Back to Journals » Clinical Ophthalmology » Volume 8
Utility of Heidelberg retinal tomography as a screening tool for analyzing retinal nerve fiber layer defects
Authors Belyea D ![]() , Alhabshan R, Mahesh S, Gertner G, Ibisevic M, Habib A, Dan J
, Alhabshan R, Mahesh S, Gertner G, Ibisevic M, Habib A, Dan J
Received 28 April 2014
Accepted for publication 31 July 2014
Published 28 November 2014 Volume 2014:8 Pages 2409—2414
DOI https://doi.org/10.2147/OPTH.S66898
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
David A Belyea, Rashed N Alhabshan, Sankaranarayana P Mahesh, Gregory S Gertner, Mirsad M Ibisevic,† Abdullah S Habib, Jacob A Dan
Department of Ophthalmology, The George Washington University, Washington, DC, USA
†Dr Mirsad Ibisevic passed away on January 4, 2013
Context: Although Heidelberg retinal tomography (HRT)-generated topographic images have been studied extensively for the detection of retinal nerve fiber layer (RNFL) defects, little is known about the role of HRT-generated surface reflectivity images in the detection of RNFL defects in either patients with glaucoma or glaucoma suspects.
Aims: To evaluate the effectiveness of HRT version II (HRT II) optic nerve reflectivity images in uncovering RNFL defects in an outpatient population evaluated for glaucoma.
Study design/materials and methods: In 102 consecutive eyes from 60 patients evaluated for glaucoma in an academic-based practice, HRT II optic nerve images were prospectively imaged and compared with clinical optic nerve exam techniques to see if HRT II was able to detect RNFL defects overlooked in clinical practice.
Results: Nine eyes (8.8%) were found to have RNFL defects recognized by screening with HRT II. Of these nine eyes, eight (88.9%) were recognized to demonstrate RNFL defects by conventional examination techniques. One additional eye had an RNFL defect seen on physical exam that was not detected by HRT.
Conclusion: In academic practice, HRT II may be helpful in complementing conventional exam techniques in the recognition and documentation of acquired RNFL loss.
Keywords: HRT, RNFL defect, optic nerve, glaucoma, glaucoma suspect
Introduction
Glaucoma is a disease process in which there is a progressive loss of the retinal ganglion cells resulting in characteristic optic atrophy and visual field loss.1 Early identification of individuals with glaucoma is important to initiate timely treatment and prevent vision loss, as glaucomatous damage is irreversible.2 The diagnosis of glaucoma depends on intraocular pressure measurements, visual field analysis, and, most importantly, reliable optic nerve head evaluations.3 Evaluating structural changes in optic nerve head and retinal nerve fiber layer (RNFL) as well as functional monitoring of progressive visual field changes are employed in assessing ongoing glaucomatous damage.4
A number of imaging devices, including Heidelberg retinal tomography (HRT) (versions I, II, and III) (Heidelberg Engineering, Germany), optical coherence tomography, and GDx scanning laser polarimetry, have been developed with the objective to reliably measure and follow structural changes in optic nerve head or the thickness of RNFL.5 HRT, one such imaging modality, uses a confocal scanning laser to image serial sections of optic nerve to create a map of topographical sections of optic nerve head and surrounding retina. HRT, based on the surface reflectivity pattern, also has the ability to detect changes in, or localized loss of, RNFL, though this has not been studied extensively. Burk et al6 showed that surface reflectivity images by HRT II can yield information on the loss of RNFL while evaluating patients with glaucoma.
In this study we sought to evaluate the utility of HRT II surface reflectivity images in an academic referral practice. The aim of this study was to explore 1) the ability of HRT II in quantitative detection of RNFL defects in glaucoma suspects as well as patients with glaucoma as compared with clinical examination and 2) whether the RNFL defects detected correlate with functional changes in visual function.
Materials and methods
Enrollment of patients
This was a retrospective comparative study. The study was approved by the Institutional Review Board at the George Washington University, and all procedures followed were in accordance with the ethical standards of the Helsinki Declaration of 1975. The study was performed in an academic-based glaucoma practice clinic. One hundred and two eyes from 60 consecutive patients aged >18 years who were following up with the glaucoma clinic at our institution and who were willing to participate were included in the study. Patients enrolled in the study included those with a diagnosis of glaucoma or those followed as glaucoma suspects. Glaucoma was defined as a diagnosis of primary open angle glaucoma that was made when there was definite evidence of tissue damage or visual function loss related to glaucoma. Diagnosis of glaucoma suspects was based on signs of cup to disc ratio asymmetry or symmetrically large physiologic cup with presumed predisposition because of a risk factor such as elevated intraocular pressure, positive family history of glaucomatous visual field loss, pigment dispersion syndrome, hyperopia, myopia, or the presence of a gene known to be associated with glaucoma. Patients with pupils <2.5 mm; pathological myopia; congenital ocular or optic nerve anomalies; anomalies with concurrent ocular disorders that interfere with imaging, including cataract; and corneal scarring were excluded. Any patients with vitreoretinal disorders including vascular occlusions and optic neuropathy were also excluded. Patients with disc areas <1.00 mm or >3.00 mm on HRT imaging were also not included in the study.
All patients underwent a complete eye examination including slit lamp biomicroscopy of the ocular surface and anterior segment, gonioscopy, dilated fundus examination with a +78D/20D lens, as well as disc stereo photography.
All patients underwent clinical evaluation prior to imaging studies. Two experienced clinicians (DAB, JAD) evaluated in a masked fashion for presence of RNFL defects based on clinical examination as well as fundus stereophotographs. In addition, optic and RNFL analysis with HRT II was performed by experienced clinicians (MMI, ASH) to evaluate the presence of any RNFL defects. HRT II measures the surface of the optic disc and peripapillary retina and then estimates the retinal thickness as an indirect measurement of the nerve fiver layer, as described previously.7,8 In short, the instrument performs A-scan in 32 focal planes, constructs a three-dimensional map, and displays the information as two images: a topographical image and a reflectivity image. Each HRT II scan includes a three-scan series of a 10×10° frame and creates a composite image with a reference plane for data analysis. The mean topography of the three series was used for the analysis, and the contour line of the optic disc edge drawn by an experienced technician was used. RNFL defect dimensions, including the smallest and largest width along with the height, were measured using the scale provided by the HRT II reflectivity image, and the area of the defect was approximated into an isosceles trapezoid shape and calculated in mm2. The area of defect was converted to the average retinal arterial width by dividing the calculated area by the square of the average width of the imaged retinal arteriole (0.1912 mm2).
All patients underwent standard 24-2 or 30-2 achromatic Humphrey visual field analysis (Carl Zeiss Meditec, Germany) with an SITA (Swedish interactive threshold algorithm) standard or full threshold protocol. A reliable visual field test was defined as one with <10% false positive response, <5% false negatives, and <20% fixation losses. A retrospective chart review was performed to collect the demographic details as well as current Humphrey visual field analysis. Student’s t-test statistical analyses were performed using IBM SPSS® Statistics version 19.0 (IBM Corporation, Armonk, NY, USA).
Results
A total of 102 eyes (with glaucoma n=40, glaucoma suspect n=62) from 60 patients were evaluated for detection of RNFL defects with HRT II and compared with physical exam. The demographic details of the patient population are given in Tables 1 and 2. The mean cup to disc ratio was higher in the patients with glaucoma as compared with those with suspicion of glaucoma (P=0.04). Similarly, the corrected pattern standard deviation was higher in patients with glaucoma as compared with glaucoma suspects (P=0.03).
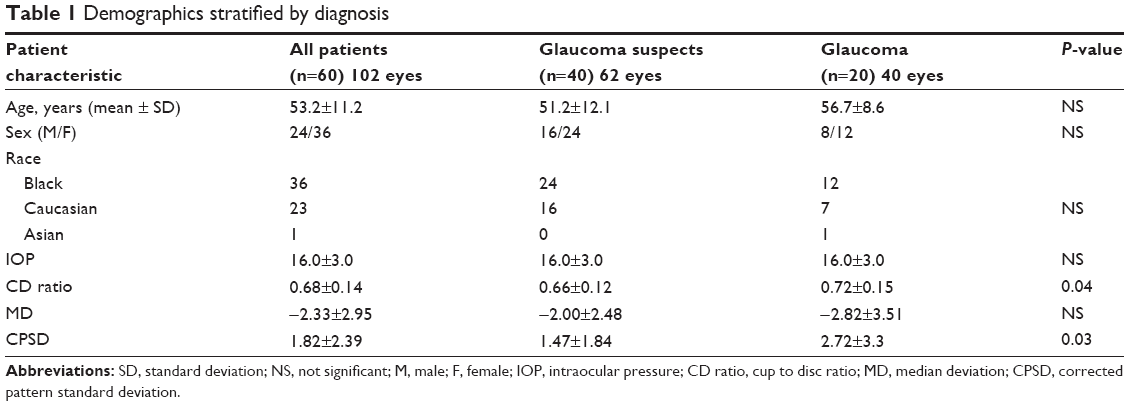 | Table 1 Demographics stratified by diagnosis |
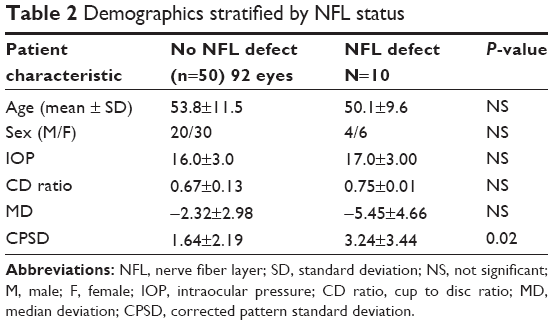 | Table 2 Demographics stratified by NFL status |
Nine eyes (8.8%) were found to have RNFL defects by HRT II surface reflectivity image, glaucoma = five eyes and glaucoma suspects = four eyes (see Table 3). Of these nine eyes, eight were recognized to demonstrate NFL defects by physical examination. In addition, one RNFL defect was observed by clinical examination on one eye that was not detected by HRT II.
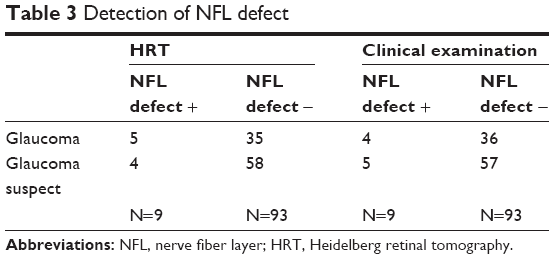 | Table 3 Detection of NFL defect |
The smallest width noted ranged from 1.31 mm to 2.62 mm while the largest width ranged from 2.62 mm to 9.93 mm. The mean area of RNFL defect detected in the nine patients by HRT II was 23.60±9.82. Visual field defects were detected in five of nine patients who had RNFL defect seen with HRT II. There was no correlation between the areas of the RNFL defects with presence of visual field defects (22.68 in patients with visual field defects vs 24.75 in patients with no visual field defects). Patients with corresponding visual field losses had lower mean deviation (−8.6 vs −1.3) and higher corrected pattern standard deviation values (8.11 vs 2.02) than those with no visual field defects (see Tables 4 and 5).
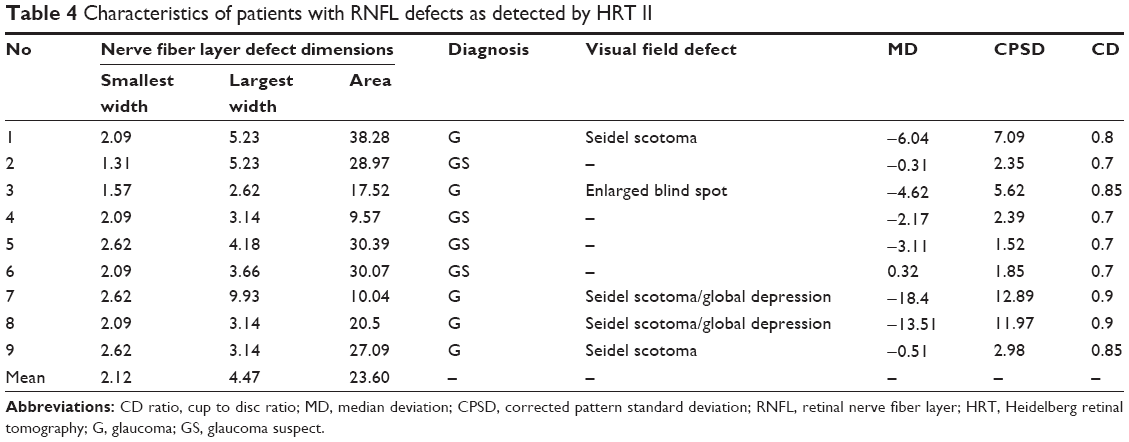 | Table 4 Characteristics of patients with RNFL defects as detected by HRT II |
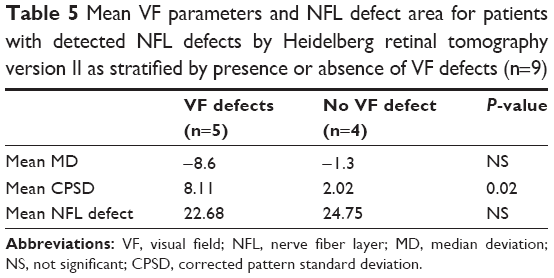 | Table 5 Mean VF parameters and NFL defect area for patients with detected NFL defects by Heidelberg retinal tomography version II as stratified by presence or absence of VF defects (n=9) |
Discussion
Diagnostic tools such as HRT have been used for community screening of patients with glaucoma to allow early diagnosis and treatment. HRT II has conventionally used optic nerve head topographic parameters as well as indirect assessment of retinal RNFL thickness to follow progression in glaucoma patients.7 Though widely used in clinical practice, RNFL thickness is indirectly assessed by HRT software based on assumption of an arbitrary reference plane located 50 microns posterior to the retinal surface at the papillomacular bundle, contributing to lower diagnostic accuracy.9
When used in the conventional manner evaluating structural optic disc changes, the sensitivity of HRT in diagnosing glaucoma in different studies has ranged from 57% to 94% and has been associated with high false positives.10,11 In this study we sought to evaluate the utility of HRT II as a screening tool in the detection of RNFL defects using surface reflectivity in a patient population with documented glaucoma or who were suspected to have glaucoma (see Figure 1). Although it is well known that HRT II can also detect RNFL loss seen with early glaucomatous damage, based on changes in surface reflectivity, review of literature suggests that this has not been well studied.
 | Figure 1 Heidelberg retinal tomography version II surface reflectivity image showing nerve fiber layer defects (arrows). |
In this study, based on surface reflectivity pattern, HRT II imaging was comparable and showed good concordance with a focused clinical examination in detection of RNFL defects. We observed that HRT II had a sensitivity of 88.8% and a specificity of 98.9% compared with physical examination in detecting focal RNFL defects in a population with documented glaucoma or who were suspected to have glaucoma. In addition, HRT II and physical exam conjointly yielded the highest number of recognizable RNFL defects in an academic referral glaucoma population. In a previous study, Burk et al6 explored the use of surface reflectivity images in a series of 12 patients with documented nerve fiber loss seen on optic disc photography, and showed a much lower detection rate of 75% with HRT II.
In our case series, all five patients who showed visual field defects revealed the presence of RNFL loss on HRT II. No correlation was seen between the size of RNFL defects and visual field defect parameters such as mean deviation or corrected pattern standard deviation. Since most of the patients in our study population had less advanced visual field changes, as reflected by lower mean deviation values, it is likely that our series may be having localized or less advanced nerve fiber layer loss. It has been shown in previous studies that 40%–50% of nerve fiber is lost prior to detection of visual field changes and often occurs earlier by as much as 5 years.12 If RNFL loss is a predictor of future field defects, assessment of RNFL defects may have greater specificity than evaluation of disc changes in glaucoma suspect eyes as well as in monitoring patients who already show RNFL defects. Another interesting fact observed was that glaucoma suspects with RNFL defects were significantly younger than the glaucoma patients with RNFL loss.
There are several limitations to our study. First, all our patients were from a tertiary academic practice, where most of the patients were referred, and may not reflect a community-based screening population. Differences in sensitivities and specificities for glaucoma testing have been shown to vary between institutional settings and mass screening environments.13 Secondly, we had a small sample size with less advanced visual field defects. Future studies looking at long-term follow-up of these patients looking for any progressing of these defects and correlation with visual field changes will be helpful. Further, we are planning on including patients with early as well as advanced glaucoma and a larger sample size in future studies.
Conclusion
In summary, we evaluated the utility of HRT II in assessing and documenting acquired RNFL loss in glaucoma or glaucoma suspect patients, and hence it can be used as a screening tool for identifying potential patients for further workup.
In an academic practice, HRT may be helpful in complementing conventional examination techniques in the recognition and documentation of acquired RNFL loss. HRT and a focused examination conjointly yielded the highest number of recognizable RNFL defects.
Acknowledgment
This article is dedicated to the memory of Mirsad Ibisevic, an energetic thinker, consummate scientist, dedicated ophthalmologist, and accomplished oil painter. Dr Ibisevic was deeply respected by his patients and colleagues and he is sadly missed by those he touched with his kindness and expertise.
Disclosure
The authors report no conflicts of interest in this work.
References
King AJW, Bolton N, Aspinall P, O’Brien CJ. Measurement of peripapillary retinal nerve fiber layer volume in glaucoma. Am J Ophthalmol. 2000;129(5):599–607. | ||
Sharma P, Sample PA, Zangwill LM, Schuman JS. Diagnostic tools for glaucoma detection and management. Surv Ophthalmol. 2008; 53(6 Suppl):S17–S32. | ||
Schumann J, Orgül S, Gugleta K, Dubler B, Flammer J. Interocular difference in progression of glaucoma correlates with interocular differencesn retrobulbar circulation. Am J Ophthalmol. 2000;129(6):728–733. | ||
Kass MA, Heuer DK, Higginbotham EJ, et al. The ocular hypertension treatment study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):701–713. | ||
Nucci C, Mancino R, Martucci A, et al. 3-T diffusion tensor imaging of the optic nerve in subjects with glaucoma: correlation with GDx-VCC, HRT-III and stratus optical coherence tomography findings. Br J Ophthalmol. 2012;96(7):976–980. | ||
Burk ROW, Tuulonen A, Airaksinen PJ. Laser scanning tomography of localised nerve fibre layer defects. Br J Ophthalmol. 1998;82(10): 1112–1117. | ||
Zangwill LM, Chan K, Bowd C, et al. Heidelberg retina tomograph measurements of the optic disc and parapapillary retina for detecting glaucoma analyzed by machine learning classifiers. Invest Ophthalmol Visual Sci. 2004;45(9):3144–3151. | ||
Weinreb RN, Lusky M, Bartsch DU, Morsman D. Effect of repetitive imaging on topographic measurements of the optic nerve head. Arch Ophthalmol. 1993;111(5):636–638. | ||
Zangwill LM, Bowd C, Berry CC, et al. Discriminating between normal and glaucomatous eyes using the Heidelberg retina tomograph, GDx nerve fiber analyzer, and optical coherence tomograph. Arch Ophthalmol. 2001;119(7):985–993. | ||
Robin TA, Müller A, Rait J, Keeffe JE, Taylor HR, Mukesh BN. Performance of community-based glaucoma screening using frequency doubling technology and Heidelberg retinal tomography. Ophthalmic Epidemiol. 2005;12(3):167–178. | ||
Healey PR, Lee AJ, Aung T, Wong TY, Mitchell P. Diagnostic accuracy of the Heidelberg retina tomograph for glaucoma: a population-based assessment. Ophthalmology. 2010;117(9):1667–1673. | ||
Sommer A, Katz J, Quigley HA, et al. Clinically detectable nerve fiber atrophy precedes the onset of glaucomatous field loss. Arch Ophthalmol. 1991;109(1):77–83. | ||
Maul EA, Jampel HD. Glaucoma screening in the real world. Ophthalmology. 2010;117(9):1665–1666. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.