Back to Journals » International Medical Case Reports Journal » Volume 15
Upper GI Bleeding Due to Leech Infestation in Ethiopian Patients: A Case Series and Review of Literature
Received 19 July 2022
Accepted for publication 20 October 2022
Published 24 November 2022 Volume 2022:15 Pages 677—680
DOI https://doi.org/10.2147/IMCRJ.S381990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Abdulsemed Mohammed Nur,1 Zebeaman Tibebu Gorfu2
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Internal Medicine, Adera Medical Center, Addis Ababa, Ethiopia
Correspondence: Abdulsemed Mohammed Nur, Email [email protected]
Abstract: Upper GI bleeding secondary to a live foreign body (leech) is a very rare condition, causing diagnostic and therapeutic challenges. Aquatic leeches could infest the upper gastrointestinal (GI) mucosa, resulting in bleeding and/or anemia. A history of contact with a contaminated water source is necessary to establish the diagnosis. We, herein, present two cases of upper GI bleeding caused by leech infestation and a technique for extraction of the leech.
Keywords: leech infestation, upper GI bleeding, anemia, Africa, Ethiopia
Introduction
Leeches are a rare cause of upper gastrointestinal bleeding. They are hermaphroditic, carnivorous, segmented worms from the phylum Annelida and the class Hirudinea. Aquatic leeches can be found in both freshwater and saltwater habitats, such as streams, pools, mud, and sand, where they may be encountered by humans. A history of contact with contaminated water bodies (drinking or swimming) is essential to the diagnosis.1 The mucosal surfaces of the nose, esophagus, larynx, pharynx, rectum, and vagina are target sites of infestation by aquatic leeches.2 Their ability to attach and suck blood is aided by natural anticoagulants produced by leeches, as well as histamine-like vasodilators, hyaluronidase, and anesthetic agents.3 Clinically, patients could present with bleeding of the mucosal surface and/or anemia.
Case Report
Case 1
A 53-year-old female patient arrived at the emergency department with hematemesis and black tarry stool of one week duration. She has no comorbid illnesses and no prior history of bleeding tendencies. She was not on any form of anticoagulants. She is from a rural area where frequent contact with contaminated water sources is common.
Her vital signs were stable, blood pressure 100/60 mmHg, pulse rate 88, and her physical examination was unremarkable. She was investigated with a Complete Blood Count (CBC), Renal Function Test (RFT), and Liver Function Test (LFT). She had mild anemia (hemoglobin 11g/dL, MCV 82fL). Otherwise, her investigations were in the normal range. An endoscopic evaluation revealed an alive leech attached to the oropharynx with active mucosal bleeding from the attachment site. Under endoscopic guidance, the leech was extracted gently using non-toothed foreign-body forceps and removed from the body (Figure 1). The oropharynx was inspected after the removal of the leech and no active bleeding was seen. Post-procedure, the patient was stable and doing well. Thus, she was advised on hygienic practices for drinking water and contact with water bodies.
 |
Figure 1 5cm long leech extracted from the pharynx. |
Case 2
A 50-year-old male patient presented to the outpatient department with a history of blood-mixed vomiting of 2 weeks duration with associated throat discomfort. He has no known chronic medical illnesses or bleeding tendencies. He was not on any anticoagulant. He lives in a rural area. For these complaints, he visited a traditional healer who prescribed him herbal juice of an unknown constituent. Even though he mostly uses tap water, he has a history of consumption from untreated sources a month back. On vital signs, blood pressure was 110/75 mmHg and pulse rate was 80. Physical examination was unremarkable. All investigations (CBC, RFT, LFT) were in the normal range.
Endoscopic examination revealed an adherent leech on the right side of the oropharynx (Figure 2). The leech was removed under endoscopic guidance using non-toothed foreign body forceps. The bleeding stopped immediately after the removal of the leech. The patient was advised on safe water drinking practices and sent home.
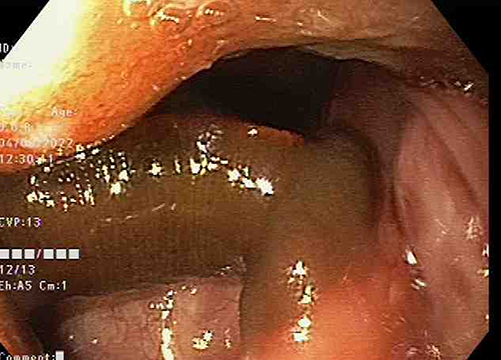 |
Figure 2 An adherent leech to the pharynx, grasped and extracted with non-toothed foreign body forceps. |
Discussion
Leeches are blood-sucking parasitic organisms of the phylum Annelida and class Hirudinea. The majority live in freshwater environments such as rivers and ponds, while some species can be found in terrestrial and marine environments.4 Upon successful contact with a human host, aquatic leeches inhabit mucosal surfaces. Their cartilaginous cutting plates, which are concealed below the front sucker, are capable of making a 2 mm incision. A single leech can drink 5 to 15 cc of blood (10 times its body weight) in just 30 minutes. Their blood-sucking nature lies majorly in their saliva, which contains a natural anticoagulant (hirudin), a local anesthetic, hyaluronidase (a spreading factor), and a histamine-like vasodilator that increases regional blood flow.3
The clinical presentation of patients is highly variable and is solely dependent on the site of mucosal attachment. The nose is the most frequently reported site, while epistaxis is the most common presentation.5 After entering the mucosal surfaces of the upper body, aquatic leeches primarily inhabit the nose, nasopharynx, oropharynx, and vagina, resulting in a variety of clinical presentations such as hemoptysis, epistaxis, vaginal bleeding, and shortness of breath.6–11 If the leech enters the esophagus and upper gastrointestinal tract, patients may experience vomiting and hematemesis, with the leech being automatically removed with the vomitus in some cases.11,12 Leech infestation of the lower GI tract presents with painless, bright red rectal bleeding in most cases.13,14 In severe cases, it can result in death.9
The bleeding presentation of patients is attributed to the anticoagulant hirudin, found in the saliva of aquatic leeches. Hirudin is the most potent natural thrombin inhibitor that combines with thrombin at a molar ratio of 1:1.15 It, thus, inhibits the cross-linking polymerization process of fibrin monomers in internal and external coagulation pathways.16
The approach to a patient with leech infestation includes thorough history-taking and systematic examination followed by appropriate investigation. A physical examination might be unremarkable in most cases.9 Even though complete blood cell count and other investigations are needed to supplement the case, endoscopic evaluation is generally required for diagnosis. Although coagulation profiles can help in differential diagnosis, their use in leech infestation is limited as the anticoagulant effect is only local secondary to the low level of hirudin.
The mainstay of management is the extraction of the leech from the mucosal surface. Management of underlying anemia should not be overlooked as well.1 The bleeding ceases within minutes after the removal of the leech. However, in some cases, minor oozing might persist for hours after detachment due to the effect of the anticoagulant.17
The soft and slippery body surfaces of aquatic leeches combined with strong attachment of the suckers to the mucosal surface, render a challenge in the removal of the parasite, as it is more likely to rupture.18 Thus, several techniques have been suggested. Forceps application to the center of the leech’s body and giving a quick pull is one such method that is successful in several cases.13,19 An electric shock of the infesting leech, 4% pantocain and oxymetazoline application, adrenaline injection followed by forceps removal, and hypertonic saline irrigation have also been effective.9,14,20 Successful extraction by squeezing the midpoint of the body for up to 20 seconds, resulting in a spontaneous release of mouthparts was also reported.5 We used, somewhat, similar technique with some modification. Application of a non-toothed extraction forceps close to the mouth part (posterior sucker) while maintaining a steady pull with a gentle squeeze will allow simpler extraction of the leech as witnessed in both cases. The detachment from the site should be immediately followed by the complete extraction of the leech from the body. The attachment site should be inspected for ongoing bleeding after the removal of the leech.
Conclusion
Even though leech infestation as a cause of upper GI bleeding is a rare finding, clinicians should be aware of symptoms and have a high index of suspicion in patients from rural areas, where there is no clean and safe drinking water. Gentle removal of the leech should be done under endoscopic guidance to ensure complete removal of the leech and prevent complications.
Ethical Statement
No institutional approval was required to publish the case details. All patients have provided their consent to the publication of these case reports, and any accompanying images.
Acknowledgments
We would like to express our deepest gratitude to the patients and their families, as well as to our colleagues who were involved in the care of the patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cundall DB, Whitehead SM, Hechtel FOP. Severe anaemia and death due to the pharyngeal leech Myxobdella africana. Trans R Soc Trop Med Hyg. 1986;80(6):940–944. doi:10.1016/0035-9203(86)90265-8
2. Saki N, Rahim F, Nikaghlagh S, Saki G. Meta-analysis of the leech as a live foreign body: detection, precaution, and treatment. Pak J Biol Sci. 2009;12(24):1556–1563. doi:10.3923/PJBS.2009.1556.1563
3. Daane S. Leeches. In: Plastic Surgery Secrets. Elsevier Inc.; 2010:721–723. doi:10.1016/B978-0-323-03470-8.00111-3
4. Sawyer RT. Leech Biology and Behaviour: Anatomy, Physiology and Behaviour. Oxford Science Publications; Vol. 1. 1986.
5. Harun K. Management of upper airway leech infestations. Ear Nose Throat J. 2020;99(10):NP126–NP128. doi:10.1177/0145561319860527
6. Taşkesen M, Katar S, Başçik H. An unusual cause of gastrointestinal bleeding and severe anemia in a child: leech infestation. J Trop Pediatr. 2009;55(5):338–339. doi:10.1093/TROPEJ/FMP015
7. Getahun AM, Endayehu Y, Berhanu GD. A case report on leech infestation as a cause of severe anemia in a 10-month-old infant in Ethiopia. Int Med Case Rep J. 2021;14:111–114. doi:10.2147/IMCRJ.S292226
8. Hasanzadeh M, Zarrinfar H, Najjari M. Unusual vaginal bleeding due to a leech bite in a girl from a tropical area: a case report. Rev Soc Bras Med Trop. 2019;52:2. doi:10.1590/0037-8682-0425-2018
9. Garça MF, Kürşat MY, Mehmet HO, Yuca SA. Leech infestation of the nasopharynx; a rare cause of epistaxis and hemorrhage. Eur J Gen Med. 2010;8(2):141–143.
10. Asrat K. Leech as a cause of abnormal vaginal bleeding: presentation of three cases in adults. J Eritrean Med Assoc. 2010;4(1):59–60. doi:10.4314/jema.v4i1.52122
11. Tsetsos N, Poutoglidis A, Skoumpas I, et al. A rare case of hemoptysis caused by a laryngeal leech. Ear Nose Throat J. 2021;26:1455613211000804. doi:10.1177/01455613211000804
12. Rutagumba D, Niyoyita B, Nyirasafari R. Severe anemia by a leech infestation in a pediatric patient: a case report. Rwanda Med J. 2020;77(2):1–3.
13. González LM, Janniger CK, Schwartz RA. Intermittent gastrointestinal bleeding in a child: leech infestation. Iran J Pediatr. 2012;22(4):572.
14. Narayan J, Nath P, Singh A, et al. Leech infestation presenting as severe rectal bleeding. J Dig Endosc. 2017;08(03):132–133. doi:10.4103/jde.jde_66_16
15. Junren C, Xiaofang X, Huiqiong Z, et al. Pharmacological activities and mechanisms of hirudin and its derivatives - A review. Front Pharmacol. 2021;12. doi:10.3389/fphar.2021.660757
16. Beeton C. Targets and therapeutic properties. In: Handbook of Biologically Active Peptides. Elsevier Inc.; 2013:473–482. doi:10.1016/B978-0-12-385095-9.00064-6
17. Karimian M, Nourmohammadi H, Salamati M, Hafezi Ahmadi MR, Kazemi F, Azami M. Epidemiology of gastroesophageal reflux disease in Iran: a systematic review and meta-analysis. BMC Gastroenterol. 2020;20(1). doi:10.1186/S12876-020-01417-6
18. Tilahun T, Babu H, Berhane M. Leech in the rectum causing lower gi bleeding in a four years old child: a case report. Ethiop J Health Sci. 2020;30(6):1055–1057. doi:10.4314/ejhs.v30i6.27
19. Al B, Yenen ME, Aldemir M. Rectal bleeding due to leech bite: a case report. Ulusal Travma ve Acil Cerrahi Derg. 2011;17(1):83–86. doi:10.5505/tjtes.2011.75318
20. Sarathi K. Nasal leech infestation causing persistent epistaxis. J Emerg Trauma Shock. 2011;4(3):413–414. doi:10.4103/0974-2700.83875
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Case Report of Belly Dancer Dyskinesia in a 54 Years Old Female: Gastroenterology Meets Neurology

Bane A, Seid AS, Ejeta A, Gorfu ZT
International Medical Case Reports Journal 2022, 15:661-663
Published Date: 15 November 2022