Back to Journals » Clinical Ophthalmology » Volume 13
Updated chandelier illumination-assisted scleral buckling using 3D visualization system
Authors Kita M, Kusaka M, Yamada H, Hama S
Received 10 June 2019
Accepted for publication 29 August 2019
Published 6 September 2019 Volume 2019:13 Pages 1743—1748
DOI https://doi.org/10.2147/OPTH.S218975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Supplementary video of ID 218975
Views: 799
Mihori Kita, Mami Kusaka, Hiroshi Yamada, Sachiyo Hama
Department of Ophthalmology, National Organization Kyoto Medical Center, Kyoto, Japan
Correspondence: Mihori Kita
Department of Ophthalmology, National Organization Kyoto Medical Center, 1-1 Mukouhata-cho, Fukakusa, Fushimi-ku, Kyoto 612-8555, Japan
Tel +81 75 641 9161
Fax +81 75 643 4325
Email [email protected]
Purpose: To assess the updated chandelier illumination-assisted scleral buckle procedures using a 3D visualization system.
Subjects and methods: We report a single-center, retrospective, consecutive surgical case series of 18 eyes of 16 patients that underwent scleral buckle procedures combining the use of chandelier endoillumination, a noncontact wide-angle viewing system, an anti-drying contact lens, and a recently developed 3D visualization system. The mean age of the patients was 30.2 years, and the mean follow-up time was 11.3 months.
Results: Retinal reattachment was achieved after the first surgery in all cases. There were no cases that required conversion of the 3D visualization to a conventional microscopic view. This updated chandelier-assisted scleral buckle procedure was successfully performed without any intraoperative or postoperative complications, except for the occurrence of postoperative diplopia in one case in which a supplementary radial buckle was used for a deep tear.
Conclusion: The updated chandelier illumination-assisted scleral buckling surgery using a 3D visualization system appears to be a valuable and promising method for managing rhegmatogenous retinal detachment due to atrophic holes in lattice degeneration or ciliary tears in younger cases.
Keywords: scleral buckling, chandelier illumination, wide-angle viewing system, 3D visualization system, retinal detachment, contact lens
Introduction
Scleral buckling is still the first choice for cases with rhegmatogenous retinal detachment caused by atrophic holes in lattice degeneration or ciliary tears without posterior vitreous detachment. Recent studies have demonstrated the efficacy of chandelier-assisted scleral buckling procedures compared to conventional approaches that use an indirect ophthalmoscope.1–12
The recent development of a 3D heads-up visualization system has helped lead to technological improvements in the ophthalmological field.13–17 However, efficacy of the system has been mainly reported for only vitrectomy.
In this study, we assess the updated scleral buckle procedure that combines the use of chandelier endoillumination, a noncontact wide-angle viewing system, an anti-drying contact lens,18,19 and a recently developed 3D visualization system.
Subjects and methods
This study was approved by the Ethics Committee of the National Hospital Organization Kyoto Medical Center, and all procedures involved adhered to the tenets of the Declaration of Helsinki. Written informed consent for the procedure and participation in the study was obtained from all patients after receiving an explanation of the surgical procedures. When patients are under the age of 20, a parent or legal guardian provided the written informed consent with the patients’ assent.
We report a single-center, retrospective, consecutive surgical case series of 18 eyes in 16 patients (10 males, 6 females, mean age 30.2 years) that underwent scleral buckling between May 2017 and May 2019. The mean follow-up time was 11.3 months.
All of the cases were phakic and had multiple retinal breaks without posterior vitreous detachment. There were 17 cases that had atrophic holes in the lattice degeneration, which was accompanied with retinal tears in 3 cases, while the other remaining atopic dermatitis case had ciliary tears. The macula was detached in 8 cases, with the demarcation-lines and/or the subretinal strands observed in 7 and 3 cases, respectively. LASIK had been performed in 2 cases, while there was a history of ocular trauma in 2 cases, and atopic dermatitis treatments in 2 cases (Table 1).
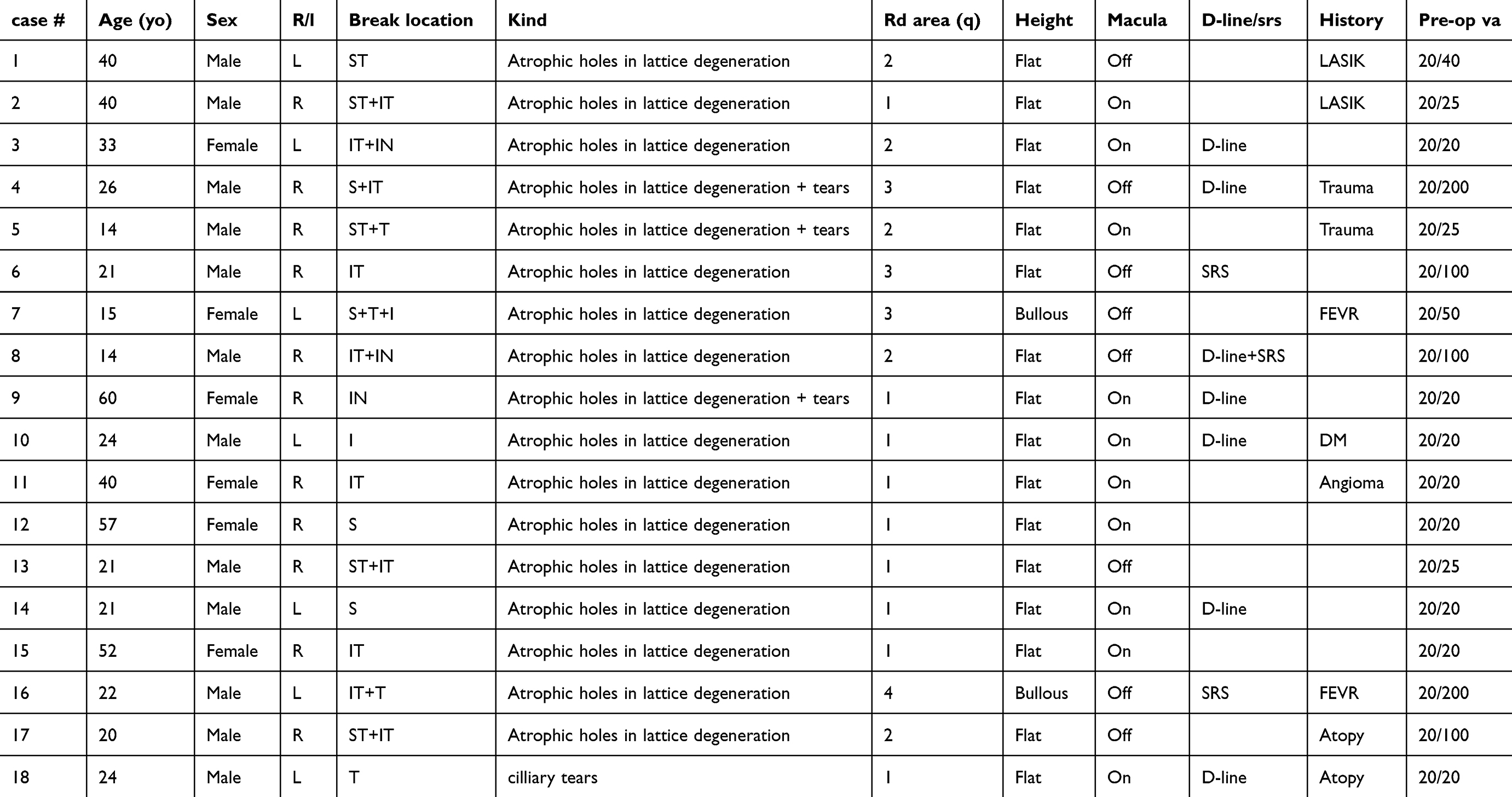 |
Table 1 Preoperative clinical characteristics of the 18 cases |
Instruments
All surgical procedures were observed using the NGENUITY 3D visualization system (Alcon Laboratories, Fort Worth, TX, USA), which was attached to a VISU 210 microscope (Carl Zeiss Meditec, Jena, Germany). A 27G mono chandelier light system (DORC, Zuidland, Netherlands) was used for the intraocular illumination. Images of the fundus on the NGENUITY 3D visualization system monitor were obtained using a RESIGHT wide-angle viewing system (Carl Zeiss Meditec). Observation of the fundus with a noncontact wide-angle viewing system was performed in all cases using a newly developed contact lens (HOYA Corporation, Tokyo, Japan).16,17
Surgical procedures
In the 3 teenage subjects, the surgery was performed under general anesthesia. In the other 15 cases, sub-Tenon anesthesia was used (Table 2).
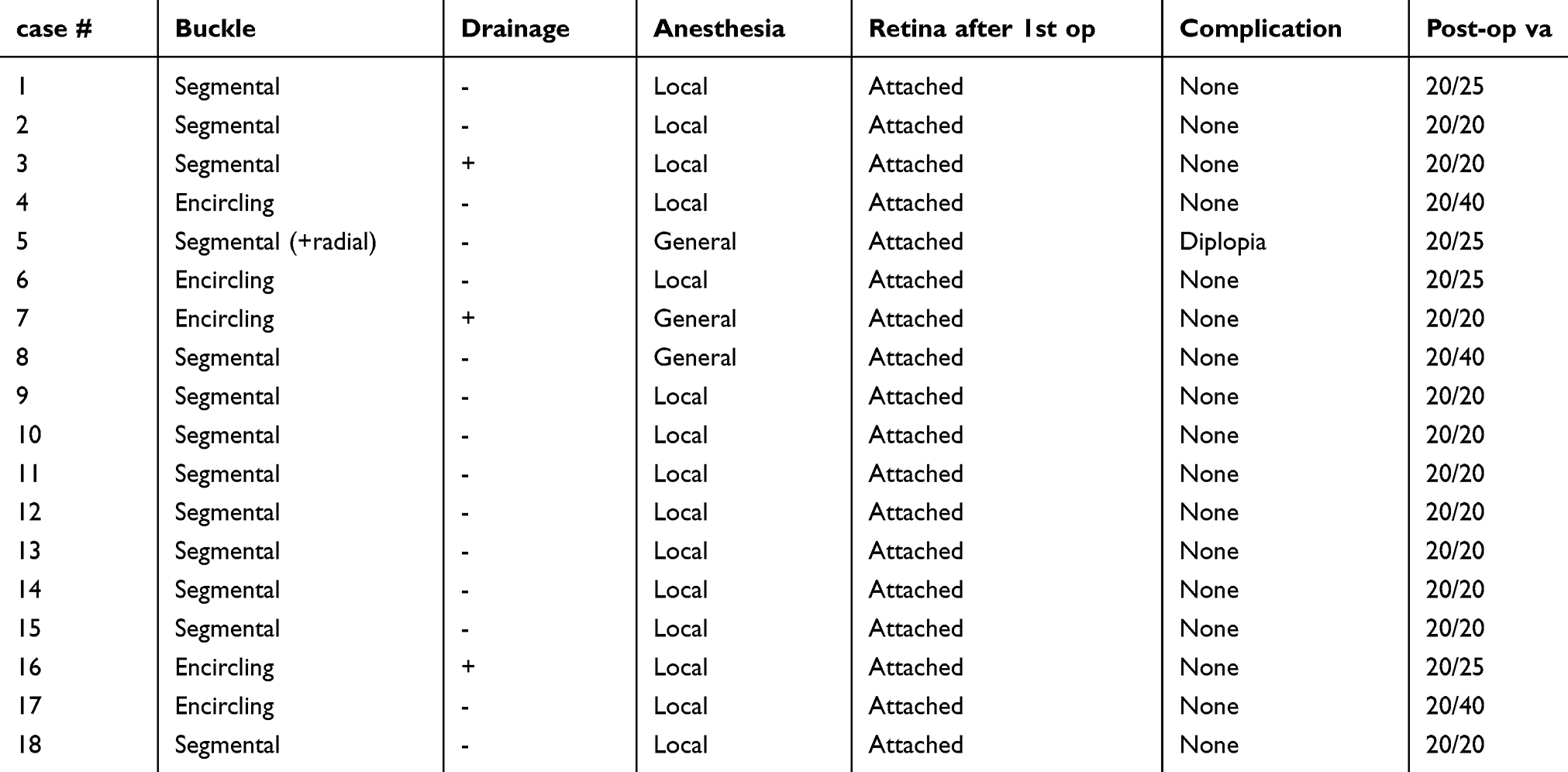 |
Table 2 Surgical procedures and postoperative clinical characteristics of the 18 cases |
Following conjunctival peritomy around the limbus, rectus muscles were isolated and 4–0 silk was passed underneath each muscle for the purpose of rotating the eye. A chandelier illumination fiber was placed 4.0 mm behind the limbus either at the quadrant opposite the breaks or at the place where it is easy to manipulate the fiber to illuminate the retinal breaks during the retinopexy (Figure 1, Video S1).
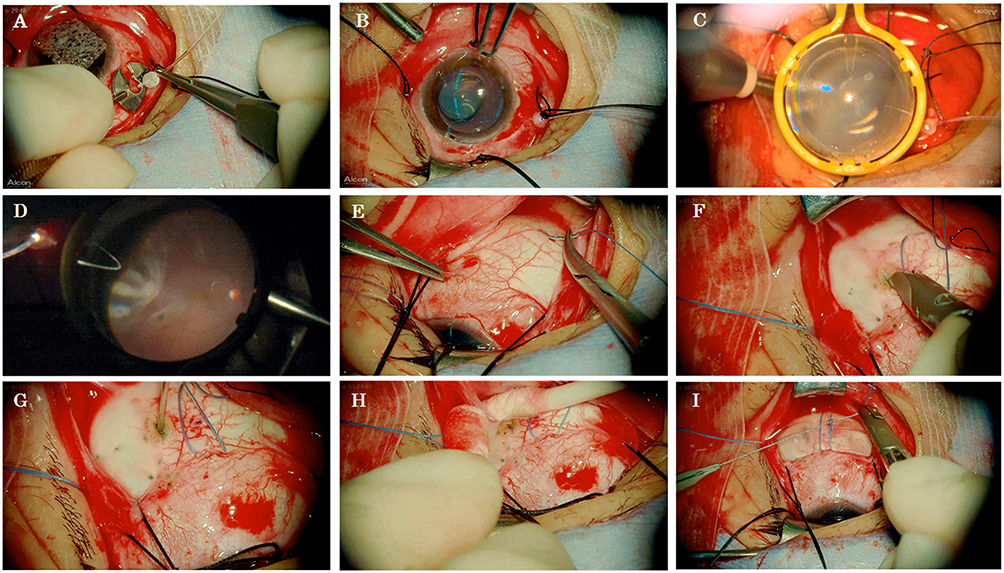 |
Figure 1 Intraoperative 2D snapshots of chandelier-assisted scleral buckling in case #16. All the images were pictured in the large monitor of the 3D visual system. (A) Following conjunctival peritomy around the limbus and isolation of the rectus muscles with 4–0 silk, a chandelier illumination fiber was placed 4.0 mm behind the limbus at the quadrant opposite the breaks. (B) An anti-drying contact lens was positioned on top of the cornea covered with viscoelastic material. (C) The wide-angle viewing system was activated. (D) Cryopexy was applied to the retinal breaks. With pilot diathermy, flecks applied prior to the chandelier setting were observed. (E) After the light fiber was removed, 5–0 Dacron sutures were applied for the buckle under a microscope with high magnification. (F) Sclerotomy for the external drainage site was also made under a microscope with high magnification. (G) Puncture of the uvea was carried out by a single application of an endolaser. (H) External drainage of subretinal fluid was carried out by scleral depression. (I) The silicone tire was explanted. |
A wide-angle viewing system was activated after the anti-drying contact lens was positioned on the top of the cornea covered with viscoelastic material. Retinopexy with cryopexy was applied to the retinal breaks. Diathermy with illumination was applied to mark the position of the breaks on the sclera while using the wide-angle viewing system. Prior to the chandelier setting, a pilot diathermy with a 0.5 mm penetrating needle under an indirect ophthalmoscope was used in some cases as an alternative marking procedure, as the clearer marks on the sclera made it easier to perform the buckle procedure (Figure 1, Video S1).
After removal of the light fiber, a segmental or circumferential encircling buckling consisting of a silicone sponge or tire was sutured with 5–0 Dacron, and if necessary, external drainage of the subretinal fluid were carried out under a microscope (Figure 1, Video S1).
The fundus was checked either under a panoramic view using the noncontact wide-angle viewing system with the illumination fiber once again inserted, or through the use of indirect ophthalmoscopy. The peritomy was closed using a 8–0 Vicryl suture.
A single surgeon (MK) performed all of the surgeries. Polarized glasses were worn by all of the surgical staff, including the primary surgeon, during the surgical procedures.
Results
Conversion of the 3D visualization to a conventional microscopic view was not required in any of the current cases. The 3D visualization system was successfully used in all surgeries to perform chandelier illumination-assisted scleral buckling. The microscope and chandelier light illuminations were reduced by 40%.
Segmental buckling or encircling buckling was performed in 13 and 5 cases, respectively. External drainage was performed in 3 cases in which the retinal detachment remained bullous after the preoperative bed rest (Table 2).
Reattachment was achieved in all 18 of the cases after the first scleral buckling and the retina remained attached at the final visit (Table 2). There were no intraoperative or postoperative complications in the patients except for postoperative diplopia that occurred in one case that had undergone supplemental radial buckle for a deep retinal tear. None of the patients exhibited endophthalmitis, lens opacity, or retinal phototoxicity (Table 2).
Discussion
Micro-incision vitrectomy surgery has recently become the preferred first choice of surgery for retinal detachment, with the use of the scleral buckle procedures to treat retinal detachment now declining. This trend may be due in part to advancements that have been made in vitrectomy surgery including its platforms and instrumentation.8 The use of a wide-angle viewing system has now become the global standard, as this option can easily provide a panoramic view of the surgical field. In contrast, visualization of the fundus during conventional scleral buckle procedures requires using an indirect ophthalmoscope. Indirect ophthalmoscope images are inverted and small, and cannot be readily shared with the medical staff, which can be disadvantageous when trying to identify tiny retinal breaks.
In 2012, Aras et al first demonstrated that the simultaneous use of a noncontact wide-angle viewing system combined with a 25G light fiber illumination for fundus visualization was also feasible for use in scleral buckle procedures.1 In 2013, we described an updated technique for endoilluminator-assisted scleral buckling and reported that it seemed promising for the management of not only simple rhegmatogenous retinal detachments, but also complicated cases such as those with undetected retinal breaks.2 The advantages of the chandelier-assisted scleral buckling are that clear images of the retina are directed through the surgical microscope, and can thus be enlarged and seen even with a small pupil. This allows detection of retinal breaks during dynamic scleral compression with a cryoprobe using a wide-angle viewing system.
Recently, a 3D heads-up visualization system has also been developed for use in the ophthalmological field.13–17 The advantages of using this type of system as compared to viewing the surgical field through a microscope includes better ergonomics for the surgeons, educational capability, enlargement of the images, and reduction of the illumination by enhancing the gain of the image. Furthermore, these advantages of the 3D visualization system additionally enhance the benefits of the chandelier-assisted scleral buckle procedure. When performing chandelier-assisted buckling, there is improved ergonomics due to the use of a microscope to perform the examination and improved treatment of retinal breaks as compared to when using indirect ophthalmoscopy. A 3D visual system further improves the ergonomics aspects of the surgeon due to the use of the heads-up position. Also, when using the 3D visualization system, images of the fundus during retinopexy can be shared on a large monitor, which will undoubtedly prove more useful in surgical education. In addition, larger images on a 55 inch monitor make it possible to more easily manipulate buckle suture and external drainage of the subretinal fluid. One of the concerns during the use of the chandelier-assisted buckle procedure is retinal light toxicity. Due to the use of a digital control of the brightness of the images in the 3D visualization system, this can reduce the light of the microscope and chandelier by 40%, thereby potentially reducing the risk of light toxicity. Moreover, the time latency and the use of a 16:9 size monitor in the 3D visualization system, which results in a view that is much different from that seen with the microscope, did not result in any difficulties in the surgical manipulations.
Drying of the cornea during surgery, which causes poor visibility of the fundus, is one of the most serious problems when using a noncontact type wide-angle viewing system. We have previously developed a new lens for observing the fundus with a noncontact wide-angle viewing system18,19 and reported that the smooth surface of this lens was able to achieve an intraoperative view of good quality without continuous hydration by an assistant, not only during vitrectomy but also during scleral buckle procedures.17 Thus, this lens is able to prevent damage of the corneal surface, especially in LASIK eyes. Moreover, in order to observe retinal breaks at the periphery, we can position the front lens of the wide-angle viewing system close to the cornea without the risk of touching the viscoelastic material on the cornea.
Several studies have reported that the use of chandelier-assisted scleral buckling yielded a reattachment rate of 83.3–95.5% without any significant intraoperative and postoperative complications.3–11 In our current study, reattachment was achieved in all of the 18 cases after the first scleral buckling. None of the patients exhibited any intraoperative or postoperative complications directly due to the system, such as endophthalmitis, lens opacity, or retinal phototoxicity.
In conclusion, updated chandelier-assisted scleral buckling using a 3D visualization system appears to be a valuable and promising method that can be used to manage rhegmatogenous retinal detachment due to atrophic holes or ciliary tears that occur in younger cases.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aras C, Ucar D, Koytak A, Yetik H. Scleral buckling with a non-contact wide-angle viewing system. Ophthalmologica. 2012;227(2):107–110. doi:10.1159/000333101
2. Kita M, Fujii Y, Kawagoe N, Hama S. Scleral buckling with a noncontact wide-angle viewing system in the management of retinal detachment with undetected retinal break: a case report. Clin Ophthalmol. 2013;7:587–589. doi:10.2147/OPTH.S42923
3. Nam KY, Kim WJ, Jo YJ, Kim JY. Scleral buckling technique using a 25-gauge chandelier endoilluminator. Retina. 2013;33(4):880–882. doi:10.1097/IAE.0b013e318271f265
4. Zhong LX, du Y, Liu W, Huang SY, Zhang SC. Using surgical microscope for sclera buckling and transscleral cryopexy: an alternative procedure of treatment for rhegmatogenous retinal detachment. Biomed Res Int. 2014;2014:364961–364967. doi:10.1155/2014/364961
5. Nagpal M, Bhardwaj S, Mehrotra N. Scleral buckling for rhegmatogenous retinal detachment using vitrectomy-based visualization systems and chandelier illumination. Asia Pac J Ophthalmol (Phila). 2013;2(3):165–168. doi:10.1097/APO.0b013e3182929b75
6. Gogia V, Venkatesh P, Gupta S, Kakkar A, Garg S. Endoilluminator-assisted scleral buckling: our results. Indian J Ophthalmol. 2014;62(8):893–894. doi:10.4103/0301-4738.141068
7. Imai H, Tagami M, Azumi A. Scleral buckling for primary rhegmatogenous retinal detachment using noncontact wide-angle viewing system with a cannula-based 25G chandelier endoilluminator. Clin Ophthalmol. 2015;9:2103–2107. doi:10.2147/OPTH.S91339
8. Seider MI, Nomides REK, Hahn P, Mruthyunjaya P, Mahmoud TH. Scleral buckling with chandelier illumination. J Ophthalmic Vis Res. 2016;11(3):304–309. doi:10.4103/2008-322X.188402
9. Assi A, Abdelmassih Y, El-Khoury S. Endoillumination-assisted modified scleral buckling. Retina. 2018;38(2):320–324. doi:10.1097/IAE.0000000000001568
10. Narayanan R, Tyagi M, Hussein A, Chhablani J, Apte RS. Scleral buckling with wide-angled endoillumination as a surgical educational tool. Retina. 2016;36(4):830–833. doi:10.1097/IAE.0000000000000792
11. Cohen E, Rosenblatt A, Bornstein S, Loewenstain A, Barak A, Schwartz S. Wide-angled endoillumination vs traditional scleral buckling surgery for retinal detachment – a comparative study. Clin Ophthalmol. 2019;13:287–293. doi:10.2147/OPTH.S182751
12. Yokoyama T, Kanbayashi K, Yamaguchi T. Scleral buckling procedure with chandelier illumination for pediatric rhegmatogenous retinal detachment. Clin Ophthalmol. 2015;9:169–217. doi:10.2147/OPTH.S75648
13. Weinstock RJ, Diakonis VF, Schiwartz AJ, Weinstock AJ. Heads-up cataract surgery: complication rates, surgical duration, and comparison with traditional microscopes. J Refract Surg. 2019;35(5):318–322. doi:10.3928/1081597X-20190410-02
14. Riemann CD Vision and vitrectomy three-dimensional high definition (3DHD) video for surgical visualization in the retina OR.
15. Eckardt C, Paulo EB. Heads-up surgery for vitreoretinal procedures: an experimental and clinical study. Retina. 2016;36:137–147. doi:10.1097/IAE.0000000000000689
16. Yonekawa Y. Seeing the world through 3-D glasses. Retina Today. 2016;11:54–60.
17. Kita M, Mori Y, Hama S. Hybrid wide-angle viewing-endoscopic vitrectomy using a 3D visualization system. Clin Ophthalmol. 2018;12:313–317. doi:10.2147/OPTH.S156497
18. Chihara T, Kita M. New type of antidrying lens for vitreous surgery with a noncontact wide-angle viewing system. Clin Ophthalmol. 2013;7:353–355.
19. Kita M, Fujii Y, Kawagoe N, Hama S. A new lens for observing fundus with a noncontact wide-angle viewing system. Clin Ophthalmol. 2018;12:313–317. doi:10.2147/OPTH.S156497
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.