Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
Understanding the associations between psychosocial factors and severity of crime in juvenile delinquency: a cross-sectional study
Authors Taşkıran S, Mutluer T, Tufan AE ![]() , Semerci B
, Semerci B ![]()
Received 5 December 2016
Accepted for publication 9 February 2017
Published 18 May 2017 Volume 2017:13 Pages 1359—1366
DOI https://doi.org/10.2147/NDT.S129517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Sarper Taşkıran,1 Tuba Mutluer,2 Ali Evren Tufan,3 Bengi Semerci4,5
1Department of Child and Adolescent Psychiatry, Koç University School of Medicine, 2Child and Adolescent Psychiatry Department, Koç University Hospital, Istanbul, 3Department of Child and Adolescent Psychiatry, Abant Izzet Baysal University School of Medicine, Bolu, 4Department of Psychology, Hasan Kalyoncu University, Gaziantep, 5Bengi Semerci Enstitusu, Istanbul, Turkey
Purpose: Juvenile delinquency is a serious and common problem. To date, several studies have focused on possible psychosocial risk factors for delinquency among youths and on the implications of childhood mental illness on child criminality. However, the literature on prevalence of psychopathology and predictors of crime severity among delinquent youths in Turkey is sparse. Therefore, the aim of this study was to show the associations between crime severity and psychosocial factors such as gender, age, criminal history, concomitant attention deficit hyperactivity disorder (ADHD) and other comorbid psychiatric conditions, along with behavioral problem domains of Child Behavior Checklist (CBCL).
Participants and methods: This analytical cross-sectional study sample consisted of 52 individuals (30 females and 22 males) who were sent to a pilot detention facility in Istanbul, Turkey. The participants’ age ranged from 8 to 18 years (M =13.4; SD =2.9). Self-rating scales were administered in an interview format, and the crime severity information was provided by participants’ admission documents.
Results: No differences were found in terms of gender, age, children’s past history of crime and substance abuse. However, family crime history was significantly higher in the high severity crime group (P=0.026). Having one or more comorbid psychiatric disorder was associated with high crime severity (P=0.018). The most common psychiatric disorders were found to be ADHD, oppositional defiant disorder, conduct disorder (CD) and anxiety disorder.
Conclusion: Findings suggest that a family history of crime comes across as a very strong predictor of severity of crime. Among psychiatric factors, ADHD and CD were associated with commitment of more severe crimes in delinquent youths in our sample. Anxious/depressed traits as depicted by CBCL are found to be associated with less severe crimes.
Keywords: crime severity, delinquent behavior, ADHD, conduct disorder, risk factors, juvenile delinquency
Introduction
Juvenile delinquency is a serious and common problem that warrants a careful understanding of its psychosocial underpinnings. The prevalence of crime among youths was found to be 18.4% in a recent national survey in the US.1 There is an increased risk of adult criminality and tendency of poor personal outcomes for delinquent adolescents.2 Juvenile delinquency is on the rise in many countries. There is an 11.6% increase in the number of detained youths in Turkey in 2013 compared to that in the year before according to the Turkish Statistical Institute.3
To date, several studies have focused on possible psychosocial risk factors for delinquency among youths. Male gender,4 lower intellectual ability,5 race,6 adolescence age,7 immigration and poverty,4,8 association with delinquent peers,9 child maltreatment,10,11 academic achievement of youths12 and inadequate parental support13 have been demonstrated as precipitating risk factors. The concentration of crime within families and the intergenerational transmission of crime could be explained by environmental factors, genetic factors and a combination of these factors.14 Crime and other antisocial behaviors are shown to be heritable, with ~50% of the variance being explained by genetic factors.15
The implications of childhood mental illness on child criminality have been an area of interest in the recent years. It was found that 80% of young offenders had two or more psychiatric disorders according to the UK Office of National Statistics (ONS).16 Similar results were found in terms of the proportion of comorbid mental disorders in another large Finnish cohort study.17 The childhood mental illnesses that are mainly linked to child criminality are conduct disorder (CD), oppositional defiant disorder (ODD), attention deficit hyperactivity disorder (ADHD),18 alcohol use disorder (AUD),19 substance use disorder (SUD),20 depression,21 posttraumatic stress disorder (PTSD) and anxiety disorder.22
It has been consequently demonstrated that childhood conduct problems are developmental precursors of later criminality and antisocial behavior.2,23,24 Many studies have shown that almost 50% of offender youths fulfilled the diagnostic criteria of serious CD or antisocial personality disorder.25 Psychopathic traits often co-occur with conduct problems, and the characteristics of these traits are grandiosity, impulsiveness, arrogance, deceitfulness and lack of empathy.26 It was demonstrated that delinquent offenders with these traits commit more violent crimes and re-offend more frequently than non-psychopathic criminal youths.27
Virtually, all constructs of ADHD, such as impulsiveness, hyperactivity, restlessness, not considering consequences before acting, poor ability to plan ahead, low sense control, risk taking and poor ability to delay gratification, measured in different ways, are persistently associated with offending.28 Hyperactivity (restlessness and poor concentration) at the age of 11–13 years significantly anticipated arrest for violence in the Copenhagen Parenteral Project.29 According to the Pittsburgh ADHD Longitudinal Study (PALS), individuals with childhood ADHD + CD displayed significantly worse delinquency outcomes than ADHD only and ADHD + ODD groups.18
The literature on the prevalence of psychopathology and predictors of crime severity among delinquent youths in Turkey is sparse. Most of the studies30 on delinquent youths in Turkey depend on clinical unstructured interviews for determination of psychopathology. The prevalence of any psychiatric disorder was found to be 70.8%, and the prevalence for two or more psychiatric disorders was found to be 13.9% among criminal youths. The most relevant mental disorders were CD (38.1%) and SUD (11.1%) according to a Turkish study.30
Most of the literature tries to explore the relationship between mental illness and juvenile delinquency; however, there lies a gap in the literature on how mental illness affects severity of the committed crimes. Some psychiatric disorders, such as presence of CD and childhood ADHD, emerge as a predictor of more violent crimes.31 Investigation on the degree of violence or severity of the crimes is important because in addition to being a heavier burden for the society, it increases the time spent in the detention facilities and recidivism. In addition to ADHD and CDs, callous and unemotional traits are shown as robust predictors of more violent crimes.32 Callous and unemotional traits are inversely correlated with internalizing symptoms such as depression and anxiety symptoms. In this study, our primary hypotheses were to find increased ADHD, CD and ODD among most severe offenders and to find possibly less internalizing problems in this subgroup. As secondary hypotheses, we also wanted to explore the demographics such as gender, age, criminal history and familial characteristics of the offenders and show if family history of crime behavior emerges as an independent contributor to crime severity.
Participants and methods
Participants
The study sample consisted of 52 individuals (30 females and 22 males) who were sent to a pilot detention facility in Istanbul, Turkey. “Social Services and Children Protection Agency, Kemerburgaz – Ağaçli Protection, Maintenance and Rehabilitation Center” is a center acting as a detention facility for delinquent children and adolescents who are between the ages of 7 and 18 years. The center receives all types of offenders except those with the highest degree of crimes such as first-degree murder, who are sent to high-degree correctional facilities in the city. The center receives juvenile offenders aged <18 years from the entire Istanbul province. Hosting approximately one-fourth of the whole country, with a population of >18 million inhabitants, Istanbul province is a good representative of Turkish population at large. Sociodemographic features were obtained from the admission documents. All youths who were brought to the center between the years 2012 and 2013 were included in the study. There were no exclusion criteria. Participants’ age ranged from 8 to 18 years (M =13.4; SD =2.9).
Procedures
This research was designed as an analytical cross-sectional study. The institutional review board approval was obtained through the Turkish Ministry of Health, and all procedures were conducted according to the Declaration of Helsinki on Ethical Conduct of Clinical Studies. A team of psychologists and social workers evaluated the residents individually. Participation to this study was voluntary. The risks and benefits of the participation to this study were explained. There were no foreseen risks to the subjects from their participation in this study. However, if participants felt uncomfortable or unsafe due to the interview, they were offered support by a psychologist or psychiatrist from the research team. Written consent forms were obtained from all the participants who agreed to participate. Since most of the participants’ parents were unavailable at the time of the study and many of the participants were wards of the state, consent from individual health care proxies was obtained.
Instruments, including self-rating scales, were administered in an interview format due to frequent literacy problems in our population. The crime severity information was filled in by the research team after consulting the participant’s admission documents, which included official legal history. Parental history was obtained by self-report of adolescents whose parents could not be contacted. For teacher report forms, the teachers who best knew the resident were selected to fill out forms and surveys.
Instruments
Sociodemographic form
This form was specifically designed for this study by the research team. The questions included demographic information such as gender and age and criminal history of participants and their relatives.
Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children – Present and Lifetime Version (K-SADS-PL): a diagnostic interview in Turkish
The K-SADS-PL is a validated semi-structured diagnostic interview designed to assess current and past episodes of psychopathology in children and adolescents according to the Diagnostic and Statistical Manual of Mental Disorders, Third Edition – Revised (DSM-III-R) and DSM, Fourth Edition (DSM-IV) criteria.33 K-SADS-PL was translated to Turkish and was found to be reliable and valid.34 Following K-SADS-PL interviews, final diagnoses were confirmed by an experienced child and adolescent psychiatrist.
Conners’ Teacher Rating Scales for ADHD
Conners’ Rating Scales are validated assessment scales designed to assess ADHD symptoms in children and adolescents.35 They were translated in Turkish and were found to be reliable and valid.36,37
Child Behavior Checklist (CBCL) – Turkish version
The CBCL is a widely accepted and validated screening tool designed to identify behavioral and emotional problems in children and adolescents.38,39 For the purposes of this study, Youth Self Report and Teacher’s Report Form were provided to participants and to their Detention Center teachers. The Turkish versions are available and have been used in numerous studies on both community and clinical samples.40
Severity of crime
The severity of the crimes was gathered from the participants’ admission documents. We collected the data of individual crimes committed and then coded and assorted the data based on the National Criminal Justice Reference Service ranking system.41
Statistics
Continuous variables were first tested for normal distribution using the Shapiro–Wilk and Kolmogorov–Smirnov tests. Parametric tests and nonparametric (ie, Kruskal–Wallis) tests were used according to the distribution of data. Univariate logistic regression (LR) analyses were also performed for sociodemographic features, psychiatric comorbidities and T-scores of CBCL domains as a dichotomous outcome variable. Subsequently, multivariate prediction models with crime severity as a dichotomous outcome (with regard to median) variable were developed by considering all significant variables from the previous univariate analyses. SPSS (version 22) was used to make all statistical calculations on the data.
Results
A total of 52 adolescents with the mean age of 13±2.44 years (8–18 years) participated in the study. All the individuals agreed to participate in the study due to the willingness to spend extra time with psychologists. All documents were reviewed by the psychologists at the time of data collection: missing data were identified and were asked to be filled by the raters. Therefore, there were no missing data. A total of 56% (n=30) of patients were females and 42% (n=22) were males. Proportion and type of crime according to the National Crime Severity Survey Index (NCSSI) in the sample are given in Table 1. Sociodemographic information of patients and the associated crime severity status are given in Table 2.
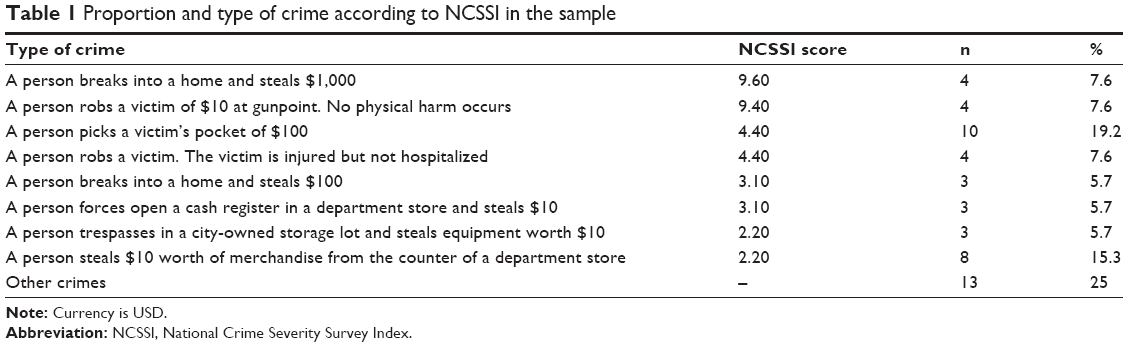 | Table 1 Proportion and type of crime according to NCSSI in the sample |
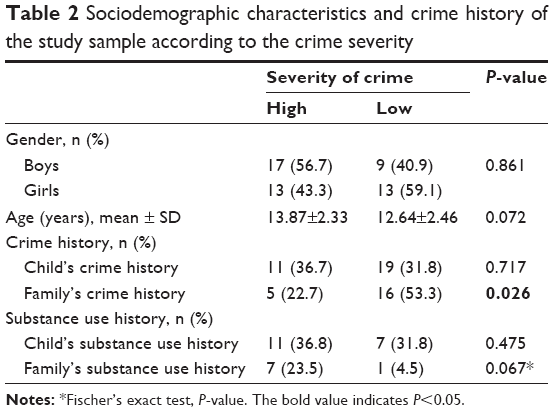 | Table 2 Sociodemographic characteristics and crime history of the study sample according to the crime severity |
First, we divided our sample into two groups according to total NCSSI median score. There were no predetermined cutoff points for NCSSI, so the median was used to dichotomize NCSSI scores. There were no between-group differences in terms of gender and age. In all, 30 (58%) adolescents had a history of at least one criminal act. A total of 21 (40%) children had a family history of crime. Children’s past history of crime did not differ (P=0.717), whereas family crime history was significantly higher in the high severity crime group (P=0.026). There was no difference between the two crime severity groups according to the substance use history of children or their families.
We found that having one or more comorbid psychiatric disorder is associated with high crime severity (P=0.018). The most common psychiatric disorders were ADHD, ODD, CD and anxiety disorder in our sample. Severity of crime was higher in youths with ADHD (P=0.04) and also in those with CD (P=0.019). We did not find significant differences in the ODD group (P=0.152) and the anxiety disorder group (P=0.74) in terms of crime severity (Table 3).
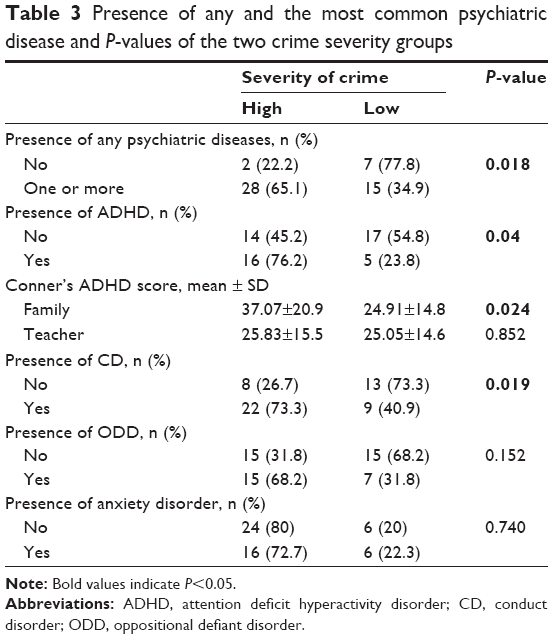 | Table 3 Presence of any and the most common psychiatric disease and P-values of the two crime severity groups |
None of the domains of CBCL domains significantly differentiated the high and low crime severity groups when the two groups were split according to the median. We then divided our total sample into two subgroups according to the NCSS score at 75th percentile (top severity group) to focus on the subjects with the most severe criminal acts. Anxious-depressed subscale score was significantly lower in the top crime severity group when compared to the low severity group (P=0.006; Table 4).
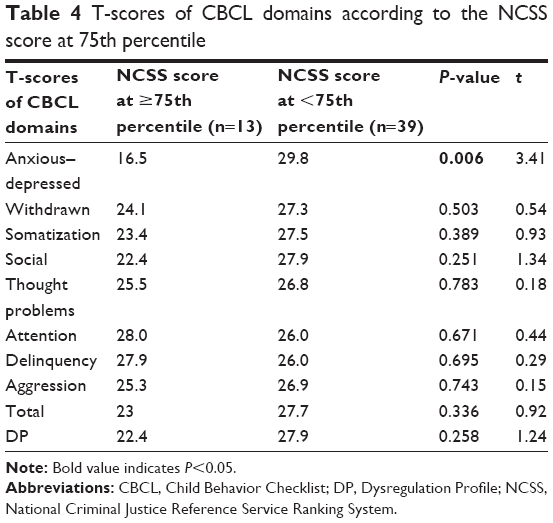 | Table 4 T-scores of CBCL domains according to the NCSS score at 75th percentile |
Finally, a multivariate prediction model with crime severity as a dichotomous outcome (regarding median) variable was developed by considering all significant variables from the previous univariate analyses (presence of ADHD, CD, family history of crime, CBCL anxious/depressed subscale, Conners’ ADHD scores). Binary LR analysis showed that while controlling for family history of crime, having higher T-scores of CBCL anxiety–depression domains leads to ~15% decrease (odds ratio [OR] =0.855) in crime severity (P=0.013). We found that, after adjusting for CBCL anxiety–depression scores, having a positive family history of crime increases the odds of committing more severe crimes ninefold (OR =9.16, P=0.007; Table 5).
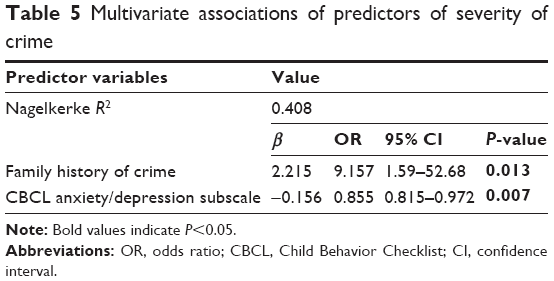 | Table 5 Multivariate associations of predictors of severity of crime |
Discussion
Understanding the psychiatric and psychosocial underpinnings of crime behavior is a complicated issue with multiple confounders. Heritable and environmental effects are often intertwined. There have been significant contributions to the field by trying to explain the precipitating factors of juvenile delinquency. It is important to know the basic relationship between psychiatric disorders and crime behavior, as it will serve as the key in designing programs for offenders with mental illness in an effort to decrease recidivism. Previous literature suggests that targeting symptoms of mental illness alone specifically does not help with recidivism in vast majority of offenders with mental illness, and psychiatric symptoms alone are not robust independent risk factors for criminal behavior. It is suggested that cognitive strategies that help cope with criminal behavior are also recommended in addition to treatment of underlying psychiatric symptoms.42
Although there are numerous reviews on the impact of mental illness on crime behavior, little is known about the factors that mediate the severity of the crimes committed. The implication of this knowledge would be profound as specific target groups within offenders can be identified as being at high risk for committing more severe crimes and be offered more rigorous follow-up and treatment programs.
In previous studies, male gender was significantly associated with the commission of a greater variety of crime.4,12 In our study, we did not find a significant relationship between crime severity and gender or age. However, both younger age and male gender were associated with a more severe criminal activity in other studies, which included longitudinal data.43,44 Our findings may be explained by a relatively small sample size and also a larger presence of female gender in our population.
Children’s past history of crime did not differ (P=0.717), whereas family crime history was significantly higher in the high severity crime group (P=0.026), which is in line with the current literature. We found that having a positive family history of crime increases crime severity in children (OR =9.16). Statistically significant associations were reported between violent crime in parents and violent crime in their children in population-based studies from Sweden45 and the Netherlands.46
There were no differences between the two crime groups according to substance use history of youths and their families; however, family substance use history showed a strong trend toward more severe crimes. The reason that this finding was not replicated in this study may be due to subjects’ concealment of the presence or extent of their substance use, as substance use history was only collected through self-report. Adolescent criminals tend to deny or minimize their substance use due to fear of additional charges being brought up against them.
In our sample, we found that having one or more comorbid psychiatric disorders was associated with high crime severity (P=0.018), which is in line with previous research.22,30 Severity of crime was significantly higher in youths with ADHD and also in those with CD, but not in the ODD and anxiety disorder groups. Findings of ADHD subjects can be explained by poor judgment and difficulties in impulse control. CD may increase severity of crime by lack of empathy and unemotional and callous traits, which render youths unable to feel responsible for the consequences of their actions. Our findings are in line with NCS-A analyses, which revealed that youths with CD, AUD and SUD demonstrated greater odds of crime involvement when compared to internalizing disorders such as anxiety and affective disorders.1 We find that it is important to discuss that diagnosis of ODD does not increase severity of crime. Although both disorders are listed as disruptive behavioral disorders, children with ODD have a milder course and are less likely to progress into antisocial personality disorder. Possible explanation of this finding could be having less callous and unemotional traits, which are tightly linked to criminal behavior.
Among T-scores of CBCL domains, only anxious-depressed subscale significantly differed between the two groups (P=0.006), and regression analysis showed that having higher T-scores of CBCL anxiety–depression domains causes 15% decrease in crime severity (P=0.007). It is interesting that the subjects who commit less severe crimes do not meet diagnostic criteria for anxiety or depression, but their CBCL profiles show higher scores. One explanation could be that they are more affected by their crimes committed and show sub-syndromal anxiety and depression scores, as opposed to being unburdened by them due to unemotional or callous traits. A second explanation could be that these subjects could have had more anxious/depressed traits at baseline, rendering them more inhibited, cautious and risk averse, thus committing crimes of less severity. Our findings in this sample suggest that CBCL anxious and depressed domains may be utilized as a marker for better prognostic outcome in terms of crime severity.
In the Pittsburgh Youth Study, Loeber et al47 showed how CBCL delinquency scores are related to progression or escalation of crime severity by using national survey crime severity rating.48 However, we did not find a significant relationship between crime severity and CBCL delinquency score. This may be explained by the fact that our study only included criminal offenders as opposed to general population; thus, each subject already had received high scores.
Given that the CBCL-Dysregulation Profile (DP) consists of the simultaneous elevation of three preexisting CBCL scales (attention, aggression and depression/anxiety) severe dysregulation could indicate comorbid internalizing and externalizing problems, such as co-occurring ADHD or ODD and depression.49 Meyer et al50 found that CBCL-DP in childhood was associated with marked psychosocial impairment, increased rates of suicidal thoughts and behaviors and heightened risk for anxiety disorder, bipolar disorder, cluster B personality disorder and ADHD in young adulthood. Our findings suggest that although DP is associated with heightened risk for ADHD and ADHD is associated with more severe crime, in our sample, DP score and crime severity did not show statistical correlation. There is also research showing that CBCL-DP profile is associated with severe mood dysregulation or the recent diagnosis of disruptive mood dysregulation disorder. We report that mood dysregulation, as measured by CBCL-DP, was not associated with higher severity of crime in our sample.
Limitations of the study
Several limitations of the study should be considered. Our study sample size was determined by the availability of residents in the detention center for a given period of time (1 year). Post hoc power analyses revealed power <0.8; thus, our study is underpowered. Our sample size is relatively small when compared to large studies that pool data from legal or social service systems. However, this provided us to thoroughly examine the sample at hand by using comprehensive tools such as K-SADS and CBCL ratings. Ağaçli Detention Facility is designed for juvenile offenders throughout Istanbul province. Many of the most severe offenders (with offenses such as murder) are sent to a high-degree correctional facility, which could lead to a selection bias in our sample. Information on family history for crime and psychiatric diseases was obtained from participants solely. This might have caused recall bias. In addition, interviewers knew that the participants were criminals and this might have affected their neutrality and objectivity, which might result in measurement bias.
Additionally, crime severity was evaluated from the participant’s admission documents, which were then sorted using the National Criminal Justice Reference Service ranking system. It is possible that this information may not represent the whole extent of their crimes committed, due to the fact that we included only registered offenses. This study is a cross-sectional evaluation. As a result, no inferences of causality or impact can be made, and a longitudinal study may have better predictive value of risk factors.
Conclusion
Our findings suggest that in our sample, a family history of crime comes across as having strong association with the severity of crime. Among psychiatric factors, ADHD and CD diagnoses are associated with commitment of more severe crimes in delinquent youths in this sample. Additionally, the study makes an important contribution to the existing literature on the likelihood of scoring lower on the CBCL-anxious–depressed subscale, which emerges as a factor that is associated with decreased crime severity. Better understanding of the relationship between crime severity and associated risk factors may provide an important tool to screen the youths at risk and design effective interventions for prevention or treatment. These factors should be carefully considered, especially in treatment and follow-up of delinquent youths. Providing preventive services and rehabilitation opportunities as early as possible to both the children and their family is imperative. More research with prospective longitudinal designs is required to demonstrate the impact of mental health disorders and traits on crime severity.
Acknowledgments
The study was funded by Koç University, without external grant funds. Psychologists affiliated with Turkish Ministry of Health and Ministry of Justice gave their time to the current study. The authors would also like to acknowledge the support and contribution of Aslihan Ozcan, MA, during the early stages of development of this manuscript.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Coker KL, Smith PH, Westphal A, Zonana HV, McKee SA. Crime and psychiatric disorders among youth in the US population: an analysis of the National Comorbidity Survey-Adolescent Supplement. J Am Acad Child Adolesc Psychiatry. 2014;53(8):888–898, 898.e1–e2. | ||
Moffitt TE, Caspi A, Harrington H, Milne BJ. Males on the life-course-persistent and adolescence-limited antisocial pathways: follow-up at age 26 years. Dev Psychopathol. 2002;14(1):179–207. | ||
Korkmaz MN, Erden G. Risk factors related to child delinquency. Türk Psikoloji Yazilari. 2010;13(25):76–87. | ||
Cheung C-K, Ngai N-P, Ngai SS-Y. Family strain and adolescent delinquency in two Chinese cities, Guangzhou and Hong Kong. J Child Fam Stud. 2007;16(5):626–641. | ||
Koolhof R, Loeber R, Wei EH, Pardini D, D’escury AC. Inhibition deficits of serious delinquent boys of low intelligence. Crim Behav Ment Health. 2007;17(5):274–292. | ||
Wright BRE, Younts CW. Reconsidering the relationship between race and crime: positive and negative predictors of crime among African American youth. J Res Crime Delinquen. 2009. | ||
Najman JM, Hayatbakhsh MR, McGee TR, Bor W, O’Callaghan MJ, Williams GM. The impact of puberty on aggression/delinquency: adolescence to young adulthood. Aust N Z J Criminol. 2009;42(3):369–386. | ||
Bal H. Toplumsal Eşitsizlik Temelinde Çocuk Suçluluğu (Isparta-Van Karşilaştirmasi). Sosyoloji Dergisi. 2007;17:293–311. | ||
Haynie DL, Osgood DW. Reconsidering peers and delinquency: how do peers matter? Soc Forces. 2005;84(2):1109–1130. | ||
Mann EA, Reynolds AJ. Early intervention and juvenile delinquency prevention: evidence from the Chicago Longitudinal Study. Soc Work Res. 2006;30(3):153–167. | ||
Mersky JP, Topitzes J, Reynolds AJ. Unsafe at any age linking childhood and adolescent maltreatment to delinquency and crime. J Res Crime Delinquen. 2012;49(2):295–318. | ||
Mancini JA, Huebner AJ. Adolescent risk behavior patterns: effects of structured time-use, interpersonal connections, self-system characteristics, and socio-demographic influences. Child Adolesc Soc Work J. 2004;21(6):647–668. | ||
Deng S, Roosa MW. Family influences on adolescent delinquent behaviors: applying the social development model to a Chinese sample. Am J Community Psychol. 2007;40(3–4):333–344. | ||
Farrington DP, Jolliffe D, Loeber R, Stouthamer-Loeber M, Kalb LM. The concentration of offenders in families, and family criminality in the prediction of boys’ delinquency. J Adolesc. 2001;24(5):579–596. | ||
Moffitt TE. The new look of behavioral genetics in developmental psychopathology: gene-environment interplay in antisocial behaviors. Psychol Bull. 2005;131(4):533. | ||
Lader D, Singleton N, Meltzer H. Psychiatric morbidity among young offenders in England and Wales. Int Rev Psychiatry. 2003;15(1–2):144–147. | ||
Sailas ES, Feodoroff B, Virkkunen M, Wahlbeck K. Mental disorders in prison populations aged 15-21: national register study of two cohorts in Finland. BMJ. 2005;330(7504):1364–1365. | ||
Sibley MH, Pelham WE, Molina BS, et al. The delinquency outcomes of boys with ADHD with and without comorbidity. J Abnorm Child Psychol. 2011;39(1):21–32. | ||
Elbogen EB, Johnson SC. The intricate link between violence and mental disorder: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2009;66(2): 152–161. | ||
Cuellar AE, Markowitz S, Libby AM. Mental health and substance abuse treatment and juvenile crime. J Ment Health Policy Econ. 2004;7(2):59–68. | ||
Harrington RC. Childhood depression and conduct disorder: different routes to the same outcome? Arch Gen Psychiatry. 2001;58(3):237–238. | ||
Pliszka SR, Sherman JO, Barrow MV, Irick S. Affective disorder in juvenile offenders: a preliminary study. Am J Psychiatry. 2000;157(1):130–132. | ||
Sourander A, Jensen P, Davies M, et al. Who is at greatest risk of adverse long-term outcomes? The Finnish from a boy to a man study. J Am Acad Child Adolesc Psychiatry. 2007;46(9):1148–1161. | ||
Diamantopoulou S, Verhulst FC, van der Ende J. Testing developmental pathways to antisocial personality problems. J Abnorm Child Psychol. 2010;38(1):91–103. | ||
Fazel S, Danesh J. Serious mental disorder in 23000 prisoners: a systematic review of 62 surveys. Lancet. 2002;359(9306):545–550. | ||
Cooke DJ, Michie C. Refining the construct of psychopathy: towards a hierarchical model. Psychol Assess. 2001;13(2):171–188. | ||
Spain SE, Douglas KS, Poythress NG, Epstein M. The relationship between psychopathic features, violence and treatment outcome: the comparison of three youth measures of psychopathic features. Behav Sci Law. 2004;22(1):85–102. | ||
Pratt TC, Cullen FT, Blevins KR, Daigle L, Unnever JD. The relationship of attention deficit hyperactivity disorder to crime and delinquency: a meta-analysis. Int J Police Sci Manage. 2002;4(4):344–360. | ||
Brennan PA, Mednick BR, Mednick SA. Parental psychopathology, congenital factors, and violence. Mental Disorder and Crime. Thousand Oaks, CA: SAGE; 1993:244–261. | ||
Beşer NG, Arabaci LB, Uzunoğlu G. The profiles of children pushed to crime who are treated in a regional psychiatric hospital in Turkey. Anadolu Psikiyatri Derg. 2016;17(4):317–324. | ||
Young S, Thome J. ADHD and offenders. World J Biol Psychiatry. 2011;12(suppl 1):124–128. | ||
Pardini DA, Fite PJ. Symptoms of conduct disorder, oppositional defiant disorder, attention-deficit/hyperactivity disorder, and callous-unemotional traits as unique predictors of psychosocial maladjustment in boys: advancing an evidence base for DSM-V. J Am Acad Child Adolesc Psychiatry. 2010;49(11):1134–1144. | ||
Lauth B, Arnkelsson GB, Magnusson P, Skarpheethinsson GA, Ferrari P, Petursson H. Validity of K-SADS-PL (Schedule for affective disorders and schizophrenia for school-age children – present and lifetime version) depression diagnoses in an adolescent clinical population. Nord J Psychiatry. 2010;64(6):409–420. | ||
Gökler B, Ünal F, Pehlivantürk B, Kültür EÇ, Akdemir D, Taner Y. Reliability and validity of schedule for affective disorders and schizophrenia for school age children-present and lifetime version-Turkish version (K-SADS-PL-T). J Child Adolesc Mental Health. 2004;11(3):109–116. Çocuk ve Gençlik Ruh Sağliği Dergisi/Turkish. | ||
Conners CK, Sitarenios G, Parker JD, Epstein JN. Revision and restandardization of the Conners Teacher Rating Scale (CTRS-R): factor structure, reliability, and criterion validity. J Abnorm Child Psychol. 1998;26(4):279–291. | ||
Kaner S, Buyukozturk S, Iseri E, Ak A, Ozaydin L. Conners’ parent rating scale long form-revised: factor structure, reliability and validity studies. Turk J Child Adolesc Ment Health. 2011;18(1):45–58. | ||
Dereboy Ç, Şenol S, Şener Ş, Dereboy F. Conners anababa derecelendirme ölçeği uyarlama çalişmasi. X Ulusal Psikoloji Kongresi, Ankara; 1998. | ||
Achenbach TM. Manual for the Child Behavior Checklist/4-18 and 1991 profile. Department of Psychiatry. Burlington, VT: University of Vermont; 1991. | ||
Achenbach TM, Rescorla L. ASEBA School-Age Forms & Profiles. Burlington, VT: ASEBA; 2001. | ||
Erol N, Arslan B, Akçakin M. The adaptation and standardization of the child behavior checklist among 6–18 year-old Turkish children. Eunethdis: European Approaches to Hyperkinetic Disorder. Zürih: Fotoratar; 1995:97–113. | ||
Wolfgang ME, Figlio RM, Tracy PE, Singer SI. The National Survey of Crime Severity. Washington, DC: US Department of Justice, Bureau of Justice Statistics; 1985. | ||
Peterson JK, Skeem J, Kennealy P, Bray B, Zvonkovic A. How often and how consistently do symptoms directly precede criminal behavior among offenders with mental illness? Law Hum Behav. 2014;38(5):439–449. | ||
Kinlock TW, O’Grady KE, Hanlon TE. Prediction of the criminal activity of incarcerated drug-abusing offenders. J Drug Issues. 2003;33(4):897–920. | ||
Gordon MS, Kinlock TW, Schwartz RP, Couvillion KA, O’Grady KE. The severity, frequency, and variety of crime in heroin-dependent prisoners enrolled in a buprenorphine clinical trial. Prison J. 2013;93(4):390–410. | ||
Frisell T, Lichtenstein P, Langstrom N. Violent crime runs in families: a total population study of 12.5 million individuals. Psychol Med. 2011;41(1):97–105. | ||
Bijleveld CC, Wijkman M. Intergenerational continuity in convictions: a five-generation study. Crim Behav Ment Health. 2009;19(2):142–155. | ||
Loeber R, Stouthamer-Loeber M, Van Kammen W, Farrington DP. Initiation, escalation and desistance in juvenile offending and their correlates. J Crim Law Criminol. 1991;82:36–82. | ||
Wolfgang ME, Figlio RM, Tracy PE, Singer SI. National Survey of Crime Severity. Washington, DC: University of Pennsylvania; 1985. | ||
Holtmann M, Buchmann AF, Esser G, Schmidt MH, Banaschewski T, Laucht M. The Child Behavior Checklist-Dysregulation Profile predicts substance use, suicidality, and functional impairment: a longitudinal analysis. J Child Psychol Psychiatry. 2011;52(2):139–147. | ||
Meyer SE, Carlson GA, Youngstrom E, et al. Long-term outcomes of youth who manifested the CBCL-Pediatric Bipolar Disorder phenotype during childhood and/or adolescence. J Affect Disord. 2009;113(3):227–235. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.