Back to Journals » Open Access Emergency Medicine » Volume 18
Utilization of Virtual-Reality in Establishing a Code Trauma Crisis Resource Management Training Module
Authors Firdaus R ![]() , Tantri AR
, Tantri AR ![]() , Manggala SK, Dwiputra AG, Pramodana B, Auerkari AN, Hafidz N
, Manggala SK, Dwiputra AG, Pramodana B, Auerkari AN, Hafidz N ![]() , Omega A, Larasati D
, Omega A, Larasati D
Received 31 July 2025
Accepted for publication 8 January 2026
Published 13 January 2026 Volume 2026:18 557517
DOI https://doi.org/10.2147/OAEM.S557517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Charles V Pollack
Riyadh Firdaus,1,2 Aida Rosita Tantri,1 Sidharta Kusuma Manggala,1,2 Anggara Gilang Dwiputra,1 Bintang Pramodana,1 Aino Nindya Auerkari,1,2 Noor Hafidz,1 Andy Omega,1 Dewi Larasati1
1Department of Anesthesiology and Intensive Care, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; 2Rapid Response Team, Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia
Correspondence: Riyadh Firdaus, Department of Anesthesiology and Intensive Care, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia, Tel +62 21 3143736, Email [email protected]
Purpose: Crisis Resource Management (CRM) is critical in managing code trauma cases, yet remains underemphasized in many medical training programs in Indonesia. This study aimed to develop and evaluate a virtual reality (VR)-based CRM training module tailored for emergency physicians.
Patients and Methods: A pilot CRM module was designed through expert focused group discussions (FGDs) and refined using the Delphi method. The module included a lecture, roundtable discussion, and VR simulation. Fifteen emergency physicians participated in the training and were assessed using pre- and post-tests, a checklist based on CRM objectives, the Ottawa General Rating Scale (GRS), and a satisfaction questionnaire.
Results: Participants showed a significant improvement in knowledge (mean pretest 70 vs posttest 95.33; p < 0.001). Checklist completion rates had a median of 81% individually and 80% at the team level. Ottawa GRS scores indicated strong performance in leadership, problem-solving, communication, and situational awareness (overall mean score: 6.2/7). Satisfaction ratings reflected positive participant experiences with the module.
Conclusion: VR-based simulation is an effective, accessible tool for enhancing CRM skills in emergency settings, particularly in low-resource or remote environments. The module demonstrated high participant satisfaction and notable improvements in both individual and team performance and incorporating VR into trauma team CRM training should be considered.
Keywords: clinical competence, continuing medical education, emergency medicine, focus groups, healthcare team, virtual reality, focused group discussion, Ottawa GRS scores, crisis resource management
Introduction
The medical field is susceptible to errors, particularly in critical and emergency situations. Increased error rates are commonly observed in high-stress, rapidly evolving environments such as emergency departments, intensive care units, and operating theaters.1 This presents a significant challenge in emergency departments, where misdiagnosis can have severe consequences for admitted patients, particularly those classified as code trauma cases such as traumatic brain injuries (TBIs). This has become a challenge in emergency department, where misdiagnosis can lead to deleterious effect following patient admission, especially in code trauma patient.2 A crucial element within emergency department operations is crisis resource management, which aims to facilitate the effective allocation and utilization of resources during periods of heightened pressure and urgency.
Crisis resource management (CRM) traces its origins to the aviation industry. During the 1970s, the National Transportation Safety Board identified human error as a significant factor in over 70% of aviation accidents. Further investigations revealed that the majority of these errors stemmed from failures in teamwork rather than deficiencies in knowledge or technical skills.3 The healthcare sector, notably anesthesiology, was among the first to integrate CRM principles into the training of its practitioners. In the late 1980s, David Gaba and his et al recognized a parallel between aviation and anesthesiology: traditional training in the latter emphasized technical proficiency in patient management but overlooked the critical behavioral aspects of team dynamics and performance.4
Not all medical professionals in Indonesia have received sufficient CRM training. Many medical institutions do not include CRM training in their modules and curricula, resulting in students learning CRM only after completing their studies and beginning their work in emergency rooms directly. Indonesia, being an archipelagic nation, presents challenges in providing access to education for its populace, particularly medical professionals, including doctors, who work in remote areas. In recent years, virtual reality (VR) has emerged as a promising modality for simulation-based education, offering advantages over traditional manikin or lab-based training, particularly in terms of accessibility, cost-efficiency, and scalability. Evidence from recent emergency medicine and team-based training literature supports the use of VR to enhance situational awareness, communication, and coordinated decision-making in high acuity settings. These features make VR especially relevant in Indonesia, where geographical fragmentation and variable availability of simulation facilities pose substantial barriers to standardized CRM training, positioning VR as a practical and adaptable solution for expanding educational reach. In this report, we detail our experience in developing a CRM module tailored for emergency physicians conducting code trauma simulations in the emergency department. We utilized VR technology to minimize costs and broaden access for participants.
Materials and Methods
Target Participants
During the creation of the CRM module, our aim was to target medical professionals, including physicians and nurses, who are in their final year of study or have recently graduated. In this pilot study, we opted to include only physicians as study participants to facilitate the establishment of foundational rules and to gain insight into the current status of medical school graduates. Several previous modules have been developed that uses this approach.5 The process of module creation encompassed a series of focused group discussions (FGDs) led by anesthesiology experts to evaluate the needs of the participants, structure the module, develop its content, and design instructional, assessment, and evaluation components. This pilot implementation was intentionally limited to emergency physicians to ensure a homogenous participant group with comparable clinical backgrounds and familiarity with trauma resuscitation workflows. Restricting the cohort in this early developmental phase allowed for focused evaluation of content validity, feasibility, and clarity of the module without the confounding variability that may arise from mixed professional roles.
Design Foundation
We conducted a FGD with three experts in anesthesiology and emergency medicine (RF, AT, SM). These experts assessed the unmet needs of the study participants. Through extensive and comprehensive deliberation, it was determined that medical professionals in Indonesia, particularly emergency physicians who manage patients in the acute phase of TBIs in code trauma, are subjected to cognitive and interpersonal challenges. The cognitive aspect is largely influenced by multiple factors, including technical proficiency, experience in the current role, and frequency of exposure to such cases. Interpersonal challenges remain significant in this field, particularly in communication and leadership. The experts emphasized the critical importance of this component of CRM in forming effective teams for optimal patient management. Therefore, this module focuses its learning objectives on enhancing interpersonal aspects. The learning objectives, as defined by the experts, are as follows: understanding the environment, anticipating and planning, leading the team, being an effective team member, allocating attention wisely, distributing workload, and engaging in effective communication.
Outcome Objectives
The Delphi method was employed with five additional experts in anesthesiology and emergency medicine (AGD, BIN, ANA, AGA, NH) to establish a consensus on learning indicators for each learning objective. The learning indicators, along with criteria for each indicator, were gathered through a series of Delphi rounds aimed at achieving the most suitable consensus for defining each indicator. Delphi rounds were also conducted to determine the criteria for automatic failure and the minimum passing score. The learning objectives are aligned to the hierarchical models in Bloom’s taxonomy model.6
Content Development
All information gathered in previous stage was used in the module development. Following extensive discussions among the experts, it was decided that the teaching methods would include; 1) lectures, 2) roundtable discussions, and 3) simulation using VR. The participants will attend a 30-minute lecture, followed by a 15-minute question and answer session. The lecture materials were provided by RF. The roundtable discussion was conducted using several hypothetical clinical cases in a code trauma setting, including scenarios involving pneumothorax, stroke, and placental abruption. The roundtable discussion was led by one anesthesiologist per group of three participants. The simulation was then conducted at the end of the module, with the intention of also scoring participants’ performance. The technical road map of developing the module in this study is illustrated in Figure 1. The roadmap delineates the progression from initial expert-focused group discussions, through iterative Delphi consensus rounds, to the formulation of learning objectives, instructional components, and VR-based simulation workflows. It further outlines the integration of assessment instruments and the subsequent pilot implementation.
 |
Figure 1 Technical road map of module creation. |
The scenario involved a 50-year-old male brought by ambulance from a crash scene to the emergency room. The patient was unconscious, and the participants in the module assumed the role of physicians working in the emergency room and proceeded to provide treatment to the patient (see Figure 2). An anesthesiologist led the simulation from a far and scored the participants based on the evaluation form.
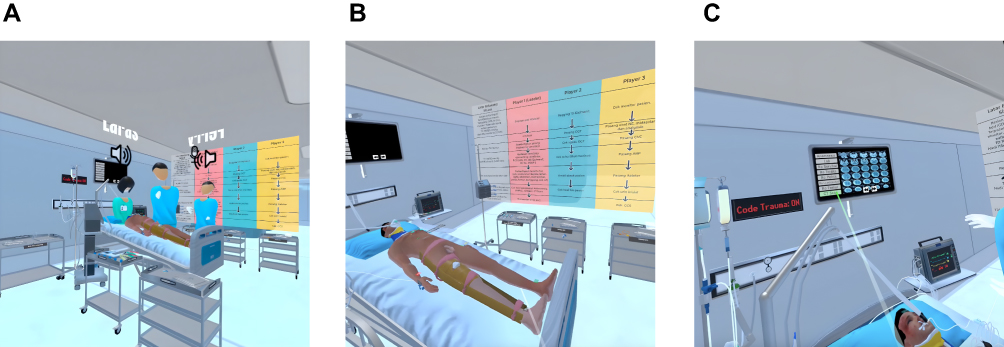 |
Figure 2 Snapshots from the code trauma simulation in virtual reality. (a) Multiple users with distinct roles managing a trauma case through interactive collaboration. (b) Role-specific algorithm displayed on a board for guidance. (c) Diagnostic evaluation interface simulating a real-world emergency situation. |
Assessment and Evaluation
Before and after the lecture, participants will complete a series of questionnaires to assess their baseline knowledge. The questionnaire consists of 10 items derived from the lecture materials. These multiple-choice questions have been previously validated, with each score corresponding to a significance level of p<0.05 and a correlation coefficient ranging from 0.3 to 0.6, indicating validity. Reliability testing yielded a Cronbach’s alpha of 0.86 for the total 10 items, demonstrating high internal consistency. Questionnaire is in Supplementary file and Figures 1 and 2. The checklist assessment was developed based on the learning objectives and success indicators previously established through the Delphi method consensus. In addition to the checklist, we also evaluated the team’s performance using the Ottawa General Rating Scale (GRS) for CRM, which is widely recognized and validated globally.7 We also adopted the satisfaction questionnaire used in medical simulation training from Turatsinze et al8 to reflect the subjective experiences of participants.8
Results
Fifteen emergency physicians were enrolled in the study, with thirteen also serving on the hospital’s rapid response team. Participants were organized into five teams of three, each consisting of one designated leader and two team members. The learning indicators and corresponding minimum passing scores used for assessment are summarized in Table 1.
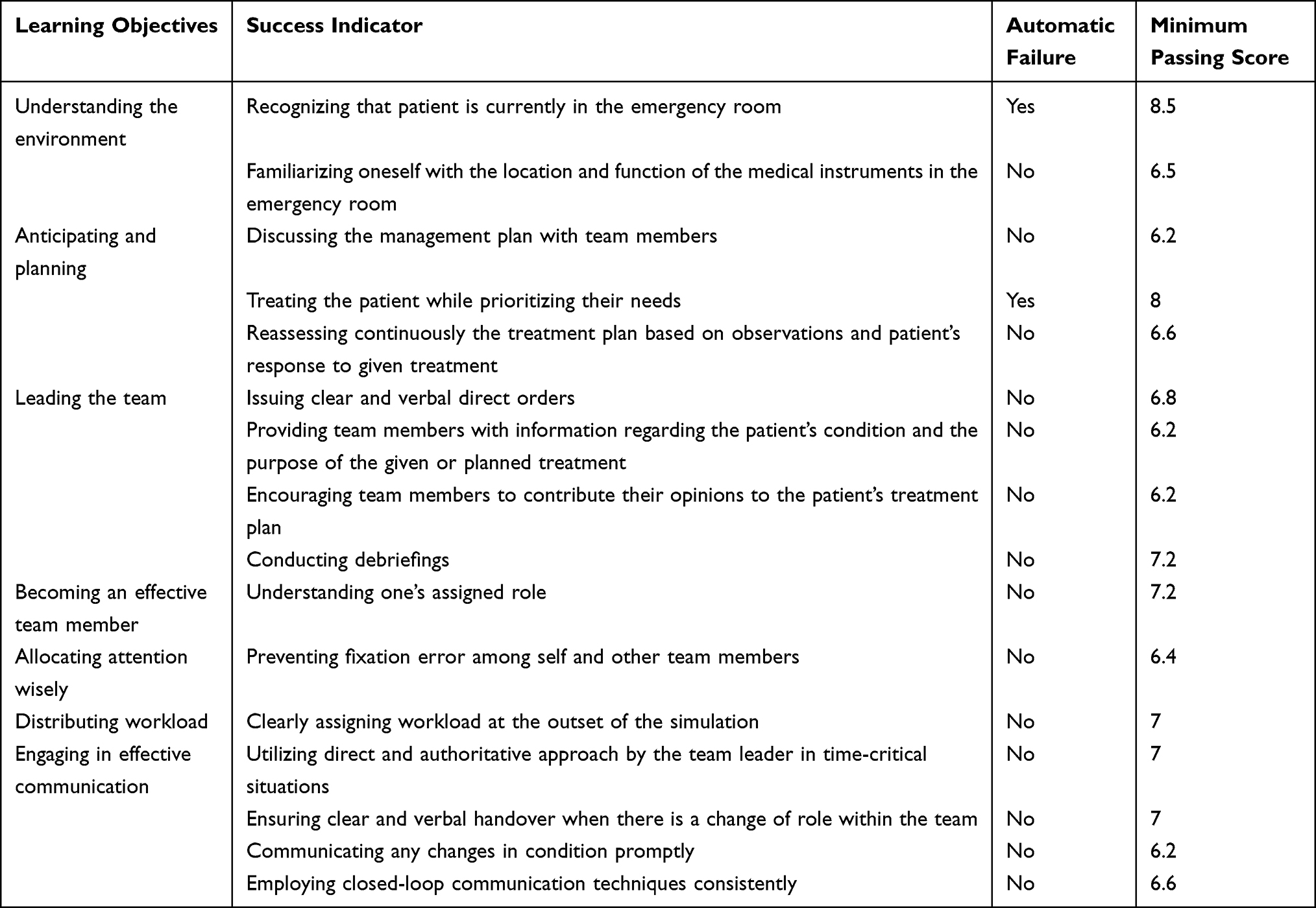 |
Table 1 Learning Objectives and Success Indicators |
The mean pretest score was 70 (SD = 7.5), and the mean posttest score was 95.33 (SD = 5.1), resulting in a mean difference of 25 points (95% CI: 19—31) between the pretest and posttest scores. The result is statistically significant (p < 0.001). The checklist derived from the learning indicators was assessed by one anesthesiologist for each team. The completion rate of the checklist was scored individually and as a team. The data were not normally distributed. Individual checklist completion demonstrated a median score of 81% (range: 60–100%), while team completion demonstrated a median of 80% (range: 72–92%). Although overall performance was strong, item-level patterns revealed consistent gaps in several interpersonal CRM domains. Participants frequently missed behaviors related to preventing fixation errors, ensuring continuous reassessment, and explicitly distributing workload at the start of the simulation.
The overall team performance was assessed with Ottawa GRS for CRM which consists of five discriminating domains and one overall domain, each rated on a 7-point Likert scale. The overall domain score (leadership, problem-solving, situational awareness, resource utilization, and communication) for team performance is 6.2 out of 7 (see Figure 3) indicating generally high proficiency. Notably, leadership and problem-solving were the strongest domains, with consistently high ratings across teams. Situational awareness and resource utilization showed modestly lower scores, with greater variability between teams. This pattern aligns with the checklist findings, suggesting that while participants readily demonstrated directive leadership and decision-making, they were less consistent in integrating environmental cues and optimizing task distribution.
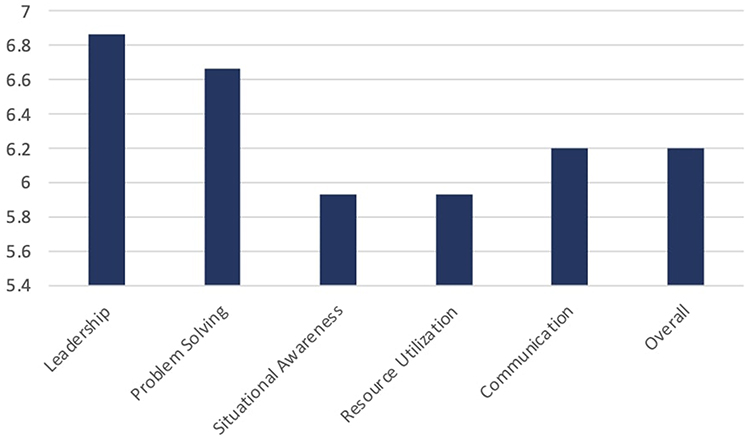 |
Figure 3 The team’s performance based on Ottawa General Rating Scale (GRS) showed that the leadership and problem-solving domains received the highest ratings. Situational awareness and resource utilization scored below the average, suggesting areas for improvement within the module. |
Participants’ subjective experiences, as reflected in the satisfaction questionnaire, were overwhelmingly positive. The majority selected “strongly agree” or “agree” across items related to realism of the VR scenario, perceived enhancement of teamwork, clarity of instructions, and relevance to clinical practice. Several items also captured participants’ perceptions of teamwork dynamics and communication efficiency during the simulation. Respondents frequently commented on how the VR environment heightened engagement and encouraged more explicit communication, particularly during complex or rapidly evolving phases of the scenario (see Figure 4).
 |
Figure 4 The satisfaction questionnaire revealed that the participants perceived significant benefits from the module, particularly in teamwork involvement and optimizing patient care. Nevertheless, areas for improvement such as, improving leadership skills, should be addressed in future evaluations. |
Discussion
The results of this pilot study demonstrate the effectiveness of the simulation training program in enhancing the participants’ knowledge and non-technical skills in CRM. The significant improvement in posttest scores compared to pretest scores indicates the positive impact of the training intervention. This finding is consistent with previous research highlighting the efficacy of simulation-based training in improving clinical competencies and decision-making skills among healthcare professionals. Several previous studies showed that CRM training model developed for initial care of polytrauma patients improved theoretical knowledge, participants perceptions, and attitudes regarding leadership, communication, roles, and situational awareness of members of the trauma team.9–11
The assessment of team performance using the Ottawa GRS for CRM revealed a high overall domain score, indicating proficient performance in leadership, problem-solving, situational awareness, resource utilization, and communication. This suggests that the participants effectively applied CRM principles during the simulation scenarios, demonstrating their ability to manage complex clinical situations collaboratively. Previous studies corroborate these findings suggesting training in CRM increases the overall team performance in emergency cases.12–14 Effective leadership is essential in managing crises and coordinating team efforts. CRM emphasizes the importance of clear communication, decision-making, and direction from leaders. Strong leadership fosters team cohesion, ensures task allocation, and promotes adherence to protocols, ultimately enhancing overall performance. By employing problem-solving techniques such as situation assessment, decision-making, and action planning, teams can navigate complex scenarios more effectively. This proactive approach to problem-solving minimizes errors, optimizes resource utilization, and promotes efficient patient care.4,12,15
This study also demonstrated a trend indicating that the CRM module may benefit participants in future code trauma cases. The majority of participants responded positively to various aspects of the module, predominantly selecting “strongly agree” and “agree.” The three outcomes evaluated from the CRM module are sufficient to conclude that the module positively impacts participants’ knowledge and skills in code trauma patient management, particularly in terms of non-technical skills.
Another consideration that should be discussed in this study is the use of VR in simulation training for CRM module. Our initial rationale for utilizing VR was based on the understanding that many medical professionals in remote areas may face challenges in accessing traditional training programs conducted in urban centers. Therefore, our objective was to develop a teaching method that could enhance the coverage and accessibility of training for all medical professionals working in remote areas in Indonesian archipelago. Once this teaching instrument is validated and widely accepted, taking into account technical issues and internet connectivity requirements, we believe that medical professionals in remote areas will no longer need to travel to urban centers multiple times, incurring costly expenses for plane tickets, to attend one-day training sessions.
Despite the promising outcomes of this study, several challenges and areas for improvement should be considered for future iterations of the training program. We identified several limitations within our study. Firstly, there was a limited number of participants enrolled in the study. As we conducted the study in a national referral hospital, the majority of doctors were residents rather than general physicians. Consequently, we faced challenges in collecting data from a more diverse group of medical professionals. This limitation impacts the generalizability of our findings and the potential implementation of the module across different healthcare settings. Secondly, one such challenge is the variability in individual and team performance observed during the simulation exercises. Addressing this variability may require targeted feedback and debriefing sessions tailored to the specific learning needs of each participant. We encourage the further development of this module for future implementations. Thirdly, we have not compared the groups receiving the module with those not receiving the module to establish a clear association between module implementation and team overall performance in a code trauma setting. Lastly, the integration of VR technology into the simulation-based training program presents both opportunities and challenges. While VR offers immersive and realistic training environments, ensuring the fidelity and accuracy of the simulations remains a crucial consideration. We have not performed validity and fidelity test in our study. These limitations may be subject to future improvement of module and study design. Future research should explore ways to enhance the realism and authenticity of VR simulations to maximize their educational impact.
Conclusion
In conclusion, VR-based simulation training represents a valuable educational approach for enhancing crisis resource management skills among emergency physicians. This pilot study demonstrates the effectiveness of simulation-based training in improving knowledge, skills, and teamwork abilities in managing code trauma cases. Therefore, incorporating VR into trauma team CRM training should be considered. Moving forward, continued efforts to refine and expand simulation-based training programs are essential to ensure the ongoing professional development of healthcare professionals and optimize patient outcomes in high-stakes clinical environments.
Abbreviations
CI, confidence interval; CRM, crisis resource management; FGDs, focused group discussion(s); GRS, general rating scale; SD, standard deviation; TBIs, traumatic brain injuries; VR, virtual reality.
Ethics Approval and Informed Consent
This study was approved by The Ethical Committee of The Medical Faculty of Universitas Indonesia (approval number KET-65/UN2.F1/ETIK/PPM.00.02/2023, dated 09/01/2023) and by The Dr. Cipto Mangunkusumo Hospital Review Committee with protocol number 22-12-1471, and was performed according to the Declaration of Helsinki (2013) and in adherence to Good Clinical Practice Guidelines. All participants involved in this study provided informed consent. Participant data were securely stored in encrypted, password-protected files, with access restricted to the research team.
Acknowledgments
We extend our heartfelt gratitude to the entire team for their unwavering dedication and valuable contributions. Special appreciation goes to the Department of Anesthesiology and Intensive Care, Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia for their consistent support throughout this project.
Funding
This work was supported by Universitas Indonesia under the Publikasi Terindex Internasional (PUTI) grant scheme [grant number: NKB-600/UN2.RST/HKP.05.00/2022]. The grant was given to increase the university lecturer publication index and has not affected the study process neither it has interfered the result of the study.
Disclosure
The authors declare no conflict of interest related to the writing, content, or publication of this manuscript.
References
1. Robertson JJ, Long B. Suffering in silence: medical error and its impact on health care providers. J Emergency Med. 2018;54(4):402–8. doi:10.1016/j.jemermed.2017.12.001
2. Gillman LM, Brindley PG, Blaivas M, Widder S, Karakitsos D. Trauma team dynamics. J Crit Care. 2015;32:218–221. doi:10.1016/j.jcrc.2015.12.009
3. Helmreich RL. Does CRM training work? Air Line Pilot. 1991;60(5):17–20.
4. Gaba DM. Crisis resource management and teamwork training in anaesthesia. Br J Anaesth. 2010;105(1):3–6. doi:10.1093/bja/aeq124
5. Lucas A, Edwards M. Development of crisis resource management skills: a literature review. Clin Simul Nurs. 2017;13(8):347–358. doi:10.1016/j.ecns.2017.04.006
6. Orgill BD, Nolin J. Learning taxonomies in medical simulation [homepage on the Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559109/.
7. Kim J, Neilipovitz D, Cardinal P, Chiu M, Clinch J. A pilot study using high-fidelity simulation to formally evaluate performance in the resuscitation of critically ill patients: the university of ottawa critical care medicine, high-fidelity simulation, and crisis resource management i study. Crit Care Med. 2006;34(8):2167–2174. doi:10.1097/01.CCM.0000229877.45125.CC
8. Turatsinze S, Willson A, Sessions H, Cartledge PT. Medical student satisfaction and confidence in simulation-based learning in Rwanda – pre and post-simulation survey research. Afr J Emerg Med. 2020;10(2):84–89. doi:10.1016/j.afjem.2020.01.007
9. Alegret N, Valle A, Subirana L, Fuentes S, Montmany S, Valero R. Design and implementation of a “crisis resource management” training program for the initial assessment of polytrauma patients. Cir Esp. 2023;101(9):617–623. doi:10.1016/j.ciresp.2023.02.007
10. Gillman LM, Brindley P, Paton-Gay JD, et al. Simulated trauma and resuscitation team training course—evolution of a multidisciplinary trauma crisis resource management simulation course. Am J Surg. 2016;212(1):188–193.e3. doi:10.1016/j.amjsurg.2015.07.024
11. Hughes KM, Benenson RS, Krichten AE, Clancy KD, Ryan JP, Hammond C. A crew resource management program tailored to trauma resuscitation improves team behavior and communication. J Am Coll Surg. 2014;219(3):545–551. doi:10.1016/j.jamcollsurg.2014.03.049
12. Lei C, Palm K. Crisis resource management training in medical simulation [homepage on the Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551708/.
13. Bernardino-Santos M, Arnal-Velasco D, Reboto-Cortés P, et al. Comparative analysis of the impact of training through simulation using the crisis resource management tool for primary care professionals. Healthcare. 2024;12(2):230. doi:10.3390/healthcare12020230
14. Clarke S, Horeczko T, Carlisle M, et al. Emergency medicine resident crisis resource management ability: a simulation-based longitudinal study. Med Educ Online. 2014;19(1):25771. doi:10.3402/meo.v19.25771
15. Reznek M, Smith-Coggins R, Howard S, et al. Emergency medicine crisis resource management (EMCRM): pilot study of a simulation-based crisis management course for emergency medicine. Acad Emerg Med. 2003;10(4):386–389. doi:10.1197/aemj.10.4.386
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.