Back to Journals » Risk Management and Healthcare Policy » Volume 15
Vaccine Inequity and Hesitancy: A Vicious Cycle Undermining the Fight Against the COVID-19 Pandemic
Authors Gudina EK ![]() , Mekonnen Z
, Mekonnen Z ![]() , Yilma D
, Yilma D ![]()
Received 29 January 2022
Accepted for publication 21 April 2022
Published 29 April 2022 Volume 2022:15 Pages 865—869
DOI https://doi.org/10.2147/RMHP.S360480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Esayas Kebede Gudina,1 Zeleke Mekonnen,2 Daniel Yilma1
1Department of Internal Medicine, Jimma University Institute of Health, Jimma, Ethiopia; 2School of Medical Laboratory Sciences, Jimma University Institute of Health, Jimma, Ethiopia
Correspondence: Esayas Kebede Gudina, Department of Internal Medicine, Jimma University Institute of Health, P. O.Box 5058, Jimma, Ethiopia, Email [email protected]
Abstract: The world has come a long way in the fight against the COVID-19 pandemic by averting the initially feared humanitarian crisis and by producing effective vaccines in a record time. Paradoxically, more new daily cases are being reported today than when there was not any effective vaccine around. The success against the pandemic so far is dented by inadequate vaccine supply in most low-income countries and widespread vaccine hesitancy. By the end of 2021, only half of WHO Member States have reached the target of immunizing 40% of their populations, while only less than 10% of the population in low-income countries have received at least one dose of the vaccine. This happened while more than nine billion doses of the vaccines were administered globally, predominantly in rich countries. On the backdrop of these man-made factors, the evolution of highly mutated variants of the virus is causing more uncertainties than the pre-vaccine time. If the vaccine inequities and hesitancy are not properly addressed, we are likely to enter into the vicious cycle of inequitable vaccine distribution leading to low vaccination rates in most low-income countries where the majority of the world population resides. This will ultimately enhance sustained transmission of the virus, leading to evolution of new variants of concern. As the highly mutated variants are likely to infect both vaccinated and unvaccinated individuals, it will inevitably lead to major doubts in the effectiveness and acceptance of the vaccines. In this review, we present how this vicious cycle may prolong the pandemic and discuss the importance of concerted global action to tackle it.
Keywords: COVID-19, SARS-CoV-2, variants of concern, vaccine hesitancy, vaccine scepticism, vaccine inequity
Background
While addressing the World Health Organization (WHO) executive board meeting in Geneva on January 18, 2021, Director-General Dr. Tedros Adhanom Ghebreyesus said “The world is on the brink of a catastrophic moral failure – and the price of this failure will be paid with lives and livelihoods in the world’s poorest countries. Vaccine equity is not just a moral imperative, it is a strategic and economic imperative.1” A year on, only half of WHO Member States have reached the target to immunize 40% of their populations by the end of 20212 and only 8.5% of people in low-income countries have received at least one dose of the vaccine, much less than the rate of booster doses received in rich countries.3 In Africa, only 13.7% of the population received at least one dose and only 27% of the health workers were fully vaccinated by the end of 2021.4 The evolution and global spread of immune escape variants and vaccine scepticism against the backdrop of such inequities in vaccine distribution will only prolong the pandemic and global suffering. A concerted global action is thus needed to avert further setbacks.
Vaccine Inequity Dents the Success so Far
Within a year of the initial reported cases of COVID-19, the first dose of the vaccine against SARS-CoV-2, the novel corona virus causing the pandemic, was administered.5 This led to the optimism that the pandemic would soon be under control. A year on, ten COVID-19 vaccines were approved for use by WHO.6 As 2021 came to an end, about 9.15 billion doses have been administered globally and some 58% of the world population have received at least one dose of a COVID-19 vaccine.3 Nonetheless, we received 2022 with more uncertainties and a record number of daily new COVID-19 cases globally. The remarkable success so far is overshadowed by a global vaccine inequity and, to some extent, vaccine hesitancy. As the WHO Director-General remarked on 29 November 2021, more than 80% of the world’s vaccines have gone to G20 countries; low-income countries, Africa in particular, received only 0.6% of all vaccines.7
This has resulted in uncontrolled spread of the virus particularly in countries with low vaccination rates and currently posing a real threat to the emergence of new variants of concerns (VOCs). The discovery in South Africa of a heavily mutated variant, Omicron, in November 2021 has created the assumption that the variant might have originated in unvaccinated people. Ever since, the variant has reached every corner of the world and is currently driving the global wave of the pandemic in all countries, regardless of the vaccination achievements (Figure 1). If humans do not understand fairness, the virus does, proving what has been stated by WHO: “no region, no country, no community and no individual is safe until we are all safe.”7
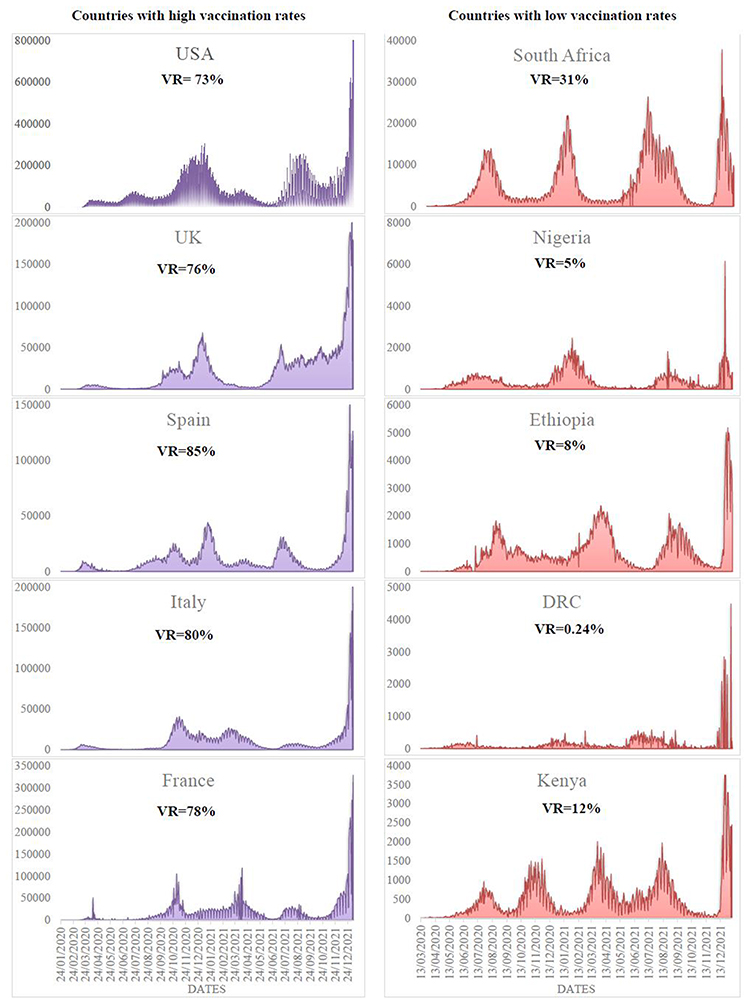 |
Figure 1 Reported daily new case in five countries with high vaccination rate and five countries with low vaccination rates as January 05, 2022. Data sources: Our world in Data (5) and John Hopkins University.8 Abbreviations: DRC, Democratic Republic of Congo; UK, United Kingdom; USA, United States of America; VR, vaccination rate indicating at least one dose of COVID-19 vaccine. |
Vaccine inequities and low vaccination rates are not concerns of the poor countries only, but they are major threats that undermine the global pandemic control efforts. Unless dealt with more proactively, vaccine inequities will result in continuous human sufferings and loss of lives and livelihood. Moreover, it is important to underline that the longer vaccine inequity persists, the more opportunity this virus has to spread and evolve in ways we cannot predict nor prevent, perpetuating the cycle of panic and neglect.
Vaccine Inequity Will Perpetuate the Vicious Cycle of Hesitancy
Vaccine inequities and the resultant low vaccine coverage in low-income countries may lead to the emergence and spread of new VOCs. Because of their highly immune escape behaviour, such variants may spread, as we observed in the case of Omicron, in an almost similar pattern in both poorly vaccinated and highly vaccinated countries. In Figure 1, we tried to compare the patterns of the outbreak in terms of daily new confirmed cases of COVID-19 as reported by John Hopkins Coronavirus Resource Center8 between countries with high vaccination rates and those with low vaccination coverage. In this figure, we present the vaccination rate as a proportion of the population of each country who have received at least one dose of the COVID-19 vaccine as of January 05, 2022 as reported in Our World in Data.3 In the high coverage group, the rate ranged from 73% in the United States of America to 85% in Spain. In the low coverage category, all countries presented in the figure had rates of <10% except South Africa (31%).
In countries with vaccination coverage of >70%, one would logically expect some form of herd immunity9 and hence, a difference in outbreak pattern from countries with low vaccination rates. However, as depicted in Figure 1, countries in both high and low vaccination rates had similar outbreak patterns. This may be an indirect indicator of reduced vaccine effectiveness against the variants causing the current wave. Although vaccinated individuals are less likely to suffer from severe COVID-19, high vaccine breakthrough infection rate will inevitably lead the community to doubt vaccine effectiveness. This may be enough to erode public confidence and may ultimately lead to even more profound vaccine scepticism. Vaccine inequities may thus indirectly contribute to the increase in vaccine refusal despite their availability. Vaccine hesitancy, also referred to as vaccine scepticism, is not a new phenomenon though. There are a number of driving factors for vaccine hesitancy, including perceptions of the effectiveness and safety of the vaccine, trust in health systems, and perceived risk of vaccine-preventable disease.10
Vaccines are still very effective in preventing severe COVID-19 disease and hospitalization in all VOCs, and remain the most important tools in the fight against the pandemic.11 However, the recent dramatic escalation of the outbreak in highly vaccinated communities is creating more uncertainties about the effectiveness and impact of the vaccines. Although scepticism against COVID-19 vaccines started even before their arrival,12 the uncertainties created by vaccine inequality might have already initiated a vicious cycle of vaccine hesitancy (Figure 2) that will create further difficulty in controlling this pandemic. Although infection in vaccinated people may not lead to severe disease and death in most of the cases, it is enough to deepen the profound vaccine hesitancy. With the current trend of vaccination rates and vaccine hesitancy, Omicron may not be the last variant of concern. The world should thus stay vigilant and prepare for most likely future VOCs and wave, even waves, of the outbreak unless this vicious cycle of vaccine inequity-hesitancy is broken by concerted global actions.
 |
Figure 2 Vicious cycle of vaccine inequity and vaccine hesitancy. |
Despite WHO’s relentless appeal for equitable vaccine distribution, the current global action is likely to sustain this cycle of vaccine inequity and hesitancy. This can lead to more uncertainties in the future, not just in poor countries but globally. At the time of this writing, while many countries are still striving to provide the first shot of the vaccine for the most vulnerable, many rich countries have approved third and fourth doses even for the younger population. Daily booster dose vaccination in rich countries is now given at a rate of many folds of that of the first dose in Africa.3 Such actions are likely to perpetuate the vicious cycle and prolong the pandemic and global suffering. This is indicative of the fact that we cannot end this pandemic unless we solve the man-made chain of actions.
We, as humans, have come a long way with our actions and are currently harvesting what we sowed first. The harm has already been done, and it is now an act of damage limitation. We are now at a point where we find it difficult to convince people, particularly in low-income countries, to take the vaccine.13 Improving the vaccine supply alone may not be enough anymore. If we have to correct the mistakes we committed so far, we have to double our efforts to ensure equitable distribution of vaccine and convince the majority of low-income countries to receive the vaccine. Lest, the vicious circle will continue until everybody gets multiple infections of the virus and SARS-CoV-2 becoming a member of the group of globally endemic flu-like infections. That will come at a huge suffering, economic cost, and humanitarian crisis.
In conclusion, COVID-19 vaccines were produced in a record time and within a year, nearly two-thirds of the world population had received at least one dose of the vaccine. This success is dented by inequitable distribution of the vaccines. The uncontrolled spread of the virus in unvaccinated communities, especially in low-income countries, is becoming a risk for the emergence of new SARS-CoV-2 VOCs that affect the whole world at a similar pace regardless of vaccination achievements. Such a pattern may provoke a profound vaccine hesitancy that may further compromise the global effort against the pandemic. Knowing that vaccine equity is not charity, rather it is in every country’s interest, the world now needs proactive actions to improve access to COVID-19 vaccines across all nations, as well as to tackle vaccine hesitancy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO Director-General’s opening remarks at 148th session of the executive board. WHO Director-General; 2021. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-148th-session-of-the-executive-board.
2. World Health Organization. WHO director-general’s opening remarks at the media briefing on COVID-19. WHO Director-General; 2021. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-22-december-2021.
3. Our World in Data. Coronavirus (COVID-19) Vaccinations; 2021. Available from: https://ourworldindata.org/covid-vaccinations.
4. World Health Organization. Only 1 in 4 African health workers fully vaccinated against COVID-19. Africa: World Health Organization; 2021. Available from: https://www.afro.who.int/news/only-1-4-african-health-workers-fully-vaccinated-against-covid-19.
5. Ledford H. Six months of COVID vaccines: what 1.7 billion doses have taught scientists. Nature. 2021;594(7862):164–167. doi:10.1038/d41586-021-01505-x
6. World Health Organization. 10 vaccines approved for use by WHO. World Health Organization; 2021. Available from: https://covid19.trackvaccines.org/agency/who/.
7. World Health Organization. WHO director-general’s opening remarks at the stakeholder engagement event: progress made so far on implementing the partnerships for vaccine manufacturing in Africa. World Health Organiztion; 2021. Available from: https://www.who.int/director-general/speeches/detail/who-director-generals-opening-remarks-progress-made-so-far-on-implementing-the-partnerships-for-vaccine-manufacturing-in-africa.
8. John Hopkins University. COVID-19 dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University; 2021. Available from: https://coronavirus.jhu.edu/map.html.
9. Kwok KO, Lai F, Wei WI, Wong SYS, Tang JWT. Herd immunity - estimating the level required to halt the COVID-19 epidemics in affected countries. J Infect. 2020;80(6):e32–e33. doi:10.1016/j.jinf.2020.03.027
10. MacDonald NE, Hesitancy S. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–4164. doi:10.1016/j.vaccine.2015.04.036
11. Liu Q, Qin C, Liu M, Liu J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: a systematic review and meta-analysis. Infect Dis Poverty. 2021;10(1):132. doi:10.1186/s40249-021-00915-3
12. Hou Z, Tong Y, Du F, et al. Assessing COVID-19 vaccine hesitancy, confidence, and public engagement: a global social listening study. J Med Internet Res. 2021;23(6):e27632. doi:10.2196/27632
13. Mallapaty S. Researchers fear growing COVID vaccine hesitancy in developing nations. Nature. 2021;601(7892):174–175.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.