Back to Journals » Risk Management and Healthcare Policy » Volume 14
Utilization of Integrated Community Case Management Service and Associated Factors Among Mothers/Caregivers Who Have Sick Eligible Children in Southern Ethiopia
Received 30 October 2020
Accepted for publication 18 January 2021
Published 3 February 2021 Volume 2021:14 Pages 431—438
DOI https://doi.org/10.2147/RMHP.S278231
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Serawit Samuel1 1, Aseb Arba2 2
1School of Public Health, College of Medicine and Health Science, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2School of Nursing, College of Medicine and Health Science, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Aseb Arba Tel +251916038833
Email [email protected]
Background: Proper utilization of integrated community case management service has a significant contribution in reducing the under-five children mortality. However, the utilization of integrated community case management service is low especially in developing countries like Ethiopia. Therefore, this study was planned to assess the utilization of integrated community case management service and associated factors among mother/caregivers who have sick children aged 2– 59 months in Boloso Sore Woreda, Southern Ethiopia.
Methods: Community-based cross-sectional study design was done from January 15-February 15, 2018. Face to face interview was conducted using pre-tested structured questionnaire. Bivariable and multivariable logistic regression analysis were carried out to assess the association between independent and outcome variables. Odds ratio along with 95% confidence interval and p-value < 0.05 were estimated to measure the strength of the association and statistical significance.
Results: The magnitude of the utilization of integrated community case management service was 25.3%. Mothers/caregiver’s education of secondary and above (AOR=4.15, 95% CI: 1.94– 8.90), mothers/caregivers having good knowledge about childhood illness (AOR=2.00, 95% CI: 1.08– 3.69), the previous visit of mothers/caregivers to health post (AOR=2.92, 95% CI: 1.01– 8.54), short distance to health post (AOR=2.42, 95% CI: 1.02– 5.76), the child with cough (AOR=2.52, 95% CI: 1.13– 5.63) and mother’s/caregiver’s perception of high severity of illness (AOR=2.51, 95% CI: 1.19– 5.27) were significantly associated with utilization of integrated community case management service.
Conclusion: The magnitude of the utilization of integrated community case management was low in the study area. Mother/caregiver’s education of secondary and above, having good knowledge of childhood illness, history of mother’s/caretaker’s visit to the health post, short distance to the health post, and perceived high severity of disease and presence of cough were factors significantly determining service utilization. Therefore, health education should be provided to mothers by Health Extension Workers, community leaders, and organizations.
Keywords: common childhood illness, integrated community case management, mothers/caregivers
Introduction
Globally, there was 43 under-five child deaths per 1000 live birth in 2015.1 The leading causes were neonatal conditions (33%), diarrheal diseases (22%), pneumonia (21%), malaria (9%), and Acquired Immuno-deficiency Disease (AIDS) (3%).2 In Ethiopia, nearly 205,000 children are dying every year before they reach their fifth birthday, mostly from preventable or treatable diseases, including Pneumonia (18%), diarrhea (13%), and malaria (7%).3
To overcome this, World Health Organization (WHO) and United Nations Children’s Fund (UNICEF) in collaboration with other development partners developed an approach named Integrated Community Case Management (iCCM) to bring treatment services closer to home particularly to those with poor access to health facilities and advocated for low- and middle-income countries in the 2000s.4,5 It is an approach of providing integrated case management services such as assessment, treatment, and referral following locally adapted WHO/UNICEF guidelines for illnesses including diarrhea, pneumonia, malaria, and malnutrition among children younger than five years of age at the community level (ie, health posts) by health extension workers where there is limited access to health facility.4,6
The Government of Ethiopia has committed to further reduce the under-five mortality rate below 20 per 1000 live births by the year 2035. To achieve this goal, the country is implementing the iCCM strategy starting from February 2010. Ethiopia is using the platform of the Health Extension Program Strategy to improve coverage by delivering curative interventions to sick children in communities that lack access to health centers. It includes diagnosing and treating diarrhea, pneumonia, and malaria in children under five at the community level, as well as identifying and referring sick newborns has the potential to decrease childhood mortality from these three diseases.6
The utilization of integrated community case management had a great effect on reducing child mortality, especially in developing countries, with about 35% reduction from pneumonia and a 21% reduction in overall mortality.5 It also prevents the need for transportation or walking the long distance to the health center, minimize time, halt the progress of disease severity, and reduce patient overload at the health center and hospitals.7
However, the utilization of integrated community case management towards common childhood illness is low in Asia and sub-Saharan countries. In Guatemala, 63–83% of mothers relied on home-based care for their under-five children who suffered from diarrhea, fever, and cough.8 And a study conducted in Uganda stated that 47.7% had not utilized integrated community case management services among those are eligible to use.9 Southern Ethiopia is one of the four regions where iCCM service has been implemented as a pilot program. However, the proportion of sick children receiving treatment in health facilities was about 54.5% in 2008.10 In the Hadiya Zone, South Ethiopia, 43.6% of sick children received treatment from health facilities, but only 3.9% of sick under-five children have sought treatment from health extension workers, the rest bypass health posts, and sought treatment from health centers.11
There were few studies conducted on the assessment of the quality, treatment rate, and utilization of iCCM service from secondary data (record review) at HP level, but that did not clearly get the target denominator of sick children and also did not identify factors that affect service utilization. However, there is no study was conducted on the magnitude of iCCM service utilization and factors affecting utilization using community-based study.
Objectives
- To assess the magnitude of integrated community case management service utilization among mothers/caregivers who have sick children aged 2–59 months in Boloso Sore Woreda, Southern Ethiopia, 2018.
- To identify factors associated with integrated community case management service utilization among mothers/caregivers who have sick children aged 2–59 months in Boloso Sore Woreda, Southern Ethiopia, 2018.
Methods
Study Area
The study was conducted in Boloso Sore Woreda, Wolaita zone, southern Ethiopia. The Woreda 30km far from Sodo which is the capital town of Wolaita zone, 184km far from Hawassa capital city of SNNPR, and 330km far from Addis Ababa capital of Ethiopia.
Study Design and Period
A community-based cross-sectional study was conducted from January 15 to February 15, 2018.
Population
Source Population were all mothers/caregivers who had sick children aged between 2 and 59 months living in the Boloso Sore Woreda. Study Population were all mothers/caregivers who had sick children aged between 2 and 59 months live in selected kebeles of Boloso Sore Woreda.
Sample Size Determination
The sample size was calculated for the first objective using single population proportion formula at 95% confidence level with 4% margin of error, and magnitude of iCCM utilization 9.3% from a study conducted in Jimma and Hararghe zones.12 We got 444 by using design effect of 2 and 10% non-response. For the second objective, we used double population formula using Epi Info 7 software for individual factors at 95% confidence level with 5% margin of error, 80% power, and exposed to the unexposed ratio of 1:1. After adding 10% in sample size obtained from second objective, the final sample size of the study was 449.
Sampling Procedure
From a total of 26 kebeles in the Boloso Sore Woreda, 8 kebeles were selected by a simple random sampling method. The preliminary survey was conducted to identify households had a sick child from the households who had under-five children age between 2 and 59 months by using a family folder from health posts. Then, the total sample size allocated proportionally to each kebeles based on the number of sick under-five children age between 2 and 59 months in the kebeles. A simple random sampling technique was employed for household selection.
Within each selected household only one mother/caregiver with index child was selected. Whenever there was more than one mother/caregiver with under-five children in a household, only one was selected using the lottery method, and more than one under-five children age between 2 and 59 months to a mother/caregiver in a household the younger child was selected.
Data Collection Methods
Data were collected using a structured and pre-tested questionnaire. The questionnaire was adapted to the research objectives and developed based on literature. The questionnaire was first designed in English then translated into Wolaita language to facilitate a better understanding of each question.
Eight diploma nurses were used for data collection and two BSc public health officers were used as a supervisor after providing two days of training. Data were collected through face-to-face interviews of mothers/caregivers by using structured questionnaires in a private place.
Data Quality Control
Data quality was controlled through training of data collectors on objectives, questionnaires, and ways of conducting the interview. Data collectors were supervised by 2 supervisors and the principal investigators received the report on a daily basis. Before actual data collection, a pretest was conducted in 5% of the sample size in Damote Gale Woreda. Completeness and consistency of the questionnaire were checked before and immediately after the interview by each interviewer and supervisor. Simple frequencies and cross-tabulation were done for missing data, outliers, and improvable values and variables.
Data Processing and Analysis
Data entry was made using Epi-data version 3.1 software after coding and checking for completeness and consistencies. Then, the data were exported to the SPSS statistical package version 22 for further analysis. Data were presented using frequency, proportions, and summary statistics to describe the study variables and factors under study.
The bivariable analysis was carried out to identify variables candidate for multivariable analysis. Variables whose p-value less than 0.25 in bivariate analysis were included in multivariable logistic regression. Multi-Collinearity was diagnosed using standard error and also Hosmer-Lemeshow was performed to test for model fitness. The odds ratio along with 95% CI was estimated to measure the strength of association. Variables were interpreted as having a statistically significant association when p-value < 0.05.
Ethical Considerations
The study was approved by the Institutional Health Research Ethics Review Committee of Haramaya University College of Health and Medical Sciences. The study was conducted in accordance with the declaration of Helsinki. The data collection was made after written and signed voluntary consent was taken from each participant after informing about the study. The participant identification information was not collected to maintain the anonymity and confidentiality of the study of information on the record. Severely sick child and mother/caregiver in the household during data collection were referred and contacted to a nearby health facility.
Results
Socio-Demographic Characteristics of Study Participants
A total of 439 mothers/caregivers were involved in the study giving an overall response rate of 97.8%. Two-thirds 289 (65.8%) of respondents were in the age group of 25–34 years. The mean (±SD) age of respondents was 27.6 (±4.5) years with a minimum age of 18 years and maximum age of 40 years. Most 388 (88.4%) of respondents were Wolaita in their ethnicity as shown in Table 1.
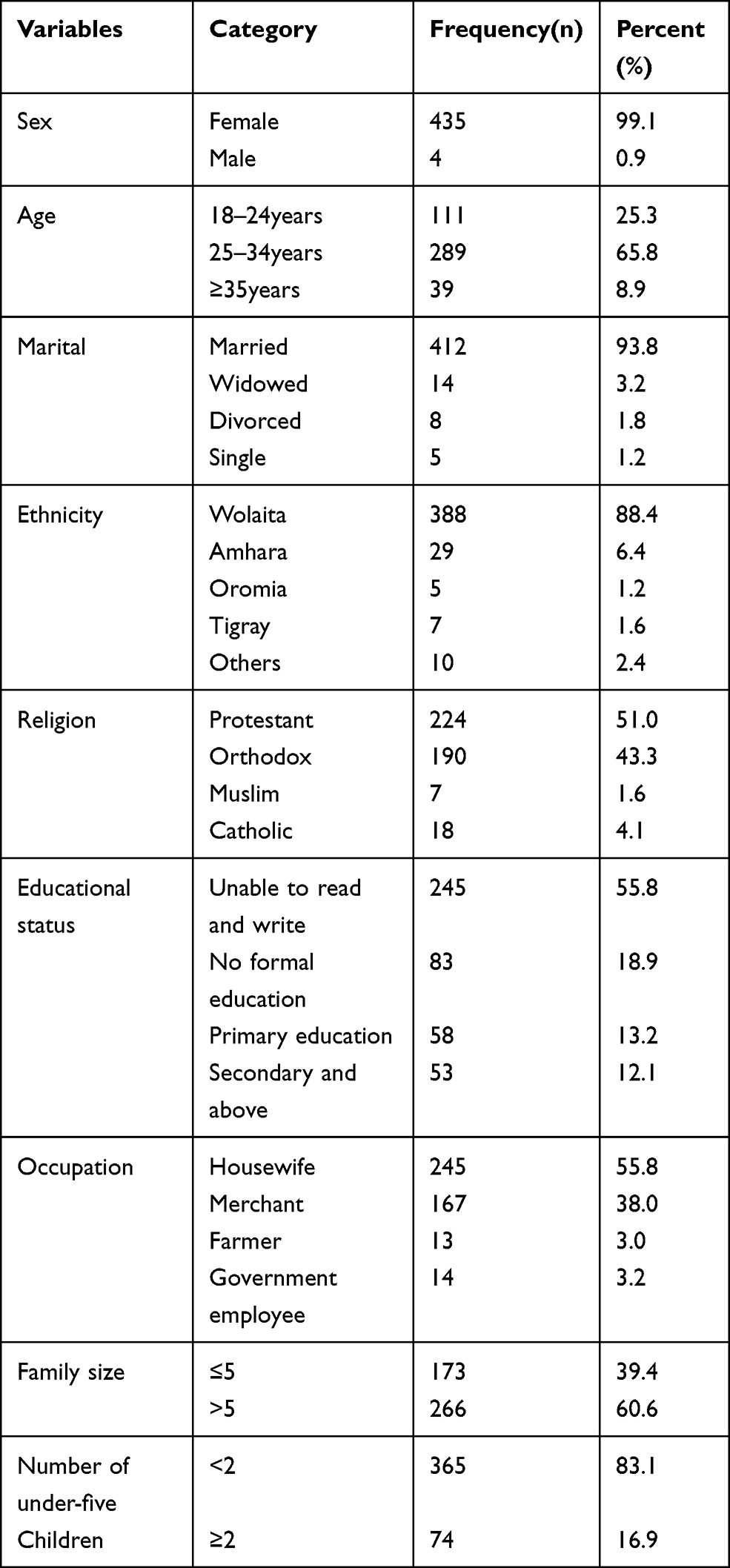 |
Table 1 Socio-Demographic Characteristics of Study Participants in Boloso Sore Woreda, Southern Ethiopia, 2018 (n=439) |
Childhood Illness-Related Characteristics
Out of the 439 under-five children age between 2 and 59 months who were sick within two weeks before the survey, 228 (51.9%) were male and 211 (48.1%) were female. One-third 150 (34.2%) of children were in the age group 12-<24 months. The mean (±SD) age was 22.2 (±12.5) months with a minimum of 3 months and a maximum of 58 months.
The Magnitude of iCCM Service Utilization
The overall integrated community case management service utilization of this study was 25.3% at 95% CI (21.4–29.4%). 111 (25.3%) received iCCM service in health posts shown in Table 2. From them, two-thirds 80 (66.7%) of sick children have received treatment for symptoms of cough and followed by 26 (22.5%) of sick children were received treatment for symptoms of fever shown in Figure 1.
 |
Table 2 Magnitude of iCCM Service Utilization of Children Aged Between 2 and 59months in Boloso Sore Woreda, Southern Ethiopia, 2018 (n=439) |
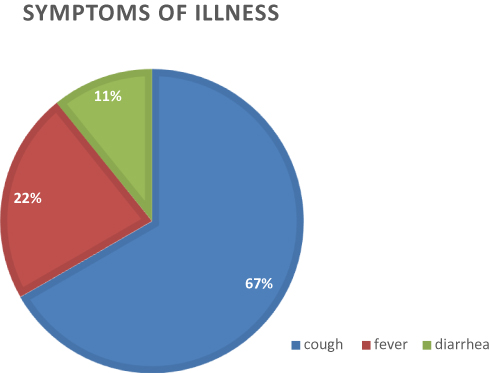 |
Figure 1 The symptoms of children illness that treated at health posts in Boloso Sore Woreda, 2018. |
Bivariable and Multivariable Analysis Result
In bivariable analysis; educational status of mother/caregiver, sex of the child, age of the child, presence of cough, perceived severity of childhood illness by mothers/caregivers was high, knowledge of mothers/caregivers on children illness, history of the visit to health post, and mothers/caregivers who travel <30 minutes to reach health post were variable candidate for multivariable analysis.
In multivariable analysis, the utilization of iCCM service for their sick children among mothers/caregivers who had primary education and secondary and above education was four times more likely to utilize iCCM than those of mothers/caregivers who were unable to read and write [AOR=4.14, 95% CI (1.91–8.97)] and [AOR=4.15, 95% CI (1.94–8.90)], respectively. The utilization of iCCM service among mothers/caregivers who had good knowledge towards children illness was two times more likely than those who had poor knowledge [AOR=2.00, 95% CI (1.08–3.69)] and the utilization of iCCM service among mothers/caregivers who had previous visit health post for any purpose was nearly three times more likely than mothers/caregivers who had no history of the previous visit of health post [AOR=2.92, 95% CI (1.01–8.54)].
The utilization of iCCM service among mothers/caregivers who walk less than 30 minutes to reach health post was 2.42 times more likely than mothers/caregivers who walk above 60 minutes [AOR=2.42, 95% CI (1.02–5.76)]. Children who had symptoms of cough receive iCCM service three times more than children who had diarrhea [AOR=2.52, 95% CI (1.13–5.63)]. Mothers/caregivers who perceived the severity of illness of their child as high were 2.51 times more likely to receive iCCM service than those perceived severity of illness as low [AOR=2.51, 95% CI (1.19–5.27)] as shown in Table 3.
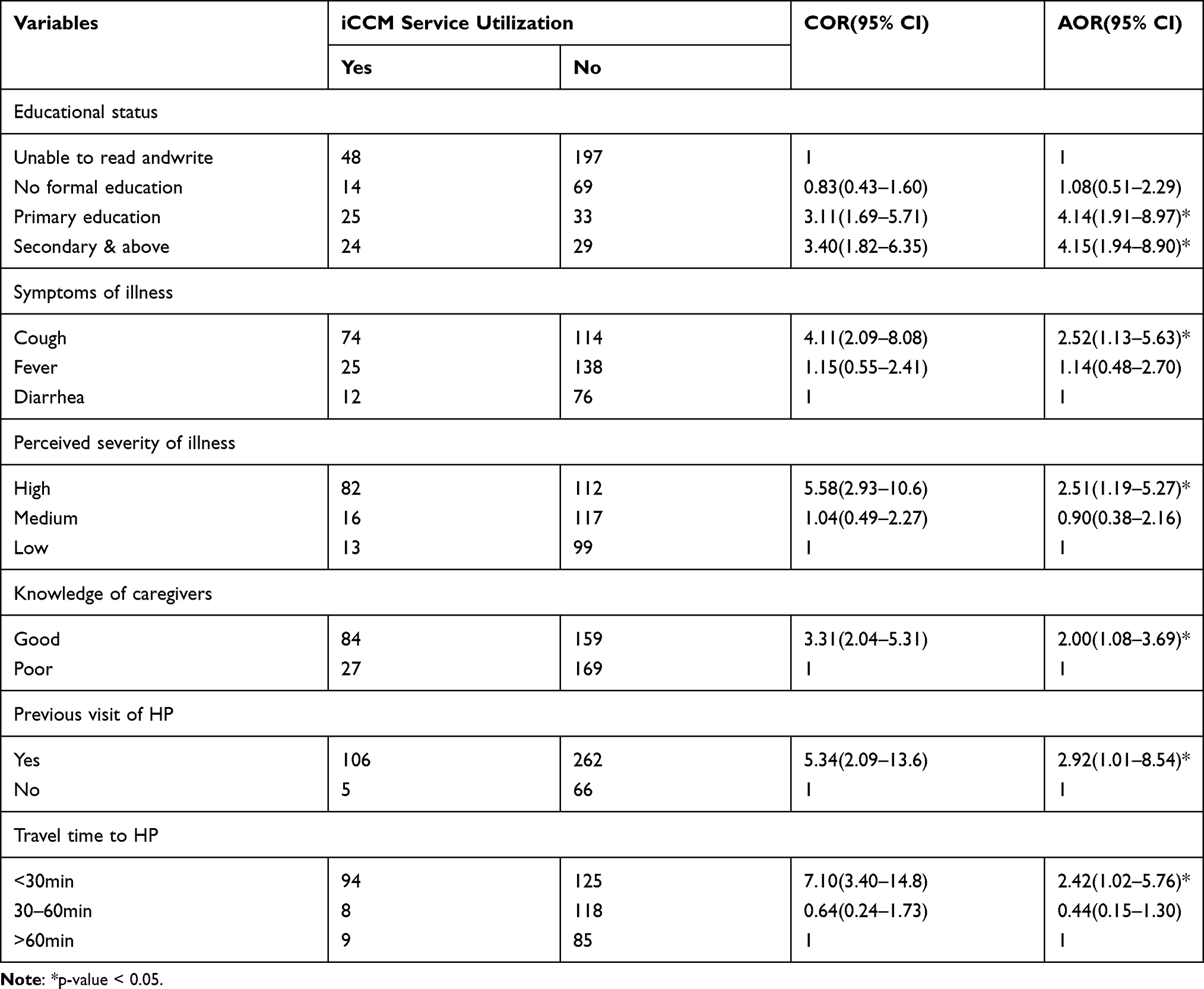 |
Table 3 Factors Associated in Multivariable Analysis with iCCM Service Utilization in Boloso Sore Woreda, Southern Ethiopia, 2018 (n=439) |
Discussion
The magnitude of integrated community case management service utilization in this study was 25.3%. In addition, factors like the educational status of mothers/caregivers, knowledge of mothers/caregivers on danger signs and causes of childhood illness, previous history of the visit to the health post, travel time to reach health post, symptoms of illness, and perceived severity of illness were factors significantly associated with utilization of iCCM service.
In this study, more than one-third (43.2%) of sick children were receiving treatment from home remedies, private clinic/drug shop, and traditional healers. This magnitude of 25.3% was in line with the study done in Kenya 22.1%.13 However, it was lower than studies done in Zambia which was 79.1%, and in Uganda where iCCM service utilization was 52.3%.7,9 This variation may be due to the difference in accessibility to health posts, service quality, supply chain, the policy the country following and educational background of mothers. However, the magnitude in the current study was much better than studies done in Hadiya 3.9% and Oromia 9.3%.11,12 This difference could be due to iCCM service was started as pilot program for a long time in the study area before expanding to other areas of the country. In addition, the difference in the study period, and this study included only sick under-five children than general under-five children that in turn increases utilization.
This study revealed that the educational status of mothers/caregivers was strongly associated with iCCM service utilization. The utilization of iCCM service among mothers/caregivers who had primary education, secondary education and above was four times more likely than those of mothers/caregivers unable to read and write. This result goes in line with the finding from the study done in Oromia.12 This is due to the fact that when level of education increase, the awareness of mothers/caregivers towards modern treatment increases, and literate mothers can read newspapers, banners, brochures, and billboards. Also educated mothers/caregivers have high confidence to decide on the health of their sick children to take treatment from health facilities by challenging the influence from family.
In this study, caregivers/mothers who had good knowledge were two times odds to utilize iCCM service than their counterparts. This finding was consistent with the finding of studies done in Uganda and Hadiya.9,11 This might be due to the fact that having good knowledge helps to recognize danger sign and symptoms of ill children that is necessary to take immediate action and appropriate management for disease conditions, thereby reducing complications and deaths in these children.
Caregivers/mother’s previous visit to health post for any service strongly determines iCCM service utilization. Caregivers/mothers who had a history of the previous visit to health posts for any other service were nearly three times the odds to utilize iCCM service than mothers/caregivers who did not. This finding was similar to the finding from the study which was done in Oromia.12 The plausible explanation for this visiting to health post might provide opportunity to get information about availability of treatment of common childhood illness at health post level, provide awareness about the service and develop trust in HEWs, which in turn increases iCCM service utilization. The compassionate, respectful, and patient-centered care for clients during facility visits is a top priority to improve the quality and increases utilization of health service delivery.14
This study result showed that distance from home to health post was strongly associated with iCCM service utilization. The utilization of iCCM service among mothers/caregivers of sick children who travels less than 30 minutes to reach health post from home were nearly two times more commonly utilize iCCM service than those who travel above 60 minutes. This finding was consistent with the finding of a study conducted in Uganda.9 This could be due to the distance determines accessibility, availability, affordability and acceptability of the services. The short distance saves time, saves transport costs, and is convenient for the mothers/caregivers. Hence, making the mothers/caregivers too easily access the health post in turn increases the iCCM service utilization.
This study showed that the present compliant of sick children strongly associated with iCCM service utilization. The sick under-five children with symptoms of cough were about two times more likely to utilize iCCM service than children with symptoms of diarrhea. This finding was comparable with the finding from a study done in Oromia and Hadya.11,12 This could be a result of poor knowledge of the mothers/caregivers with regards to recognizing the danger signs of in the children and also taking that the symptoms like diarrhea were not serious enough to warrant immediate treatment or intervention. This may also explain the reason why the first place of treatment by a greater proportion of the mothers/caregivers was at home and traditional healers.
This study also provided that perceived severity of illness was strongly predicted the utilization of iCCM service. The mothers/caregiver who perceives the child’s illness as highly severe were two times more likely to utilize iCCM service than children with perceived severity of illness was low. This finding was in line with the study done in Kenya and Oromia.12,13 This was compounded by the fact that most of the respondents took the sick child to treatment when the severity of illness was high because they are unable to treat severe case at home, traditional healers and from drug shop medications and this is why most respondents took their children for treatment after 24 hours of the onset of illness.
Limitation of the Study
The possible limitation of the study was recall bias since it based on self-report of past children health condition so that may be affected by recall bias that can underestimate the magnitude of outcome. To minimize this bias, we took two weeks history of children health condition prior to the study and interviewers probed to memorize.
Conclusions
The magnitude of the utilization of integrated community case management was low in the study area. Mother’s/Caregiver’s education of secondary and above, having good knowledge on childhood illness, history of the previous visit to health post, short distance to health post and perceived high severity of disease and presence of cough were factors significantly determining service utilization.
Recommendations
According to the finding of the result, the following recommendations are forwarded:
- The zonal health department should promote integrated community case management through mass media, leaflets and different medias.
- Zonal health department and Woreda health office should begin collaboration with locally available mass media to increase the awareness of mothers/caregivers towards availability of integrated case management service at health post and strengthen mobilization of community using health development army to utilize the service.
- The zonal health department and Woreda health office should avail health posts for those far away or travel more than an hour to reach health posts.
- Woreda health office should strengthen health education and IEC/BBC strategies in health facilities to increase knowledge of mothers/caregivers on danger signs and causes of childhood illness.
- Health extension workers should provide health education of mothers/caregivers on recognition of complications of common childhood illness to give equal emphasis for all signs and symptoms of childhood illness and the advantages of taking treatment immediately or before the illness becomes severe.
- Health extension workers also should be compassionate, respectful while caring for the clients who visit health posts for their sick children.
Operational Definitions
iCCM service utilization: The proportion of sick children aged between 2 and 59 months who received treatment or consultation and/or referral for one of the complaints; cough, fever, and diarrhea from the health post after mother/caregiver took a sick child to the health post in the first place within two weeks prior to the study period.
Caregiver: This is a person who is responsible for taking care of a child and age 18 years and above; can be the mother/father or the relative of the child.
Good Knowledge of mothers/caregivers on danger signs and causes of childhood illness: respondents who scored above or equal to the mean in knowledge questions were labeled as having good knowledge and those scoring below the mean were labeled as poor knowledge.11
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; AIDS, acquired immuno-deficiency syndrome; WHO, World Health Organization; UNICEF, United Nations International Children Emergency Fund; iCCM, integrated community case management; HP, health post; SNNPR, Southern Nation Nationalities and Peoples Region; SPSS, Statistical Package for Social Sciences; SD, standard deviation; HEW, health extension worker; IEC, information education and communication; BBC, behavioral change communication.
Data Sharing Statement
Additional files can be received via email by contacting [email protected].
Acknowledgment
We would like to appreciate the managers of health center, study participant and data collectors for their cooperation.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. All authors reviewed and agreed on the final manuscript for publication.
Funding
Authors received no fund for this study.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Inter-agency Group for Child Mortality Estemation. Levels and trends in child mortality: 2–36; 2015. Available from: www.who.int/maternalchildadolescentlevelstrendschildmortality2015/en/.
2. Victora C, Requejo J, Barros A, et al. Countdown to 2015: a decade of tracking progress for maternal, newborn, and child survival. Lancet. 2015.
3. Ethiopia, FMOH. Health and health-related indicators 2004 EFY (2011/2012); 2014. Available from: https://www.dktethiopia.org/sites/default/files/PublicationFiles/Health%20and%20Health%20Related20Indicators202004%20E.C.pdf.
4. WHO. World health statistics; Switzerland, Geneva; 2012. Available from: https://www.google.com/search?q=WHO.%202012.%2d%20health%20statistics;%20Switherland,%20Geneva.
5. Diaz T, Aboubaker S, Young M. Current scientific evidence for integrated community case management (iCCM) in Africa: findings from the iCCM Evidence Symposium. J Glob Health. 2014;4(2).
6. Ethiopia, FMOH. National implementation plan for community based management; 2010. Available from: https://www.unicef.org/ethiopia/FMOHPolicyPracticeBulletinApril14.pdf.
7. Philip D, Hamer DH, Iyer H. Impact of integrated community case management on health-seeking behavior in Rural Zambia. Am J Trop Med Hyg. 2012;87:105–110. doi:10.4269/ajtmh.2012.11-0799
8. Van der P, Sorensen SC, Delgado E, Bocaletti E. Health seeking behaviour for child illness in rural Guatemala. Trop Med Int Health. 2006;1:161–170.
9. Muhumuza G, Mutesi C, Mutamba F, Ampuriire P, Nangai C. Acceptability and utilization of community health workers after the adoption of the integrated community case management policy in Kabarole District in Uganda. iMedPub J. 2015;2(11).
10. ESHE(Essential Service for Health of Ethiopia). End-line household survey report: Southern Nation, Nationalities, and Peoples of Ethiopia, Hawassa; 2008. Available from: http://www.jsi.com/JSIInternet/Inc/Common/_download_pub.cfm?id=13205&lid=3.
11. Demissie B, Ejie B, Zerihun H, et al. Assessment of healthcare seeking behavior of caregivers for common childhood illnesses in Shashogo Woreda, Southern Ethiopia. Ethiopia Med J. 2014.
12. Bryan S, Amouzou A, Miller NP, et al. Determinants of utilization of health extension workers in the context of scale-up of integrated community case management of childhood illnesses in Ethiopia. Am J Trop Med Hyg. 2015;93(3):636–647. doi:10.4269/ajtmh.14-0660
13. Taffa N, Chepngeno G. Determinants of health care seeking for childhood illnesses in Nairobi slums. Trop Med Int Health. 2005;10(3):240–245. doi:10.1111/j.1365-3156.2004.01381.x
14. Ethiopia, FMOH. Health Sector Transformation Plan (2015/16–2019/20). 2017.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.