Back to Journals » International Journal of Women's Health » Volume 18
Validity and Reliability Assessment of the Health Behaviour Inventory (HBI-20) Among Iranian Women
Authors Hosseini SA, Feizi A ![]() , Yaghoubizadeh Vanini F
, Yaghoubizadeh Vanini F
Received 1 November 2025
Accepted for publication 13 February 2026
Published 26 February 2026 Volume 2026:18 578301
DOI https://doi.org/10.2147/IJWH.S578301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Seyedeh Asma Hosseini,1 Awat Feizi,2 Fatemeh Yaghoubizadeh Vanini1
1Department of Psychology, Faculty of Education and Psychology, Alzahra University, Tehran, Iran; 2Department of Biostatistics and Epidemiology, School of Health, Clinical Toxicology Research Center and Pharmaceutical Sciences Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
Correspondence: Awat Feizi, Department of Biostatistics and Epidemiology, School of Health, Clinical Toxicology Research Center and Pharmaceutical Sciences Research Center, Isfahan University of Medical Sciences, Isfahan, Iran, Tel +983137923250, Email [email protected]
Objective: This study aimed to examine the psychometric properties of the Persian version of the Health Behavior Inventory (HBI-20) among Iranian women by investigating its factor structure, internal consistency, test–retest reliability, and criterion validity.
Participants and Methods: A total of 265 Iranian women completed the HBI-20. Construct validity was assessed through both exploratory and confirmatory factor analyses. Internal consistency was measured with Cronbach’s alpha, and test–retest reliability was calculated using intraclass correlation coefficients (ICC) along with their 95% confidence intervals. Criterion validity was further evaluated by correlating the HBI-20 dimensions with corresponding scales from the Health-Promoting Lifestyle Profile II (HPLP II).
Results: Exploratory factor analysis identified a four-factor model consisting of the Diet, Angerand Stress, Proper Use of Health Care Resources and Preventive Self-Care, and Substance Use dimensions, which together accounted for 52.33% of the total variance. Confirmatory factor analysis supported this four-factor model with acceptable indices (CMIN/DF = 2.391; GFI = 0.959; AGFI = 0.920; CFI = 0.934; RMSEA = 0.073). Reliability analyses demonstrated robust internal consistency with Cronbach’s alpha values of 0.704 (Diet), 0.665 (Anger and Stress), 0.793 (Proper Use of Health Care Resources and Preventive Self-Care), and 0.726 (Substance Use), and an overall alpha of 0.902. Test–retest reliability was also strong, with ICC values of 0.840 (95% CI: 0.755– 0.898) for Diet, 0.781 (95% CI: 0.669– 0.858) for Anger and Stress, 0.853 (95% CI: 0.773– 0.906) for Proper Use of Health Care Resources and Preventive Self-Care, and 0.703 (95% CI: 0.561– 0.804) for Substance Use. Additionally, correlation analyses with HPLP II dimensions confirmed the criterion validity.
Conclusions: The Persian HBI-20 is a psychometrically sound, reliable, and valid tool for assessing health behaviors in Iranian women. Its clear dimensions, high internal consistency and test–retest reliability support its use in health and clinical practice.
Keywords: health behaviours, psychometrics, validity, reliability, health behaviors inventory, women
Introduction
Evaluating health-promoting and health-risk behaviors is crucial for understanding how individuals manage their physical and mental well-being. These behaviors, encompassing actions that either enhance health, such as maintaining a balanced diet and managing stress, or compromise it, like substance use or poor self-care, play a pivotal role in disease prevention and health maintenance. Understanding health-promoting and health-risk behaviors is a foundational step in addressing the factors that influence overall well-being.1–5 These behaviors reflect the choices individuals make daily, which can either foster optimal health—such as engaging in regular physical activity, consuming a nutritious diet, and practicing effective stress management—or contribute to adverse outcomes, including poor dietary habits, sedentary lifestyles, or substance use. The interplay between these behaviors significantly impacts the prevention of chronic diseases, the promotion of mental resilience, and the maintenance of social and emotional health. Therefore, systematically evaluating these behaviors provides critical insights into the root causes of health challenges, helping guide targeted interventions and policies aimed at improving public health and individual outcomes.
The development and use of tools and methods for assessing health-promoting and health-risk behaviors are essential for advancing public health initiatives and individual well-being. Reliable assessment tools enable researchers and practitioners to identify patterns in behaviors such as diet, physical activity, stress management, and substance use, which are critical for designing targeted interventions and policies.6,7 Studies have extensively explored the assessment of health-promoting and health-risk behaviors through the development and validation of various tools and questionnaires. For instance, the Health-Promoting Lifestyle Profile (HPLP), developed by Walker et al, evaluates behaviors across six dimensions, including nutrition, physical activity, and stress management, and has been widely validated across diverse populations. The Youth Risk Behavior Surveillance System (YRBSS), created by the CDC, assesses health-risk behaviors among adolescents, such as substance use and unsafe dietary habits, providing critical data for public health policies. Additionally, the General Health Behavior Inventory (GHBI) has been employed to capture a wide range of preventive and risk-reducing behaviors related to physical and mental health. Tools like the Self-Rated Abilities for Health Practices (SRAHP) evaluate individuals’ confidence in maintaining health-promoting practices, including diet and stress management. Furthermore, the European Health Interview Survey (EHIS) incorporates modules addressing health behaviors at a population level, offering a valuable perspective for international comparisons. These tools, alongside others like the Health Behavior Inventory (HBI-20), emphasize the importance of psychometric validation to ensure their reliability and applicability in diverse settings, contributing significantly to the understanding of behavioral patterns and their impact on health outcomes.8–11
The Health Behavior Inventory-20 (HBI-20) is a psychometric tool designed to assess both health-promoting and health-risk behaviors. Developed by Levant, Wimer, and Williams in 2011, the HBI-20 is a revision of the earlier Health Risks Inventory (HRI).12 It consists of 20 Likert-scaled items across five subscales: Diet, Proper Use of Health Care Resources, Anger and Stress Management, Preventive Self-Care, and Substance Use. The inventory was initially validated using a sample of college men, where exploratory factor analysis confirmed its five-factor structure. Evidence for its reliability and concurrent validity was also established.
Subsequent studies have expanded the application of the HBI-20 to diverse populations and contexts. For example, research has explored its relationship with constructs such as masculinity and attitudes toward seeking psychological help, highlighting its utility in understanding gender-specific health behaviors2. Additionally, international adaptations, such as the Chinese validation of the HBI-SF (Short Form), have demonstrated its applicability across cultural contexts, further confirming its psychometric properties.12–14
The HBI-20 has proven to be a valuable tool for identifying patterns in health behaviors, enabling targeted interventions and contributing to the broader understanding of factors influencing physical and mental health outcomes. Its continued use and validation in different populations underscore its importance in health behavior research. The Health Behavior Inventory-20 (HBI-20) has demonstrated its immense value in identifying patterns of health-promoting and health-risk behaviors, playing a pivotal role in designing targeted interventions and advancing the understanding of factors influencing physical and mental health. Its psychometric strengths and adaptability for various populations have made it a cornerstone tool in health behavior research globally.15,16
The necessity for such validated tools stems from the growing recognition that individual behaviors whether they promote health, such as proper nutrition and regular exercise, or pose risks, like substance use and neglect of preventive care have a profound impact on public health outcomes.17 Systematic assessment of these behaviors through standardized instruments like the HBI-20 ensures consistency, accuracy, and actionable insights, supporting healthcare professionals in shaping effective interventions.16
The need for the HBI-20 or similar tools becomes even more pressing in countries such as Iran, where cultural, social, and dietary factors differ significantly from Western contexts where many tools are developed. Local validation and adaptation of the HBI-20 could address these cultural nuances, making it an essential resource for assessing health behaviors in the Iranian population. For instance, the increasing prevalence of chronic conditions such as diabetes and cardiovascular diseases highlights the critical need for reliable instruments to monitor and modify health behaviors at both the individual and community levels.18 Moreover, psychometric innovation through the adaptation and validation of the HBI-20 in Iran would not only enrich its global applicability but also pave the way for the development of localized norms.
This study was conducted with the aim of evaluating the reliability and validity of the Health Behavior Inventory-20 (HBI-20) in the Iranian women adult population. Recognizing the necessity of reliable tools for assessing health-promoting and health-risk behaviors across various regions, this research focuses on the cultural adaptation and psychometric evaluation of the HBI-20 within the context of Iran. The findings of this study are expected to contribute to a better understanding of health-related behavioral patterns in Iranian adults and provide a foundation for designing effective interventions to promote healthier lifestyles.
Methods
Study Design and Participants
This methodological cross-sectional study was conducted between April and June 2023, involving 265 Iranian women aged 18 to 60 years. Participants were recruited from various regions of Iran.
Sample Size Justification
The sample size for this study was determined based on established methodological recommendations for factor analysis. For the Exploratory Factor Analysis (EFA), a minimum of 5–10 participants per questionnaire item is advised. With 20 items in the HBI-20, a sample of 100–200 participants are considered adequate. For the subsequent Confirmatory Factor Analysis (CFA), a similar or larger sample is recommended to ensure stability of the model.19 To robustly meet these requirements and account for potential incomplete responses, we initially invited 300 potential participants. A final sample of 265 respondents provided a ratio of approximately 13 participants per item, which exceeds common thresholds for both EFA and CFA, thereby ensuring sufficient statistical power for the planned analyses.
Sampling and Recruitment
A multistage convenience sampling method was employed. In the first stage, 300 student identification numbers were randomly selected from the central registry of Al-Zahra University. These students were then contacted and served as referral points or recruitment intermediaries. Each student was asked to invite one eligible adult female family member (aged 18–65, residing in different households across Iran) to participate in the study. The invited family members constituted the actual study sample. It is critical to note that the students themselves were not participants in the study; their role was solely to facilitate initial contact with a broader, geographically dispersed female population outside the university setting. Al-Zahra University students come from diverse regions across Iran. All subsequent screening, consent procedures, and data collection were conducted directly with the invited family members. The questionnaires were distributed electronically via social media. An online link to the questionnaires, along with a detailed explanation of the study objectives, instructions on completing the survey, and informed consent materials, was prepared on the Porsline platform (link: [https://survey.porsline.ir/n/survey/203178/build/]). Only individuals without any confirmed major psychological or cognitive disorders or life-threatening physical illnesses at the time of recruitment were included in the study. Of the 300 potential participants who were contacted via the student intermediaries, 265 completed and returned the questionnaire, yielding a response rate of 88.3% and these responses were used to evaluate construct validity and criterion validity. Information on the specific demographics of the 35 non-responders was not systematically collected, as the recruitment was anonymous at the initial contact stage to protect privacy. Therefore, a formal comparison between responders and non-responders could not be conducted. However, the high response rate helps mitigate concerns about potential non-response bias influencing the primary findings of this validation study.
Additionally, data from 70 women were utilized for reliability analysis, including assessments of internal consistency and test-retest reliability. All participants received sufficient information regarding the study’s purpose and objectives and provided informed consent. The study protocol was approved by Al-Zahra University, and the research was conducted in full compliance with the ethical standards of the Declaration of Helsinki. The research code for this study was 397289.
Study Instruments and Translational and Cultural Adaptation Procedures
Health Behaviour Inventory-20 (HBI-20)
This is a 20-item self-report tool developed by Levant et al.12 The questionnaire uses a 7-point Likert scale where 1 represents “completely disagree”, 2 “disagree”, 3 “slightly disagree”, 4 “have no opinion”, 5 “slightly agree”, 6 “agree”, and 7 “completely agree”. The original instrument comprises five subscales. Three subscales assess health-promoting behaviors (diet, preventive care, and medical adherence), while two subscales evaluate risky health behaviors (anger, stress, and drug use). In preliminary research, Levant et al (2011) examined the psychometric properties of the HBI-20 using a sample of men. They assessed convergent validity by hypothesizing negative correlations between the HBI-20 and three established measures the Gender Role Conflict Scale (GRCS), the Conformity to Male Norms Inventory (CMNI), and the Male Role Norms Inventory-Revised (MRNI-R) and a positive correlation with the Attitudes Toward Seeking Professional Psychological Help Questionnaire (ATSPPH). The correlations with the GRCS and CMNI were between −0.12 and −0.20, both statistically significant, while the correlation with the MRNI-R was −0.08, which was not significant. Moreover, the HBI-20 showed a significant positive correlation of 0.18 with the ATSPPH, further supporting its convergent validity. Exploratory factor analysis indicated that the five components accounted for 56.03% of the total variance. Internal consistency, assessed by Cronbach’s alpha, was reported as 0.72 for the overall scale, with subscale values ranging from 0.68 to 0.79.12
Translation and Face and Content Validity
This questionnaire was developed by Levant et al. Permission was obtained from the original developer (Levant et al), and the HBI-20 was translated from English into Persian using the forward–backward translation method recommended by Beaton et al.18 In the forward translation stage, two expert translators fluent in both languages independently translated the questionnaire items into Persian. One translator was familiar with the underlying concepts of the questions, while the other was not acquainted with the original instrument. Their translations were then merged into a unified version. Subsequently, two additional translators back-translated this unified Persian version into English to ensure conceptual equivalence with the original. After a careful review by the research team (Feizi et al), necessary modifications were implemented, resulting in the provisional Persian version of the HBI-20. Following the translation, content validity was assessed both qualitatively and quantitatively by a panel of experts consisting of 15 university faculty members, psychologists, and specialists in health behaviors. The items were initially reviewed qualitatively, and then quantitative indices the content validity ratio (CVR) and content validity index (CVI) were calculated. Given that the panel comprised 15 experts, the minimum acceptable CVR for each item was set at 0.59, according to the Lawshe table.20 All items had CVR values ranging from 0.7 to 1, and the overall CVI for the questionnaire was 0.85, thereby confirming its content validity through quantitative analysis. Additionally, face validity was determined through qualitative evaluation. The expert panel confirmed face validity by examining the appropriateness and relevance of the items, eliminating ambiguity and misconceptions, and ensuring that the concepts were easily understood.
Health-Promoting Lifestyle Profile II (HPLP II)
The Health-Promoting Lifestyle Profile (HPLP) questionnaire was developed by Walker et al (1987) to assess health behaviors among adults.8 Later, modifications resulted in the HPLP-II, developed by Walker and Hill-Polerecky (1996), which comprises 52 items across six subscales. Content validity was established through expert review, and construct validity was confirmed via factor analysis supporting the six-factor structure.21 Convergent validity was demonstrated by a significant correlation of 0.67 with a personal lifestyle questionnaire and by a non-significant relationship with social desirability measures. In addition, criterion validity was supported by correlations ranging from 0.269 to 0.491 with perceived health status and quality of life measures. Reliability was evaluated using Cronbach’s alpha (0.943) and a 3-week test-retest method (0.892).21 The questionnaire was subsequently translated into Persian, and its psychometric properties were thoroughly evaluated. For the Persian version, Cronbach’s alpha was reported as 0.82 for the overall instrument and ranged from 0.64 to 0.91 for its subscales. A two-week test-retest analysis confirmed reliability with an intra-class correlation coefficient of 0.9, while subscale correlations ranged from 0.71 to 0.89 (P < 0.001). Factor analysis indicated that the six subscales accounted for 58.25% of the total variance, and the overall reliability for the Persian version was reported as 0.942.22
Psychometric Analysis of the Persian-HBI-20
Validity
The factor structure of the Persian-HBI-20 was first examined using exploratory factor analysis (EFA) on a sample of 265 women. Prior to performing the EFA, data suitability was confirmed using the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy (values > 0.7) and Bartlett’s test of sphericity (P < 0.05).23 A principal component extraction approach with orthogonal Varimax rotation was employed to facilitate interpretability. The number of factors was determined based on eigenvalues greater than 1 and inspection of the scree plot, and items with loadings above 0.40 were retained and assigned to factors based on their predominant content. Subscale scores were computed by summing the scores of the corresponding items weighted by their respective loadings.
In addition, confirmatory factor analysis (CFA) was conducted to verify the factor structure obtained from the EFA. The adequacy of the model was evaluated using a range of fit indices including the chi-square-to-degrees of freedom ratio, Goodness-of-Fit Index (GFI), Adjusted Goodness-of-Fit Index (AGFI), Comparative Fit Index (CFI), and Root Mean Square Error of Approximation (RMSEA). All indices indicated acceptable model fit (eg, chi-square/df ratio below 3, GFI and AGFI values above 0.90, CFI exceeding 0.90, and RMSEA below 0.08), thereby supporting the construct validity of the Persian-HBI-20.24
Known-Groups Validity
Known-groups validity was assessed based on the Persian- HBI-20 ability to discriminate between less and high educated women (Participants were categorized into two groups based on their level of education: (1) “Lower education level”, which included women with an associate degree, a high school diploma (12 years of formal education), or less, and (2) “Higher education level”, comprising individuals with a bachelor’s degree, master’s degree, or doctorate.) in terms of sum of score of total scale and its subscales. We hypothesized that there would be a significant difference in terms of mean scores between women with high and less educational attainment. Accordingly, the known-groups validity of the measure is supported if mean scores of Persian HBI-20 are significantly different between considered groups. We tested difference in mean score of total scale and each sub-scale between women educational attainment groups using independent samples t-test.
Criterion Validity
Criterion validity was evaluated using Spearman correlation coefficients between the score of total scale score of Persian-HBI-20 and its sub-scale and Health-Promoting Lifestyle Profile II (HPLP II). We hypothesized that there are positive correlations between total score of HBI-20 and its subscale with positive nature with total score of (HPLP II) and its subscales while negative correlation between drug use subscale of HBI-20 with (HPLP II) total scores and scores of its subscales.
Reliability
To investigate internal consistency and test-retest reliability of Persian-HBI-20, 70 women were as pilot sample recruited, also internal consistency was evaluated on total sample. Participants were asked to complete the Persian-HBI-20 at two separate days with an interval of 7–10 days. To evaluate test–retest reliability, the ICC coefficient with 95% confidence using two-way mixed model, was estimated. We considered the ICC more than 0.70 as excellent reliability.25 We also used Cronbach’s α coefficient in order to evaluate internal consistency with considering the values more than 0.6 as satisfactory.26 The ceiling and floor effects were assessed for all dimensions and the total score of the Persian-HBI-20 by analysing the distribution of responses. Specifically, the percentage of participants who obtained the highest and lowest possible scores was calculated to determine whether a significant proportion of respondents clustered at the extremes, which could indicate potential limitations in the scale’s sensitivity.
Other Measurements and Statistical Analysis
In this paper, quantitative and qualitative variables were expressed as mean (Standard Deviation: SD) and number (precent), respectively. All analyses were conducted using SPSS and Amos software (version 16; SPSS Inc., Chicago, IL, USA).
Results
Sample Description
In a sample of 265 Iranian women, the mean age was 24.89 years (SD = 9.01; range: 18–60). Regarding educational attainment, 45.3% held a Bachelor’s degree, 34.0% had a high school diploma, 10.6% possessed a Master’s degree, 4.9% had education levels below high school, 3.0% held an Associate degree, and 2.3% attained a Doctorate. In terms of marital status, 73.2% were single, 25.3% were married, and 0.4% were divorced. Employment status varied, with 59.6% being unemployed/or student, 14.7% self-employed, 13.6% housewives, 5.7% working in governmental positions, 0.8% retirees, and 1.5% engaged in volunteer work. Among the married women, the average number of children was 1.54 (SD = 1.06; range: 0–4).
Validity and Reliability Analyses Results
Construct Validity
Construct validity of the HBI-20 questionnaire was evaluated using exploratory factor analysis (EFA). The original version of the questionnaire consisted of five dimensions: Diet (D), Anger and Stress (A.S), Substance Use (S), Proper Use of Health Care Resources and Preventive Self-Care (H.C.U.P).
Table 1 presents the results of exploratory factor analysis on our sample that revealed a clear four-factor structure, accounting for a total of 52.33% of the variance. The first factor, termed Diet (D), included items 1 to 5 and explained 12.39% of the variance. The second factor, labeled Anger and Stress (A.S), comprised items 6, 7, and 8 and accounted for 9.97% of the variance. The third factor, termed Proper Use of Health Care Resources and Preventive Self-Care (H.C.U.P), merged the items originally associated with Proper Use of Health Care Resources and Preventive Self-Care into a single composite factor. This factor included items 9 to 17 and explained 17.02% of the variance. Finally, the fourth factor, labeled Substance Use (S), included items 18, 19, and 20 and accounted for 12.93% of the variance.
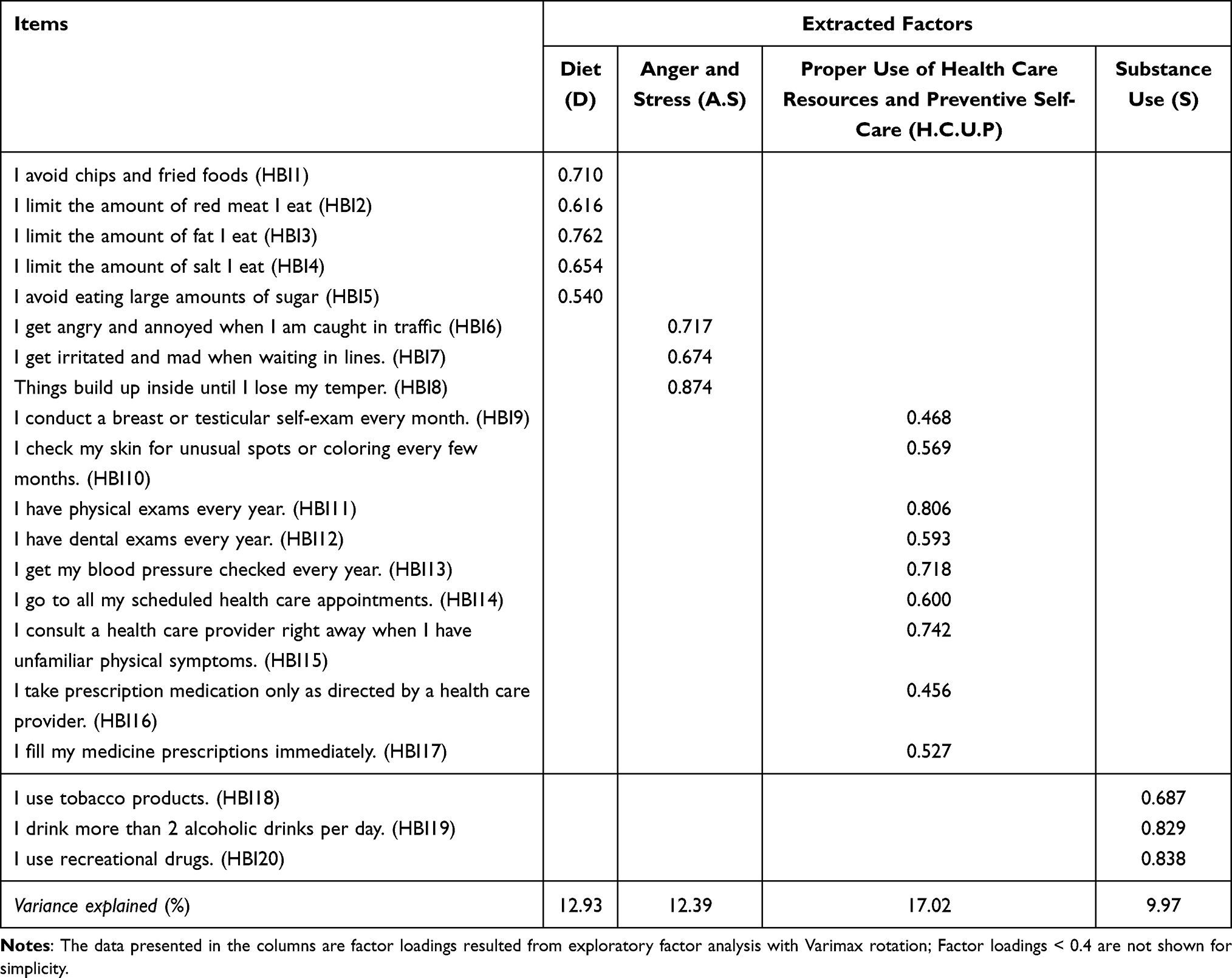 |
Table 1 Exploratory Factor Analysis Results: Factor Loadings of Items on the Extracted Factors for the Persian HBI-20 |
Additionally, the KMO statistic was 0.77, and Bartlett’s test was significant (P< 0.001), confirming the adequacy of the sample size and the factorability of the data. Table 1 provides the factor loadings for the four extracted factors of the HBI-20 questionnaire, demonstrating acceptable factor loadings for all items. This analysis underscores the natural grouping of items into four coherent dimensions, offering enhanced interpretability and practical insights (Table 1).
Results of Confirmatory Factor Analysis (CFA)
The confirmatory factor analysis (CFA) represented in Figure 1 and fit indices in Table 2, supported the four-factor structure identified in the exploratory factor analysis (EFA) with acceptable model fit indices. The chi-square statistic (CMIN = 394.548, DF = 165, p < 0.001) and the ratio of chi-square to degrees of freedom (CMIN/DF = 2.391) indicate a reasonably good fit to the data. As summarized in Table 2, the Root Mean Square Residual (RMR = 0.232) and the Goodness-of-Fit Index (GFI = 0.959) demonstrated strong fit, while the Adjusted Goodness-of-Fit Index (AGFI = 0.920) and Parsimony Goodness-of-Fit Index (PGFI = 0.775) reflected appropriate adjustment for model complexity. Baseline comparison indices, including the Normed Fit Index (NFI = 0.849), Incremental Fit Index (IFI = 0.937), Comparative Fit Index (CFI = 0.934), and Tucker-Lewis Index (TLI = 0.909), were all within acceptable ranges, further confirming the adequacy of the model. Additionally, the Root Mean Square Error of Approximation (RMSEA = 0.073; 90% CI: 0.063–0.082) underscores the model’s robustness, with details presented in Table 2 for clarity. These results confirm the validity of the four factors: Diet (D), Anger and Stress (A.S), Proper Use of Health Care Resources and Preventive Self-Care (H.C.U.P), and Substance Use (S). The model demonstrated that all items loaded well onto their respective factors, supporting the structural coherence and practical applicability of the model in assessing the dimensions of the HBI-20 questionnaire (Table 2).
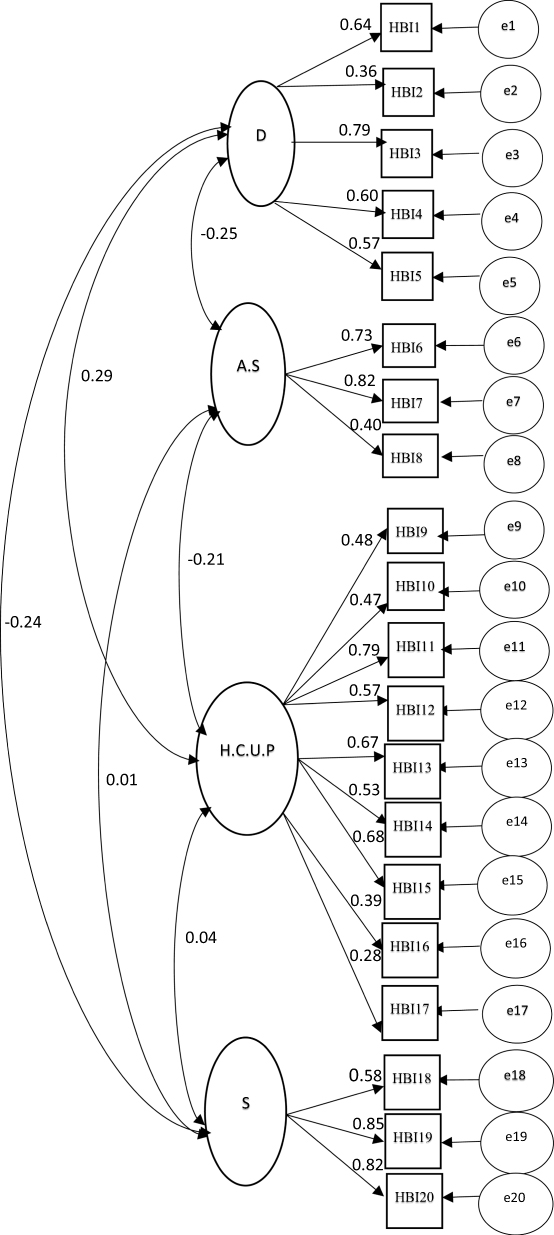 |
Figure 1 Confirmatory Factor Analysis Path Diagram for the Four-Factor Structure of HBI-20 Questionnaire. |
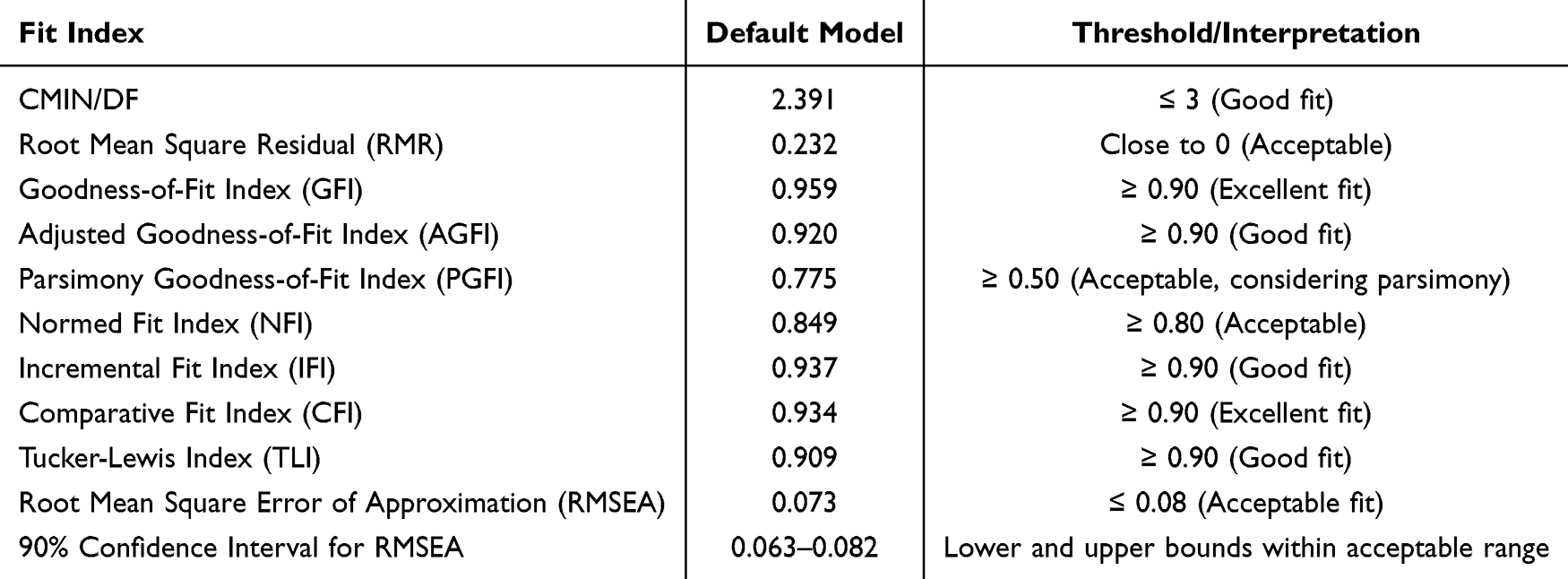 |
Table 2 Summary of Model Fit Indices for Confirmatory Factor Analysis |
Criterion Validity
We assessed the criterion validity of the HBI-20 questionnaire by analyzing the correlation of its dimensions and total score with the corresponding dimensions and total score of the Health-Promoting Lifestyle Profile II (HPLP II) questionnaire. The results, presented in Table 3, revealed significant positive and negative correlations that support the distinction between these constructs while acknowledging relevant conceptual associations. Specifically, the Diet dimension of the HBI-20 exhibited moderate positive correlations, particularly with Health Responsibility (0.526) and Total Health-Promoting Lifestyle (0.554), indicating alignment with responsible health behaviors while maintaining construct separation. In contrast, the Anger and Stress dimension demonstrated significant negative correlations across the HPLP II dimensions, such as Spiritual Growth (−0.360) and Interpersonal Relations (−0.261), reinforcing the expected inverse relationship between psychological distress and health-promoting practices. Moreover, the Proper Use of Health Care Resources and Preventive Self-Care dimension displayed moderate positive correlations with several HPLP II dimensions, highlighting its conceptual relevance to personal health responsibility. Meanwhile, the Substance Use dimension exhibited mostly negative or weak correlations, including with Nutrition (−0.137) and Spiritual Growth (−0.156), further supporting its distinct nature. These findings indicate that the HBI-20 effectively differentiates health-related constructs while maintaining the expected associations, thereby demonstrating strong divergent validity. Further validation through confirmatory factor analysis or discriminant validity tests could provide additional insights into these relationships (Table 3).
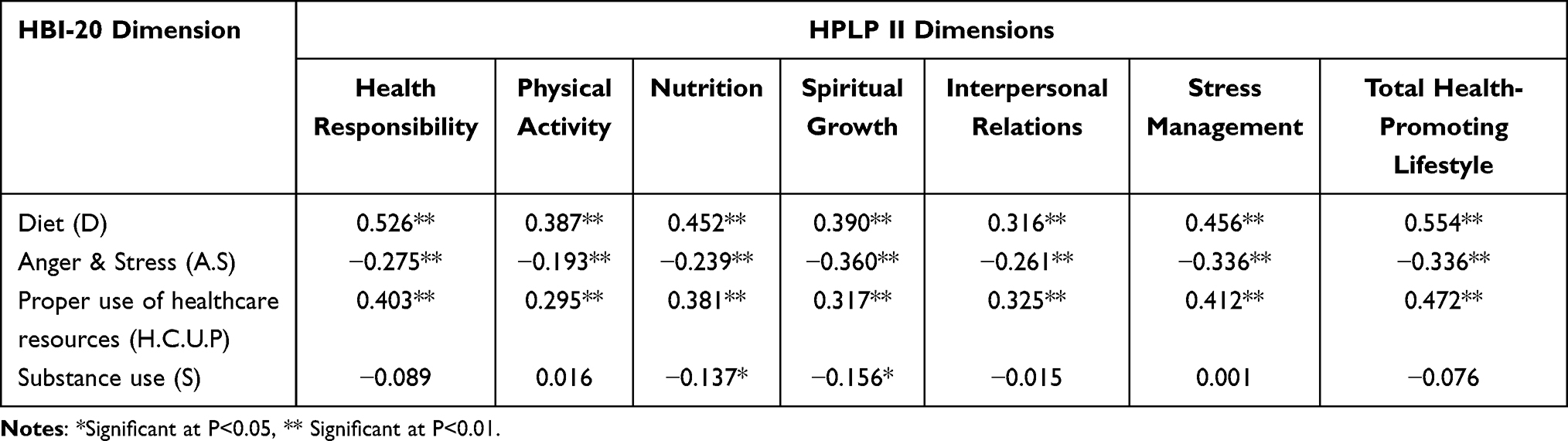 |
Table 3 Assessment of Criterion Validity: Correlation Between HBI-20 and HPLP II Dimensions |
Reliability Analysis Results
We examined the reliability and response distribution characteristics of the HBI‐20 questionnaire as provided in the Table 4. In this analysis, each dimension’s descriptive data (mean ± SD), internal consistency (Cronbach’s α for both full and pilot samples), test–retest reliability (ICC with 95% CI), and extreme response percentages (floor and ceiling effects) were evaluated. The Diet (D) dimension (Items 1–5) demonstrated moderate score variability with a mean of 22.91 ± 6.17, acceptable internal consistency (α = 0.704/0.737), and good stability (ICC = 0.840), coupled with a relatively low floor effect (7.6%) and a moderate ceiling effect (24.2%). The Anger and Stress (A.S) dimension (Items 6–8) had a mean of 11.63 ± 4.03 with slightly lower internal consistency (α ≈ 0.665/0.644) and an ICC of 0.781, while displaying 13.1% floor and 20.0% ceiling effects. Meanwhile, the Proper use of Health Care Resources & Preventive Self-Care (H.C.U.P) dimension (Items 9–17) yielded a mean of 44.11 ± 8.66, robust reliability indices (α = 0.793/0.750; ICC = 0.853), and exhibited a modest floor effect (10.3%) in contrast to a fairly marked ceiling effect (29.2%). In contrast, the Substance Use (S) dimension (Items 18–20) showed a mean of 4.62 ± 3.04, acceptable reliability (α = 0.726/0.763; ICC = 0.703), but a very high floor effect (79.1%) and minimal ceiling effect (4.0%), indicating that the majority of respondents reported very low substance use. Overall, the total score (all 20 items, mean = 83.13 ± 10.96) demonstrated excellent internal consistency (α = 0.902/0.904) and good stability (ICC = 0.819), with floor and ceiling effects of 20.4% and 22.8%, respectively. These results indicate that while some dimensions (especially Substance Use) have skewed response patterns, the overall HBI‐20 questionnaire shows acceptable reliability and reasonably balanced extreme response distributions (Table 4).
 |
Table 4 Descriptive Statistics, Internal Consistency, Test–Retest Reliability, and Floor/Ceiling Effects of the HBI‐20 Questionnaire Dimensions |
Known-Group Validity Results
We examined the mean scores of the HBI-20 dimensions by educational attainment to assess known-groups validity. Results are presented in Table 5. Participants were categorized into two groups based on their level of education: (1) “Lower education level”, which included women with an associate degree, a high school diploma (12 years of formal education), or less, and (2) “Higher education level”, comprising individuals with a bachelor’s degree, master’s degree, or doctorate. Although there were small differences between the higher and lower education groups, none reached statistical significance. For example, the Diet dimension score was slightly lower in the higher education group compared to the lower education group (21.73 vs 22.94, P = 0.116), while the Anger and Stress dimension showed a trend toward higher scores in the higher education group (11.88 vs 10.86, P = 0.062). The Substance Use, Healthcare & Preventive Self Care, and total score were nearly identical between groups, with p values well above 0.05. Overall, these results suggest that the HBI-20 scores are not significantly associated with education level in our sample, indicating that the instrument functions similarly across these educational groups (Table 5).
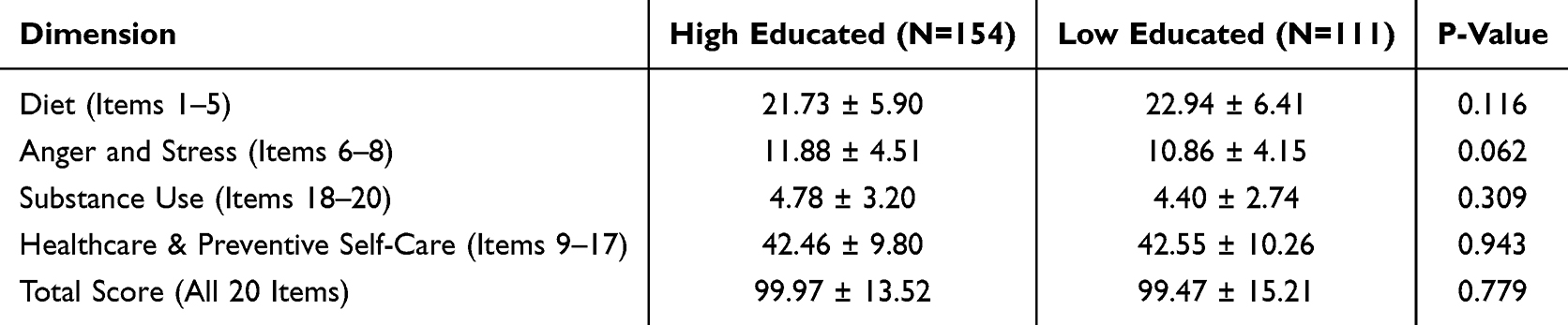 |
Table 5 Comparison of HBI-20 Dimensional Scores by Education Level (BSc-PHD vs Less Than BSc) |
Discussion
In the present study, we validated the Persian version of the Health Behavior Inventory (HBI-20) in a sample of 265 Iranian women. Using exploratory and confirmatory factor analyses, we derived a coherent four-factor structure that includes the domains of Diet; Anger and Stress; Proper Use of Health Care Resources and Preventive Self-Care; and Substance Use. Although the original HBI-20 was conceptualized as a five-dimensional instrument, our analysis suggested that items originally intended to capture “Proper Use of Health Care Resources” and “Preventive Self-Care” clustered together. Similar deviations from the theoretically proposed factor count have been reported in other cross-cultural adaptations. For example, Levant et al12 in their evaluation of the HBI-20 among college men noted variations that appeared to be influenced by cultural and demographic contexts, while Tong et al observed analogous structural adjustments in a Chinese validation study.15 Such findings indicate that the dimensionality of health behavior instruments may vary with cultural nuances and that a merged factor in our study could reflect the integrated way in which Iranian women conceptualize proactive health management.
Our reliability analyses demonstrated excellent internal consistency and test–retest stability across the subscales and the overall score. The Cronbach’s alpha and intraclass correlation coefficients in our sample compared favorably with results reported in previous studies, which underscores the robustness of the Persian HBI-20 as a measure of health behaviors.12,15,17
A particularly notable issue was the presence of a pronounced floor effect in the Substance Use domain. In the context of Iranian society, behaviors perceived as risky or taboo such as substance use are strongly discouraged socially and culturally. Consequently, respondents overwhelmingly selected the “never” option for these items, leading to restricted variability. Such ceiling and floor effects have been documented in other studies examining socially sensitive constructs. Liu and Wang found that items assessing behaviors subject to cultural taboos often yield minimal variance, suggesting that extreme response patterns may be more a reflection of social desirability biases and cultural constraints than a failure of the instrument per se.27,28 Additionally, Aminian et al encountered similar issues when adapting psychosocial questionnaires in Iran, indicating that such effects are common when sensitive behaviors are measured in conservative contexts.17 These response patterns, therefore, should be interpreted as indicative of the underlying cultural milieu rather than as a flaw within the HBI-20. However, the process of instrument validation also brought to light challenges that warrant further discussion, particularly regarding ceiling and floor effects and the absence of significant differences based on educational attainment. In future research, supplementing quantitative measures with qualitative approaches might yield deeper insights into these taboo behaviors and help refine item sensitivity.
Another important finding was the lack of a significant association between health behavior scores (both overall and within dimensions) and educational level. At first glance, one might expect that higher education would correlate with healthier behaviors; yet our data did not support this assumption. This phenomenon is not unique to our study. Raghupathi and Raghupathi have shown that while education is an important determinant of health, its impact is often intertwined with other socioeconomic and cultural factors.29 In environments where strong cultural norms and social desirability pressures prevail, such as in Iran, variations in educational attainment may not necessarily translate into significant differences in health behavior reporting. Other factors including religious values, family traditions, and community norms might exert a more powerful influence on behavior than formal education alone further argue that health behaviors emerge from a complex interplay of individual, familial, and societal factors rather than from education independently.30,31 Therefore, the observed invariance in HBI-20 scores across educational levels should not be viewed as a psychometric weakness but rather as reflective of the multifaceted determinants of health behavior in our target population.
Limitations and Future Directions
Despite these encouraging findings, several limitations should be considered. First, the study employed a multistage convenience sampling method, where participants were recruited through referrals from a university student registry. While this approach provided access to a geographically dispersed national sample of Iranian women with only one female member invited per family, and no students included in the final sample the use of a non-probability sampling technique may still affect the generalizability of the findings to the broader female population in Iran. Second, the exclusive focus on Iranian women restricts the applicability of the results to other genders and cultural contexts. Future research would benefit from employing random sampling techniques, such as national household registries, to improve representativeness, and should extend the validation of the HBI-20 to more diverse demographic and cultural groups. Longitudinal research would be valuable to establish predictive validity and to better understand how health behaviors evolve over time in different cultural contexts. Moreover, the extreme response patterns observed in the Substance Use domain suggest that alternative item formulations or response scaling methods might be needed to capture the full range of health behaviors in societies where certain practices are heavily stigmatized.
Conclusions
In summary, our study demonstrates that the Persian version of the HBI-20 is a reliable and valid tool for assessing health behaviors among Iranian women. The four-factor structure—despite deviating from the original five-dimensional model is supported by both exploratory and confirmatory analyses and reflects culturally contextualized understandings of health. The observed ceiling and floor effects, particularly in the Substance Use domain, highlight important cultural influences on self-reporting of sensitive behaviors. Meanwhile, the lack of significant differences in health behavior scores by education underscores the complexity of behavioral determinants, suggesting that factors beyond formal education, such as cultural norms and social influences, play critical roles. Future research should aim to refine the instrument in light of these cultural nuances, incorporate longitudinal designs, and consider mixed-method approaches to better capture the subtleties of health behavior in diverse settings.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study received ethics approval from Al-Zahra University (Ethics Code: 397289), and informed consent was acquired from all participants.
Consent for Publication
As all data collected and presented in this study are entirely anonymous, aggregated, and contain no personally identifiable information, separate consent for publication was not required.
Acknowledgments
We sincerely and wholeheartedly thank all participants for their valuable contributions to this study.
Funding
This study received no financial support from any external source.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. World Health Organization. Health promotion: key concepts [Internet]. Geneva: World Health Organization; 2020 [cited 2025 May 23]. Available from: https://www.who.int/health-topics/health-promotion.
2. Nigg CR, Long BJ. Health Promotion and Disease Prevention: a Comprehensive Approach. In: Health Behavior: Theory, Research, and Practice.
3. Schneider M, McCauley S, Merians A, Lust K. Health-risk and health-promoting behaviors among college students. J Am College Health. 2019;67(6):562–566. doi:10.1080/07448481.2019.1571926
4. Glanz K, Rimer BK, Viswanath K. Health Behavior and Health Education: Theory, Research, and Practice. Jossey-Bass; 2015.
5. Keller C, Siegel J. The role of health-promoting behaviors in the prevention of chronic disease. Am J Lifestyle Med. 2019;13(6):590–601. doi:10.1177/1559827618765055
6. Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot. 1997;12(1):38–48. doi:10.4278/0890-1171-12.1.38
7. Flay BR, Snyder F, Petraitis J. The theory of triadic influence: a new theory of health behavior with implications for preventive interventions. Adv Med Sociol. 1995;4:19–44.
8. Walker SN, Sechrist KR, Pender NJ. The health-promoting lifestyle profile: development and psychometric characteristics. Nurs Res. 1987;36(2):76–81. doi:10.1097/00006199-198703000-00002
9. Kann L, McManus T, Harris WA, et al. Youth risk behavior surveillance—United States, 2019. MMWR Surveill Summ. 2020;69(1):1–83.
10. Schwarzer R, Renner B. Health-specific self-efficacy scales. Health Psychol. 1997;16(2):139–145.
11. Puciato D, Borysiuk Z, Rozpara M. Quality of life and physical activity in an older working-age population. Clin Interv Aging. 2017;12:1627–1634. doi:10.2147/CIA.S144045
12. Levant RF, Wimer DJ, Williams CM. An evaluation of the health behavior inventory-20 (HBI-20). Psychol Men Masc. 2011;12(1):74–83. doi:10.1037/a0021014
13. Levant RF, Richmond KK. Masculinity ideology and health risk behavior in college men. J Am Coll Health. 2007;56(5):441–448.
14. Jiang Y, Wong ML, Zhang X, et al. Validation of the health behavior inventory (Short Form) among Chinese university students. J Health Psychol. 2020;25(3):421–432.
15. Tong LK, Au ML, Zheng MR, Liu YB, Fu GL, Li YY. Health behavior inventory - short form: a Chinese validation study using classical test theory and item response theory. BMC Public Health. 2024;24(1):2281. PMID: 39174965; PMCID: PMC11340048. doi:10.1186/s12889-024-19774-2
16. Levant RF, Wimer DJ, Williams CM. An evaluation of the health behavior inventory-20 (HBI-20) and its relationships to masculinity and attitudes toward seeking psychological help. J Health Psychol. 2011;16(1):26–41.
17. Aminian M, Dianat I, Miri A, Asghari-Jafarabadi M. The Iranian version of the Copenhagen Psychosocial Questionnaire (COPSOQ) for assessment of psychological risk factors at work. Health Promotion Perspect. 2017;7:7–13. doi:10.15171/hpp.2017.03
18. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
19. Streiner DL, Norman GR, Cairney J. Health Measurement Scales: A Practical Guide to Their Development and Use.
20. Romero Jeldres M, Díaz Costa E, Nadim TF. A review of Lawshe’s method for calculating content validity in the social sciences. Front Educ. 2023;8:1271335. doi:10.3389/feduc.2023.1271335
21. Walker SN, Hill-Polerecky DM. Psychometric evaluation of the health-promoting lifestyle profile II. Unpublished manuscript, University of Nebraska Medical Center. 1996.
22. Mohammadi Zeidi I, Pakpour AH, Mohammadi Zeidi B. Psychometric properties of the Persian version of the health-promoting lifestyle profile II. J Res Med Sci. 2011;16(6):751–757.
23. Sharma P, Verma K. Application of KMO and Bartlett’s test in exploratory factor analysis: ensuring sampling adequacy in research. Int J Eng Technol Res Manag. 2025;12(5):28–36.
24. Sathyanarayana S, Mohanasundaram T. Fit indices in structural equation modeling and confirmatory factor analysis: reporting guidelines. Asian J Econ Bus Account. 2024;24(7):561–577. doi:10.9734/ajeba/2024/v24i71430
25. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
26. Taber KS. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Educ. 2018;48(6):1273–1296. doi:10.1007/s11165-016-9602-2
27. Liu Q, Wang X. t-test and ANOVA for data with ceiling and/or floor effects. Behav Res Meth. 2020;53(2):264–277. doi:10.3758/s13428-020-01407-2
28. Liu J, Wang Y, Ja’afar S, Jusoff K, Idris N. Exploring taboo culture: a cross-cultural analysis of taboos in China and Malaysia. Cogent Arts Humanities. 2025;12(1):2442828. doi:10.1080/23311983.2024.2442828
29. Raghupathi V, Raghupathi W. The influence of education on health: an empirical assessment of OECD countries for the period 1995–2015. Arch Public Health. 2020;78:20. doi:10.1186/s13690-020-00402-5
30. Olsen JA, Chen G, Lamu AN. The relative importance of education and health behavior for health and wellbeing. BMC Public Health. 2023;23:16943. doi:10.1186/s12889-023-16943-7
31. Gumà J, Solé-Auró A, Arpino B. Examining social determinants of health: the role of education, household arrangements, and country groups by gender. BMC Public Health. 2019;19(699). doi:10.1186/s12889-019-7054-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.