Back to Journals » Clinical Ophthalmology » Volume 8
Unexpected and permanent central visual loss after removal of intraocular silicone oil
Authors Toso A, Cappello E, Morselli S ![]()
Received 14 May 2014
Accepted for publication 19 June 2014
Published 11 September 2014 Volume 2014:8 Pages 1831—1836
DOI https://doi.org/10.2147/OPTH.S67760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Antonio Toso, Ezio Cappello, Simonetta Morselli
Department of Ophthalmology, Saint Bassiano Hospital, Bassano del Grappa, Italy
Abstract: Here we report a case of unexplained sudden visual loss after removal of silicone oil for rhegmatogenous retinal detachment repair. A patient with visual loss in one eye after removal of silicone oil was investigated with best-corrected Snellen visual acuity assessment, fundus biomicroscopy, optical coherence tomography, color fundus photograph, fluorescein angiography, electrophysiologic examination, automated perimetry, and visual evoked potentials. Best-corrected Snellen visual acuity was 20/30 while the silicone oil was in place. Visual acuity dropped dramatically to 20/200 after silicone oil removal. No other complications associated with oil removal were noted. The retina remained attached. Visual evoked potentials revealed decreased amplitude due to a damaged optic nerve, while the earliest central visual field defects disappeared unexpectedly almost 2 years after the last surgical procedure. No other abnormalities were demonstrated. Vision loss is a possible complication of silicone oil and removal. This case was distinguished by the permanent decrease of visual acuity despite the unexplained and quite complete recovery of the foveal threshold with no other relevant visual field defects.
Keywords: central visual loss, intraocular silicone oil, removal
Introduction
Silicone oil is used as an intravitreal tamponading agent in vitreoretinal surgery for rhegmatogenous retinal detachment complicated by proliferative vitreoretinopathy or with large, multiple retinal tears. Usually, silicone oil is left in the posterior segment for at least 3 months. Although its use can lead to well-known complications, intraocular silicone oil is generally well tolerated. Some studies have reported unexpected and unexplained central vision loss due to deep central scotoma after silicone oil removal.1–5 A deep central scotoma within the central 10 degrees and a fallen foveal threshold can be clearly detected with automated perimetry. However, postoperative evaluations including optical coherence tomography and fluorescein angiography are sometimes uninformative. Multifocal electroretinography and pattern electroretinogram can indicate pathology within the macula as opposed to the optic nerve. Although several possible hypotheses have been proposed, no previous reports provide a solid conclusion regarding the etiopathological mechanisms of vision loss. We report a case of unexpected sudden central visual loss after silicone oil removal in uncomplicated pars plana vitrectomy for rhegmatogenous retinal detachment.
Case report
A 50-year-old man underwent 23-gauge pars plana vitrectomy for macula-off rhegmatogenous retinal detachment due to a large tear in the superior peripheral retina between 12 and 2 o’clock. Preoperative visual acuity was count fingers (February 2011). Triamcinolone acetonide-assisted surgery was performed through valved trocar cannulae, using a microsurgical system with integrated pressurized infusion and intraocular pressure compensation (Constellation®; Alcon Laboratories Inc., Fort Worth, TX, USA). Perfluorocarbon liquid was used to flatten the retina and laser treatment was performed to seal the retinal tear. Neither epimacular membrane removal nor inner limiting membrane peeling was performed. Following perfluorocarbon liquid-air exchange, ultrapurified 1,000 centistokes silicone oil was injected. During the same procedure, prior to vitrectomy, phacoemulsification of the crystalline lens and intraocular lens implantation were performed. Following this uncomplicated procedure, an intraocular pressure rise to 35 mmHg was reported a few days after surgery. A treatment regimen comprising a fixed combination of timolol 0.5% and latanoprost was successfully administered. The retina appeared to be completely attached, and the patient’s vision was good with a best-corrected visual acuity of 20/30 Snellen. After 11 weeks, silicone oil removal was performed under general anesthesia by using 23 gauge nonvalved trocars with a xenon-source light chandelier and without any coaxial fiber optic light. Passive removal was performed while maintaining an open infusion with balanced salt solution and allowing the silicone oil to float out of the vitreous cavity. During exchange, subretinal fluid suddenly appeared in the entire macular region. No unrelieved tractions were observed. It is likely that the laser treatment failed to seal the original large tear. Perfluorocarbon liquid was used as a solvent for the silicone oil and to evacuate the subretinal fluid and flatten the retina. No epimacular membrane peeling was performed. Additional laser treatment was performed around the previous laser retinal scars. Perfluorocarbon liquid was exchanged with air at the end of the procedure. After complete air reabsorption, the eye maintained a stable retinal situation and a normal intraocular pressure. Unexpectedly, however, central vision decreased, and visual acuity dropped dramatically to 20/200 and was maintained at that value. No posterior capsular opacity and macular abnormalities were observed during biomicroscopy. Two weeks after the second surgery, central 24 degree perimetry (Humphrey system; Carl Zeiss Meditec, Dublin, CA, USA) did not reveal any central defect but only a deep peripheral defect. However, the foveal threshold was zero dB (Figure 1), while the normal value is usually 30 dB or more. Although the intraocular pressure was successfully managed with topical medication, 2 months later, perimetry revealed a small central scotoma (9 dB) within the central 10 degrees with no foveal threshold improvement (Figure 2). This pattern remained stable over the following months. The central visual defect disappeared unexpectedly almost 2 years after the last surgical procedure, with a sensitivity increase to 28 dB and foveal threshold improvement from zero to 21 dB (Figure 3); visual acuity was still 20/200, and the patient did not experience any subjective improvement. He always reported persistent blurred vision only in the central visual field. Fluorescein angiography was unremarkable (Figure 4), and electrophysiology findings (electro-ocular retinography, and pattern and multifocal electroretinograms) were normal. Visual evoked potentials revealed decreased amplitude, probably due to a damaged optic nerve. B-scan images with high-resolution spectral domain optical coherence tomography (OCT; Cirrus HD-OCT, Carl Zeiss Meditec; RS-3000L SD-OCT, Nidek Co. Ltd., Gamagori, Japan; Spectralis OCT, Heidelberg Engineering Inc., Heidelberg, Germany), did not show any architectural abnormalities of the retinal layers (Figure 5). Tilting during acquisition made the Henle fiber layer prominent in the nasal area. The short hyperreflective line in the temporal border of the macula may have the same origin. A small shiny gray–white area adjacent to the foveal depression observed by “en face” scan OCT at the level of the inner limiting membrane (Figure 6) perfectly matched an area adjacent to the foveal depression observed on enhanced color fundus photography (Figure 7). However, B-scan did not show any defect in the area (Figure 8). Equally, OCT B-scan of the optic nerve head did not show remnants of silicone oil (Figure 9). Retinal nerve fiber layers findings were unreliable in both eyes due to the tilted optic disc. Furthermore, color fundus photography showed a slightly pale optic disc.
 | Figure 1 Central 24 degree perimetry from May 2011 showing peripheral deep defects and no defects within the 10 central degrees. Foveal threshold is zero dB (shown by oval gray line). |
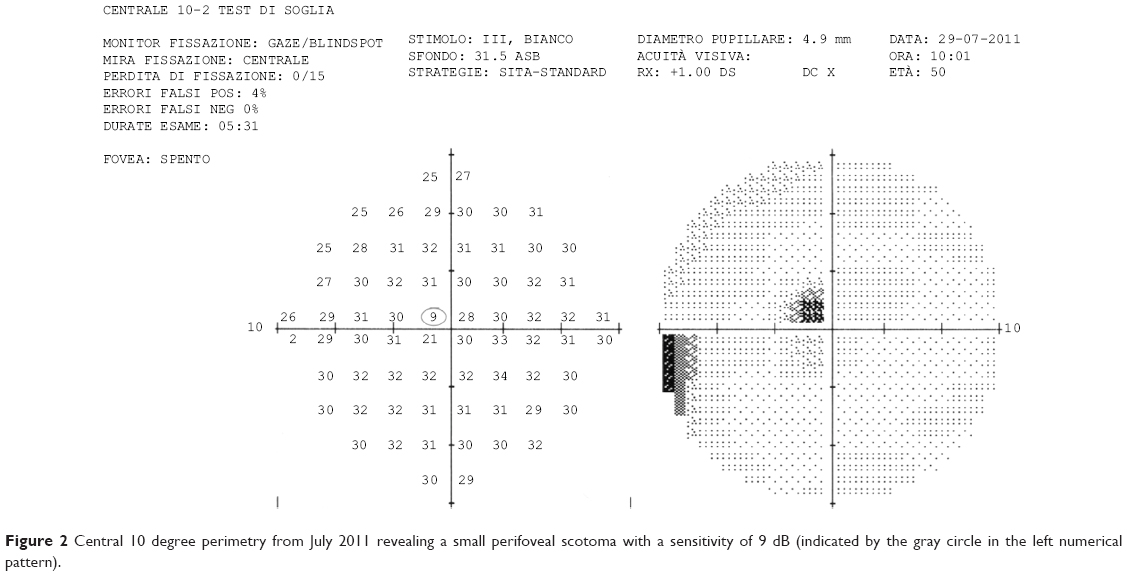 | Figure 2 Central 10 degree perimetry from July 2011 revealing a small perifoveal scotoma with a sensitivity of 9 dB (indicated by the gray circle in the left numerical pattern). |
 | Figure 3 Central 10 degree perimetry from April 2013 showing disappearance of the previous scotoma and sensitivity improvement to 28 dB at the same point (shown by gray circle in the left numerical pattern). Foveal threshold increased to 21 dB (shown by oval gray line). |
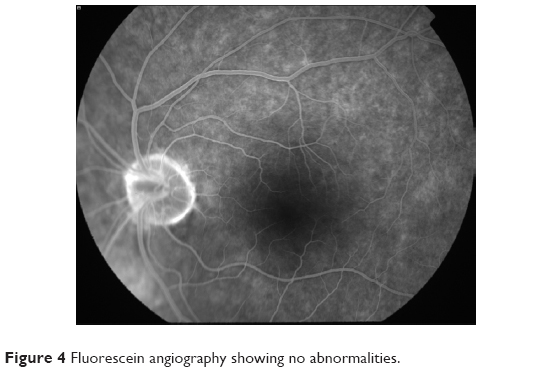 | Figure 4 Fluorescein angiography showing no abnormalities. |
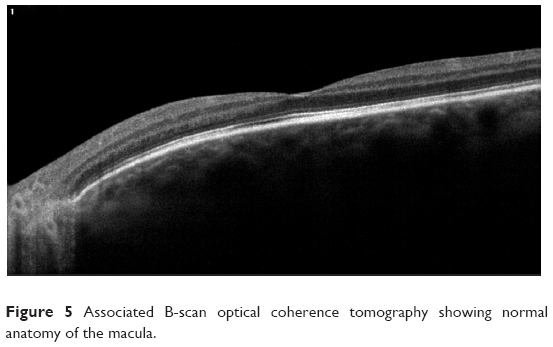 | Figure 5 Associated B-scan optical coherence tomography showing normal anatomy of the macula. |
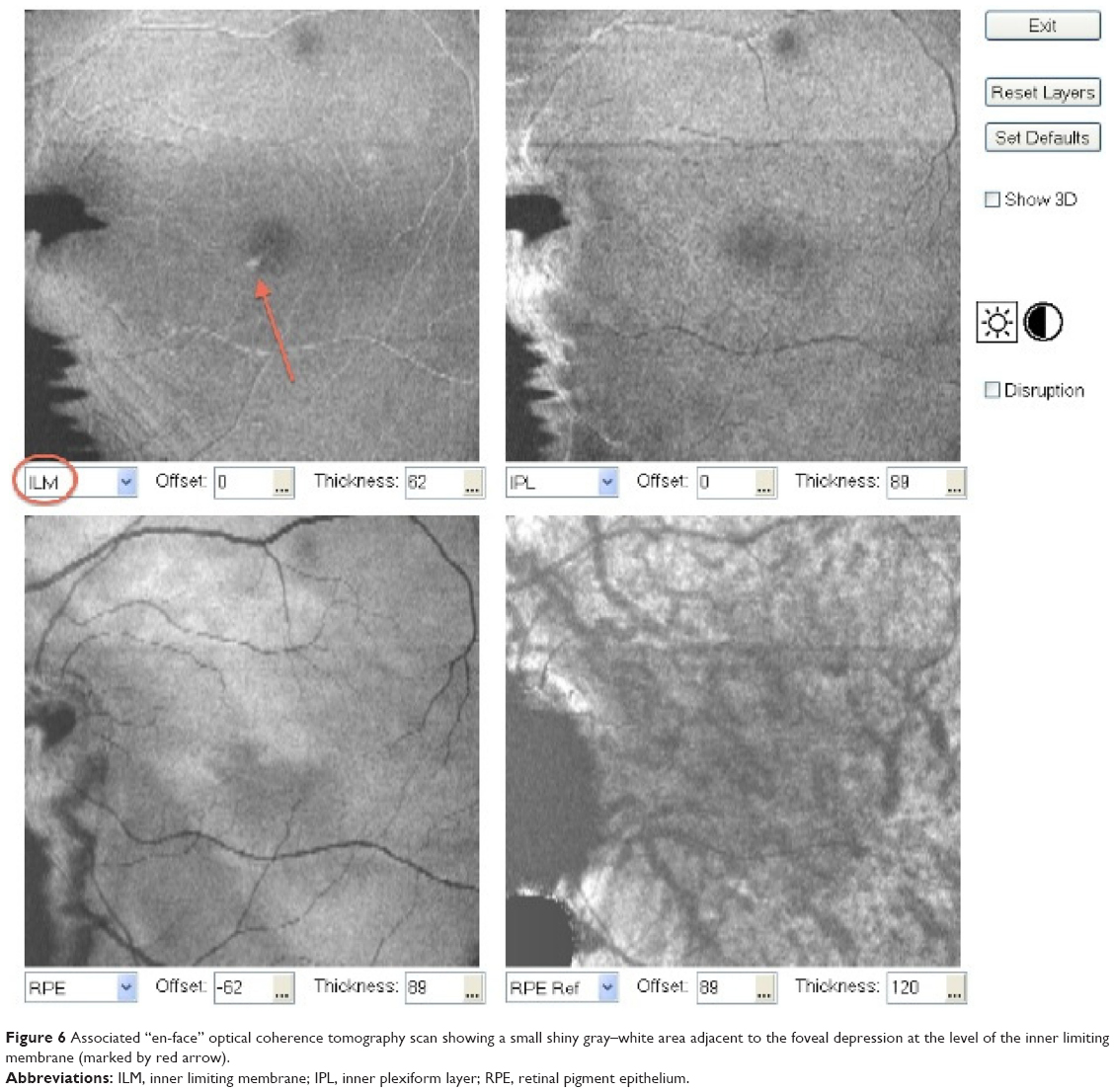 | Figure 6 Associated “en-face” optical coherence tomography scan showing a small shiny gray–white area adjacent to the foveal depression at the level of the inner limiting membrane (marked by red arrow). |
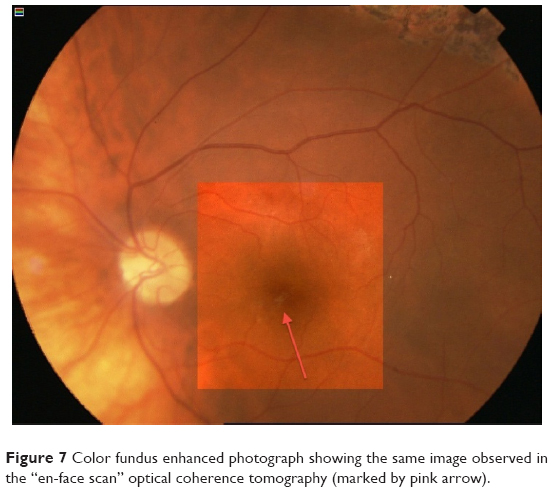 | Figure 7 Color fundus enhanced photograph showing the same image observed in the “en-face scan” optical coherence tomography (marked by pink arrow). |
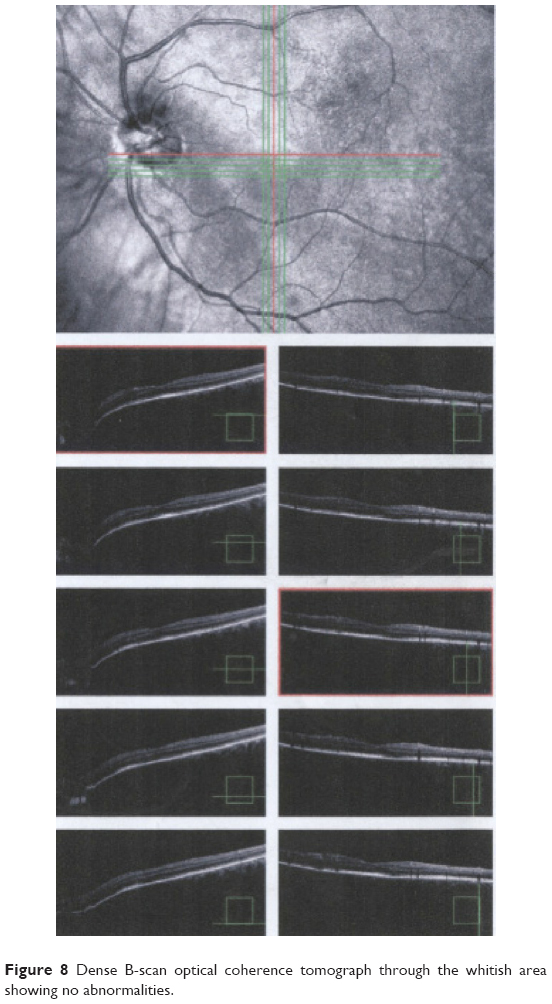 | Figure 8 Dense B-scan optical coherence tomograph through the whitish area showing no abnormalities. |
 | Figure 9 B-scan optical coherence tomographic image through the optic disc showing no silicone oil trapped. |
Discussion
Visual loss following silicone oil removal is not uncommon and has been described in some reports.1–5 It is also typically permanent. Although good visual acuity was recorded in the current case prior to silicone oil removal, an unexpected sudden decrease in visual acuity was observed after removal. A recent major review has considered potential etiologies of unexplained vision loss after pars plana vitrectomy.6 In light of this, the investigators focused on any macular abnormality and optic neuropathy. In the current case, no abnormalities based on fluorescein angiography or electrophysiology were demonstrated. An interesting case series described central scotoma associated with electroretinography suggestive of macular dysfunction that developed before oil removal.7 The only suspected sign in the macular region was the unexplained perifoveal image on the color fundus photograph and the en face scan with spectral domain OCT. An en face scan is capable of generating high-resolution cross-sectional images of deeper regions in the eye. The interpretation of these abnormal areas is challenging because it is quite difficult to attribute them to a residual silicone oil–fluid interface. Furthermore, the patient never developed cystoid macular edema or an epiretinal membrane. The unique objective sign of vision loss was recorded by visual evoked potentials that demonstrated optic nerve damage. This pattern might correspond to the deep peripheral defects observed on the first 24 degree perimetry. Regarding this visual evoked potential abnormality and central visual field defect, at no time did the patient exhibit persistent spikes in intraocular pressure, and the investigators never had solid reasons to suspect that glaucoma played an important etiological role in this case. However, the most unexplained phenomenon was the foveal threshold recovery observed in perimetry with the disappearance of the scotoma in the central 10 degrees. Nevertheless, the poor visual acuity of the patient did not improve and currently remains stable at 20/200.
In conclusion, the etiology of this sudden vision loss remains unclear. Further research is needed to explain the mechanism of central vision loss after silicone oil removal. We advocate an ongoing report of every similar case from other investigators to better understand such an adverse outcome and to develop measures that can be taken to avoid vision-threatening complications.
Disclosure
The authors report no conflicts of interest in this work.
References
Cazabon S, Groenewald C, Pearce IA, Wong D. Visual loss following removal of intraocular silicone oil. Br J Ophthalmol. 2005; 89:799–802. | ||
Herbert EN, Liew SH, Williamson TH. Visual loss after silicone oil removal. Br J Ophthalmol. 2005;89:1667–1668. | ||
Newsom RS, Johnston R, Sullivan PM, et al. Sudden visual loss after removal of silicone oil. Retina. 2004;24:871–877. | ||
Williams PD, Fuller CG, Scott IU, Fuller DG, Flynn HW. Vision loss associated with the use and removal of intraocular silicone oil. Clin Ophthalmol. 2008;2:955–959. | ||
Christensen UC, la Cour M. Visual loss after use of intraocular silicone oil associated with thinning of inner retinal layers. Acta Ophthalmol. 2012;90:733–737. | ||
Jain N, McCuen BW 2nd, Mruthyunjaya P. Unanticipated vision loss after pars plana vitrectomy. Surv Ophthalmol. 2012;57:91–104. | ||
Herbert EN, Habib M, Steel D, Williamson TH. Central scotoma associated with intraocular silicone oil tamponade develops oil removal. Graefes Arch Clin Exp Ophthalmol. 2006;244:248–252. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.