Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Upper Eyelid Blepharoplasty Improved the Overall Periorbital Aesthetics Ratio by Enhancing Harmony Between the Eyes and Eyebrows
Received 12 August 2022
Accepted for publication 14 September 2022
Published 20 September 2022 Volume 2022:15 Pages 1969—1978
DOI https://doi.org/10.2147/CCID.S385057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yingbo Zhang, Zhibo Xiao
Department of Plastic Surgery, The Second Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China
Correspondence: Zhibo Xiao, Department of Plastic Surgery, The Second Affiliated Hospital of Harbin Medical University, 157 Xuefu Road, P.O. Box:150086, Harbin, People’s Republic of China, Tel +86 86605967, Email [email protected]
Purpose: In upper eyelid blepharoplasty, most aesthetic surgeons and patients focus on improvements in the appearance of the upper eyelids, such as changing the vertical dimension of the palpebral fissure and the width of the pretarsal crease. Nevertheless, appropriately balanced periorbital aesthetics stemming from harmony between the eyelids and eyebrows is often ignored. The aim of this study was to explore the use of upper eyelid blepharoplasty to improve the overall periorbital aesthetics by enhancing the harmony between the eyes and eyebrows in young Asian women.
Patients and Methods: From December 2019 to December 2020, 45 young Asian female patients underwent external incision upper eyelidplasty without ptosis repair or brow lift at The Second Affiliated Hospital of Harbin Medical University. The pre- and 6-month post-operative follow-up changes in the overall periorbital aesthetics were studied retrospectively.
Results: The vertical position of the eyebrows in the upper face and shape of the brow apex were significantly improved after surgery. As a result, the height of the upper face was increased. Furthermore, the facial width proportion and midface ratio were closer to the ideal aesthetic golden ratio due to changes in the size of the periorbital area. All patients were satisfied with the result, and they achieved excellent surgical outcomes for not only the upper eyelids but also the overall periorbital region.
Conclusion: This study revealed that upper eyelid blepharoplasty, which enhances the appearance of the upper eyelids while regulating the eyelid position and shape of the eyebrows by considering the eye to eyebrow ratio, optimizes the proportion of the periorbital area and improves the overall periorbital aesthetics.
Keywords: periorbital aesthetics, eyelid blepharoplasty, eyebrows, facial proportions
Introduction
Attractive eyes, which are considered as the windows to the soul, are one of the most important features of facial beauty. The forehead-eyebrow complex and the brow-eyelid continuum are critical aesthetic components of upper facial rejuvenation.1 The contour of the eyebrows and appearance of the eyelids play key roles in aesthetics of the periorbital region.
In most Asian people, there is lack of thin fibers that connect the levator palpebrae muscles to the skin, and therefore, they do not have double-fold eyelids.2 However, a recent cadaveric study of Asian eyelids showed that distinctions in the volume and configuration of upper eyelid fat probably lead to differences in the appearance.3 Generally speaking, orbital fullness is a symbol of youth, but orbital swelling is undesirable. Excessive orbital fat can even affect the height of the marginal reflex distance (MRD1) when the eyelids are open. These particular patients look tired and unhappy; and in most cases, their MRD1 is close to the diagnostic criteria for ptosis (blepharoptosis is defined as a MRD1 <2.5 mm and levator excursion >14 mm),4 while the strength of the levator muscle is normal. The distance between the brow and the eye can significantly influence a person’s appearance; for example, a very long distance leads to an older looking visage.5
Brow position is an integral part of facial expression and an essential component of periorbital aesthetics.6 With respect to the ideal female eyebrow shape, the current literature suggests that the brow apex should be positioned at the lateral two-thirds of the eyebrows. The full forehead is twice as wide as its vertical height.7 The distance from the eyebrows to the inferior palpebral margin was found to be smaller in beauty pageant contestants than in ordinary young women.8 Perfect sagittal facial width proportions conform to the ratio of 1.618:1, which is called the Golden Ratio “Phi”, and it was regularly used by the Greek sculptor Phidias.9 The aim of our study was to determine whether descent of the brow position is accompanied by lowering and flattening of the first two-thirds of the eyebrows and increased prominence of brow peaks and to determine whether this change optimizes the proportion of the periorbital area and improves the overall facial aesthetics.
Materials and Methods
The study included 45 young Asian female patients aged 18–28 years. Brow position is dependent on age, gender, and race of the patient.2,10 In order to eliminate these factors, only young Asian female patients were included in our study. These young women provided their consent for participation in this study and signed the authorization for release of medical photographs and/or videotapes. This study was conducted in accordance with the Chinese laws of clinical practice. They underwent upper eyelid blepharoplasty without ptosis repair or brow lift between December 2019 and December 2020 at The Second Affiliated Hospital of Harbin Medical University. Patients with a history of facial, eyelid, orbital, or neurologic disease were excluded. Before the operation, face-to-face communication and evaluation of the patients’ periorbital region proportion were necessary. The patient shown in ►Figure 1 looked older than her actual age (19 years) before the operation because of a very long distance between the brow and the eye. The location of the palpebral crease line was dependent on the height of the eyebrows, the width of the forehead, and the distance between the medial canthi in each individual.
 |
Figure 1 Preoperative photograph of the patient. |
Operation procedures and techniques were similar for all patients, and they were as follows:
- All procedures were performed under local anesthesia by injecting 2% lidocaine containing 1:100,000 epinephrine.11
- The palpebral crease line followed the previous design based on the evaluation of patients’ periorbital region proportion.
- Upper eyelid puffiness is present in many single-fold eyelid patients.12 All patients included in our study had different degrees of upper eyelid puffiness. The heavy eyelid fat pad presses on the levator aponeurosis, affecting the strength of the levator muscle. As a result, limited orbicularis and redundant upper eyelid fat pads, particularly the lateral fat pad, were removed with scissors and cauterization.
- The septum was not opened.
- The tarsal plate was fixed to the orbicularis muscle layer using 6–0 nylon sutures at three to four points along the palpebral crease line before closure of the skin with 7–0 nylon sutures.
- All sutures were removed on the 6th postoperative day.
Photographs were taken by Canon EOS-60D camera at several stages, including pre-operation, immediately after upper eyelidplasty, and during the follow-up visit from 1 week to 6 months after surgery. The desired midface proportion (the ratio between a and b) was reproduced from the study by Rhee and Lee (2010) with permission from Springer Nature,13 as shown in ►Figure 2. Landmark data (H1–H6, shown in ►Table 1) were collected for locating the brow position. As shown in ► Figure 3A and B, line Q was drawn between the pupil centers, and the distance between line Q and the upper border of the brow was measured at defined positions (H1–H6, shown in ►Table 1). The vertical lines of Q through the pupils were marked P. H3 was located at the intersection of line P and the upper border of the brow. In order to reduce the measurement error, we set the position of H3 on the abscissa (line Q) at 3 cm and measured the average abscissa positions of H1, 2, 4, 5, and 6 on both sides of H3 before and after the operation. The highest brow point (H5) was defined as the arch of the upper eyebrow border.14 In most preoperative patients, the eyebrow peak sites were not obvious; therefore, we used the average postoperative position of H5 to replace the preoperative H5 position for making a comparison. ► Figure 3A and B show the positions of landmark data measurements before and after surgery in two patients. ►Figure 4 show graphical plots of the changes in the landmark data before and after surgery in patients. The change in the position of the brows shown in ►Figure 3 can be clearly seen in ►Figure 4. Furthermore, we analyzed the following information before and after the operation: pupil-to-brow distance (PTB), MRD1, the distance between medial canthi (X), the width from the medial canthus to the ipsilateral cheek apex (Y), the height of the forehead, the distance between the upper edge of the eyebrow and the edge of the lower eyelid (a), and the distance between the edge of the lower eyelid and the nasal base (b) ►Figures 5 and 6. All photographs were taken with the face in full repose and with the frontalis muscle in a fully relaxed state.15 Pre- and post-operative data were analyzed with SPSS (version 22.0; Armonk, NY, US), and statistical outcomes were presented as mean ± standard deviation. Statistical significance was considered to have been achieved at P < 0.05.
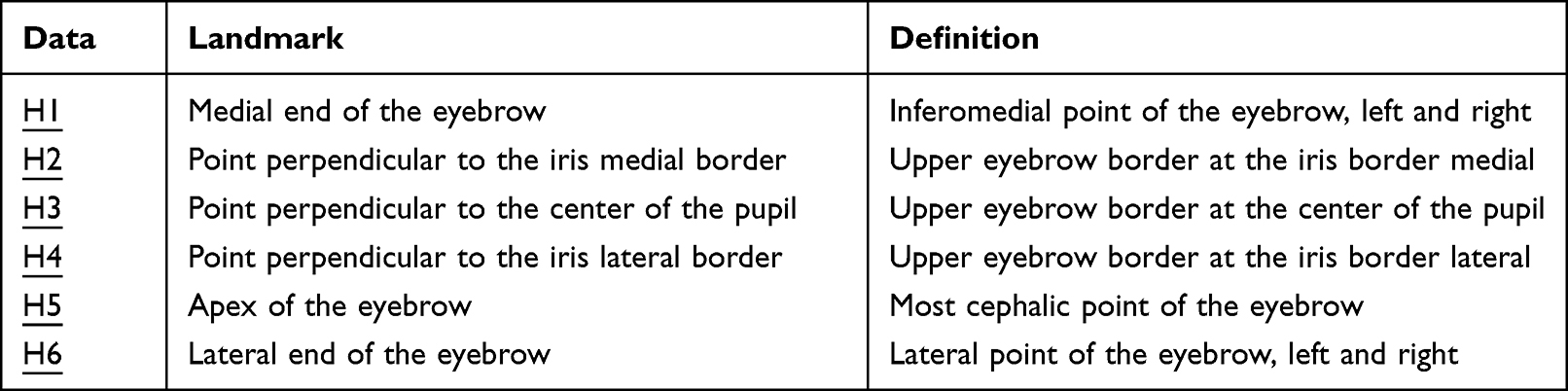 |
Table 1 Landmarks Used for Brow Positional Analysis |
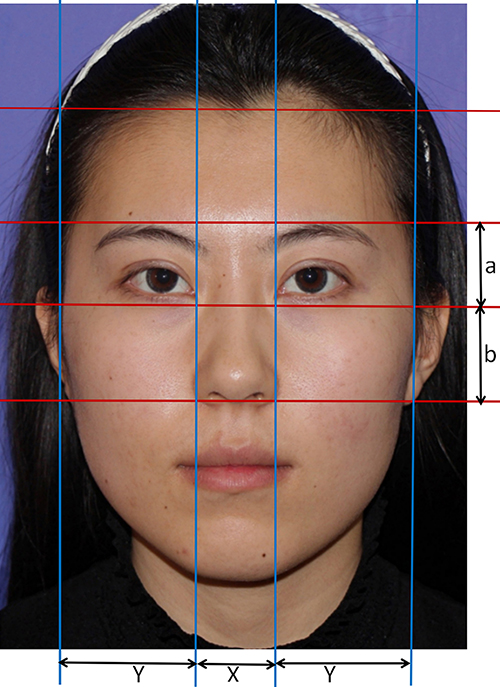 |
Figure 2 Medial canthus to medial canthus is measured as X; medial canthus to ipsilateral cheek apex is measured as Y = 1.618x. The distance between the upper edge of the eyebrow and the edge of the lower eyelid (a) and the distance between the edge of the lower eyelid and the nasal base (b) were measured. |
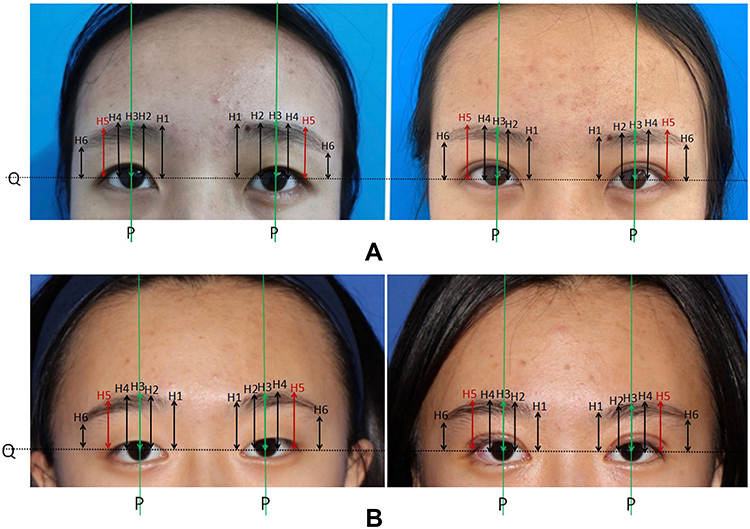 |
Figure 3 (A and B) both show the changes in the eyebrow shape before and after surgery. Before the operation (Left). Three months after external incision upper eyelidplasty (Right). The indicators of H1~H6 are shown in Table 1. |
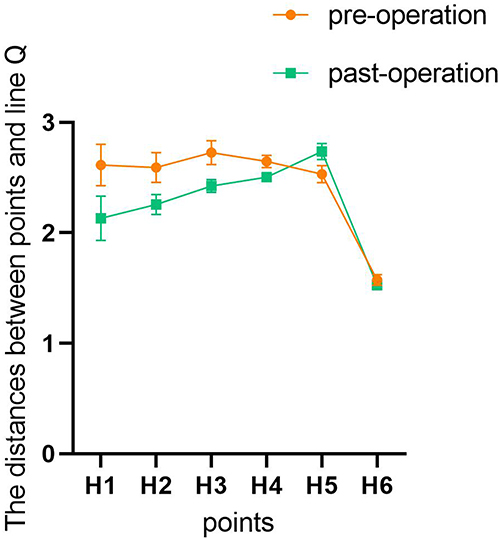 |
Figure 4 Graphical plots of the changes in the landmark data before and after surgery. The change in the position of the brows shown in.Figure 3 can be clearly seen in Figure 4. |
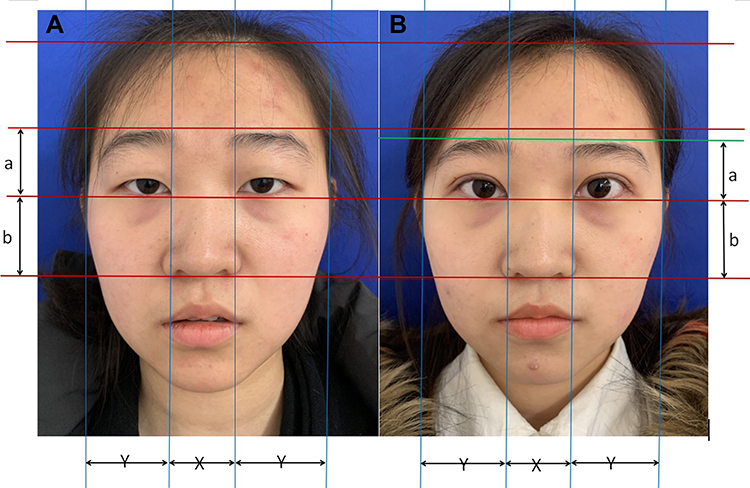 |
Figure 5 The overall changes before and after surgery Case 1. (A) Before the operation. (B) Two months after upper eyelidplasty. |
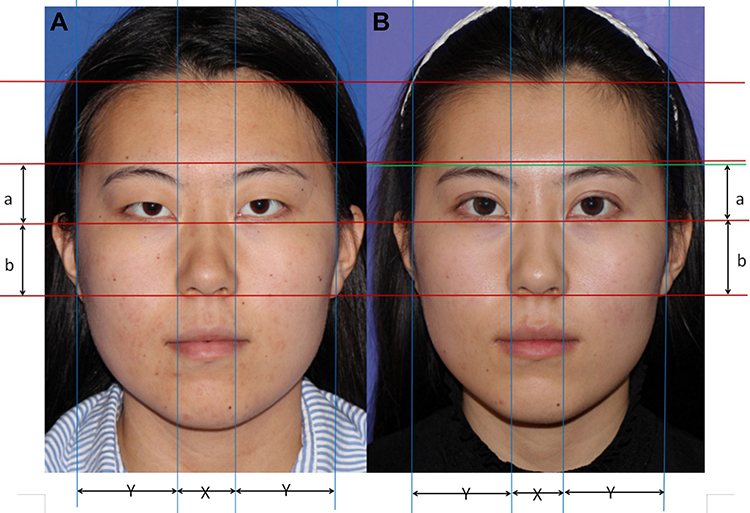 |
Figure 6 The overall changes before and after surgery Case 2. (A) Before the operation. (B) Six months after upper eyelidplasty. |
Results
A total of 45 young Asian female patients (90 eyelids and brows) were included; the mean preoperative MRD1 was 3.05 mm, and the mean post-operative MRD1 was 5.0 mm. MRD1 was significantly increased by 1.9 mm (p < 0.05, ►Table 2) after upper blepharoplasty alone. ►Table 2 shows that the change from preoperative PTB (20.7 mm) to postoperative PTB (17.3 mm) was significant (p < 0.05).
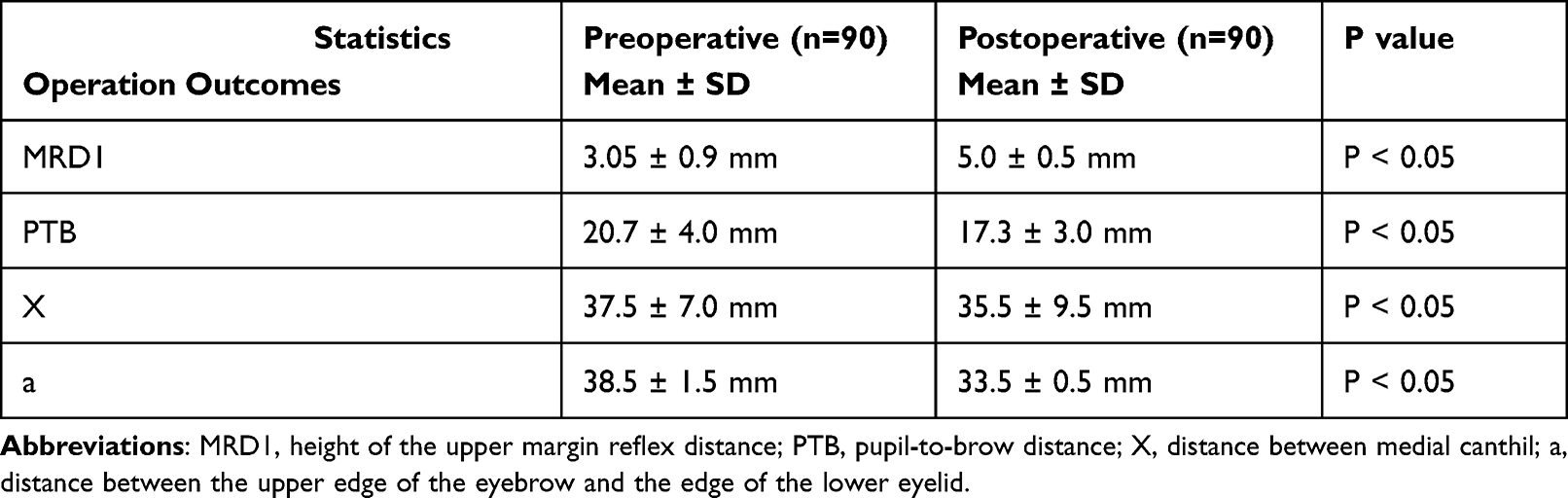 |
Table 2 Periorbital Area Measurements |
The mean facial width proportion (Y/X) changed from 1.39 to 1.58 after eyelid blepharoplasty, which was closer to the ideal ratio of 1.618:1 ►Figure 7. The average value of midfacial proportion (a/b) decreased from 0.801 before surgery to 0.698 after surgery, which was closer to the golden ratio of 0.618.16
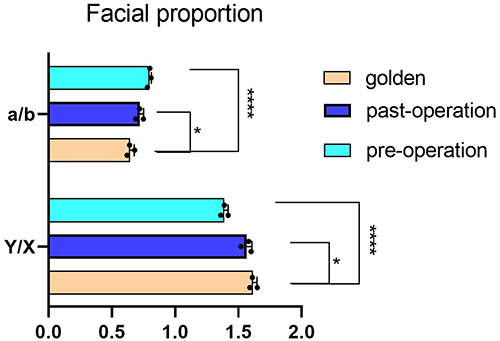 |
Figure 7 The bar chart of the average variation in facial proportion before and after surgery. Data are represented as mean ± SD. n = 3. *P < 0.05, ****P < 0.0001. |
All patients were satisfied with the results, and they achieved excellent surgical outcomes for not only the upper eyelid but also the overall periorbital region, as shown in ►Figures 8 and 9. The double eyelid effect was evident but not exaggerated. There were no intra-operative or post-operative complications in this group of patients. Furthermore, none of the patients experienced severe postoperative bleeding or swelling. Minimal bilateral asymmetry occurred in 9 of these 45 patients immediately after the operation; however, it disappeared within one week after surgery.
 |
Figure 8 (A) Photograph of the patient who was not satisfied with her appearance. (B) At the end of 6 months post-operation, the patient was satisfied with the results and became more confident. |
 |
Figure 9 (A) Photograph of the patient who looked exhausted before surgery. (B) Immediately after surgery, her MRD1 had significantly increased, her forehead was larger, eyebrows were lower, and facial proportions became more harmonious. She looked more attractive and alert after the operation. Abbreviation: MRD1, height of the upper margin reflex distance. |
Discussion
Originally, upper eyelid blepharoplasty focused on redundant skin, fat, and muscle, and it usually overlooked creating a more appropriate and harmonious ratio between the eyelid and the brow. With a deeper understanding of aesthetics, an increasing number of studies on facial proportional aesthetics have been reported.3,4 Plastic surgeons increasingly declare that the upper part of the face should be considered an extended aesthetic unit, and all patients who present for blepharoplasty should undergo an evaluation of their forehead and eyelids.17 In our study, the complete design of the palpebral crease line was based on the evaluation of patients’ periorbital region ratio. In the photographs taken at the postoperative follow-up, patient’s brows were in a more natural position, and the shape of the eyebrow was harmonious, especially the first two thirds of the brow descended significantly, and the apexes of the eyebrows were more prominent. This result is contrary to the conclusion derived in many articles. The majority of surgeons have suggested that the position of the eyebrow is not lowered significantly after an upper eyelid blepharoplasty alone.14,18 In our opinion, upper eyelidplasty is usually performed among senior citizens with dermatochalasis in western countries. Without performing brow lift or browpexy, it is difficult to restore the proportion of the brow and the eyelid in these patients. Clearly, the brow position is also dependent on the age, gender, and race of the patient;2,10 thus, to eliminate these factors, only young Asian female patients were included in our study. Young women underwent external incision upper eyelidplasty without ptosis repair or brow lift. Xu and Le et al5 demonstrated that, in Asian women, there was a statistically significant brow descent after the three-point double eyelid surgery method. However, only a single point on the brow was measured in that study, and there were no statistically significant changes in the brow shape and apex due to double eyelidplasty. In this retrospective analysis of 45 Asian female patients with an average age of 22, we found that the vertical position of the eyebrow in the upper face and the shape of the brow apex were significantly improved after our surgical procedure.
An absent (or very minor) lid fold and a fuller upper eyelid are the most obvious characteristics of the Asian eyelid, which give the impression of a smaller palpebral fissure.19 The majority of Asian patients with single eyelid have excessively swollen upper eyelids and higher eyebrow positions, which lead to an unattractive periorbital area and an increase in their midfacial ratio. An aged look is predominantly determined by an increased distance of the PTB, which is normally corrected by upper eyelid blepharoplasty without an additional operation for adjusting the position of the eyebrows.18 Based on our past experience, three-point double eyelidplasty cannot effectively remove a large amount of upper eyelid fat pads, and the levator aponeurosis folding procedure is not necessary for the large space between the eyebrows and the inferior palpebral margin. However, it is already known that blepharoptosis surgery affects the eyebrow position and is described in most of the literatures.20,21 To achieve more satisfactory surgical outcomes, we chose external incision upper eyelidplasty. Through this procedure, excess upper eyelid fat was released, the contour of eyebrows was improved, and a more attractive periorbital region was created.
A classically held principle of upper eyelid surgery is that the MRD1 is not typically altered by blepharoplasty surgery alone.22 However, some surgeons think that upper eyelid blepharoplasty without ptosis surgery results in a statistically significant increase in MRD1.14 Through the retrospective analysis of these 45 cases, we concluded that brow-lid continuum blepharoplasty can not only change the position of the eyebrows and increase MRD1, but it can also improve the shape and facial proportion of the eyebrows. Most importantly, a balance within the periorbital region results in achieving proportions of the sagittal facial width and vertical midface that are closer to the aesthetic standards. As professional plastic surgeons, we should not only care about the patients’ desires, but also about what actually suits them. In this respect, the aim of cosmetic surgery should be to achieve the maximum degree of overall aesthetic harmony while addressing the concerns of the patients.
After external incision upper eyelidplasty, mild swelling and a 1- to 2-week postoperative recovery period are inevitable. In our study, minimal bilateral asymmetry occurred in 9 of the 45 female patients immediately after the operation. However, symmetry is restored when the swelling abates, and this point should be explained to the patients to alleviate their concerns at this time. The main limitations of this study were the small sample size and participant age homogeneity. The next phase of our project will include expansion of the sample size and retrospective study of the differences in surgical outcomes with increasing age.
Conclusion
The patients included in this study achieved the following enhancements through appropriate external incision upper eyelidplasty:
- Increased upper margin reflex distance (MRD1).
- Diminished pupil-to-brow distance (PTB). PTB was measured as a vertical line from the center of the pupil to the lower eyebrow margin.23
- Increased height of the upper face.
- Lower eyebrows and more prominent eyebrow apexes, which improved the contour of the eyebrows.
- More balanced and harmonious facial proportions, including midface proportion and ratio of facial width.
We have shown that external incision upper eyelidplasty, which enhances the appearance of the upper eyelids while regulating the position of eyebrows and the shape of the brow apex by considering the eye to eyebrow ratio, optimizes the proportion of the periorbital area and improves the overall periorbital aesthetics. In future clinical work, the potential change in the postoperative brow position and shape should be explained to the patients before surgery. Furthermore, to create a more attractive periorbital area, aesthetic surgeons should consider performing upper eyelid surgery in harmony with the eyelid and eyebrow ratios.
Ethical Approval
This study was conducted in accordance with the Chinese laws of clinical practice and Declaration of Helsinki, and it was approved by the ethics committee of The Second Affiliated Hospital of Harbin Medical University.
Informed Consent
All patients provided written informed consent for use of their images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors have received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors have declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
References
1. Lam VB, Czyz CN, Wulc AE. The brow-eyelid continuum: an anatomic perspective. Clin Plast Surg. 2013;40(1):1–19. doi:10.1016/j.cps.2012.06.001
2. Park DD. Aging Asian upper blepharoplasty and brow. Semin Plast Surg. 2015;29(3):188–200. doi:10.1055/s-0035-1556853
3. Hicks K, Sclafani AP, Thomas JR. Evolution of blepharoplasty. Facial Plast Surg. 2019;35(4):340–352. doi:10.1055/s-0039-1693437
4. Sinha KR, Al Shaker S, Yeganeh A, Moreno T, Rootman DB. The relationship between eyebrow and eyelid position in patients with ptosis, dermatochalasis and controls. Ophthal Plast Reconstr Surg. 2019;35(1):85–90. doi:10.1097/IOP.0000000000001178
5. Xu L, Lee EI, Ma T, et al. Aesthetic analysis of alteration of eyebrow position after double eyelidplasty. Aesthetic Plast Surg. 2020;44(2):373–378. doi:10.1007/s00266-019-01590-4
6. Yalçınkaya E, Cingi C, Söken H, Ulusoy S, Muluk NB. Aesthetic analysis of the ideal eyebrow shape and position. Eur Arch Otorhinolaryngol. 2016;273(2):305–310. doi:10.1007/s00405-014-3356-0
7. Neimkin MG, Holds JB. Evaluation of eyelid function and aesthetics. Facial Plast Surg Clin North Am. 2016;24(2):97–106. doi:10.1016/j.fsc.2015.12.002
8. Kim YC, Kwon JG, Kim SC, et al. Comparison of periorbital anthropometry between beauty pageant contestants and ordinary young women with Korean ethnicity: a three-dimensional photogrammetric analysis. Aesthetic Plast Surg. 2017;42(2):479–490. doi:10.1007/s00266-017-1040-7
9. Branham G, Holds JB. Brow/Upper lid anatomy, aging and aesthetic analysis. Facial Plast Surg Clin North Am. 2015;23(2):117–127. doi:10.1016/j.fsc.2015.01.001
10. Hassanpour SE, Kermani HK. Brow ptosis after upper blepharoplasty: findings in 70 patients. World J Plast Surg. 2016;5(1):58–61.
11. Lu L, Zhu M, Luo X, et al. Using levator aponeurosis to create physiologically natural double eyelid. Ann Plast Surg. 2017;78(5):487–491. doi:10.1097/SAP.0000000000000951
12. Wong C-H, Hsieh MKH. Invited discussion on: orbicularis–white line fixation in Asian blepharoplasty—kiss technique. Aesthetic Plast Surg. 2019;43(6):1561–1563. doi:10.1007/s00266-019-01492-5
13. Rhee SC, Lee SH. Attractive composite faces of different races. Aesthetic Plast Surg. 2010;34(6):800–801. doi:10.1007/s00266-010-9606-7
14. Kraus D, Formoly E, Iblher N, Stark GB, Penna V. A morphometric study of age- and sex-dependent changes in eyebrow height and shape✰. J Plast Reconstr Aesthet Surg. 2019;72(6):1012–1019. doi:10.1016/j.bjps.2019.01.011
15. Nakra T, Modjtahedi S, Vrcek I, et al. The effect of upper eyelid blepharoplasty on eyelid and brow position. Orbit. 2016;35(6):324–327. doi:10.1080/01676830.2016.1193541
16. Ji C, Li R, He W, Zhang J. The aesthetic analyzing of midface ratio after folding aponeurosis of levator palpebrae superioris muscle in the ptosis correction. J Craniofac Surg. 2018;29(2):482–485. doi:10.1097/SCS.0000000000004158
17. Codner MA, Kikkawa DO, Korn BS, Pacella SJ. Blepharoplasty and brow lift. Plast Reconstr Surg. 2010;126(1):1e–17e. doi:10.1097/PRS.0b013e3181dbc4a2
18. Huijing MA, van der Palen J, van der Lei B. The effect of upper eyelid blepharoplasty on eyebrow position. J Plast Reconstr Aesthet Surg. 2014;67(9):1242–1247. doi:10.1016/j.bjps.2014.05.022
19. Saonanon P. Update on Asian eyelid anatomy and clinical relevance. Curr Opin Ophthalmol. 2014;25(5):436–442. doi:10.1097/ICU.0000000000000075
20. Kokubo K, Katori N, Hayashi K, et al. Evaluation of the eyebrow position after levator resection. J Plast Reconstr Aesthet Surg. 2017;70(1):85–90. doi:10.1016/j.bjps.2016.09.025
21. Rootman DB, Karlin J, Moore G, Goldberg R. The effect of ptosis surgery on brow position and the utility of preoperative phenylephrine testing. Ophthal Plast Reconstr Surg. 2016;32(3):195–198. doi:10.1097/IOP.0000000000000458
22. Dar SA, Rubinstein TJ, Perry JD. Eyebrow position following upper blepharoplasty. Orbit. 2015;34(6):327–330. doi:10.3109/01676830.2015.1078375
23. Karlin JN, Rootman DB. Brow height asymmetry before and after eyelid ptosis surgery. J Plast Reconstr Aesthet Surg. 2020;73(2):357–362. doi:10.1016/j.bjps.2019.07.018
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.