Back to Journals » Patient Preference and Adherence » Volume 13
Vaccination management for elderly patients in primary care settings – documentation and responsibilities during a vaccination campaign
Authors Weinmayr LM, Steinhäuser J, Gehring SC, Goetz K ![]()
Received 16 April 2019
Accepted for publication 28 June 2019
Published 31 July 2019 Volume 2019:13 Pages 1295—1302
DOI https://doi.org/10.2147/PPA.S212507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Lisa-Marie Weinmayr,1 Jost Steinhäuser,1 Svante Christoph Gehring,2,3 Katja Goetz1
1Institute of Family Medicine, University Hospital Schleswig-Holstein, Luebeck 23538, Germany; 2Ärztegenossenschaft Nord eG, Bad Segeberg 23795, Germany; 3HANN Haus & Facharztnetz Nord GmbH, Norderstedt 22851, Germany
Objective: The aims of the current analysis were to evaluate the vaccination status and attitudes towards vaccinations of elderly patients and to explore effects of a vaccination campaign.
Methods: The data were raised in primary care settings by a physicians network which collected data during routine care from 697 patients and by the analysis of health insurance claims data from the Kassenärztliche Vereinigung Schleswig-Holstein (KVSH/Association of Statutory Health Insurance Physicians of the federal state of Schleswig-Holstein, Germany), regarding vaccinations in the participating practices before and after a vaccination campaign.
Results: Vaccination documentation for tetanus (57.7%), diphtheria (55.7%) and influenza (55.8%) was available for slightly more than half of the study sample. A lower documentation rate was observed for pertussis (33.1%), pneumococcal vaccination (30.3%) and polio (26.3%). Practice assistants were more responsible for determining the vaccination status than physicians. The attitude regarding influenza and pneumococcal vaccine was positive in 72.9% and 56.9% of patients respectively. After the campaign, rates of influenza and pneumococcal vaccine utilization increased by 13.4% and 62.9%, respectively.
Conclusions: Attitudes regarding vaccination were generally positive. Documentation was missing for almost half of the elderly population. The delegation of vaccine management to practice assistants could increase the immunization rate. Moreover, it can be assumed that a campaign might be helpful in increasing vaccination awareness and vaccine coverage.
Keywords: vaccination, primary care, quality improvement, influenza, pneumococcal vaccine
Background
Vaccinations represent one of the most important measures to prevent infectious diseases. With the aid of vaccinations, diseases can be significantly reduced or even eradicated.1 Moreover, vaccinations have not only the potential to protect the individual but also to provide herd immunity. Thus, even individuals that cannot be vaccinated are less likely to be infected.2 After the World Health Assembly in May 2012, the World Health Organization (WHO) decided, along with other partners, to start the Global Vaccine Action Plan (GVAP). One aim of GVAP is national vaccination coverage of 90% or more for all vaccinations recommended in a country’s immunizations schedule. This is aimed for by the year 2020.3,4
In Germany, the “Standing Committee on Vaccination” (Ständige Impfkommission/STIKO) is an independent advisory group that provides vaccination recommendations. These recommendations form the basis of public recommendations for each of the German federal state health authorities. Each year the STIKO releases an updated immunization schedule. The current schedule includes vaccinations against tetanus, diphtheria, pertussis, haemophilus influenza type b, poliomyelitis, hepatitis B, meningococcal disease group C, rotavirus, measles, mumps, rubella, varicella and human papillomavirus.5 Furthermore, individuals aged 60 years or older are recommended to receive vaccinations against influenza and pneumococcal vaccine. Additionally, individuals living in residential care or nursing homes as well as patients with chronic diseases, are eligible to receive influenza vaccination.6 However, the recommendations are not legally binding, as there is no compulsory vaccination in Germany.6
Following the rise in pertussis cases and the risk of contagion of infants, the recommendation of a single tetanus, diphtheria, pertussis (Tdap) vaccination was given in 2009 for all adults with the next tetanus and diphtheria catch-up.7 Most data regarding adult vaccinations are obtained from secondary data analysis such as health insurance claims data from the Kassenärztliche Vereinigung Schleswig-Holstein (KVSH).8
Previous studies on tetanus and influenza vaccine uptake in Germany demonstrated that physicians were the most important source for vaccination advice.9 As 90% of the German people have contact with a general practitioner (GP) during a given year, they represent the main contact point concerning vaccinations for adults in Germany too and therefore carry great responsibility in this regard.10 However, regarding influenza vaccination, only half of the GPs recommended the vaccination to all risk groups.11 In 2014, a survey on the implementation of influenza vaccination recommendation in nursing homes in Germany showed that about 65% of participating nursing homes offered specific immunization activities. One reason for the absence of immunization activities was the belief of the nursing home staff, that this should be the responsibility of the residents’ GPs.12 Moreover, it was found that GPs show a high willingness to delegate the task if the legal requirements are clarified.13 It can be assumed that vaccination management could be a task which can be performed by practice assistants.
Against this background, the aim of the analysis was twofold: a) to evaluate the vaccination status and attitudes of elderly patients and the responsibilities towards immunization in primary care and b) to explore the effects on immunization rates of a vaccination campaign by a physicians network.
Methods
The current analysis used a quantitative approach supported by different data sources, routine care data as well as secondary data. No primary data was collected.
Design of the study and data collection
Routine care data were raised by HANN GmbH (GP and Specialist Network North) in the federal state of Schleswig-Holstein, Germany. GmbH is a legal description of this network and identifies it as a public limited company to support public health care. This network represents 22 practices with 34 physicians. Patients are free to choose a physician independent of the network. Furthermore, GPs are not gate-keepers in Germany. Therefore, a list of registered patients was not available. The network is committed to facilitating local care and quality assurance. In this context, HANN GmbH planned the analysis of their routine care data concerning vaccination coverage as a measure to improve future vaccination rates. This project was initiated by HANN members as a quality assurance project following the regulation of practice network support by the KVSH.14 This project focused on patients aged 60 years and older. GPs and practice assistants collected the data during routine care in different settings of primary healthcare between September 2016 and March 2017. These data included house calls, visits to nursing homes and patient visits to participating practices.
Evaluation of the vaccination status and patients’ attitudes
The evaluation of the vaccination status was performed by extracting routine care data. For the quality assurance project HANN GmbH compiled a patient sheet to explore sociodemographic data, place of vaccination and vaccination status through digital patient records or vaccination certificates. This patient sheet was collected by the GPs and practice assistants within routine care as an important part of their own quality assurance. They asked patients questions regarding attitudes towards vaccinations in general and towards influenza and pneumococcal vaccination in particular. The GPs and practice assistants also asked for common reasons why patients had not been vaccinated yet; here multiple responses (n=16) were possible. For example these were “I don’t feel that I’m in any danger of contracting influenza”, “I have no vaccination certificate with me”, “I do not feel that I’m in any danger of contracting pneumonia”, “I’m suspicious of vaccinations”, or “I generally reject vaccination”. The questions were asked by the HANN members especially by physicians and practice assistants. Simultaneously, the study center received a report from HANN GmbH providing information about the participating physicians including sociodemographic data, information about each practice and number of years in practice as well as the physicians’ own attitudes towards vaccination. The inclusion of patients were consecutive during routine care. Data were completely anonymized by HANN GmbH and sent for analyses to the study center. The study center had no access to personal data.
Evaluation of the vaccination campaign
The evaluation of the vaccination campaign used secondary data supplied by KVSH. In addition, HANN GmbH organized a vaccination campaign between July 2016 and November 2016.
The vaccination campaign was developed by members of HANN GmbH especially by three GPs and the coordinator of the HANN GmbH network. A practice-based approach was chosen. The campaign included resources for the practices like a vaccination checklist and training of practice assistants. The training of practice assistants included the current recommendations of the STIKO, the review of vaccination certificates regarding STIKO recommendations and the use of the vaccination checklist. Patients had been informed by posters, educational material (flyers) in the GP practices, an interview on local TV and a newspaper article both of which were about the importance of vaccination. A HANN GmbH sticker on posters reminded patients to carry their vaccination certificate with them.
To evaluate the effects of the vaccination campaign, a before-and-after analysis design was used. The period of observation prior to the vaccination campaign was between November 2015 and February 2016. The observation period following the vaccination campaign was November 2016 until February 2017.
Data analysis
The analysis consisted of two parts. The first part was the analysis of data concerning vaccination status, patients attitudes and reasons against vaccination in routine primary care settings. The second part was the analysis of health insurance claims data of KVSH regarding vaccinations in the participating practices before and after the vaccination campaign. The reimbursement for vaccination varies from federal state to federal state and is based on the recommendation of STIKO in Germany. For SH a list of recommended vaccinations can be downloaded elsewhere.15
Data for analyses were obtained from two different sources, HANN GmbH and KVSH. The data were analyzed using SPSS Statistics version 24.0 (SPSS Inc., IBM). Categorical data were presented as frequency counts and percentages. Group comparisons were analyzed using the Chi2 test for categorical data. The analysis of administered vaccinations before and after the campaign was based on health insurance claims data from KVSH and calculated for each of the practices on the network. An alpha level of p<0.05 was used for tests of statistical significance. The incidence of missing data <10% was negligible for the purposes of data analysis.
Ethical approval
The ethics committee of the University of Lübeck examined the application of the ethical approval and was informed about the data analysis. These data were an integral part of the quality assurance project developed and performed by the HANN GmbH network. No formal approval was needed (correspondence: 30 September 2016, No. 16-267A). The ethics committee of the University of Lübeck stated than an ethical approval was not necessary for the secondary data analysis (No. 16-267A). The study center processed data which were completely anonymized and got no insight into routine care data from physicians who were members from the HANN network.
Results
Evaluation of vaccination status and patient attitudes
The evaluation of vaccination status during routine care was performed by 11 out of 22 primary care practices. The participating practices included 15 GPs whose mean age was 52.7 years (SD =9.5) and 46.7% (n=7) were male. Four of them worked in single practice. The general attitude towards vaccination was highly positive.
After exclusion of incomplete forms due to missing data regarding age (n=11) and after excluding patients aged younger than 60 years (n=61), 697 patients who were 60 years and older were eligible for the analysis.
An overview of the characteristics of the study sample is given in Table 1. Nearly two thirds of patients were female and more than 70% were between 70 and 89 years old. More than half (58%) of the vaccination status data were obtained by physicians, 42% by practice assistants. The vaccination status was in most cases collected during practice visits (47%) followed by nursing home visits (44%) and home visits (8%).
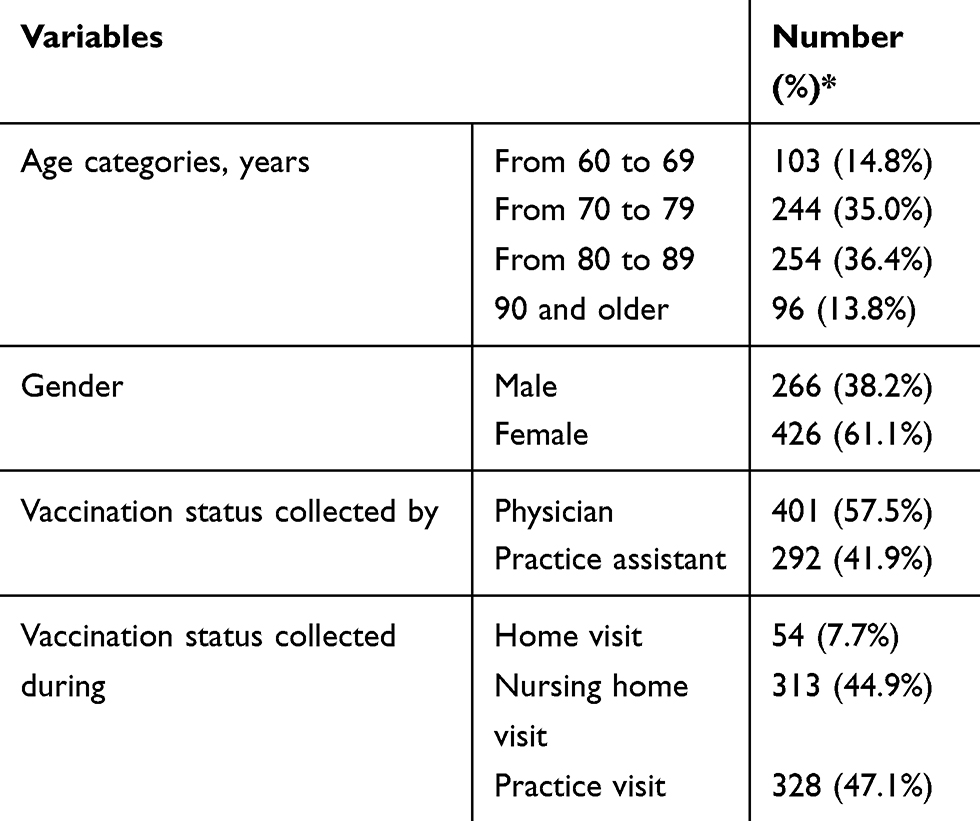 |
Table 1 Description of the study sample (n=697) |
Table 2 shows the results regarding the documentation of immunization. Six different vaccinations were checked during routine care. Vaccination documentation for tetanus (57.7%), diphtheria (55.7%) and influenza (55.8%) was available for more than half of the study sample. Almost one third showed records for pertussis (33.1%) and pneumococcal vaccination (30.3%), however, 74% of the sample did not have records for polio vaccination.
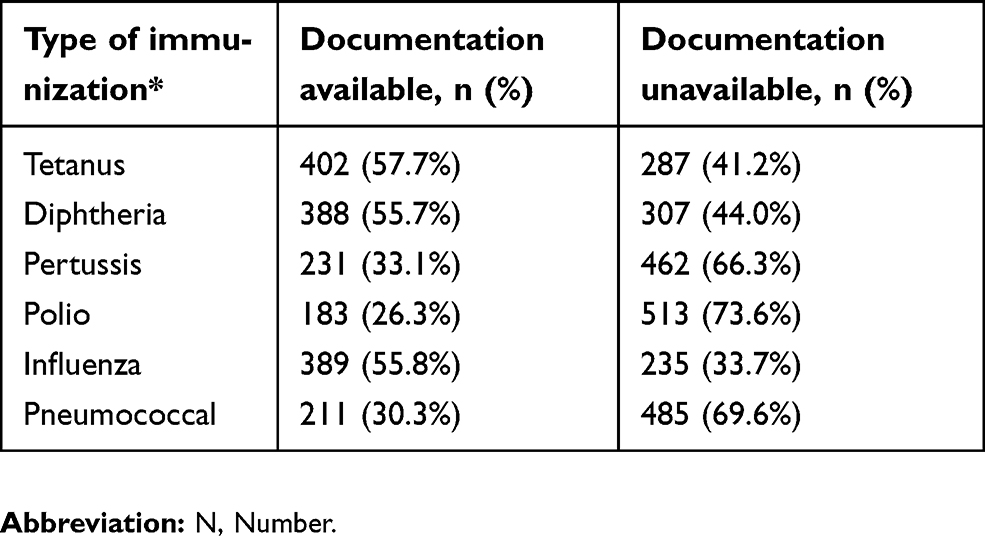 |
Table 2 Immunization of elderly patients by different vaccinations |
Different professionals collected the vaccination status in three types of settings. Table 3 shows that this task was carried out significantly more often by practice assistants in practice settings compared to home or nursing home visits. During home visits, data collection by practice assistants happened only in two cases. In nursing homes, GPs recorded more than two thirds of the documentation. During patient visits to the practice, practice assistants carried out the vaccination status collection in more than 70% of cases. In the main, practice assistants were responsible for determining of the vaccination status.
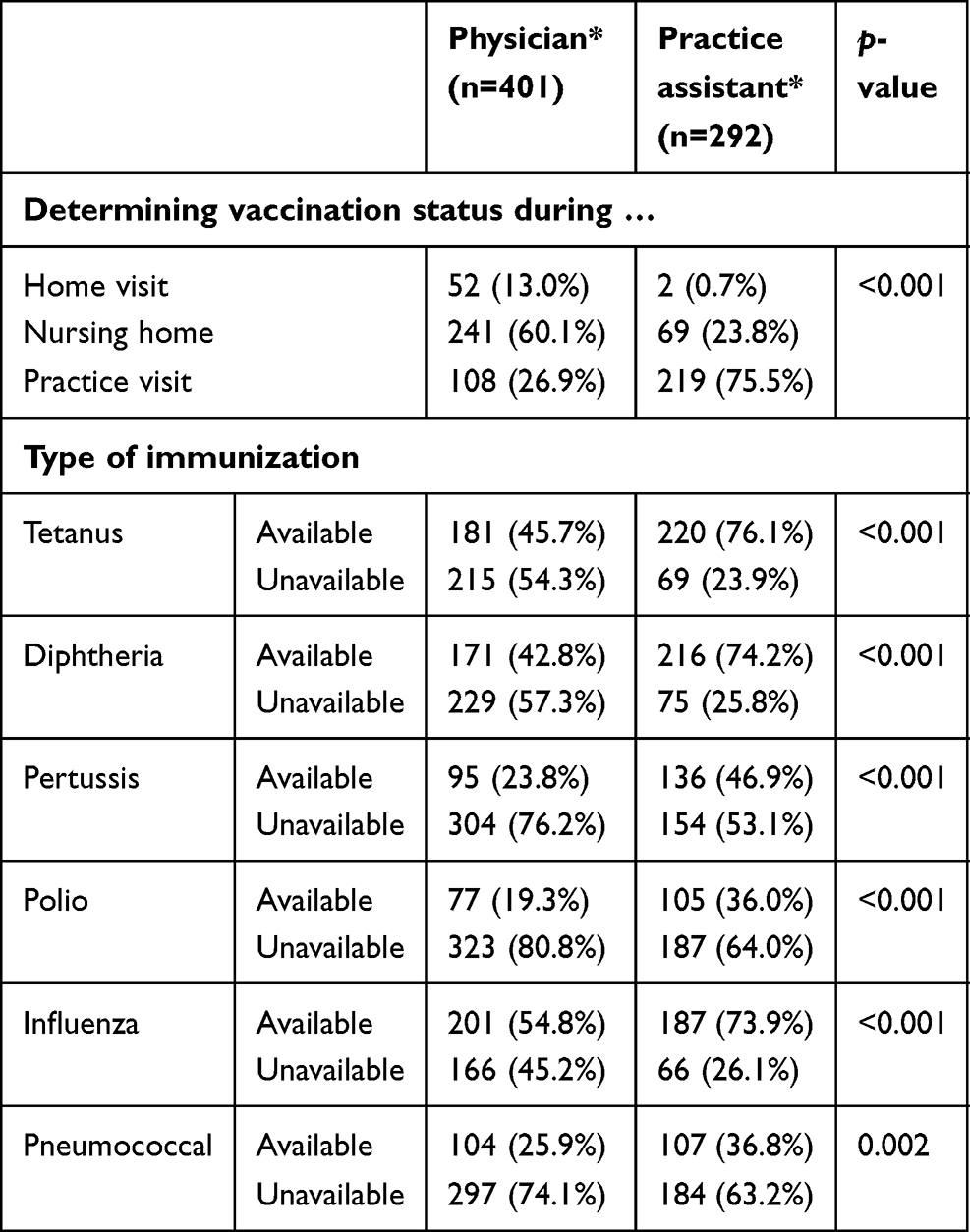 |
Table 3 Who is responsible for evaluating the vaccination status? |
The attitudes of patients towards vaccinations are illustrated in Table 4. The general attitude towards immunization was rated either “very positive” or “positive” in 60.9%. Our respondents were strongly in favor (“very positive” and “positive”) regarding influenza (72.9%) and pneumococcal (56.9%) vaccines.
 |
Table 4 Attitudes to vaccination – descriptive analysis (n=697) |
The participating patients had the possibility to state why they were against vaccination during routine care contact using 16 predefined response options. Table 5 presents the most common reasons. 205 patients responded to these reasons.
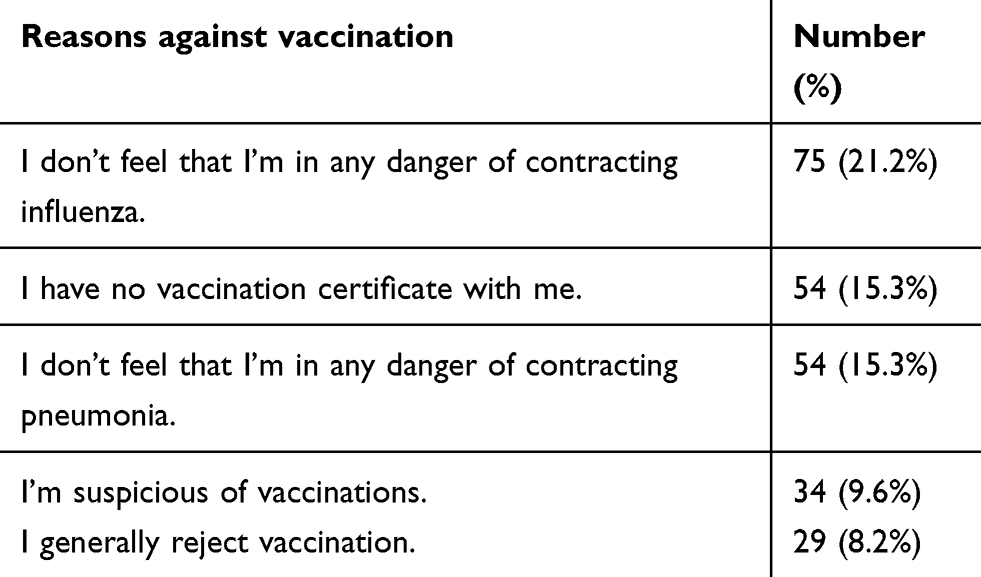 |
Table 5 The five common reasons for opposition to vaccinations (n=205) |
Evaluation of the vaccination campaign
Out of 22 HANN GmbH practices, 13 (59.1%) agreed to provide data on immunization rates. Table 6 presents an overview of the basic immunization rates before and after the vaccination campaign. An increase in immunization rates was observed for each immunization type after the vaccination campaign.
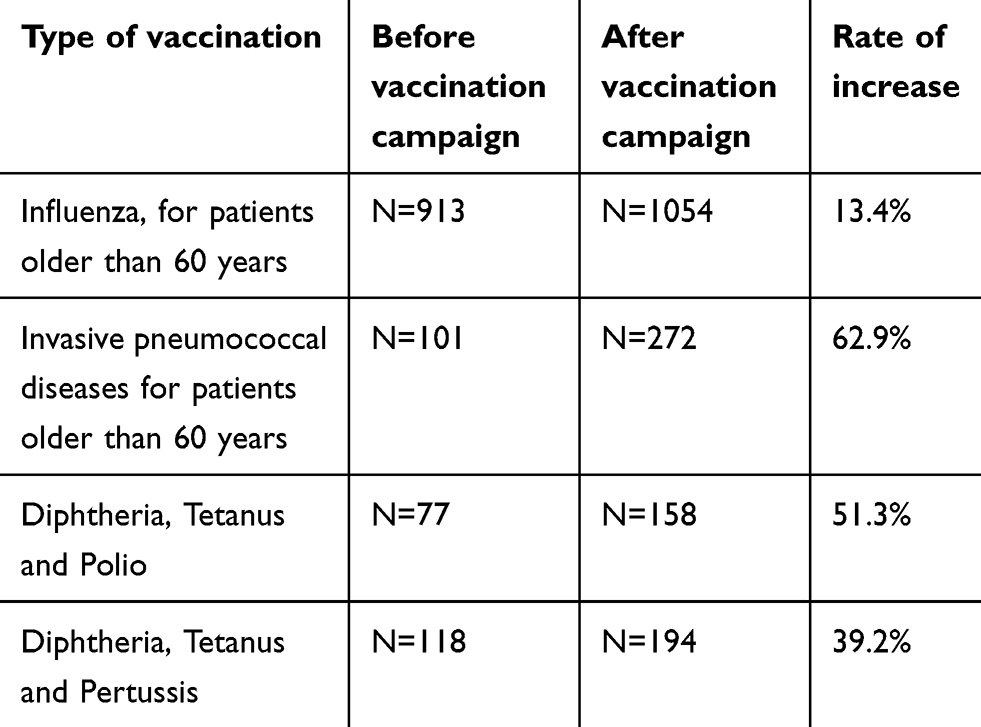 |
Table 6 Overview of vaccinations administered before and after the vaccination campaign |
Discussion
The study sample consisted of 697 patients from different primary care settings of a physicians network. The majority of patients were women between 70 and 89 years of age. The evaluation of the vaccination status by analyzing routine care data revealed a documentation rate exceeding 50% each for diphtheria, tetanus and influenza, whereas for two thirds of participants, polio, pneumococcal and pertussis records were not available. Incomplete records of immunization status were also found in the German Health Interview and Examination Survey for Adults (DEGS1) of 2013,16 which showed that these records are especially patchy for the elderly. The only vaccination that increased with patient age was the vaccination against influenza. Vaccination coverage among 60–69 year olds was 64%.16 Compared with DEGS1, our results for documented immunization against influenza were lower (55.8%). This might be due to the fact that our study population contained more patients from nursing homes and home visits than the DEGS1. However, both results (our study and the DEGS1 study) show lower rates of vaccination for influenza among elderly patients than the recommendation by the European Commission in 2009, which is 75%.17 Furthermore, even to date, the evidence in favor of this recommendation for healthy adults is limited.18,19
In this light, the discrepancy between the low immunization rates and positive attitude towards vaccination is striking. Previous findings seem to support the theory that there is a correlation between the physician’s attitude towards vaccination and the likelihood that a patient is vaccinated. This study also refers to the patient’s dependence on a GP’s recommendation for vaccination.20 Therefore, it can be assumed that future strategies to increase vaccination coverage should not only target patients but their GPs as well. The results regarding the data competence for evaluation of the vaccination status showed that in a practice setting vaccination status data were recorded more reliably by practice assistants than by GPs. The reasons for this observation should be addressed in further studies. However, it can be assumed that these results emphasize the importance of practice assistants within the primary care team in supporting their physician.
In primary care settings, vaccination management should be a task commonly delegated to practice assistants.21 However, a study about vaccination management among primary care doctors shows that GPs still predominantly take sole responsibility for this task.22 Task shifting could also have a positive effect on motivation at work. It was found that a doctor’s openness to the concept of delegation increased their own job satisfaction.13 Another solution for reducing workload could be the implementation of a digital health record system where all healthcare providers can potentially document and assess patient related data, which could facilitate the coordination of the task in the future.23
The vaccination campaign results and health insurance claims data from KVSH show a positive effect following the campaign. There is a strong possibility that campaigns affect attitudes and could lead to an increase in vaccination rates, as shown by different reviews.24,25 However, this is not conclusive in this study. Further research should explore the specific determinants of this vaccination campaign.26
Strengths and limitations
One of the strengths of this study was the practical orientation and that a practice-based approach was chosen. The evaluation of patient data was performed during routine care. Moreover, the collection of data took place via vaccination certificate and the practices’ digital record systems. This was another strength, as previous surveys have shown biased results when relying on self-reported vaccination status. Because the KVSH health insurance claims data did not provide specific information regarding the logged vaccinations, we could only analyze a limited number of vaccinations, which represents a limitation for the study. Furthermore, the analysis of the health insurance claims data had some methodological limitations. The data from KVSH only provided information about how many patients received vaccination during this time interval. Moreover, we need to take into account a selection bias, since patients with more positive attitudes towards vaccinations may have been more likely to participate in the survey. The documentation of immunization for the six different vaccines was assessed during routine care by GPs and practice assistants. A high variability between the participating practices could be assessed regarding inclusion of patients. It was not possible to analyze a multilevel model. Moreover, the vaccination status (basic immunization or booster vaccination) was unclear. Furthermore, the campaign was developed by members of the HANN GmbH network. They did not analyze the specific information needs in the target group beforehand, nor was the campaign material tested. Specific aspects, especially safety concerns, were addressed but a specific model was not considered as other studies demonstrated.27,28 Moreover, because of limited secondary data it was not possible to analyze whether the vaccination campaign was influenced by gender. In addition, the study sample consisted of patients from one region in Germany and cannot be generalized because vaccination behavior has shown regional variations nationwide.29
Conclusions
The practice-based approach which was used in this study shows that attitudes towards vaccination are positive. But particular attention needs to be given to offering vaccinations especially to the elderly population. It can be assumed that the delegation of tasks such as vaccination management from physician to practice assistants could increase the immunization rate in this population group. Under consideration of some limitations a vaccination campaign might be helpful to improve the situation of low immunization rates in primary care settings and could be of high relevance on a regional level.
Abbreviations
DEGS1, German Health Interview and Examination Survey for Adults; GP, General Practitioner; GVAP, Global Vaccine Action Plan; KV, Association of Statutory Health Insurance Physicians; SH, Schleswig-Holstein; STIKO, Standing Committee on Vaccination; Tdap, tetanus, diphtheria, pertussis; WHO, World Health Organization.
Acknowledgments
The authors would like to thank Thomas Frohberg from KVSH for providing the health insurance claims data and the Native speakers Andrea Strathausen and Michael Bauer for reviewing the manuscript.
The study was funded by Ärztegenossenschaft Nord eG.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
SCG was an employee of HANN GmbH. JS reports grants from Ärztegenossenschaft Nord eG, during the conduct of the study. SCG reports that Ärztegenossenschaft Nord eG received payment from Pfizer Deutschland for their services, to plan and carry out vaccination studies. Pfizer didn’t have any access to study design, data monitoring, statistical analysis and manuscript preparation. KG reports grants from Ärztegenossenschaft Nord eG during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Heininger U. [Complications of infectious diseases and benefits of immunization]. Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz. 2004;47(12):1129–1135. German. doi:10.1007/s00103-004-0951-z
2. Meyer C, Reiter S, Siedler A, Hellenbrand W, Rasch G. [The importance of vaccination. Epidemiology, vaccination programs, immunisation rates]. Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz. 2002;45(4):323–331. German. doi:10.1007/s00103-002-0398-z
3. WHO. Global vaccination plan. Annex 1. Available from: http://www.who.int/immunization/global_vaccine_action_plan/GVAP_Annex1.pdf?ua=1.
4. Feldstein LR, Mariat S, Gacic-Dobo M, Diallo MS, Conklin LM, Wallace AS. Global routine vaccination coverage 2016. WHO. Wkly Epidemiol Rec. 2017;92:701–716. http://apps.who.int/iris/bitstream/10665/259470/1/WER9246.pdf?ua=1. Available from:.
5. Robert Koch Institute. Recommendations of the standing committee on vaccination (STIKO) at the Robert Koch institute – 2017/2018. Epid Bull. 2017. 34: 333–376.
6. Standing committee on vaccination(STIKO). Available from: https://www.rki.de/EN/Content/infections/Vaccination/Vaccination_node.html. Accessed April
7. Robert Koch Institute. Recommendations of the standing committee on vaccination (STIKO) at the Robert Koch Institute July 2009. Epid Bull. 2009;33:339–346.
8. KV-Impfsurveillance. Available from: https://www.rki.de/DE/Content/Infekt/Impfen/Impfstatus/kv-impfsurveillance/kvis_node.html.
9. Böhmer MM, Walter D, Krause G, Muters S, Gosswald A, Wichmann O. Determinants of tetanus and seasonal influenza vaccine uptake in adults living in Germany. Hum Vaccin. 2011;7(12):1317–1325. doi:10.4161/hv.7.12.18130
10. Scherer M, Abholz HH, Chenot JF, Gerlach F, Kochen MM. Allgemeinmedizin und Familienmedizin. In: Pfaff H, Neugebauer EAM, Glaeske G, Schrappe M, editors. Lehrbuch Versorgungsforschung. Systematik – Methodik – Anwendung. Schattauer Verlag: Stuttgart 1. Aufl.; 2011. 337–341. German.
11. Wortberg S, Walter D, Knesebeck M, Reiter S. [Physicians as key communicators of the influenza vaccination for the elderly, patients with chronic conditions, and health care workers]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2009;52(10):945–952. German. doi:10.1007/s00103-009-0871-z
12. Bödeker B, Wichmann O, Mertens B, Seefeld L, Pott E. [Implementation of the influenza vaccination recommendation in nursing homes in Germany. Results of a survey as part of the national influenza immunization campaign]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2014;57(11):1315–1321. German. doi:10.1007/s00103-014-2044-y
13. Goetz K, Kornitzky A, Mahnkopf J, Steinhäuser J. At the dawn of delegation? Experiences and attitudes of general practitioners in Germany - a questionnaire survey. BMC Fam Pract. 2017;18:102. doi:10.1186/s12875-017-0607-3
14. Richtlinie der Kassenärztlichen Vereinigung Schleswig-Holstein zur Anerkennung von Praxisnetzen nach § 87b Absatz 4 SGB V. Available from: [https://www.kvsh.de/db2b/upload/downloads/2018_RiLi_Praxisnetze.pdf].
15. Public recommendation of vaccination in the federal state of Schleswig-Holstein 2019. Available from: https://www.schleswig-holstein.de/DE/Fachinhalte/I/Impfen/Downloads/OeffentlicheEmpfehlungSchutzimpfungenSH.html;jsessionid=0C7D3608923BB26517F52FFF3A74A4B9.
16. Poethko-Müller C, Schmitz R. [Vaccination coverage in German adults. Results of the German health interview and examination survey for adults (DEGS1)]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013;56(5):845–857. German. doi:10.1007/s00103-013-1693-6
17. Council Recommendation of 22 December 2009 on seasonal influenza vaccination. Available from: http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32009H1019&from=EN.
18. Demicheli V, Jefferson T, Ferroni E, Rivetti A, Di Pietrantonj C. Vaccines for preventing influenza in healthy adults. Cochrane Database Syst Rev. 2018;2:CD001269. doi:10.1002/14651858.CD001269.pub6
19. Michiels B, Govaerts F, Remmen R, Vermeire E, Coenen S. A systematic review of the evidence on the effectiveness and risks of inactivated influenza vaccines in different target groups. Vaccine. 2011;29(49):9159–9170. doi:10.1016/j.vaccine.2011.08.008
20. Paterson P, Meurice F, Stanberry LR, Glismann S, Rosenthal SL, Larson HJ. Vaccine hesitancy and healthcare providers. Vaccine. 2016;34(52):6700–6706. doi:10.1016/j.vaccine.2016.10.042
21. Mergenthal K, Beyer M, Gerlach FM, Guethlin C. Sharing responsibilities with the general practice team- a cross sectional study of task delegation in Germany. PLoS One. 2016;11:e0157248. doi:10.1371/journal.pone.0157248
22. Weltermann BM, Markic M, Thielmann A, Gesenhues S, Hermann M. Vaccination management and vaccination errors: a representative online-survey among primary care physicians. PLoS One. 2014;9:e105119. doi:10.1371/journal.pone.0105119
23. Kushniruk A, Kaipio J, Nieminen M, Nøhr C, Borycki E. Comparing approaches to measuring the adoption and usability of electronic health records: lessons learned from Canada, Denmark and Finland. Stud Health Technol Inform. 2013;192:367–371.
24. Szilagyi PG, Bordley C, Vann JC, et al. Effect of patient reminder/recall interventions on immunization rates: a review. JAMA. 2000;284(14):1820–1827. doi:10.1001/jama.284.14.1820
25. Jacobson Vann JC, Jacobson RM, Coyne-Beasley T, Asafu-Adjei JK, Szilagyi PG. Patient reminder and recall interventions to improve immunization rates. Cochrane Database Syst Rev. 2018;1:CD003941. doi:10.1002/14651858.CD003941.pub3
26. Baker R, Camosso-Stefinovic J, Gillies C, et al. Tailored interventions to address determinants of practice. Cochrane Database Syst Rev. 2015;4:CD005470. doi:10.1002/14651858.CD005470.pub3
27. Betsch C, Böhm R, Chapman GB. Using behavioral insights to increase vaccination policy effectiveness. Policy Insights Behav Brain Sci. 2015;2(1):61–73. doi:10.1177/2372732215600716
28. Betsch C, Rossmann C, Pletz MW, et al. Increasing influenza and pneumococcal vaccine uptake in the elderly: study protocol for the multi-methods prospective intervention study Vaccinication 60+. BMC Public Health. 2018;18:885. doi:10.1186/s12889-018-5787-9
29. Bätzing-Feigenbaum J, Schulz M, Schulz M, Acet S, Gisbert Miralles J [Entwicklung der saisonalen Influenzastandardimpfraten im kassenärztlichen Versorgungssektor in Deutschland seit der Pandemie 2009 - Eine Trendanalyse auf regionaler Ebene für den Zeitraum 2009/2010 bis 2013/2014]. Berlin: Zentralinstitut für die kassenärztliche Versorgung in Deutschland (Zi); 2015. Report No.: Versorgungsatlas-Bericht Nr. 15/19. Available from: http://www.versorgungsatlas.de/fileadmin/ziva_docs/68/VA-68-2015-Update%20Influenza%202014-Bericht-final.pdf.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.