Back to Journals » OncoTargets and Therapy » Volume 8
Use of transient elastography to predict de novo recurrence after radiofrequency ablation for hepatocellular carcinoma
Authors Lee SH, Kim SU ![]() , Jang JW, Bae SH, Lee S, Kim BK, Park JY, Kim DY
, Jang JW, Bae SH, Lee S, Kim BK, Park JY, Kim DY ![]() , Ahn SH, Han K
, Ahn SH, Han K
Received 28 September 2014
Accepted for publication 1 December 2014
Published 2 February 2015 Volume 2015:8 Pages 347—356
DOI https://doi.org/10.2147/OTT.S75077
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jianmin Xu
Sang Hoon Lee,1 Seung Up Kim,1–3 Jeong Won Jang,4 Si Hyun Bae,4 Sanghun Lee,1,3 Beom Kyung Kim,1–3 Jun Yong Park,1–3 Do Young Kim,1–3 Sang Hoon Ahn,1–3 Kwang–Hyub Han1–3
1Department of Internal Medicine, 2Institute of Gastroenterology, Yonsei University College of Medicine, 3Liver Cirrhosis Clinical Research Center, 4Department of Internal Medicine, College of Medicine, Catholic University of Korea, Seoul, Korea
Background/purpose: Liver stiffness (LS) measurement using transient elastography can accurately assess the degree of liver fibrosis, which is associated with the risk of the development of hepatocellular carcinoma (HCC). We investigated whether LS values could predict HCC de novo recurrence after radiofrequency ablation (RFA).
Methods: This retrospective, multicenter study analyzed 111 patients with HCC who underwent RFA and LS measurement using transient elastography between May 2005 and April 2011. All patients were followed until March 2013 to monitor for HCC recurrence.
Results: This study included 76 men and 35 women with a mean age of 62.4 years, and the mean LS value was 21.2 kPa. During the follow-up period (median 22.4 months), 47 (42.3%) patients experienced HCC de novo recurrence, and 18 (16.2%) died. Patients with recurrence had significantly more frequent liver cirrhosis, more frequent history of previous treatment for HCC, higher total bilirubin, larger spleen size, larger total tumor size, higher tumor number, higher LS values, and lower platelet counts than those without recurrence (all P<0.05). On multivariate analysis, together with previous anti-HCC treatment history, patients with LS values >13.0 kPa were at significantly greater risk for recurrence after RFA, with a hazard ratio (HR) of 3.115 (95% confidence interval [CI], 1.238–7.842, P<0.05). Moreover, LS values independently predicted the mortality after RFA, with a HR of 9.834 (95% CI, 1.148–84.211, P<0.05), together with total bilirubin.
Conclusions: Our data suggest that LS measurement is a useful predictor of HCC de novo recurrence and overall survival after RFA.
Keywords: hepatocellular carcinoma, radiofrequency ablation, recurrence, liver stiffness, fibroscan
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common malignancy worldwide, and it is also a common cause of death in patients with chronic liver disease.1 The curative treatment options for HCC that are currently available are surgical resection, liver transplantation, and radiofrequency ablation (RFA).2 Among these options, RFA has been accepted as an effective nonsurgical curative treatment modality for early-stage HCC tumors (solitary tumors <5 cm in diameter or fewer than three nodules <3 cm in diameter.2,3 RFA achieves a satisfactory local response rate, with more than 80% complete ablation in most studies.4 Several recent randomized controlled trials and repeated meta-analyses have shown that the rates of overall survival (OS) and recurrence-free survival after RFA are comparable with those after surgical therapy.4,5
Despite progressive improvements in the efficacy of RFA, the survival of patients with HCC who undergo RFA remains disappointing, mainly due to frequent intrahepatic recurrence of HCC after RFA.4 The cumulative recurrence rate 2–3 years after RFA has been reported at 72%–80%.6,7 There are two types of intrahepatic recurrence of HCC after RFA: local tumor progression and de novo recurrence. Local tumor progression, known as local recurrence, results from direct dissemination of the original tumor along the peripheral margin of the ablated lesion, while de novo recurrence accounts for multicenter occurrence of a HCC tumor in a location remote from the ablated lesion.8 Local factors, which include tumor location, tumor numbers, direct invasion into vessels, and insufficient safety margins have been identified as significant predictors of local recurrence,6,7,9 whereas the necroinflammatory activity of hepatitis and the degree of liver fibrosis or cirrhosis have been shown to be significantly associated with de novo recurrence.10
The clinical role of transient elastography (TE) to measure liver stiffness (LS) has been widely investigated in assessment of the degree of liver fibrosis or identification of the presence of portal hypertension.11 In addition, several recent longitudinal studies proposed that TE can accurately predict HCC development in patients with chronic hepatitis B and C,12,13 and HCC recurrence after curative resection,14 based on the significant correlation between the risk of HCC development and the degree of liver fibrosis.11
Therefore, in this study we investigated whether the degree of liver fibrosis assessed by performing TE could predict de novo recurrence in patients with HCC who received RFA with complete ablation.
Material and methods
Patients
Between May 2005 and April 2011, a total of 2,168 patients received RFA for HCC treatment. Of these, 139 patients with available LS values at least within 3 months (median 7 [range, 0–78] days) prior to RFA were selected for the multicenter retrospective study. A further 28 patients were excluded based on our exclusion criteria (Figure 1). Especially because TE measures LS values at right hepatic lobe, patients with a history of right hepatectomy before enrollment were excluded. Finally, 111 patients (55 from Yonsei University and 56 from Catholic University) were included in the final statistical analysis. The study protocol conformed to the ethical guidelines of the 1975 Helsinki Declaration and was approved by the institutional review board of each institute.
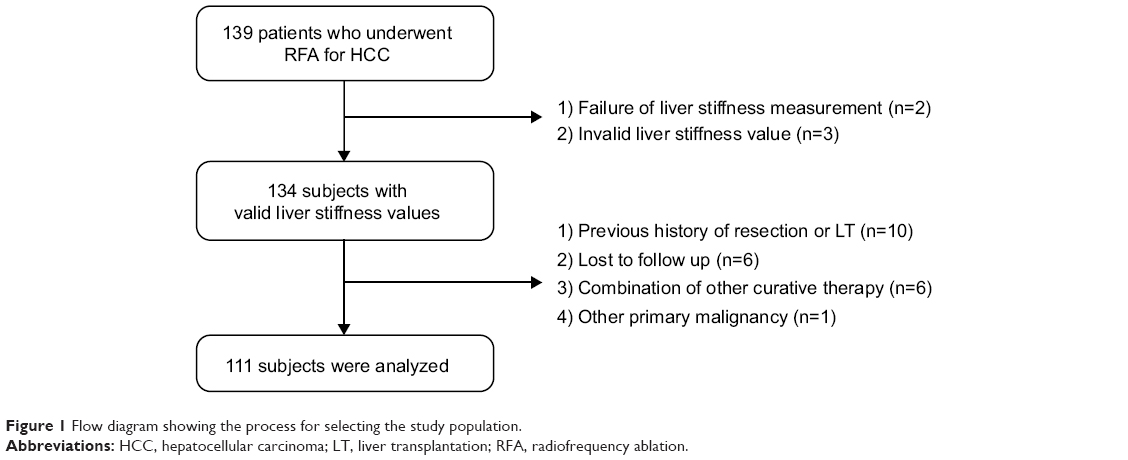 | Figure 1 Flow diagram showing the process for selecting the study population. |
Since this study was focused on whether TE could predict HCC de novo recurrence after RFA,15 15 patients who experienced local recurrence were excluded from the final analysis.
Diagnosis of HCC and liver cirrhosis
The diagnosis of HCC was based on dynamic imaging studies, biopsies, and alpha-fetoprotein (AFP) serology, according to the American Association for the Study of Liver Diseases guidelines.2 Before RFA, the size and number of HCC tumors were confirmed by performing imaging studies, including computed tomography (CT) or magnetic resonance imaging (MRI). The staging of HCC before RFA and recurrent HCC was assessed by using the Barcelona Clinic Liver Cancer (BCLC) staging system.16
If histologic information was not available, liver cirrhosis was clinically diagnosed as follows: (1) platelet count <100,000/μL and ultrasonographic findings suggestive of cirrhosis, including a blunted, nodular liver edge, accompanied by splenomegaly (>12 cm); (2) esophageal or gastric varices; or (3) overt complications of liver cirrhosis, including ascites, variceal bleeding, and hepatic encephalopathy.17
Data collection
Demographic, clinical, and laboratory data of the study population were collected from electronic medical records and were reviewed retrospectively. At admission, 1 day before RFA, blood parameters, including platelet count, total bilirubin, serum albumin, creatinine, prothrombin time, aspartate aminotransferase (AST), alanine aminotransferase (ALT), AFP, and des-gamma carboxyl prothrombin (DCP) were recorded. Because aspartate-to-platelet ratio index (APRI) can be easily obtained at no additional cost, it was calculated on the day before RFA, and its ability to predict recurrence was compared with the predictive utility of TE.18
Liver stiffness measurement
Only one experienced technician at each institute, who had performed at least 1,000 prior examinations and who was blind to the patients’ clinical data, was allowed to perform TE. The results were reported in kilopascals. The interquartile range (IQR) was defined as an index of intrinsic variability of LS values, corresponding to the interval of LS results containing 50% of the valid measurements between the 25th and 75th percentiles.19 The median value of successful measurements was selected to represent the LS value in a given patient. In this study, only LS examinations with at least ten validated measurements, an IQR-to-median ratio less than 0.3, and a success rate of at least 60% were considered reliable.14
Radiofrequency ablation
RFA was performed either by an interventionist, percutaneously (n=107 [96.4%]), or by a surgeon, in an intraoperative setting (n=4 [3.6%]). Dynamic CT was routinely performed immediately after RFA, and a subsequent session of RFA was performed when the postprocedural CT revealed that the target lesion was not completely ablated. Procedure-related complications were also checked. Most patients (n=109 [97.3%]) achieved complete ablation after one RFA session, whereas the others (n=2 [2.7%]) received two RFA sessions for complete ablation.
Follow up and recurrence
After discharge, patients underwent follow-up exams 1 month after RFA and every 3 months thereafter. Follow-up investigations included measurement of tumor markers (AFP and DCP) and imaging studies, including liver dynamic CT or MRI, for the detection of recurrence. The last follow-up date was March 31, 2013, and the median follow-up duration was 22.4 (range, 1.1–77.3) months.
The de novo recurrence was defined as intrahepatic recurrence beyond the ablative margin, which was suggested to be the 0.5–1.0 cm – wide region that should ideally be ablated during RFA.8 The primary end point was recurrence-free survival, which was defined as the period between the date of RFA and the time of the first de novo recurrence detected by performing follow-up imaging studies, and the secondary end point was overall mortality.
Statistical analysis
Data were expressed as the mean ± standard deviation (SD), median (range), or n (%), as appropriate. Variables were compared by using the chi-square test (or Fisher’s exact test) for categorical data and Student’s t-test (or the Mann–Whitney U-test) for continuous variables. The cumulative incidence rates of recurrence were calculated by using the Kaplan–Meier method. To identify independent risk factors for recurrence, multivariate Cox proportional hazard regression analysis was performed, using the variables that were significant in the univariate analysis. To prevent statistical error due to significant correlation between liver cirrhosis and LS values, multivariate analysis used LS values for grading liver fibrosis. Hazard ratios (HR) and corresponding 95% confidence intervals (CI) also were indicated. A two-tailed P-value <0.05 was considered to be statistically significant. The statistical analysis was performed with SPSS, version 18.0 (PASW Statistics Inc., Chicago, IL, USA).
Results
Baseline characteristics
The baseline characteristics of the 111 enrolled patients are summarized in Table 1. The patient population consisted of 76 men and 35 women, with a mean age of 62.4 years. Hepatitis B virus (HBV) (n=71 [64.0%]) was the most common etiology of underlying liver disease. A total 75 (67.6%) patients had liver cirrhosis,13 and most of these (65 [86.7%]) patients had preserved liver function, of Child–Pugh class A. Among patients with HBV, 53 (74.6%) patients received antiviral therapy using nucleos(t)ide analogs according to a Korean guideline.20 Among patients with Hepatitis C virus (HCV), three (15.8%) patients received antiviral treatment using pegylated interferon plus ribavirin before RFA. Of these, one patient experienced sustained virological response. Additionally, HCV eradication was achieved in two (10.5%) patients after RFA. However, the other (n=14 [73.7%]) patients with HCV could not receive antiviral treatment due to advanced cirrhosis with pancytopenia, old age, or significant thyroid dysfunction.
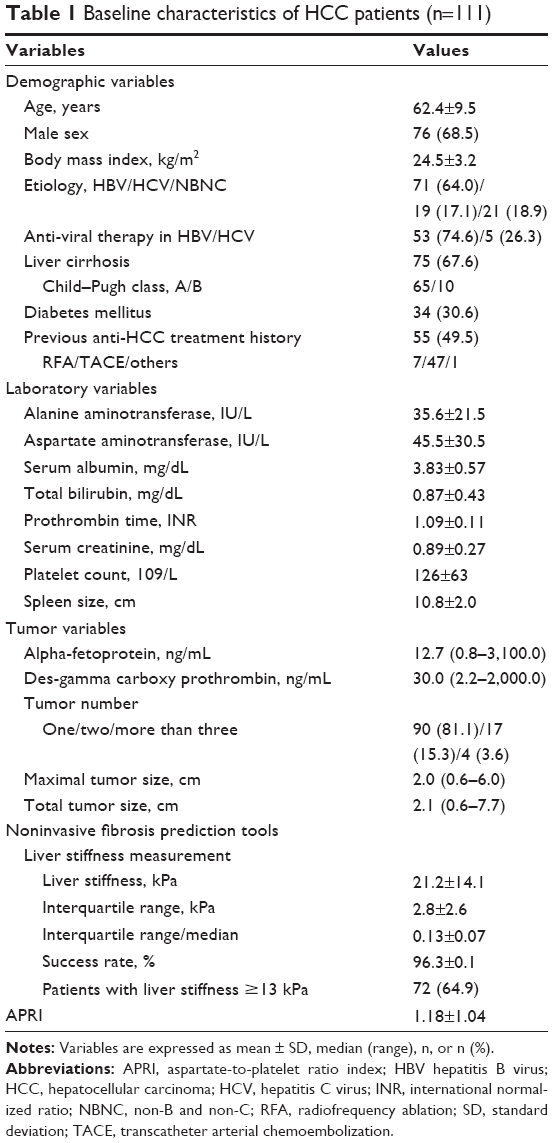 | Table 1 Baseline characteristics of HCC patients (n=111) |
A total of 55 patients (49.5%) had been treated previously by other noncurative modalities, including transcatheter arterial chemoembolization (TACE) (n=47), followed by RFA (n=7). The median maximal tumor size was 2.0 cm, and most tumors (n=90 [81.1%]) were detected as solitary masses. The mean LS value was 21.2 kPa (median 17.6 [range, 4.4–75.0] kPa) and the mean APRI was 1.18±1.04 (median 0.86 [range, 0.19–6.90]).
The mean LS value according to the etiology of HCC was significantly different in our study: 18.6 kPa in HBV-related HCC (n=71 [64.0%]), 29.5 kPa in HCV-related HCC (n=19 [17.1%]), and 21.6 kPa in Non-B and non-C (NBNC)-related HCC (n=21 [18.9%]) (P=0.009 by one-way analysis of variance ANOVA, and P=0.006 especially between HBV-related HCC and HCV-related HCC by Bonferroni method).
Complication of RFA and clinical outcomes
Significant postprocedure complications occurred, including hepatic infarction (n=2), hepatic abscess (n=1), and biloma (n=1) (Table 2).21 All patients were managed appropriately, and none of the patients died of complications related to RFA.
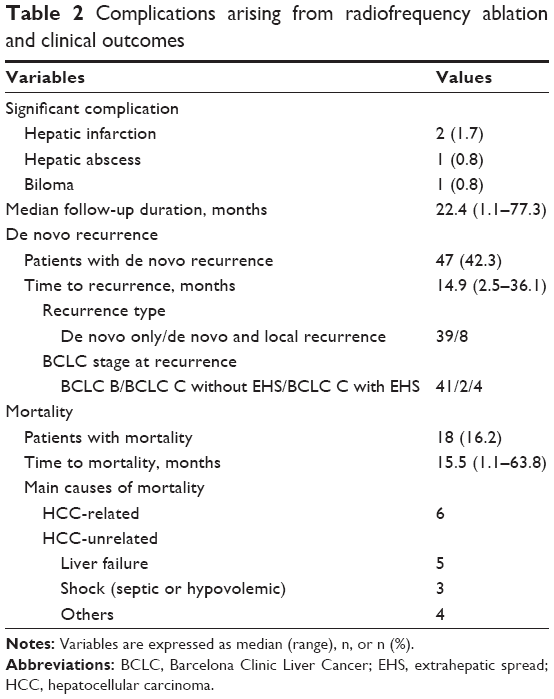 | Table 2 Complications arising from radiofrequency ablation and clinical outcomes |
Clinical outcomes of RFA are summarized in Table 2. The median follow-up duration was 22.4 (range, 1.1–77.3) months. During the study period, 47 (42.3%) patients experienced de novo recurrence, with a median time to recurrence of 14.9 (range, 2.5–36.1) months after RFA. Most de novo recurrence developed as BLCL stage B (n=41 [87.2%]). During the study period, 18 (16.2%) patients died, with a median time to overall mortality of 15.5 (range, 1.1–63.8) months.
Comparison between patients with and without recurrence
When the characteristics of patients with and without recurrence were compared (Table 3), patients with recurrence had significantly more frequent liver cirrhosis, more frequent history of previous treatment for HCC, higher total bilirubin, larger spleen size, larger total tumor size, higher tumor number, higher LS values, and significantly lower platelet counts than those without recurrence (all P<0.05). APRI score and tumor markers, including AFP and DCP, were not statistically different between the two groups (all P>0.05).
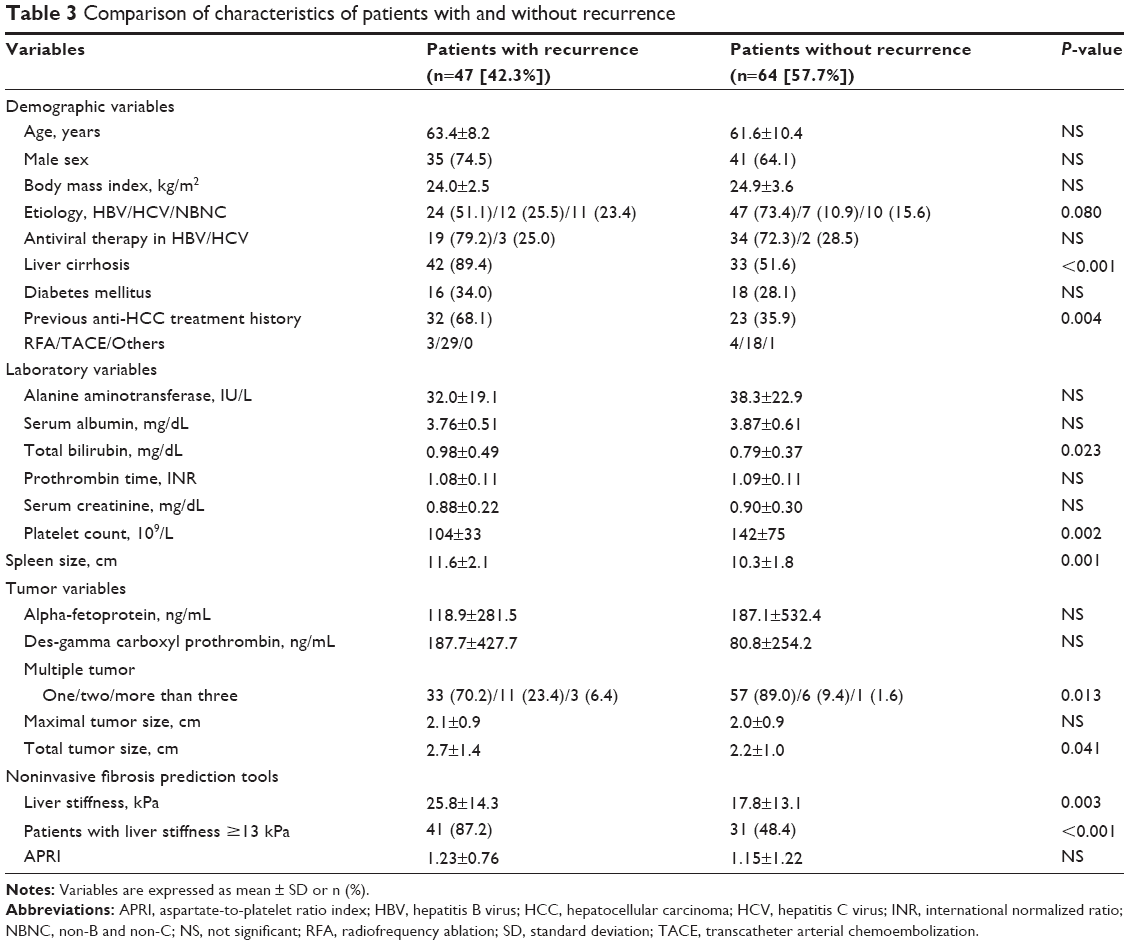 | Table 3 Comparison of characteristics of patients with and without recurrence |
For a simplified and intuitive analysis, we adopted 13.0 kPa as the optimal LS cutoff value to stratify our study population into high- and low-risk group for de novo recurrence.22 This cutoff value was similar to the calculated cutoff value from our cohort to predict de novo recurrence (13.4 kPa; sensitivity, 87.2%; specificity, 54.7%).
Factors associated with recurrence
Univariate analysis found that a history of previous anti-HCC treatments, total bilirubin, platelet count, spleen size, and LS values ≥13.0 kPa were significantly associated with recurrence (Table 4). A significant correlation was identified between clinically diagnosed cirrhosis and LS values (P<0.001 by Spearman correlation). Thus, clinically diagnosed cirrhosis was not incorporated into multivariate analysis, to avoid the statistical redundancy with LS values, in spite of its statistical significance in univariate analysis (P=0.026). Subsequent multivariate analysis identified that together with a history of previous anti-HCC treatment, patients with LS values >13.0 kPa were at significantly greater risk for recurrence after RFA, with a HR of 3.115 (P<0.05; 95% CI, 1.238–7.842) compared with those with LS values ≤13.0 kPa (Table 4). The cumulative incidence rate of recurrence was significantly higher in patients with LS values ≥13.0 kPa compared with those with LS values <13.0 kPa (logrank test, P<0.001) (Figure 2). The cumulative incidence rates of recurrence at 1, 2, and 3 years were 33.4%, 64.9%, and 70.7%, respectively, in patients with LS values ≥13.0 kPa, whereas they were 5.8%, 17.4%, and 24.9%, respectively, in patients with LS values <13.0 kPa.
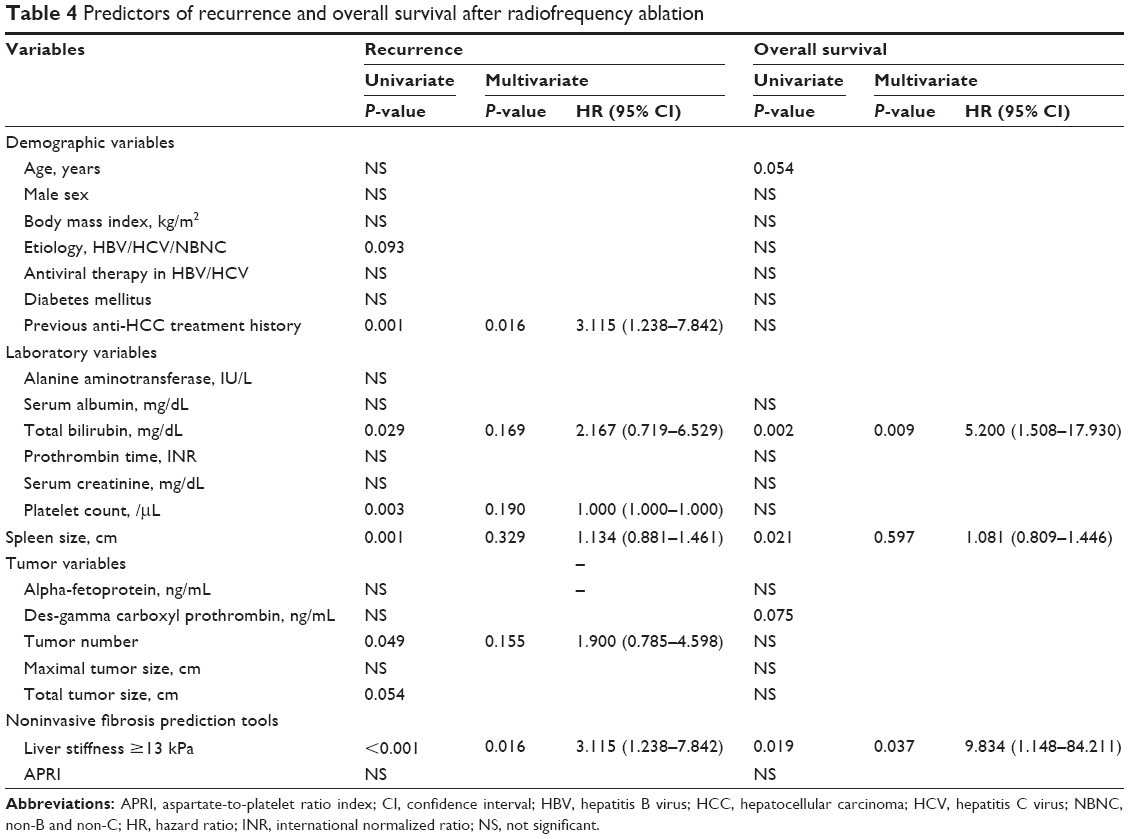 | Table 4 Predictors of recurrence and overall survival after radiofrequency ablation |
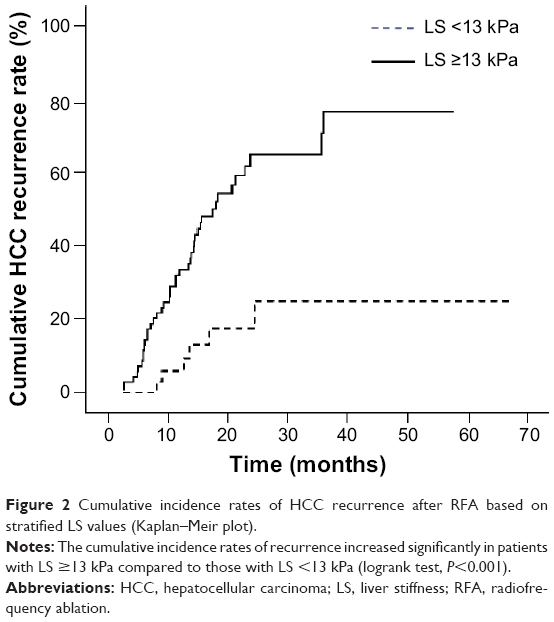 | Figure 2 Cumulative incidence rates of HCC recurrence after RFA based on stratified LS values (Kaplan–Meir plot). |
Approximately 25% of patients experienced recurrence despite having LS values <13.0 kPa, so a cutoff value that could identify low-risk patients was also calculated and found to be 9.6 kPa. The cumulative incidence rates of recurrence at 1, 2, and 3 years were 0%, 8.3%, and 8.3%, respectively, in patients with LS values <9.6 kPa. In addition, among patients with HBV-related HCC (n=71), recurrence was not significantly correlated with HBV DNA level (P=0.278) or anti-viral treatment (P=0.867). Similarly, recurrence was not correlated with HCV RNA level (P=0.552), antiviral treatment for HCV (P=0.129), or the achievement of sustained virological response (P=0.483) among patients with HCV-related HCC (n=19).
Factors associated with OS
On univariate analysis, total bilirubin, spleen size, and LS value >13.0 kPa significantly predicted OS after RFA (all P<0.05) (Table 4). Of these, LS values independently predicted OS after RFA, with a HR of 9.834 (P<0.05; 95% CI, 1.148–84.211), together with total bilirubin level (Table 4). The cumulative incidence rate of mortality was significantly higher in patients with LS values ≥13.0 kPa than in those with LS values <13.0 kPa (logrank test, P=0.002) (Figure 3). The cumulative incidence rates of mortality at 1, 2, and 3 years were 4.2%, 18.1%, and 33.3%, respectively, in patients with LS values ≥13.0 kPa, whereas no patients with LS values <13.0 kPa died during this period.
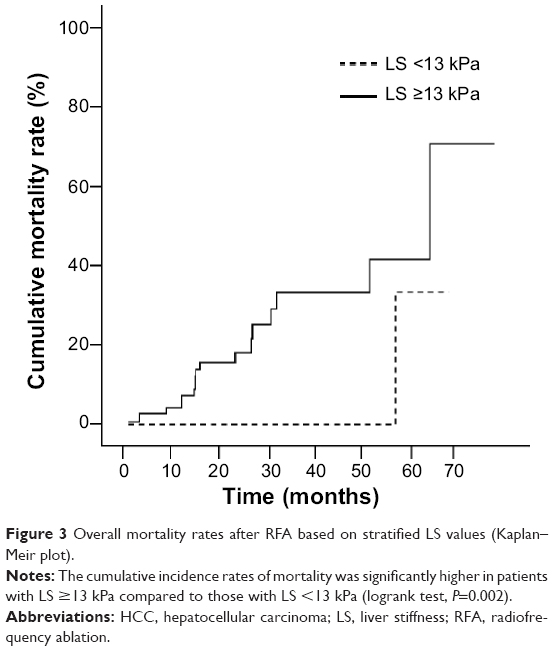 | Figure 3 Overall mortality rates after RFA based on stratified LS values (Kaplan–Meir plot). |
Discussion
In this multicenter study, we found that LS values measured by using TE were a significant predictor of HCC de novo recurrence and OS after RFA. To prevent potential confounding influences, we excluded patients who experienced only local tumor progression after RFA, which is associated with residual tumor cells and microscopic spread beyond the ablation margin.8 Although this study design allowed us to reveal the association between the risk of HCC de novo recurrence and the degree of liver fibrosis assessed by using TE, our results should be interpreted with caution because we cannot know at the time of RFA which patients will experience local recurrence. However, when we included the patients who experienced only local tumor recurrence after RFA during the same study period (n=19) and redefined our primary end point as overall recurrence, this time including both local and de novo recurrence, the independent prognostic value of TE was maintained, though there was attenuated statistical power (HR, 3.443–2.112 for overall recurrence; HR, 9.834–4.232 for overall mortality). Thus, further studies in a prospective setting that include all consecutive patients undergoing RFA are warranted to validate our results.
In our study, almost half of the patients (n=55 [49.5%]) had a previous history of local treatment, such as TACE or RFA, and previous anti-HCC treatment history was identified as an independent predictor of de novo recurrence, together with LS values. The exact mechanism is not clear, but this can be explained, in part, by altered tumor biology due to previous repeated local treatment, which can influence recurrence.23 There are other well-known risk factors for de novo recurrence after RFA that represent tumor burden or underlying liver function. These factors include AFP level,15,24,25 tumor size,24 multiplicity,25,26 presence of hepatitis,24 platelet counts,26 and serum albumin.26 However, these did not independently influence the risk of de novo recurrence in our study. This result might indicate that TE measures the degree of liver fibrosis, which is more closely related to the underlying liver function, leading to more sensitive predictions than the conventional parameters, such as platelet count, serum albumin level, or spleen size. Furthermore, although it has been recently proposed that some noninvasive fibrosis prediction indexes can predict recurrence after RFA,15 TE performed better than the well-known noninvasive fibrosis prediction index of APRI in our study. To prevent the confounding influence of underlying liver function, we proceeded with subgroup analysis for selected patients with Child–Pugh class A and found that LS values (P=0.029) and history of previous antitumor treatment (P=0.018) were also independently associated with the risk of de novo recurrence in multivariate analysis. However, because the sample size of our study was relatively small and the tumor burden of our study participants was relatively low (median AFP, 12.7 ng/mL; 81.1% had a single tumor; and median maximal tumor size was 2.0 cm), the attenuated prognostic significance of variables related to tumor burden should be reanalyzed in a future prospective study with a large sample size and wide range of tumor burdens.
We adopted a LS cutoff value of 13.0 kPa to determine cirrhotic range of LS values and high-risk group for recurrence.22 In addition, previous study concluded that chronic hepatitis B patients with LS values >13 kPa had a significantly higher risk of HCC development. Also, HCC patients with preoperative LS values >13.4 kPa experienced a higher incidence of HCC recurrence after curative resection than did their counterparts.14 Taken together, this indicates that 13 kPa might be a key cutoff, in various clinical settings, to stratify the different spectra of prognosis in patients with chronic liver disease, especially in terms of assessing the risk of HCC development. However, among the patients with LS values <13 kPa, a significant proportion of patients were still at a relatively high risk of HCC recurrence after RFA. Indeed, approximately 25% of patients experienced recurrence at 3 years after RFA despite having LS values <13.0 kPa. Thus, we calculated a second cutoff value with a high negative predictive value (94.4%) and found that 9.6 kPa (positive predictive value, 49.4%; sensitivity, 97.9%; specificity, 26.6%) was a cutoff value that could identify a subpopulation with a low risk of HCC recurrence. The cumulative incidence rate at 3 years was only 8.3% in patients with LS values <9.6 kPa. The finding that LS values below the cirrhotic range (13 kPa) can also be associated with the risk of HCC development is supported by a previous study13 that reported that patients with LS values below the cirrhotic range (8–13 kPa) had a 3.07-fold increased risk of HCC development compared with those with LS values <8 kPa. However, the use of 9.6 kPa as a cutoff value in clinical practice still needs validation.
Because of the strong correlation between clinically diagnosed liver cirrhosis and LS values in our study (P<0.001 by Spearmen correlation), we included LS values in multivariate analysis instead of liver cirrhosis to prevent the statistical redundancy. Although the clinical diagnosis of liver cirrhosis has been conventionally made based on ultrasonography and laboratory tests, a recent study proved that LS value can be more accurate in detecting compensated liver cirrhosis than can clinical criteria in terms of assessing the risk of HCC development.13 Furthermore, in contrast to TE, which has shown high reproducibility, the subjectivity of ultrasonography can be another problem in diagnosing liver cirrhosis clinically.27 Lastly, the risk of HCC recurrence was significantly higher in patients with >13 kPa and liver cirrhosis (n=59 [53.2%]) than that in patients with ≤13 kPa and liver cirrhosis (n=16 [14.4%]) in our study (P<0.001 by logrank test). All these indicate that TE has an additional role, as one of predictor for HCC recurrence, even among patients with liver cirrhosis.
Repeated studies revealed that antiviral treatment can reduce the recurrence of HBV- or HCV-related HCC after RFA.28,29 However, we could not found any significant correlation between antiviral therapy and recurrence among HBV- and HCV-related HCC patients. Because the small sample size of patients with each HCC etiology can be related to the false negative results, further large study are required to clarify this issue.
LS values, together with total bilirubin,15 were also independent predictive factors for OS after RFA, which means that the physical hardness of liver as assessed by using TE and functional liver reserve can independently and simultaneously influence the mortality after RFA. However, in contrast to previous studies,15,30 variables related to tumor burden were not identified as independent predictors of OS in our study. This phenomenon can be explained in several ways, such as the low proportion of subjects who died from HCC progression (6 of 14 [43%]) and the relatively low tumor burden in our cohort.
There are still several unresolved issues in our study. First, the criteria used to classify local recurrence and de novo recurrence are somewhat ambiguous.15 Among the de novo recurrence, it is practically impossible to distinguish intrahepatic metastasis from original tumor or a newly developed tumor in the diseased liver.8 Also, because we excluded the patients who experienced only local tumor progression, our results were subject to a selection bias, and the influence of some risk factors might have been underestimated. Third, in previous studies, HBV-related HCC developed in noncirrhotic livers, whereas HCV-related HCC occurs mostly in the presence of cirrhosis.31 Indeed, HBV-related HCC patients had significantly lower mean LS values than did HCV-related HCC patients (18.6 vs 29.5 kPa). However, the etiology of HCC only tended to influence the risk of recurrence (P=0.093) (Table 4). Although the exact reason for this result is not clear, the small sample size of patients with each etiology might have been insufficient to make a statistical difference. Finally, our short follow-up duration after RFA (median 22.4 months) does not seem sufficient to assess the influence of LS values on OS. Thus, large-scale prospective studies with consecutive enrollment and long-term follow-up duration could resolve the pitfalls of our study.
In conclusion, patients with a previous treatment history and higher LS values, >13.0 kPa, were at a significantly greater risk for de novo recurrence after RFA. In addition, patients with LS values >13.0 kPa, together with higher total bilirubin, experienced significantly decreased OS after RFA. Although our study indicates that LS measurement by using TE is useful for predicting de novo recurrence of HCC in the remnant liver as well as survival after RFA, external validation of our results in future large-scale prospective studies can expand the clinical implications of TE in a longitudinal perspective.
Acknowledgments
This study was supported by the Liver Cirrhosis Clinical Research Center, in part by a grant from the Korea Healthcare Technology R & D project, Ministry of Health and Welfare, Republic of Korea (grant number HI10C2020); in part by a grant from the Brain Korea 21 Project for Medical Science; and by a grant from Ministry for Health, Welfare and Family Affairs, Republic of Korea (grant number A050021).
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;379(9822):1245–1255. | ||
Bruix J, Sherman M; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020–1022. | ||
Livraghi T, Meloni F, Di Stasi M, et al. Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: Is resection still the treatment of choice? Hepatology. 2008;47(1):82–89. | ||
Lencioni R. Loco-regional treatment of hepatocellular carcinoma. Hepatology. 2010;52(2):762–773. | ||
Cho YK, Rhim H, Noh S. Radiofrequency ablation versus surgical resection as primary treatment of hepatocellular carcinoma meeting the Milan criteria: a systematic review. J Gastroenterol Hepatol. 2011;26(9):1354–1360. | ||
Kim YS, Rhim H, Cho OK, Koh BH, Kim Y. Intrahepatic recurrence after percutaneous radiofrequency ablation of hepatocellular carcinoma: analysis of the pattern and risk factors. Eur J Radiol. 2006;59(3):432–441. | ||
Zytoon AA, Ishii H, Murakami K, et al. Recurrence-free survival after radiofrequency ablation of hepatocellular carcinoma. A registry report of the impact of risk factors on outcome. Jpn J Clin Oncol. 2007;37(9):658–672. | ||
Goldberg SN, Grassi CJ, Cardella JF, et al; Society of Interventional Radiology Technology Assessment Committee and the International Working Group on Image-guided Tumor Ablation. Image-guided tumor ablation: standardization of terminology and reporting criteria. J Vasc Interv Radiol. 2009;20(7 Suppl):S377–S390. | ||
Hori T, Nagata K, Hasuike S, et al. Risk factors for the local recurrence of hepatocellular carcinoma after a single session of percutaneous radiofrequency ablation. J Gastroenterol. 2003;38(10):977–981. | ||
Imamura H, Matsuyama Y, Tanaka E, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003;38(2):200–207. | ||
Castera L, Forns X, Alberti A. Non-invasive evaluation of liver fibrosis using transient elastography. J Hepatol. 2008;48(5):835–847. | ||
Masuzaki R, Tateishi R, Yoshida H, et al. Prospective risk assessment for hepatocellular carcinoma development in patients with chronic hepatitis C by transient elastography. Hepatology. 2009;49(6):1954–1961. | ||
Jung KS, Kim SU, Ahn SH, et al. Risk assessment of hepatitis B virus-related hepatocellular carcinoma development using liver stiffness measurement (FibroScan). Hepatology. 2011;53(3):885–894. | ||
Jung KS, Kim SU, Choi GH, et al. Prediction of recurrence after curative resection of hepatocellular carcinoma using liver stiffness measurement (FibroScan®). Ann Surg Oncol. 2012;19(13):4278–4286. | ||
Seo JY, Kim W, Kwon JH, et al. Noninvasive fibrosis indices predict intrahepatic distant recurrence of hepatitis B-related hepatocellular carcinoma following radiofrequency ablation. Liver Int. 2013;33(6):884–893. | ||
Forner A, Reig ME, de Lope CR, Bruix J. Current strategy for staging and treatment: the BCLC update and future prospects. Semin Liver Dis. 2010;30(1):61–74. | ||
Kim do Y, Kim SU, Ahn SH, et al. Usefulness of FibroScan for detection of early compensated liver cirrhosis in chronic hepatitis B. Dig Dis Sci. 2009;54(8):1758–1763. | ||
Wai CT, Greenson JK, Fontana RJ, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38(2):518–526. | ||
Sandrin L, Fourquet B, Hasquenoph JM, et al. Transient elastography: a new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med Biol. 2003;29(12):1705–1713. | ||
Korean Association for the Study of the Liver. KASL Clinical Practice Guidelines: Management of chronic hepatitis B. Clin Mol Hepatol. 2012;18(2):109–162. | ||
Mulier S, Mulier P, Ni Y, et al. Complications of radiofrequency coagulation of liver tumours. Br J Surg. 2002;89(10):1206–1222. | ||
Friedrich-Rust M, Ong MF, Martens S, et al. Performance of transient elastography for the staging of liver fibrosis: a meta-analysis. Gastroenterology. 2008;134(4):960–974. | ||
Peng ZW, Zhang YJ, Liang HH, Lin XJ, Guo RP, Chen MS. Recurrent hepatocellular carcinoma treated with sequential transcatheter arterial chemoembolization and RF ablation versus RF ablation alone: a prospective randomized trial. Radiology. 2012;262(2):689–700. | ||
Harrison LE, Koneru B, Baramipour P, et al. Locoregional recurrences are frequent after radiofrequency ablation for hepatocellular carcinoma. J Am Coll Surg. 2003;197(5):759–764. | ||
Izumi N, Asahina Y, Noguchi O, et al. Risk factors for distant recurrence of hepatocellular carcinoma in the liver after complete coagulation by microwave or radiofrequency ablation. Cancer. 2001;91(5):949–956. | ||
Yamanaka Y, Shiraki K, Miyashita K, et al. Risk factors for the recurrence of hepatocellular carcinoma after radiofrequency ablation of hepatocellular carcinoma in patients with hepatitis C. World J Gastroenterol. 2005;11(14):2174–2178. | ||
Tchelepi H, Ralls PW, Radin R, Grant E. Sonography of diffuse liver disease. J Ultrasound Med. 2002;21(9):1023–1032; quiz 1033–1034. | ||
Dan JQ, Zhang YJ, Huang JT, et al. Hepatitis B virus reactivation after radiofrequency ablation or hepatic resection for HBV-related small hepatocellular carcinoma: a retrospective study. Eur J Surg Oncol. 2013;39(8):865–872. | ||
Ishikawa T. Secondary prevention of recurrence by interferon therapy after ablation therapy for hepatocellular carcinoma in chronic hepatitis C patients. World J Gastroenterol. 2008;14(40):6140–6144. | ||
Shiina S, Tateishi R, Arano T, et al. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am J Gastroenterol. 2012;107(4):569–77; quiz 578. | ||
Shariff MI, Cox IJ, Gomaa AI, Khan SA, Gedroyc W, Taylor-Robinson SD. Hepatocellular carcinoma: current trends in worldwide epidemiology, risk factors, diagnosis and therapeutics. Expert Rev Gastroenterol Hepatol. 2009;3(4):353–367. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.