, Zilversmit L, et al. Barriers to health care in rural Mozambique: a rapid ethnographic assessment of planned mobile health clinics for ART. Glob Health Sci Pract. 2015;3(1):109–116. | |
Aremu O. The influence of socioeconomic status on women’s preferences for modern contraceptive providers in Nigeria: a multilevel choice modeling. Patient Prefer Adherence. 2013;7:1213–1220. | |
Emina JB, Chirwa T, Kandala NB. Trend in the use of modern contraception in sub-Saharan Africa: does women’s education matter? Contraception. 2014;90(2):154–161. | |
Ngome E, Odimegwu C. The social context of adolescent women’s use of modern contraceptives in Zimbabwe: a multilevel analysis. Reprod Health. 2014;11:64. | |
Shapiro D, Tambashe BO. The impact of women’s employment and education on contraceptive use and abortion in Kinshasa, Zaire. Stud Fam Plann. 1994;25(2):96–110. | |
Eliason S, Awoonor-Williams JK, Eliason C, Novignon J, Nonvignon J, Aikins M. Determinants of modern family planning use among women of reproductive age in the Nkwanta district of Ghana: a case-control study. Reprod Health. 2014;11(1):65. | |
Tavrow P, Withers M, McMullen K. Age matters: differential impact of service quality on contraceptive uptake among post-abortion clients in Kenya. Cult Health Sex. 2012;14(8):849–862. | |
Bosco AJ, Ndugga P, Mushomi J. Socio-demographic factors associated with contraceptive use among young women in comparison with older women in Uganda. DHS Working Papers. Calverton, MD: ICF International; 2013. | |
Prata N, Weidert K, Sreenivas A. Meeting the need: youth and family planning in sub-Saharan Africa. Contraception. 2013;88(1):83–90. | |
Agadjanian V, Prata N. War, peace, and fertility in Angola. Demography. 2002;39(2):215–231. | |
Avogo W, Agadjanian V. Childbearing in crisis: war, migration and fertility in Angola. J Biosoc Sci. 2008;40(5):725–742. | |
World Health Organization. Trends in Maternal Mortality 1990 to 2010; WHO, UNICEF, UNFPA and The World Bank estimates; 2012. | |
Population Reference Bureau. World Population Data Sheet. 2014. Available from: http://www.prb.org/DataFinder/Geography/Data.aspx?loc=294. Accessed July 7, 2015. | |
Instituto Nacional de Estatistica (INE). População de Angola – Resultados Preliminares do Censo 2014. 2014. Available from: http://www.ine.gov.ao/xportal/xmain?xpid=ine. Accessed July 28, 2015. | |
World Bank. World Development Indicators. 2015. Available from: http://data.worldbank.org/indicator/SP.POP.GROW/countries/AO?display=graph. Accessed July 28, 2015. | |
Cosep Consultoria, Consaude, ICF International. Angola Malaria Indicator Survey 2011. Calverton, MD: Cosep Consultoria, Consaude, and ICF International; 2011. | |
Decker M, Constantine NA. Factors associated with contraceptive use in Angola. Afr J Reprod Health. 2011;15(4):68–77. | |
Report on the Targets of Millennium Development Angola 2010. National Strategic Plan for Reproductive Health. Luanda: Ministry of Planning, República de Angola; 2010. | |
ICF International. Demographic and Health Surveys Methodology – Questionnaires: Household, Woman’s, and Man’s. Calverton, MD: MEASURE DHS Phase III; 2011. | |
Darteh EK, Doku DT. Knowledge and usage of emergency contraceptives among university students in Ghana. J Community Health. Epub 2015 Jun 29. | |
Asiimwe JB, Ndugga P, Mushomi J, Manyenye Ntozi JP. Factors associated with modern contraceptive use among young and older women in Uganda; a comparative analysis. BMC Public Health. 2014;14:926. | |
Bandura A. Health promotion by social cognitive means. Health Educ Behav. 2004;31(2):143–164. | |
Alvarez C, Villarruel AM, Zhou Y, Gallegos E. Predictors of condom use among Mexican adolescents. Res Theory Nurs Pract. 2010; 24(3):187–196. | |
Rijsdijk LE, Bos AE, Lie R, Ruiter RA, Leerlooijer JN, Kok G. Correlates of delayed sexual intercourse and condom use among adolescents in Uganda: a cross-sectional study. BMC Public Health. 2012;12:817. | |
Wagner GJ, Holloway I, Ghosh-Dastidar B, Kityo C, Mugyenyi P. Understanding the influence of depression on self-efficacy, work status and condom use among HIV clients in Uganda. J Psychosom Res. 2011;70(5):440–448. | |
Barker G, Ricardo C, Nascimento M, Olukoya A, Santos C. Questioning gender norms with men to improve health outcomes: evidence of impact. Glob Public Health. 2010;5(5):539–553. | |
Nieves CI, Kaida A, Seage GR, et al. The influence of partnership on contraceptive use among HIV-infected women accessing antiretroviral therapy in rural Uganda. Contraception. 2015;92(2):152–159. | |
Sanusi A, Akinyemi OO, Onoviran OO. Do knowledge and cultural perceptions of modern female contraceptives predict male involvement in Ayete, Nigeria? Afr J Reprod Health. 2014;18(4):105–114. | |
Esber A, Foraker RE, Hemed M, Norris A. Partner approval and intention to use contraception among Zanzibari women presenting for post-abortion care. Contraception. 2014;90(1):23–28. | |
Kassa M, Abajobir AA, Gedefaw M. Level of male involvement and associated factors in family planning services utilization among married men in Debremarkos town, Northwest Ethiopia. BMC Int Health Hum Rights. 2014;14:33. | |
Tao AR, Onono M, Baum S, et al. Providers’ perspectives on male involvement in family planning in the context of a cluster-randomized controlled trial evaluating integrating family planning into HIV care in Nyanza Province, Kenya. AIDS Care. 2015;27(1):31–37. | |
Bui TC, Markham CM, Ross MW, et al. Perceived gender inequality, sexual communication self-efficacy, and sexual behaviour among female undergraduate students in the Mekong Delta of Vietnam. Sex Health. 2012;9(4):314–322. | |
Nguyen H, Snider J, Ravishankar N, Magvanjav O. Assessing public and private sector contributions in reproductive health financing and utilization for six sub-Saharan African countries. Reprod Health Matters. 2011;19(37):62–74. | |
Lebetkin E, Orr T, Dzasi K, et al. Injectable contraceptive sales at licensed chemical seller shops in Ghana: access and reported use in rural and periurban communities. Int Perspect Sex Reprod Health. 2014;40(1):21–27. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.