Back to Journals » Clinical Interventions in Aging » Volume 15
Validation of an Instrument for Assessing Elder Care Needs in Iran
Authors Rashidi K, Jalali A ![]() , Salari N
, Salari N ![]() , Abbasi P
, Abbasi P ![]()
Received 20 December 2019
Accepted for publication 10 February 2020
Published 25 February 2020 Volume 2020:15 Pages 275—283
DOI https://doi.org/10.2147/CIA.S243142
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Kavoos Rashidi,1 Amir Jalali,2 Nader Salari,3 Parvin Abbasi4
1Department of Psychiatric Nursing, Student Research Committee, Kermanshah University of Medical Sciences, Kermanshah, Iran; 2Substance Abuse Prevention Research Center, Research Institute for Health, Kermanshah University of Medical Sciences, Kermanshah, Iran; 3Department of Biostatistics Department, School of Nursing & Midwifery, Kermanshah University of Medical Sciences, Kermanshah, Iran; 4Department of Nursing, School of Nursing and Midwifery, Kermanshah University of Medical Sciences, Kermanshah, Iran
Correspondence: Amir Jalali
Substance Abuse Prevention Research Center, Research Institute for Health, Kermanshah University of Medical Sciences, Kermanshah, Iran
Email [email protected]
Background: The notable growth of the senior citizens population has caused problems and concerns in areas like healthcare, social care, and participation in society. The present paper is aimed at validating a Farsi version of the “International classification of functioning, disability, and health” for assessing elderly care needs in Kermanshah, Iran.
Methods: The original version of the tool was translated into Farsi using forward-backward method. The study group consisted of 301 senior citizens who were selected through cluster sampling. Validity of the tool was examined using Waltz and Basel’s content validity index, face validity, and confirmatory factor analysis. The reliability of the tool was examined using Cronbach’s alpha and internal correlation. Data analyses were performed in SPSS-25 and Amoss-16.
Results: Following confirmatory factor analysis, the number of factors decreased from nine to eight. The R2 index in the above model was estimated equal to 0.99; this indicates that 99% of the dependent variable changes (total score of ICF) are explained by the independent variables (eight items). All the indices were above 0.9, which indicates significance of the model (χ2/DF=2.7, CFI, NFI, GFI, TLI=0.9, REMSEA=0.078, R2=0.99). In addition, using internal correlation, the reliability of the tool obtained was equal to 0.77 for the whole tool and 0.7– 0.87 for the sub-scales.
Conclusion: The Farsi version of ICF had acceptable and applied specifications to assess the care needs of senior citizens and it can be used as a valid tool in different areas of nursing performance and elderly health.
Keywords: validity, reliability, psychometric, elder care needs, Iranian population
Background
Senior citizens are one of the most vulnerable groups in society. They are at more risk of debilitating disorders that attenuate their ability of programming, responding, and asking for help from others.1 A surge in the population of senior citizens who need support is expected by 2050.2 The demographic structure of the world has deeply changed compared with a hundred years ago;3 so the population of senior citizens is growing.4 Currently, more than five million Iranian citizens (7.26%) are in their old age, and it is expected that more than 10% of the population in 20 years will be constituted by the elderly.5 This trend means that an increase in demand for health services is inevitable, which is also a challenge to create new models of controlling age-related diseases and ensure health for senior citizens.6
Studies have shown that people’s need for healthcare services increases with age.2 To improve daily care of the elderly and cut the costs of care, we need to collect data about individual’s needs.7 To guarantee proper distribution and use of services for senior citizen, it is essential to comprehensively assess the needs including physical, mental, and social needs.8 Studies have shown that a person’s care needs vary with their physical, mental, and social status,9,11 and in this context, the growth criteria for physical, psychological, and social development are influential.10 Therefore, a comprehensive and coherent planning for elderly care can be designed and executed through an accurate and appropriate assessment of the care needs of the elderly.7
Over the past 25 years, different tools have been introduced to assess care needs.12 These tools examine different aspects of health such as needs and care. Development of such tools can improve the quality of health services.12,13 There are a limited number of valid and reliable tools to evaluate care needs of the elderly.7 In addition, there is no valid, reliable, and comprehensive tool to assess care needs of the elderly in Iran. The ICF was developed by Ahsberg et al13 in 2015 through three stages, and it contains nine general questions about different fields of activities based on the International standard of performance introduced by the World Health Organization (WHO). The tool fully examines the care needs of senior citizens living with their families or alone. Reliability and validity of the original form of this tool (Introduced by the WHO) have been supported for people with disabilities by Ahsberg et al for the study of elder care needs in Sweden.14 Validity and reliability of the tool for assessing the care needs of the Iranian elderly population are examined here.
Methods
The study was carried out as a methodological study and a psychometric and validation in nature.15 The study population consisted of all senior citizens living in Kermanshah City, Iran who met the inclusion criteria (included: age 60 years and older, lack of psychological and functional problems, willingness to participate in the study, ability to answer questions, and live with family members).
Sample Group Size and Sampling
To examine content validity, 12 faculty board members and experts in the related fields were selected, including one psychiatric nurse, two senior care nurses, three hygiene and fertility education experts, one PhD of health education, and five PhD of nursing. Twenty elderly people were selected through convenience sampling to confirm face validity.
To examine construct validity and for confirmatory factor analysis (CFA), the experts and senior citizens’ opinion were taken into account. The sample size was determined equal to 320 individuals given that there were 37 statements in the tool.16 The participants were selected through cluster method from two urban districts in Kermanshah. For this purpose, Kermanshah City was divided into six districts and two of them were randomly selected. Then, each of the two districts was divided into six sections and two areas were randomly selected and eligible seniors were selected from these sections. The senior citizens visiting local clinics, mosques, and community centers in these two districts were asked to answer the scale through an interview by one of the researchers.
Data Gathering Tool
The ICF was developed by Ahsberg et al13 in three stages. Nine general questions in the scale are designed based on international standards for different fields of activities. The scale consists of 37 statements and measures the care needs of the respondent as stated and perceived by them. At first a general question is asked about each one of the different nine fields of activities. If the answer to each one of these questions is “No” (ie, no problem in this field), the respondents goes to the next question and if it is “Yes” (ie, a problem in this field), the respondent has to answer more questions on this field of activity to clarify the problem. The questions are designed based on Likert’s five-point scale (0=completely, disagree, 1=disagree, 2=not sure, 3= agree, 4=completely disagree). The higher the score the higher the performance of the respondent. Totally, the tool contains 42 items (37 items for assessing elderly care needs and five separate items about social worker and individually addressed) and measures care needs of the elderly in different fields as felt and stated by the respondent. The questionnaire has nine factors as follows: 1. Learning and applying knowledge, 2. General tasks and demand, 3. Communication, 4. Mobility, 5. Self-care, 6. Domestic life, 7. Interpersonal interaction and relationship, 8. Major life areas, and 9. Community, social and civic life.13
Methodology
After making arrangements with the copyright holder of the tool, it was translated based on the translation guideline and cultural adjustment using Wild et al's17 ten steps. Afterwards, psychometric stages were followed.
Two translators did the Farsi translation job and their work results were examined by the research team before being translated back into English by two other translators. The research team also reviewed the second translations and combined them into one questionnaire, which was then sent to the designer of the tool for examination. Based on the designer’s reply, the original tool was translated into Farsi. To obtain the Content Validity Index (CVI) and Content Validity Ratio (CVR) of the translated tool, it was provided to 11 researchers and university instructors (to check the relevance and clarity of the scale items) and CVR, CVI, and Kappa’s coefficient were obtained for each item. Then, the questionnaire was administered to 20 senior citizens living in Kermanshah City with their families with the help of one of the researchers acting as an interviewer (for face validity). Afterwards, alpha coefficient was obtained to determine reliability of the tool. At the final stage, Kermanshah City was divided into six districts and two were selected randomly.
Data Analyses
Confirmatory factor analysis was used after using skewness and kurtosis to ascertain whether the prerequisites for CFA were met. At first, the CFA was performed with nine factors (as an original form of the questionnaire) and factor loads were determined using Varimax rotation. The statements were connected to the factor with highest factor load (0.5<). That is, the correlation coefficient was assumed as the minimum acceptable correlation level between each statement and the extracted factors. The second factor and statement No.3 were removed from the model due to low factor and insignificant load. Finally, confirmatory factor analysis was performed with eight factors and the results were reported. For all the indices mentioned, values higher than 0.8 are considered as acceptable. Thus, the results of this study were confirmed by eight out of the nine factors of the original questionnaire and only the second factor (General tasks and demand) in confirmatory factor analysis was omitted.
Reliability of the tool was examined using internal correlation and stability. To determine reliability and stability, the participants filled in the tool two times with a 2-week interval. Then the obtained scores of the test/re-test were compared using intra-cluster correlation index. Cronbach’s alpha coefficients were used to determine internal correlation of the tool and the sub-scales. After examining construct validity and CFA, Cronbach’s alpha was measured for the nine-factors. In the same way, Cronbach’s alpha was computed for the proposed model. In addition, Spearman correlation was used to measure internal correlation of the statements.
Results
Out of 320 questionnaires, only 301 questionnaires were returned and 19 of them were incomplete (more than 20% of the items were not answered). In total, 301 senior citizens were studied using ICF. Demographics of the participants including gender, age, marital status, job, and the like were examined (Table 1). The mean age of the participants was 72.18±6.8 years and the age range was 63–96 years.
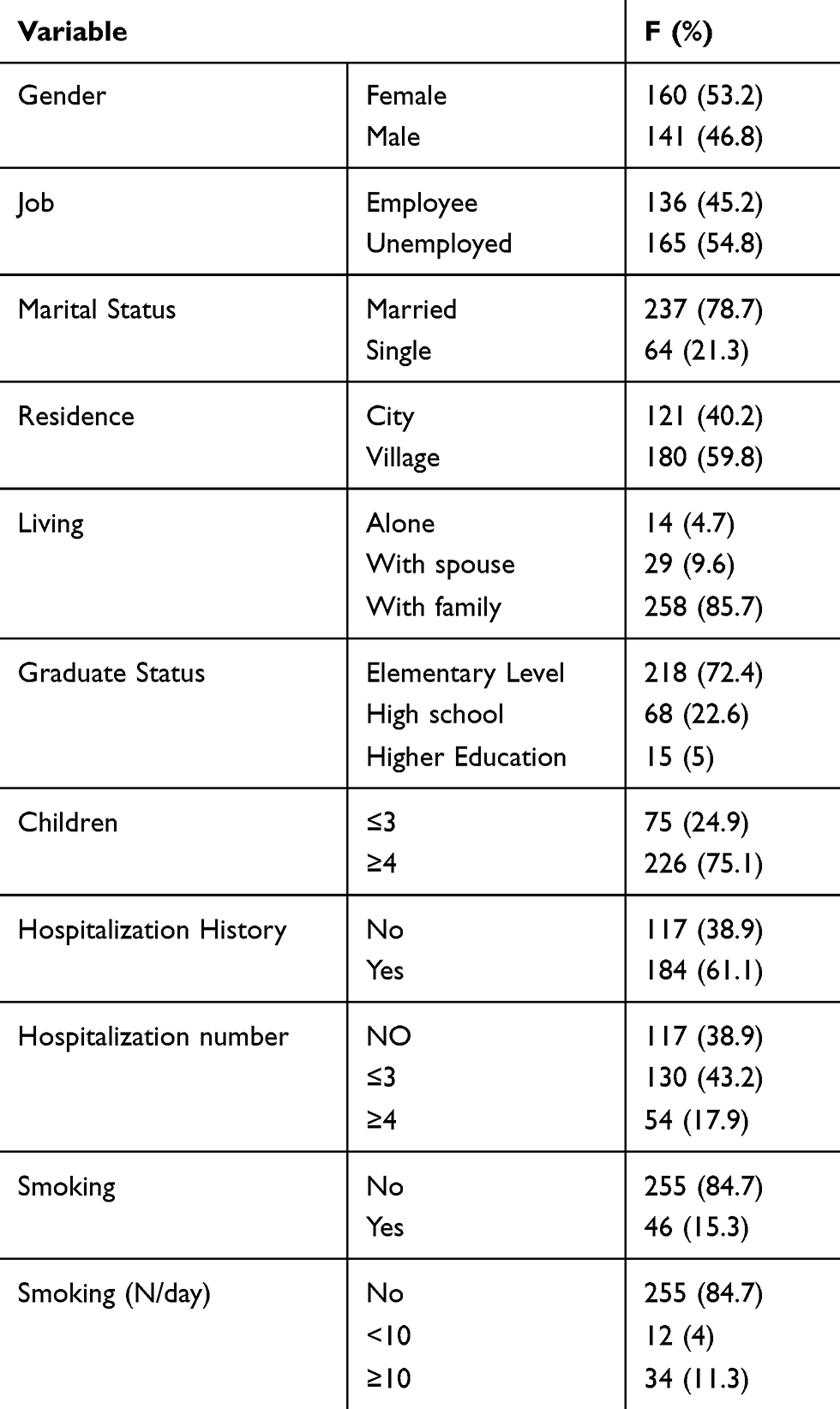 |  |
Table 1 Demographic Characters of Participants in This Study |
Table 2 lists the results of CFA on the care needs of the participants. Mean score of the questions ranges from 0.19–3.1 and the t-value range is −0.002–34.44. Therefore, based on mean score and t-value, the questions were in an acceptable range.
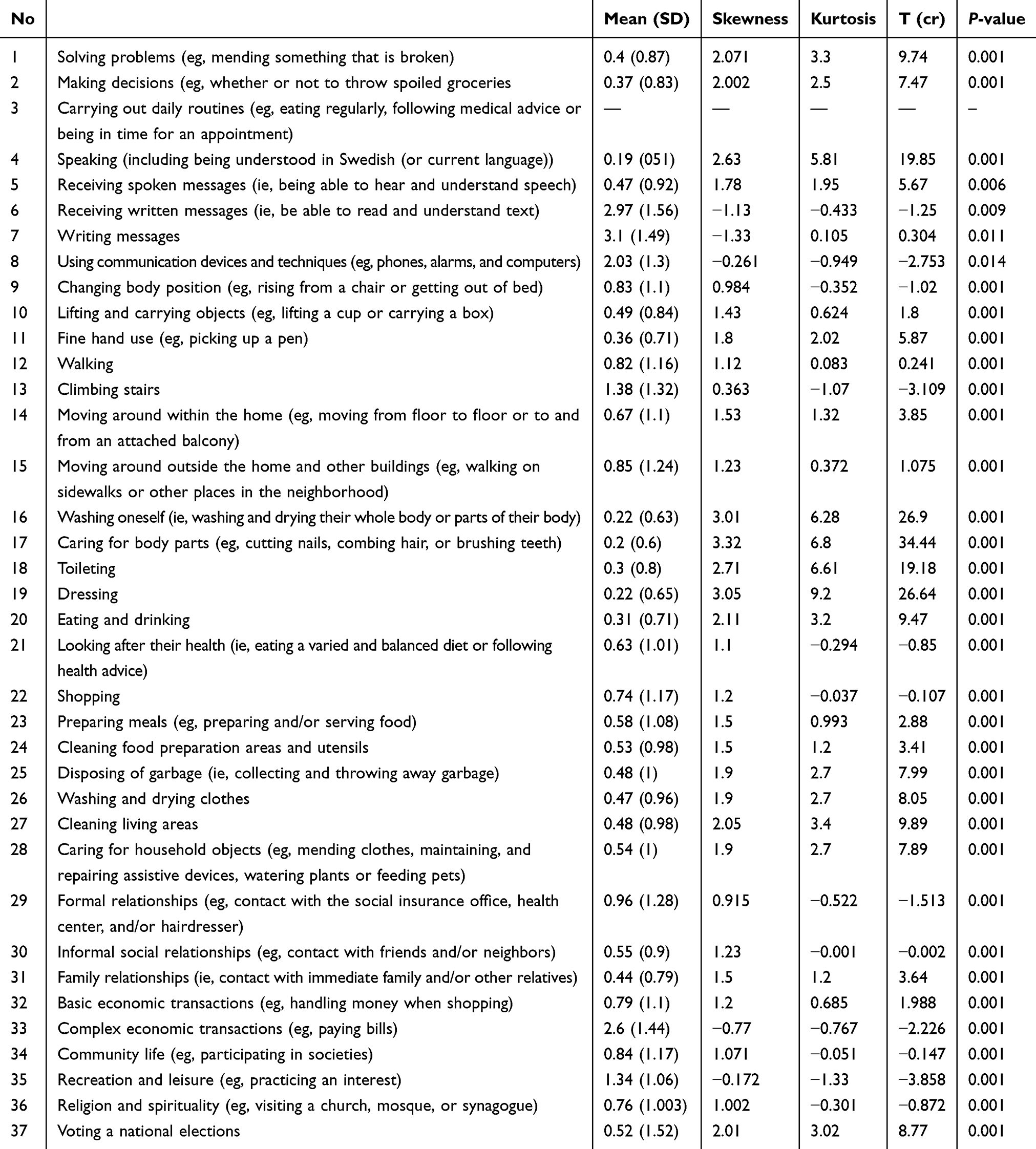 |
Table 2 Results of Confirmative Factor Analysis of ICF |

Skewness value for each statement varied from 0.172–2.7 and it was at a −2–2 range. This means that the statements are normal in terms of skewness with symmetric distribution. Moreover, Kurtosis ranged from −0.001–6.8.
Exploratory factor analysis was used to investigate the construct validity. The results of 0.937 for the Kaiser-Meyer-Olkin measure of sampling adequacy (KMO) and 6,567.35 for Bartlett’s Test of sphericity were significant at the level of P<0.001 indicating suitable data for the exploratory factor analysis. Exploratory factor analysis was performed on subjects’ answers and 37 scale questions (Figure 1). In this study, the Varimax orthogonal rotation method was used. Factors whose percentage value was greater than 1 were also selected and exploratory analysis was performed using Principal Component Analysis (PC). Initial results showed that eight factors or components could be selected for analysis.
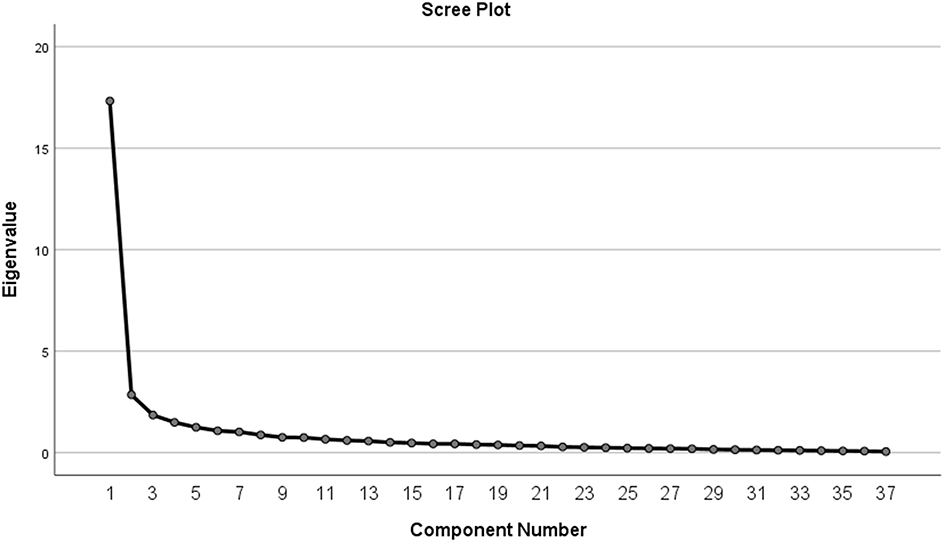 |
Figure 1 Squat chart of extracted components of questionnaire. |
As listed in Table 3, the Chi-square value is 1,421.46, with a degree of freedom (DF) of 567. Chi-square is the most important index of goodness of fit and it can measure the difference between observed and estimated matrices. The index is highly sensitive to sample group size and thus its value is divided by the DF and it is acceptable if the result is less than 5; as it was in this case.
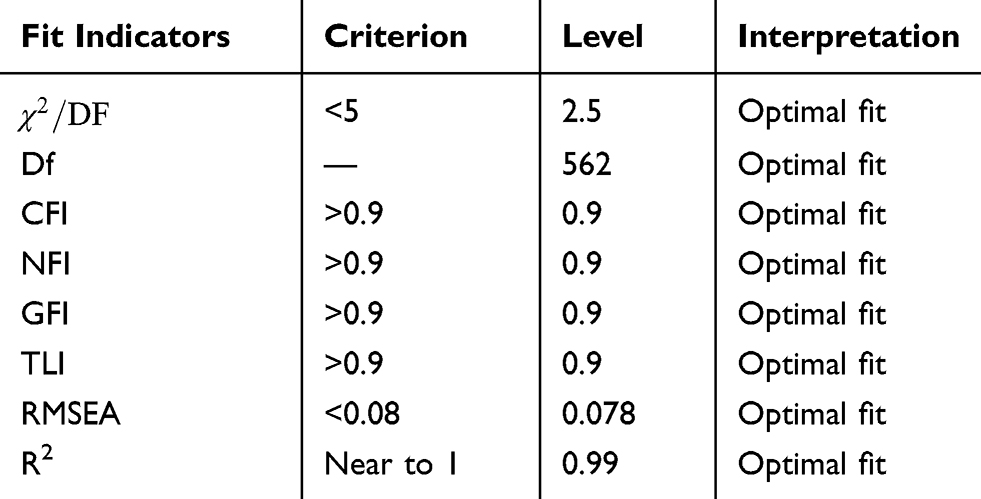 |
Table 3 Fit Indicators Confirmatory Factor Analysis Persian Version of ICF |
Goodness of fit index (GFI) represents acceptable goodness of fit and, here, GFI was equal to 0.9, ie, acceptable goodness of fit.
Root mean square error of approximation (RMESA) was obtained equal to 0.078 (RMESA<0.08: acceptable goodness of fit; and RMESA>0.1: unacceptable goodness of fit). Therefore, at a confidence level of 90% and with upper and lower limits of 0.08 and 0.01, respectively, goodness of fit of the model is confirmed. All of the indices are higher than 0.9, ie, the goodness of fit of the model is confirmed.
Moreover, the R2 index of the model was obtained equal to 0.99, so that 99% of dependent variable variances (total score of the scale) is explained by the independent variables (the eight statements). In other words, 0.99% of variance of the dependent variable is attributed to the independent variables. With R2 between 0 and 1, it is clear that the proposed model explains all variances in the data close to the mean score (Figure 2).
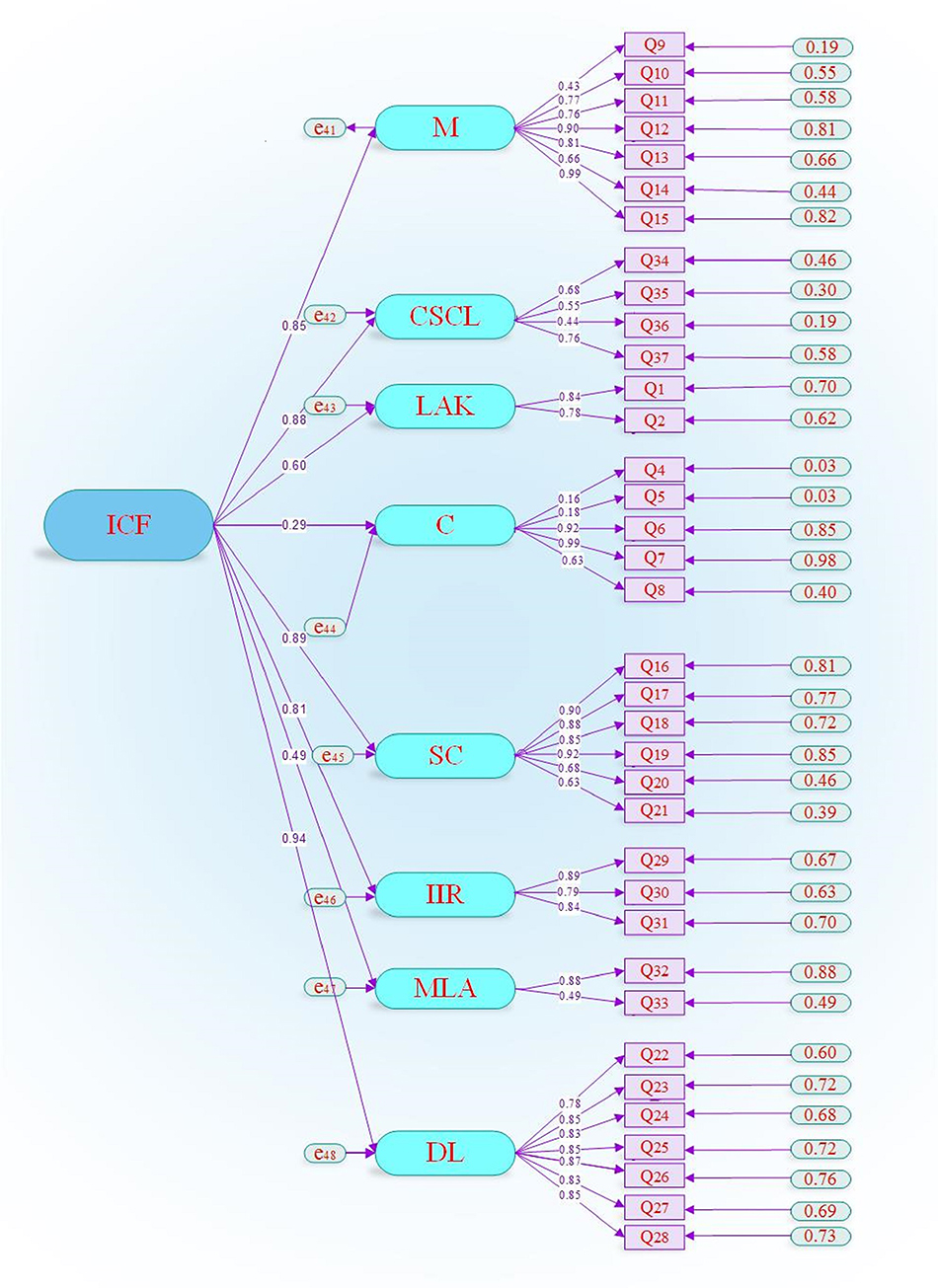 |
Figure 2 Eight factors model of assessing elder care needs and its subscales in Iranian population. |
Given that the normal distribution of the statements was not supported, internal correlation of the statements and the total score of the scale were measured using Spearman correlation coefficient. Table 4 lists the direct and significant correlation of the statements of scale with the total score of the scale. Clearly, the correlation is significant when it is less than 0.05.
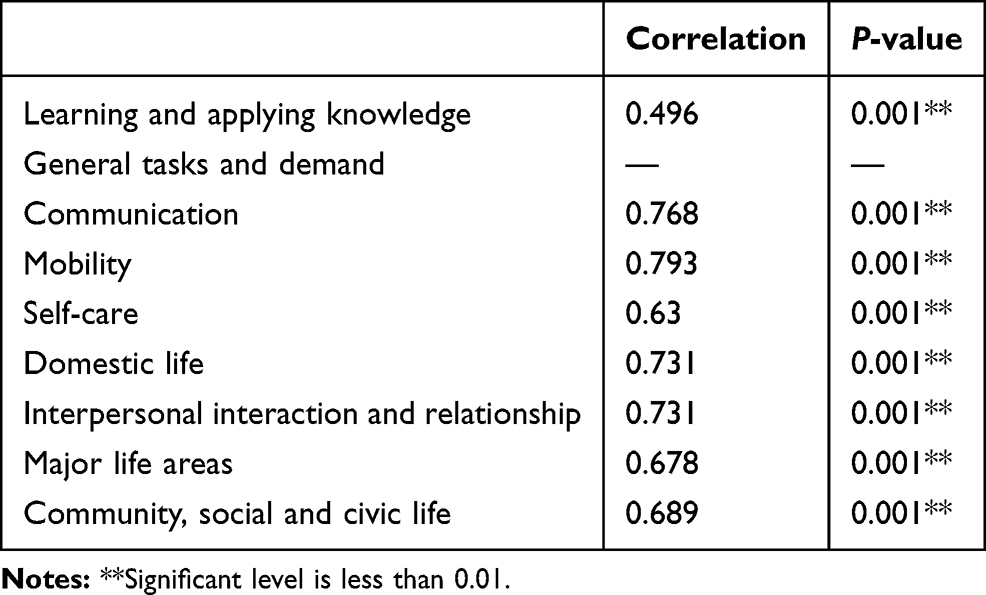 |
Table 4 Reliability Coefficients of Scale of Measurement of ICF and Its Dimensions |
To examine the internal reliability of the scale, Cronbach’s alpha was computed and it was obtained equal to 0.77. As shown by the result, the Farsi version of ICF has an acceptable internal correlation. Cronbach’s value for the sub-scales ranged from 0.7–0.87; therefore, the reliability of the sub-scales was supported (Table 5).
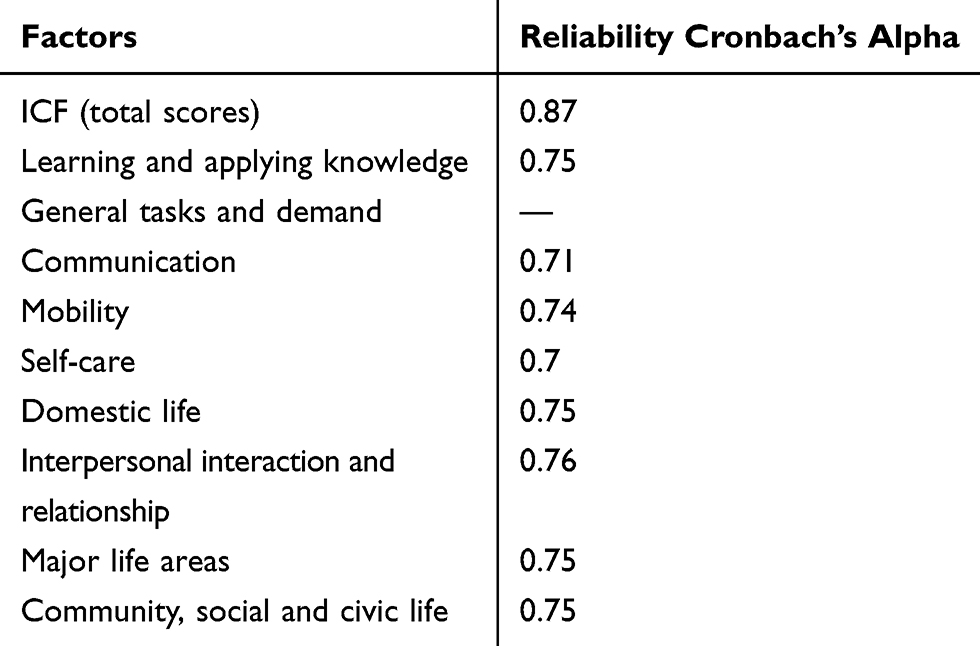 |
Table 5 The Internal Consistency of the Measurement Scale of the Assessing ICF and Its Sub-Scales |
Discussion
Face and Content Validity
In addition to using experts’ opinions about content validity, the elderly’s opinions were also used to determine clarity and understandability of the statements. It is notable that comparing with Ahsberg et al's13 study, there are similarities and differences in terms of the validity of the tool. With regard to face and construct validity, the study consulted 23 social care-givers about assessing elder care needs and all of them confirmed the comprehensiveness of the tool, except for two statements (security and keeping the primary body condition). Similarly, experts and senior citizens in the present study confirmed the face validity of the tool.
Confirmatory Factor Analysis
None of the 37 statements of the tool were removed in the assessment of content and face validity and reliability; while the number of statements and factors decreased to 36 and eight, respectively, through CFA stage. Heravi-Karimooi et al18 Based on construct validity examination, eight factors were confirmed and the internal correlation of the tool was supported.
The RMSEA index was obtained equal to 0.078, therefore the goodness of fit of the model is supported. Other studies reported consistent results so that their finding confirmed acceptability of the RMSEA value. In addition, correlation coefficients of the sub-scales supported acceptable validity of the scale.19,20
Reliability and Internal Consistency of the Tool
The results showed that the Farsi version of ICF has an acceptable internal correlation. Based on Cronbach’s alpha, reliability of the sub-scales was obtained at a 0.7–0.87 range – ie, reliability of the sub-scales is supported. Ahsberg et al13 obtained Cronbach’s alpha at a 0.6–0.8 range and supported structural validity of the tool (P<0.01). Shyu et al21 tried to design and validate a falling self-awareness scale in hospitalized elderly in Taiwan and obtained intra-rater and Cronbach’s alpha reliability at least equal to 70 – ie, acceptable reliability of the scale. Although the number of samples in their study was higher than our subjects, correlation in Cronbach’s alpha value supports the reliability of our tool. A similar study by Rajabi et al22 reported a Cronbach’s alpha of the whole scale equal to 0.95. Their results supported validity and reliability of the Farsi version of ICF to assess care needs and dependency in senior citizens, which is consistent with the present study.
Heravi-Karimooi et al18 used Cronbach’s alpha to support high correlation (0.9, 0.75–0.9) and stability (0.99) of the scale. Our results supported good internal correlation of the scale. Zadworna-Cieślak23 examined “the developmental tasks questionnaire for seniors” using internal correlation and item set correlations. There is a consistency between their results and the results reported here so that they reported that Cronbach’s alpha value for all subscales and the whole scale, for both genders, and the whole participants was acceptable in terms of psychometric. In addition, the range of the majority of correlations of the subscale sets was higher than 0.6. The threshold in the present study for all the mentioned indices is 0.9. Another study consistent with the present paper was by Ahsberg et al,13 which supported reliability and internal correlation (0.60–0.80) and that there was a correlation between the assessment made by social care-givers and senior citizens (72–94%). Both the caregivers and senior citizens found the statement relevant and useful. The psychometric characteristics of the tool confirmed its usefulness for social caregivers to collect information about care needs of senior citizens.11
Since the study was designed to collect information using a scale, it was not possible to examine the authenticity of subjective data provided by the subjects. This is a common issue in descriptive and tool development studies. Issues like impatience and fatigue in the senior citizens are other concerns that might question the accuracy of the answers given the statements. To attenuate these concerns, the author tried to inform the subjects about the necessity and importance of the objectives of study and clarify any ambiguity.
Due to the very limited number of studies on this tool, the psychometric properties of the instrument were investigated. Of course, further studies on this tool are needed to evaluate the clinimetric characteristics24,25 of this lesion and its subscales.
Conclusion
Based on confirmatory factor analysis and internal stability, the results showed that ICF has an acceptable validity for the Iranian senior citizens population. The tool can be used in studies on Iranian senior citizens.
Abbreviations
CVI, Content Validity Index; CVR, Content Validity Ratio; TLI, Tucker-Lewis Index; NFI, Normed Fit Index; GFI, Goodness of Fit Index; CFA, Confirmatory Factor Analysis; RMSEA, Root Mean Square Error of Approximation; KUMS, Kermanshah University of Medical Sciences; ICF, International classification of functioning, disability, and health.
Ethics Approval and Consent to Participate
Written permission was obtained from the designer of the tool. A letter of confirmation was obtained from the Ethics Committee (IR.KUMS.REC.139`7.685), Department of Research and Technology of the university. The study was in accordance with the Declaration of Helsinki. The subjects signed an informed letter of consent and participated voluntarily.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We are grateful to the Deputy for Research and Technology, Kermanshah University of Medical Sciences, for cooperating in this research. We thank all the participants in the study.
Funding
This study was drawn from a research project (No. 97640) sponsored by deputy of research and technology of KUMS. The cost of the payment is spent on the design and implementation of the study.
Disclosure
The authors declare that they have no conflicts of interest regarding this work.
References
1. Pekovic V, Seff L, Rothman M. Planning for and responding to special needs of elders in natural disasters. Generations. 2007;31(4):37–41.
2. Spiers G, Matthews FE, Moffatt S, et al. Impact of social care supply on healthcare utilisation by older adults: a systematic review and meta-analysis. Age Ageing. 2018:afy147–afy147. doi:10.1093/ageing/afy147
3. Sander M, Oxlund B, Jespersen A, et al. The challenges of human population ageing. Age Ageing. 2015;44(2):185–187. doi:10.1093/ageing/afu189
4. Rejeh N, Heravi-Karimooi M, Foroughan M. The needs of hospitalized elderly patients: a qualitative study. Iran J Ageing. 2010;5(1):42–52.
5. Fakhrzadeh H, Sharifi F. Cardiovascular diseases in the elderly. J Gorgan Univ Med Sci. 2012;14(3):1–9.
6. Jiang S, Li P. Current development in elderly comprehensive assessment and research methods. Biomed Res Int. 2016;2016:2016:3528248.DOI. doi:10.1155/2016/3528248
7. Wieczorowska-Tobis K, Talarska D, Kropińska S, et al. The Camberwell Assessment of Need for the Elderly questionnaire as a tool for the assessment of needs in elderly individuals living in long-term care institutions. Arch Gerontol Geriatr. 2016;62:163–168. doi:10.1016/j.archger.2015.10.005
8. Shariat F, Moradi F, Ghahramani R. Study of social, cultural, economic, well-being, and urban structure needs of Tehran seniors association members. Iran J Ageing. 2015;10(3):8–25.
9. Fusar-Poli P. Integrated mental health services for the developmental period (0 to 25 years): a critical review of the evidence. Front Psychiatry. 2019;10:355. doi:10.3389/fpsyt.2019.00355
10. Comer-HaGans D, Weller BE, Story C, Holton J. Developmental stages and estimated prevalence of coexisting mental health and neurodevelopmental conditions and service use in youth with intellectual disabilities, 2011-2012. J Intellect Disabil Res. 2020. doi:10.1111/jir.12708
11. Lynn M. Caring for the youngest students: the ABCs of preschool nursing. NASN Sch Nurse. 2020;1942602x19899703. doi:10.1177/1942602x19899703
12. Deeken JF, Taylor KL, Mangan P, Yabroff KR, Ingham JM. Care for the caregivers: a review of self-report instruments developed to measure the burden, needs, and quality of life of informal caregivers. J Pain Symptom Manage. 2003;26(4):922–953. doi:10.1016/s0885-3924(03)00327-0
13. Åhsberg E, Fahlström G, Rönnbäck E, Granberg A-K, Almborg A-H. Development of an instrument for assessing elder care needs. Res Soc Work Pract. 2015;27(3):291–306. doi:10.1177/1049731515572913
14. Raji P, Hassani Mehraban A, Aliabadi F, Ahmadi M, Schiariti V. Content validity of the comprehensive ICF core set for children with cerebral palsy aged 0-6 years: Iranian occupational therapists perspective. Iran J Child Neurol. 2018;12(3):40–58.
15. LoBiondo-Wood G, Haber J. Nursing Research-E-Book: Methods and Critical Appraisal for Evidence-Based Practice. Elsevier Health Sciences; 2014.
16. Mundfrom DJ, Shaw DG, Ke TL. Minimum sample size recommendations for conducting factor analyses. Int J Test. 2005;5(2):159–168. doi:10.1207/s15327574ijt0502_4
17. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104. doi:10.1111/j.1524-4733.2005.04054.x
18. Heravi-Karimooi M, Anoosheh M, Foroughan M, Sheykhi MT, Hajizadeh E. Designing and Determining psychometric properties of the domestic elder abuse questionnaire. Iran J Ageing. 2010;5(1):0–0.
19. Mahmoudian A, Torabi Chafjiri R, Alipour A, Shamsalinia A, Ghaffari F. The design and evaluation of psychometric properties for a questionnaire on elderly abuse by family caregivers among older adults on hemodialysis. Clin Interv Aging. 2018;13:555–563. doi:10.2147/CIA.S149338
20. Park M, Kim SK, Jeong M, et al. Psychometric validation of the korean version of the camberwell assessment of need for the elderly in individuals with dementia. Asian Nurs Res (Korean Soc Nurs Sci). 2018;12(2):106–112. doi:10.1016/j.anr.2018.04.001
21. Shyu ML, Huang HC, Wu MJ, Chang HJ. Development and validation of the self-awareness of falls in elderly scale among elderly inpatients. Clin Nurs Res. 2018;27(1):105–120. doi:10.1177/1054773817714663
22. Rajabi G, Namadmalan M, Ghasemzadeh R, Foroghan M, Zahednejad S, Dijkstra A. Psychometric properties of the Persian version of care dependency scale in older people nursing home residents. Payesh. 2015;14:193–204.
23. Zadworna-Cieślak M. Psychometric properties of the developmental tasks questionnaire for seniors. Curr Psychol. 2019. doi:10.1007/s12144-019-00380-0
24. Carrozzino D. Clinimetric approach to rating scales for the assessment of apathy in Parkinson’s disease: a systematic review. Prog Neuropsychopharmacol Biol Psychiatry. 2019;94:109641. doi:10.1016/j.pnpbp.2019.109641
25. Fava GA, Carrozzino D, Lindberg L, Tomba E. The clinimetric approach to psychological assessment: a tribute to per bech, MD (1942–2018). Psychother Psychosom. 2018;87(6):321–326. doi:10.1159/000493746
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.