Back to Journals » Clinical Ophthalmology » Volume 19
Understanding Keratoconus in Down Syndrome: From Etiology to Management – A Narrative Review
Authors Anitha V, Nallasamy N, Christy JS, Kristianslund O ![]() , Stephenson KAJ
, Stephenson KAJ ![]() , Hashemi H
, Hashemi H ![]() , Rajaraman R, Asgari S
, Rajaraman R, Asgari S
Received 27 July 2025
Accepted for publication 12 December 2025
Published 30 December 2025 Volume 2025:19 Pages 4925—4939
DOI https://doi.org/10.2147/OPTH.S556378
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Venugopal Anitha,1 Nambi Nallasamy,2 Josephine S Christy,3 Olav Kristianslund,4 Kirk AJ Stephenson,5 Hassan Hashemi,6 Revathi Rajaraman,7 Soheila Asgari8
1Department of Cornea & Refractive Services, Aravind Eye Hospital and Postgraduate Institute of Ophthalmology, Tirunelveli, TN, India; 2Department of Ophthalmology and Visual Sciences, Kellogg Eye Centre, Ann Arbor, MI, USA; 3Department of Cornea & Refractive Services, Aravind Eye Hospital, Pondicherry, India; 4Department of Ophthalmology, Oslo University Hospital, Oslo, Norway; 5Department of Ophthalmology, Royal Victoria Eye & Ear Hospital, Dublin, Ireland; 6Department of Ophthalmology, Noor Research Centre for Ophthalmic Epidemiology, Noor Eye Hospital, Tehran, Iran; 7Department of Cornea & Refractive services, Aravind Eye Hospital, Coimbatore, TN, India; 8Department of Ophthalmology, Noor Ophthalmology Research Centre, Noor Eye Hospital, Tehran, Iran
Correspondence: Venugopal Anitha, Department of Cornea & Refractive services, Aravind Eye Hospital and postgraduate institute of Ophthalmology, S.N High Road, Tirunelveli, TN, India, Tel +91 9442930404, Email [email protected]
Abstract: Paediatricians are often the first to identify children with DS and their awareness on associated ocular comorbidities, play a critical role in ensuring timely referral to general ophthalmologists for diagnosis and management. Among these, keratoconus (KC) has a significantly higher prevalence among Down syndrome (DS) compared to the general population. The awareness and understanding of KC, is essential for preventing vision loss. This review summarizes the current understanding of KC in DS, on epidemiology, pathophysiology, diagnostic challenges, and management. The children with DS, have thinner and steeper corneas since birth, complicates the diagnostic and management protocols. Poor cooperation of the children for imaging, compromised scan qualities, need for sedation and repeatability of scans poses diagnostic challenges. Early intervention with corneal cross-linking (CXL) is shown to be effective in halting disease progression. The surgical options in advanced cases, carry higher risks in DS patients due to factors such as eye rubbing, increased infection rates, and challenges in postoperative compliance. Managing KC in DS requires a comprehensive approach involving early referral by Paediatricians, pre-emptive diagnosis, and timely intervention with CXL to prevent disease progression. Future research should focus on preclinical gene prediction and developing standardized screening protocols for KC among DS to prevent vision loss and thereby improve quality of life among them.
Keywords: keratoconus, acute hydrops, down syndrome, corneal tomography
Introduction
In 1736, Benedict Duddell described keratoconus (KC) in a 14-year-old albino boy with nystagmus and cone-shaped corneas. Renamed “Staphyloma Diaphanum” by Burchard Mauchart in 1748, Johann Horner coined the term keratoconus in 1869. By 1989, increased enzymatic activity was linked to corneal thinning and vision distortion.1 KC is typically sporadic,2 with rising incidence and prevalence over the past two decades due to heightened awareness and advanced diagnostic techniques.2,3 It is associated with genetic and multi-system disorders,1,4 including Down syndrome (DS), which affects 1 in 800 births and is linked to conditions such as congenital cardiac disease, thyroiditis, and neurological issues. Ocular manifestations in DS include refractive errors (20–50%), strabismus (33–57%), KC (15–71%), and nystagmus (11–29%).1,5,6 Trisomy 21 is the primary cause of DS (92–95%). Improved medical care has increased life expectancy for children with DS from 9 years in 1910 to 49 years in 1997. KC incidence in DS (0–71%) is 10–300 times higher than in the general population (1 in 350).7,8 Woodward et al highlighted a high odds ratio of KC with sleep apnea, asthma, and DS, though consensus on this link remains elusive.9 Walsh et al reported a 7.7% incidence of KC in 91 DS patients compared to 0.3% in 378 patients with other intellectual disabilities.10 Mental disabilities in DS hinder early reporting of visual issues. This review provides updated insights on KC’s etiology, epidemiology, and outcomes in DS, emphasizing the need for early diagnosis and screening to prevent advanced KC-related blindness.
Methodology of Literature Search
A comprehensive literature search was conducted in August 2021 using PubMed Central, Google Scholar, EMBASE, the Register of Controlled Trials, and Ovid MEDLINE to identify studies on ophthalmic manifestations in Down syndrome (DS). The search strategy combined keywords such as “Down Syndrome”, “Trisomy 21”, “children”, “ocular manifestations”, and specific conditions like “strabismus”, “nystagmus”, and “keratoconus”. Inclusion criteria focused on studies involving DS patients, emphasizing genetic insights, etiology, diagnosis, and management of keratoconus. We included randomized controlled trials, observational studies, case reports, and systematic reviews, with no language or publication year restrictions. Excluded were non-peer-reviewed articles and studies unrelated to ophthalmic manifestations in DS. Relevant studies were screened by titles and abstracts, and full texts were reviewed for inclusion. Data extraction centered on prevalence, condition types, and clinical findings. Study quality was assessed using tools like the Cochrane Risk of Bias tool and the Newcastle-Ottawa Scale, ensuring a thorough review for clinical insights.
Epidemiology
The prevalence of keratoconus (KC) is influenced by environmental factors, ethnicity, geography, available diagnostic tools, and patient cohorts. In the general population, KC prevalence varies widely, from 0.0003% in Russia to 2.3% in central India, depending on diagnostic criteria. For example, using corneal refractive power >48D, prevalence is 2.3%, but decreases to 0.6% and 0.1% for >49D and >50D, respectively. DS is linked to a higher KC prevalence due to habitual eye rubbing, atopy, blepharitis, and genetic predisposition to thin, steep corneas.11,12 Reported KC incidence in DS, ranges from 0% to 71%, with lower rates in younger age groups. Corneal topography studies show prevalence rates of 10–30% or higher. Norway’s registry estimated a 5.5% KC prevalence in DS, thirty times higher than in the general population, while a Brazilian study found 27.2% prevalence among 1207 DS patients.12–14 Conversely, Kim et al found no KC in 123 Asian DS children. The global variation in KC prevalence among DS individuals is unclear, and some studies suggest lower rates in Asian DS populations, possibly due to age differences or lack of corneal tomography.15 Gender distribution in KC shows male predominance in general studies, though data on DS populations is limited. Alio et al found a 71.3% KC prevalence in DS patients with a mean age of 14.9 years, underlining the condition’s significant presence in this group.16
Corneal Anatomical and Biomechanical Alterations and Its Implications in DS
In DS patients, the cornea shows significant anatomical and biomechanical differences compared to non-DS individuals. DS corneas have steeper mean keratometry (47.35D vs 43.7D) and thinner central corneal thickness (0.50mm vs 0.55mm). Structural changes include reduced collagen, deficient interlacing, low prolidase activity affecting collagen turnover, and altered COL A1 and COL A2 expression, leading to decreased corneal rigidity and volume.17 Increased corneal density and light scatter reduce transparency and impact visual function.18 Haugen et al noted corneal thinning contributes to steepness, astigmatism, and reduced rigidity. Early screening and intervention for KC in DS are crucial to prevent disease progression.19 Box 1 and Table 1 show the detailed summary of these anatomical and biomechanical characteristics.
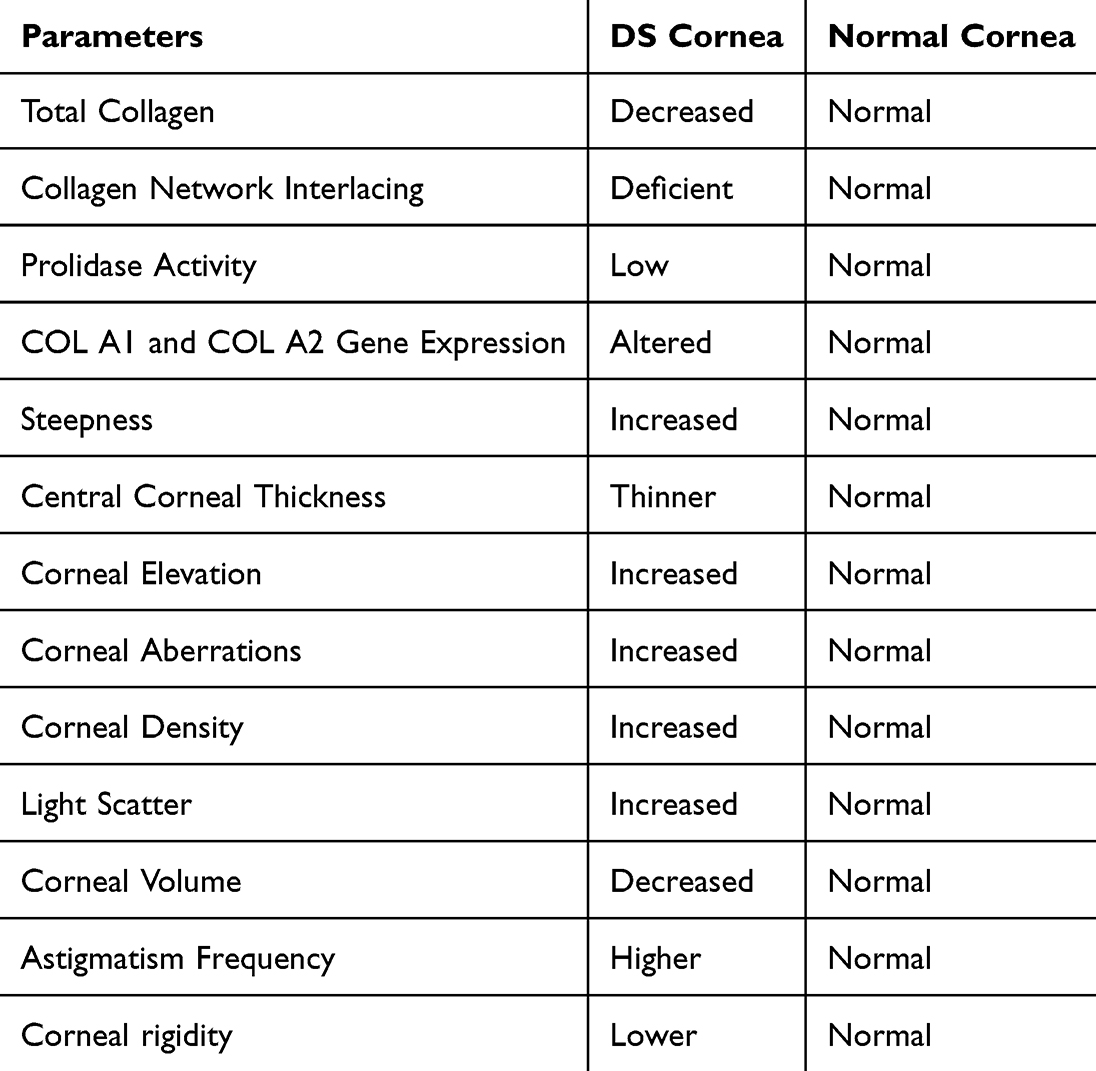 |
Table 1 Shows the Summary of Key Points on Anatomical and Biomechanical Alterations Between DS and Non-DS Corneas |
 |
Box 1 Corneal anatomical & biomechanical concerns in DS patients |
Etiology of Keratoconus in Down Syndrome
The etiology of keratoconus (KC) is multifactorial, involving genetic predispositions and environmental influences that contribute to corneal biomechanical weakness, reflected in a 60% reduction in corneal stiffness. Despite extensive research, a definitive cause for KC remains elusive.2 The understanding of KC in Down syndrome (DS) requires exploring genetic factors and environmental triggers, emphasizing the need for further studies to establish targeted management strategies. Table 2 shows the Etiology of Keratoconus in Downs Syndrome.
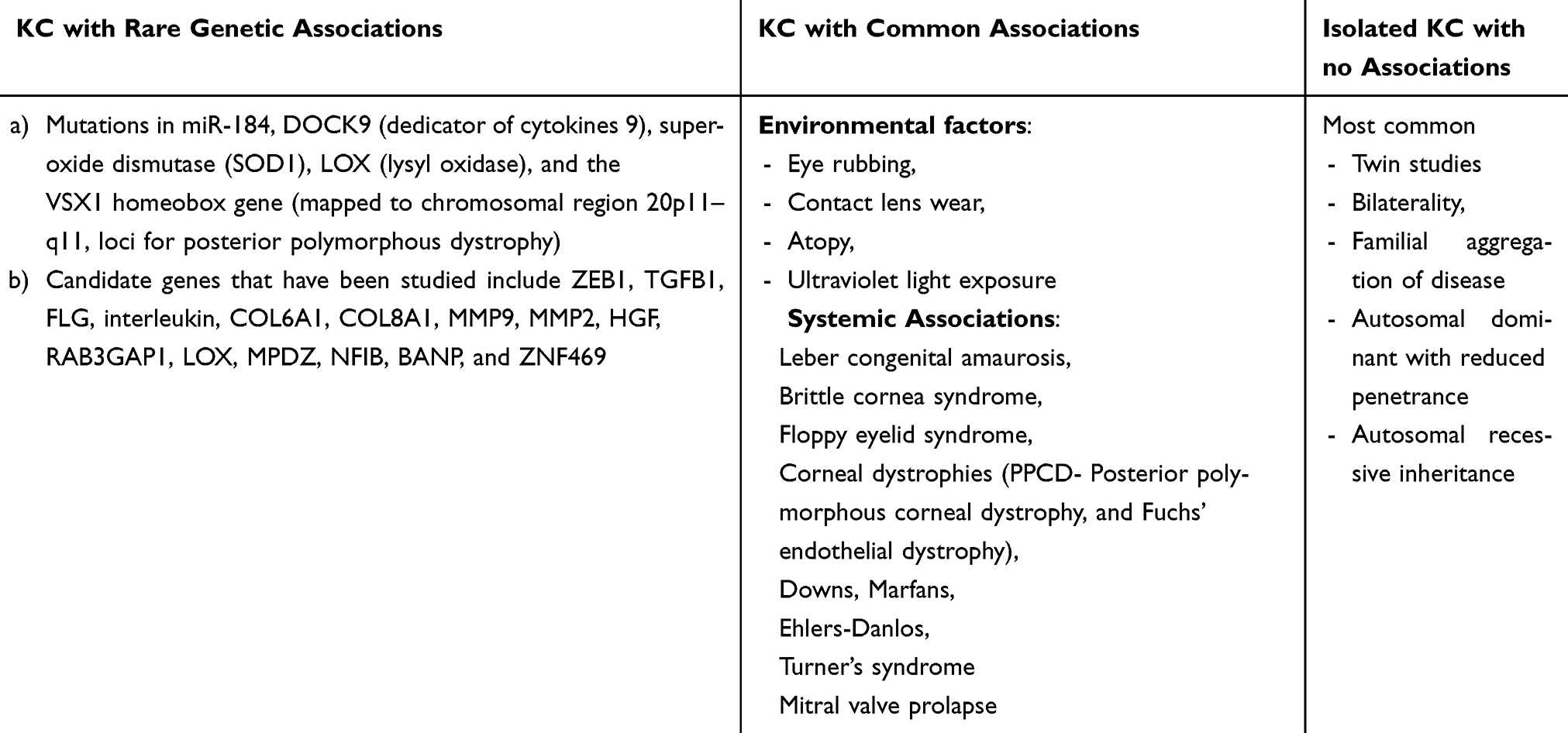 |
Table 2 Etiology of Keratoconus in Downs Syndrome |
Genetic Insights
Genetic factors play a crucial role in KC development, shown by familial associations (1.7%–23.5%), higher concordance in monozygotic twins, and connections with genetic disorders. KC is often classified as associated with rare genetic syndromes, commonly reported conditions, or isolated cases. Evidence from twin studies and familial clustering supports a genetic component, though monozygotic twin discordance suggests environmental factors also contribute. KC is associated with conditions like Leber congenital amaurosis, Marfans syndrome, Ehlers-Danlos syndrome, and DS. The inheritance pattern is typically autosomal dominant with reduced penetrance, though autosomal recessive cases exist.2,10,20
Rabinowitz studies indicated that 50% of KC cases in families show early signs, often underreported due to lack of topography-based diagnosis. Research has identified at least 17 loci linked to KC, with significant associations found in genes like miR-184, DOCK9, SOD1, LOX, and collagen-related genes (eg, COL6A1, COL8A1). The SOD1 gene, located on chromosome 21, is linked to both KC and DS due to its role in reducing oxidative stress.2,10 A Greek study identified a unique SOD1 polymorphism associated with KC, as a cytoplasmic antioxidant enzyme, SOD metabolizes harmful superoxide radicals to harmless oxygen and hydrogen peroxide and reduces oxygen toxicity.21–23 A Norwegian data showed KC incidence in DS as 30 times higher than the general population.12,24 Lu et al’s meta-analysis highlighted reduced central corneal thickness (CCT) in KC, implicating collagen-related genetic loci.25 Although key candidate genes are identified, genetic heterogeneity and gene-environment interactions require further study to clarify heritability and pathophysiology.21 Table 3, shows the list of genes commonly noted in the literature between DS and KC associated with Chromosome 21 and Table 4 summarizes the evidences of genetic associations between DS and KC.
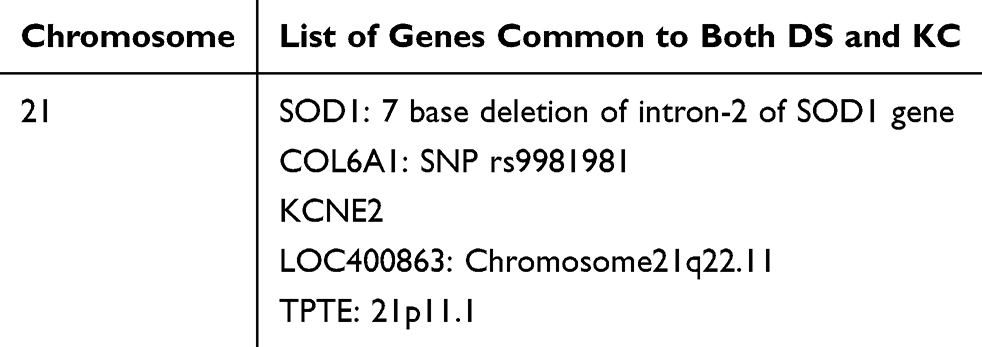 |
Table 3 List of Genes Commonly Noted in the Literature Between DS & KC Associated with Chromosome 21 |
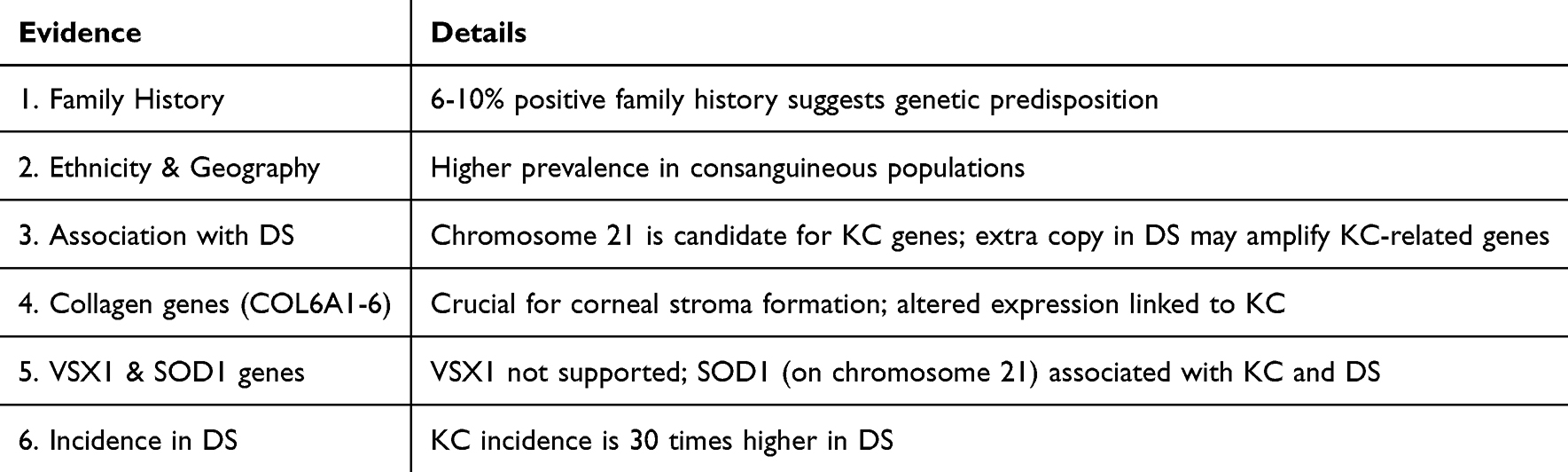 |
Table 4 Summarizes the Evidences of Genetic Associations Between DS and KC |
Environmental Factors
Environmental factors also influence KC development, including age, gender, ethnicity, eye rubbing, and oxidative damage from UV exposure. Eye rubbing, common in DS due to atopic conjunctivitis, blepharitis, and uncorrected refractive errors, is a significant mechanical contributor. Repeated eye rubbing triggers inflammatory cytokine release from damaged corneal and conjunctival epithelium, leading to keratocyte apoptosis.20 Kim et al’s findings revealed increased apoptotic keratocytes in 60% of KC corneas compared to 35% in stromal dystrophies. Additionally, KC fibroblasts express higher interleukin-1 (IL-1) receptor levels, mediating local inflammation, suggesting a potential genetic basis for this response. Overall, the etiology of KC in DS is multifactorial, involving genetic and mechanical factors.15 The combination of genetic predispositions, such as those related to SOD1 and collagen genes, and mechanical stressors like intense eye rubbing, contributes to disease progression.10 Understanding these interactions is vital for developing targeted preventive and therapeutic approaches for DS patients. Further research is necessary to elucidate the genetic mechanisms, establish causative links, and guide effective clinical interventions.
Clinical Characteristics
Keratoconus (KC) is a progressive eye disease marked by visual disturbances from high myopia and irregular astigmatism. A thorough history focusing on refractive instability is essential to determine onset. Risk factors include vernal keratoconjunctivitis, eye rubbing, systemic atopy, and family history, aiding in early identification. Proper documentation of uncorrected (UCVA) and best corrected visual acuity (BCVA) is vital for treatment planning. Early-stage KC can often be managed with glasses, while advanced cases may require contact lenses. The clinical signs of KC are explained in Table 5.26 Acute corneal hydrops (CH) is significantly more frequent in DS patients with KC (up to 15%) than in non-DS individuals (2.5–3%).27,28 Figure 1 shows the image with acute corneal hydrops in a patient with DS. DS patients are more prone to delayed diagnosis due to unique corneal features, increasing CH risk and central scarring. Figure 2 shows the image with corneal scarring, sequelae of acute corneal hydrops. Initial CH treatments include topical hypertonic drops, low potency steroids, and advanced interventions like compressive sutures or amniotic membrane transplantation. Figure 3 shows the post-operative picture of compressive sutures with pneumodescemetopexy for hydrops intractable to medical treatment. Figure 4 shows the multiple loose suture with debris, infiltrates with central epithelial defect and graft stromal rejection, in a patient with DS. Early identification and treatment are critical to preventing severe visual impairment in DS patients with KC. Figure 5 shows the treatment algorithm for KC in DS with intellectual disability. Figure 6 shows the image of advanced Keratoconus in a patient with DS. Figure 7 shows the post healed hydrops scar managed with compression sutures.
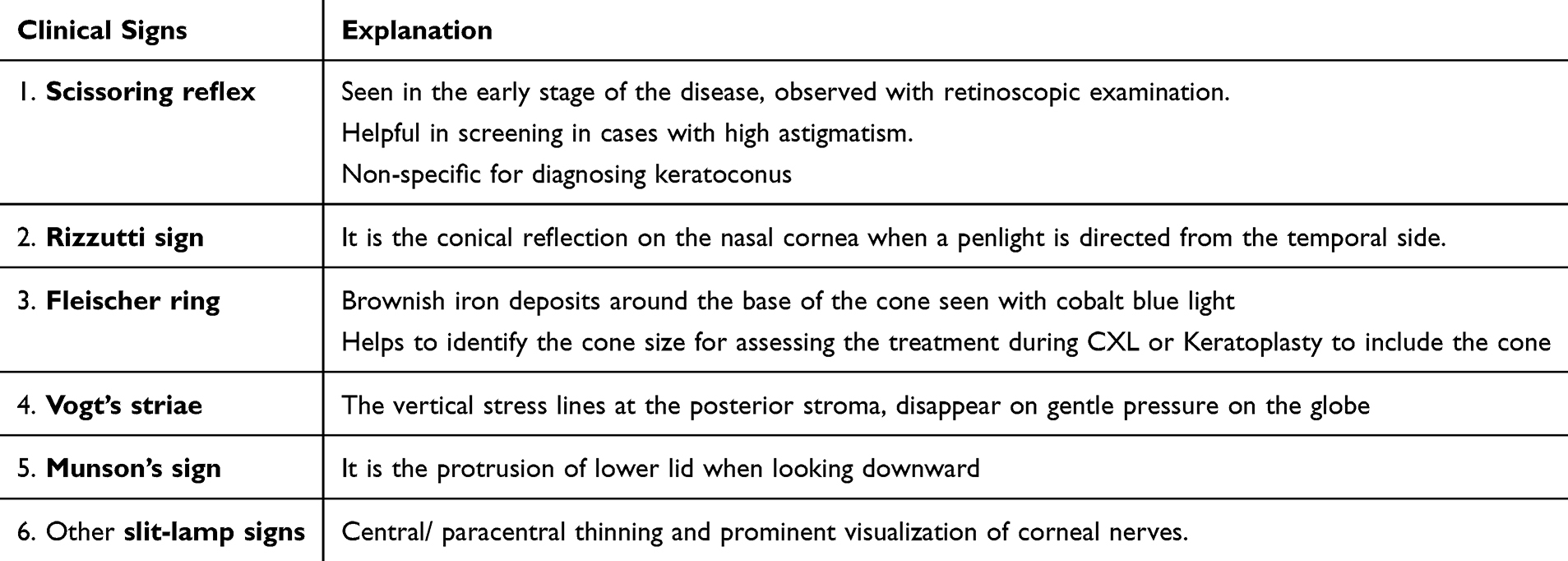 |
Table 5 The Description of Clinical Signs for KC |
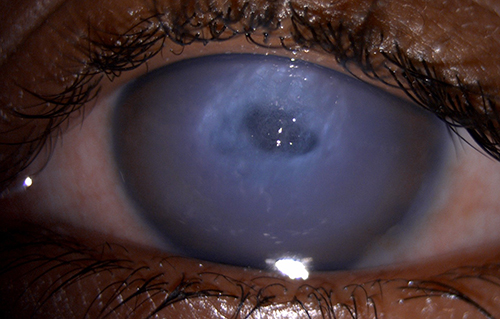 |
Figure 1 Shows the image with acute corneal hydrops in a patient with DS. |
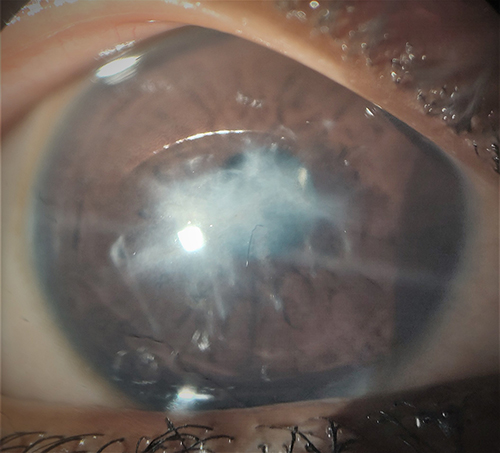 |
Figure 2 Shows the image with corneal scarring, sequelae of acute corneal hydrops. |
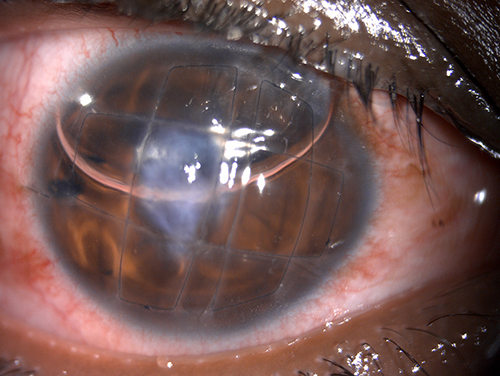 |
Figure 3 Shows the post-operative picture of compressive sutures with pneumodescemetopexy for hydrops intractable to medical treatment. |
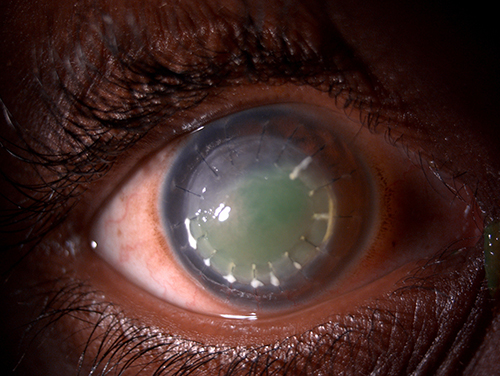 |
Figure 4 Shows the multiple loose sutures with debris, infiltrates with central epithelial defect and graft stromal rejection, in a patient with DS. |
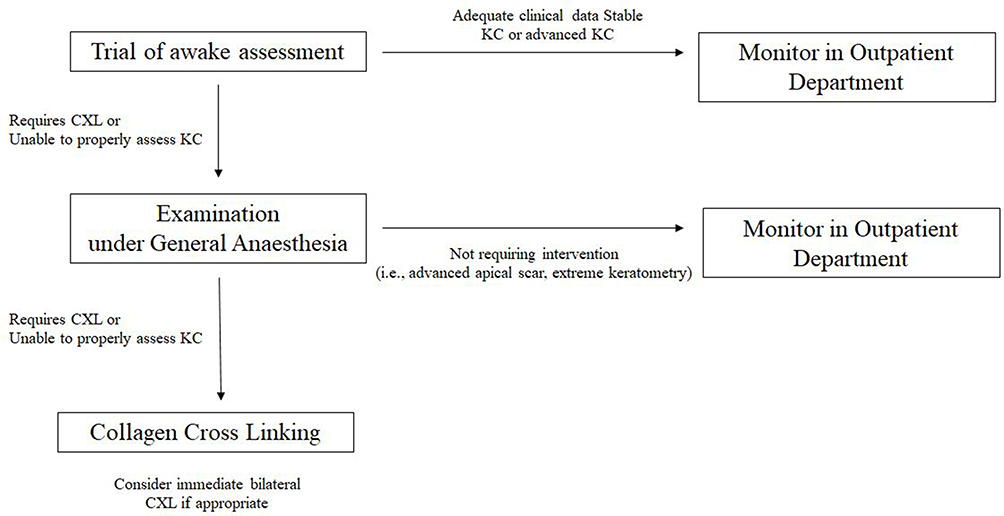 |
Figure 5 Shows the treatment algorithm for KC in DS with intellectual disability. |
 |
Figure 6 Shows the image of advanced Keratoconus in a patient with DS. |
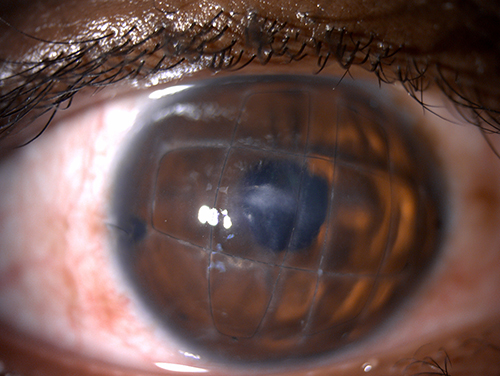 |
Figure 7 Shows the post healed hydrops scar managed with compression sutures. |
Diagnosis of Keratoconus in Down Syndrome
The diagnosis of keratoconus (KC) in Down syndrome (DS) requires the use of specialized corneal topography and tomography tools to detect early structural changes. Corneal topography maps the corneal surface curvature, while tomography, using devices like the Pentacam or CASIA2 anterior segment OCT, provides detailed three-dimensional imaging of both corneal surfaces and thickness, allowing for early detection. This is particularly important in DS, where KC prevalence ranges from 0% to 71% and progression is often more rapid. Despite often mild or absent early symptoms, timely diagnosis is critical to prevent visual impairment.13,29–31
Corneal Tomography Indices
Studies have identified several key indices for KC diagnosis. In a study by Asgari et al, 11 indices were identified as effective discriminators for diagnosing KC in a normal population. Among these, anterior higher-order aberrations (HOAs) (>0.643μm, AUROC = 0.879), posterior vertical coma (>0.0702μm, AUROC = 0.875), anterior vertical coma (>0.4124μm, AUROC = 0.868), and total HOA (>0.608μm, AUROC = 0.867) had the highest diagnostic accuracy. For non-DS individuals, key keratometry indices such as maximum keratometry (Kmax), K2, posterior radius of curvature, KISA, Belin/Ambrosio Enhanced Ectasia Display (BAD-D), Pentacam Random Forest Index, vertical asymmetry, and inferior-superior asymmetry (I-S value) are recommended for KC detection. In DS, the most effective parameters include minimum corneal thickness (≤480μm), corneal volume (≤55.3mm3), and BAD-D (>2.23). For the general population, indices like maximum keratometry (Kmax), posterior radius of curvature, and inferior-superior asymmetry (I-S value) are effective. Campbell et al noted that for DS patients, corneal astigmatism >1.6D, corneal power >50.0D, and a corneal resistance factor <8.7 were the most accurate indicators. Progressive KC cases are best monitored using zonal Kmax-3mm, with a 1.0D annual increase being a key sign of progression, followed by changes in I-S value and anterior elevation.2,5,13,29,32,33
Biomechanical Indices
Current biomechanical indices such as the Corvis Biomechanical Index (CBI) and Tomographic and Biomechanical Index (TBI) are also used for KC diagnosis. Standard cut- offs for the general population are CBI >0.583 and TBI >0.798. In DS patients with KC, CBI and TBI values have been observed at 0.54 and 0.86, respectively. Although eye-rubbing is considered a contributing factor, Hashemi et al found no strong correlation with KC severity. Aberrations and corneal thickness indices demonstrate higher diagnostic accuracy for KC in DS patients compared to keratometry indices. Zonal Kmax-3mm is preferred for tracking progression. Diagnosis criteria in DS should use higher cut-offs for tomography and biomechanical indices due to variability.13,16,34,35 Implementing these diagnostic measures, along with early intervention, helps mitigate KC progression, preserving vision and enhancing quality of life in DS patients. Table 6 shows the diagnostic indices for interpretation of KC in DS.
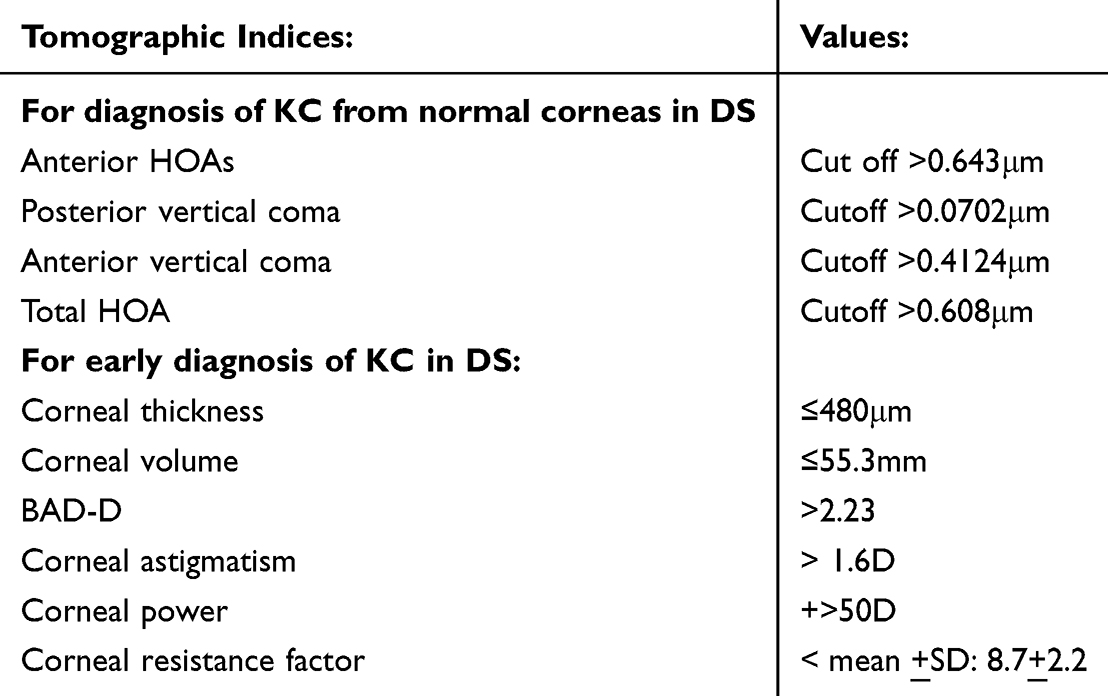 |
Table 6 Diagnostic Indices for Interpretation of KC in DS |
Management of KC in DS
Corneal Collagen Cross-Linkage
Managing KC in DS requires accurate diagnosis, which is challenging due to naturally steeper, thinner corneas and varying intellectual capabilities. Early diagnosis and corneal collagen cross-linking (CXL) are vital for halting KC progression and delaying keratoplasty.36 The epithelium-off Dresden protocol (SCXL) has shown long-term safety and efficacy in both adults and children, though prolonged anesthesia can be risky for DS patients. Preventing postoperative eye rubbing is critical in DS children.37–39 Figure 8: shows the flowchart on the management of Keratoconus in Downs Syndrome.
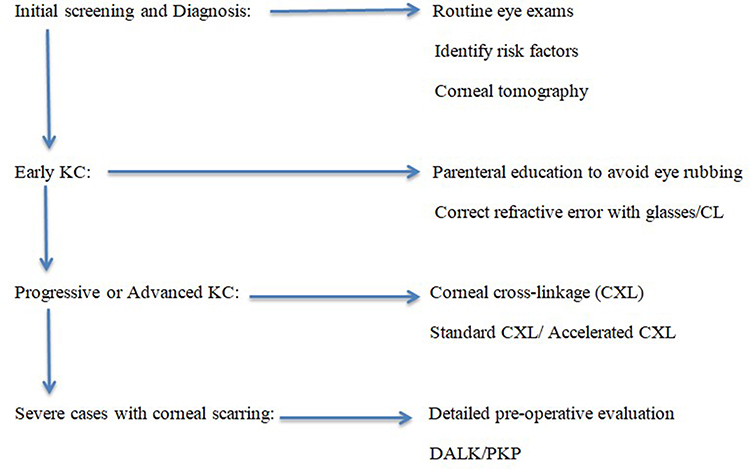 |
Figure 8 Shows the flowchart on the management of Keratoconus in Downs Syndrome. |
Accelerated CXL (ACXL) vs Standard Protocols
ACXL, which follows the Bunsen-Roscoe law, shortens treatment time while maintaining efficacy. Hashemi et al found that ACXL and SCXL both halted KC progression in DS patients, though ACXL resulted in less stiffness. SCXL performed under local anesthesia has also shown success. Corneal biomechanics change throughout life, with elasticity and viscosity increasing until age 12, followed by a period of instability from 12 to 15 years, and increased rigidity after 15 years, known as natural CXL. Children’s shorter collagen turnover (3 years vs 6 years in adults) requires frequent follow-ups and possible retreatments.17,40–42
Retreatment Efficacy and Concerns
Retreatment data are limited; Caprossi et al noted SCXL retreatment in 50% of cases where stabilization was not achieved post-T-CXL, which was less effective due to higher oxygen consumption by the epithelium. CXL is limited to corneas thicker than 400μm, and thin corneas may require hyposmolar riboflavin swelling, which is not always successful.43 A significant concern is the risk of spontaneous corneal melts in DS children, possibly due to thin corneas and keratocyte alterations leading to stromal remodelling.37–39,44,45
Treating KC in children with DS is challenging due to cooperation and anesthesia concerns, particularly with intellectual disabilities (ID) ranging from mild to severe. While mild ID may allow for awake assessments and CXL under local anesthesia, severe ID often requires general anesthesia (GA). Preoperative anesthesia assessments are essential due to the 12–60% prevalence of cardiac malformations in DS, although no cardiac complications with CXL have been reported. GA enables comprehensive, simultaneous bilateral CXL, improving resource use. Accelerated CXL protocols reduce GA time and risks, achieving an 89% success rate in corneal stabilization. Early CXL prevents visual loss, reduces the need for transplants, and enhances independence and life quality, supporting a proactive treatment approach in DS patients.8 Figure 9: shows the flow chart for treatment algorithm for KC in DS with Intellectual disability.
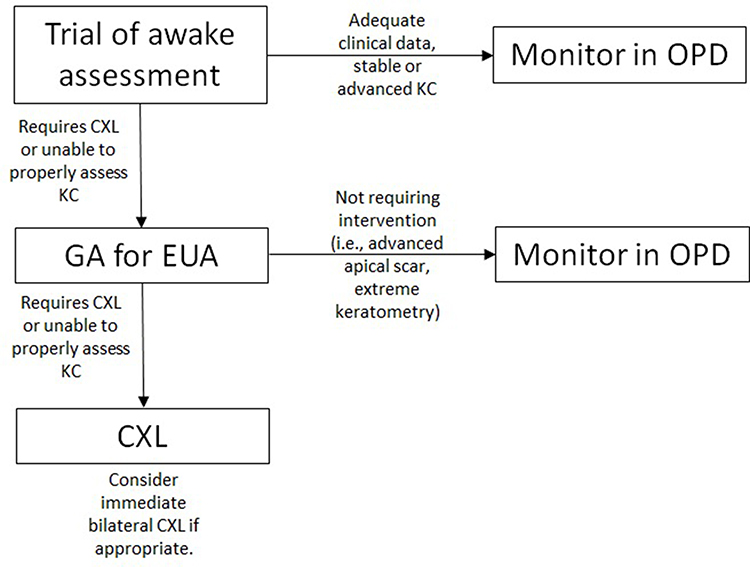 |
Figure 9 Flow chart shows the treatment algorithm for KC in DS with Intellectual disability. |
Keratoplasty and Their Concerns
Managing advanced keratoconus (KC) in children with Down syndrome (DS) often requires keratoplasty, despite its complexities and risks. Preventive measures and early intervention are crucial to reduce the need for surgery. Indications for surgery include advanced KC, scarring post-hydrops, and cooperative patients with mild disabilities supported by informed caregivers, no lid pathologies, and a commitment to follow-up and drug compliance. Emergency situations such as infectious keratitis, corneal melts, and perforations post-CXL may also necessitate surgery. Outcomes of keratoplasty in DS patients are generally poorer than in non-DS children due to anesthesia risks, infection from blepharitis and eye rubbing, lid anomalies, and higher rejection rates, particularly in large grafts. Long-term steroid use increases glaucoma risk, and DS patients are prone to trauma. Frantz JM et al reported repeated graft rejections in four out of five DS patients,46 while Volker Dieben HJ et al noted lower graft survival (67–85% in DS vs 90–95% in non-DS).39 Mc El Vanney AM documented bacterial infections, endothelial failure, and graft rejection in DS patients.47 Wroblewski et al performed keratoplasty on 18 eyes of 13 patients with an average age of 42 years, reporting that although all grafts were initially clear, three eyes required repeat grafts due to secondary graft failure, with the mean follow-up was 34.9 months.48 Similarly, Mc EL Vanney AM et al in 1997, performed keratoplasty in 5 patients (Age range between 19 and 21 years) with DS and in one patient with Dubowitz syndrome. Three grafts failed due to bacterial infection, endothelial failure followed by bullous keratopathy, and graft rejection, with only two grafts remaining clear for over two years. The high risk of graft infection remains a significant concern for graft failure, even with lamellar keratoplasty (DALK).47 DALK is preferred over PK (penetrating keratoplasty) due to fewer endothelial rejections and better structural integrity, though suture issues related to eye rubbing remain problematic. Figure 4 shows the post-operative image of DALK revealing multiple loose sutures with debris and central epithelial defect. Postoperative care is challenging due to difficulties in monitoring IOP and performing fundus exams, often requiring general anesthesia. Therefore, preventing KC progression through early diagnosis via screening and early CXL in both eyes is the most effective management strategy to maintain reasonable visual acuity in these children. Intraocular lens selection for people with cataracts requiring surgery may be more difficult in the DS population due to challenges with pre-operative assessment.8,39,49,50 ICRS (intrastromal corneal ring segments) offer a reversible option but carry risks of extrusion, refractive failure, keratitis, and corneal melting, limiting their use in DS.50 Effective management of KC in DS requires a balanced approach, prioritizing prevention, early diagnosis, CXL, and multidisciplinary care to maintain vision and reduce surgical interventions.
Screening Schedule for Keratoconus in Down Syndrome
The American Academy of Paediatrics Recommends a Structured Screening in Children with DS.51
- First 6 months: Screen for strabismus, cataracts, lacrimal duct obstruction, and nystagmus.
- Ages 1–5 years: Annual screenings for refractive errors and amblyopia.
- Ages 5–13 years: Screen every 2 years for KC and ocular allergies.
- Above 13 years: Screen every 3 years for cataracts, refractive errors, and KC.
Current Challenges in Diagnosis and Management and Future Concerns
Diagnosing and managing KC in DS patients is challenging due to cooperation and communication limitations. KC is often moderate to advance at presentation (Figure 6), complicating contact lens fitting and visual rehabilitation. Eye rubbing is a significant risk factor; educating parents and children to avoid it is crucial, especially due to the risk of acute hydrops.13 Advanced KC has a poorer prognosis, making early intervention essential. Corneal transplantation is reserved for patients with minimal intellectual disability and low eye-rubbing tendencies. Stephenson et al found 56.3% of KC cases in intellectually disabled patients, including DS, were advanced at presentation. Early CXL is essential, as it halts progression and avoids corneal transplantation.8 Suitability for CXL requires CCT >400 microns, highlighting the need for early diagnosis. Accurate assessments, including topography and biomechanics, are difficult due to patient cooperation, leading to diagnostic challenges.52 Hashemi et al noted that suspected KC cases showed stable diagnostic indices over seven years, reflecting naturally thinner, steeper DS corneas. CXL is preferred for patients under 14, performed under general anesthesia to ensure safety.41 A systemic evaluation to rule out cardiac and respiratory issues is needed. While the standard CXL protocol (3 mW/cm2, 30 minutes) yields better results, the accelerated protocol (9 mW/cm2, 10 minutes) is acceptable when anesthesia duration is a concern. Long-term studies, like Hashemi et al’s, show effective corneal flattening with the accelerated method, though follow-ups are needed to monitor potential retreatment. Postoperative care requires parental cooperation to prevent eye rubbing and ensure adherence to medications for optimal outcomes.53 Figure 8: shows the flowchart on the management of Keratoconus in Downs Syndrome.
Role of Paediatricians
With the remarkable improvement in life expectancy for individuals with DS over the past decade, the role of paediatricians has become even more vital. They not only confirm the diagnosis but also educate the parents through counselling and coordinating medical evaluations to detect congenital anomalies early. Hence, understanding of the syndrome, associated health conditions, and developmental challenges is essential to support these patients in achieving better health and social outcomes. A good vision is important for the development of a child especially in patients with DS with developmental and intellectual disabilities. Furthermore identification and registration of birth of DS needs long term follow-up of visual quality as well alongside routine systemic examinations for diagnosis of KC at the early stage, to address the quality of this longer life span.54
Future Approach
Further analysis of the genetic associations between DS and KC could significantly enhance early detection and management. New techniques for corneal imaging in DS patients with difficulty complying with mobile mounted- standard topography and telemedicine may improve the early detection of KC in DS patients. Modifications in protocols to include prophylactic treatments with CXL when diagnosed with KC and Parental education, on increased awareness about prevention eye rubbing can help avoid the progression of KC and facilitate appropriate visual rehabilitation, thereby maintaining the quality of life for these children. Table 7 enumerates the future perspective for research and preventive strategies.
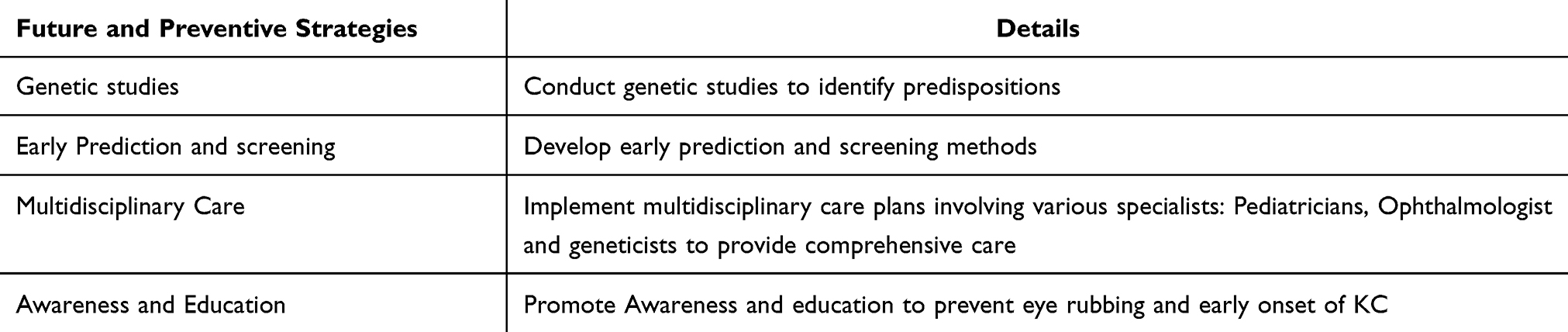 |
Table 7 Enumerates the Outline for Future Research and Preventive Strategies |
Conclusion
This review emphasizes the strong genetic link between DS and KC, with higher undiagnosed prevalence in DS. Studies consistently reveal a higher prevalence of KC in DS patients compared to the general population, with many cases going undiagnosed. This underscores the need for the heightened awareness among paediatricians about the importance of early ophthalmic screening. Timely detection and management of KC can prevent progression and subsequent blindness in these children, ultimately improving their quality of life. Early intervention and consistent follow-up are crucial in ensuing that children with DS receive the best possible care and support for their ocular health.
Abbreviations
KC, Keratoconus; DS, Down syndrome; SOD1, superoxide dismutase; VSX1, Visual system Homeobox 1 gene; DOCK 9, Dedictor of cytokine 9; LOX, Lysyl oxidase; ZEB1, Zinc finger E-box binding homeobox 1; TGFB1, Transforming growth factor beta 1; FLG, Filaggrin gene; RAB3GAP1, RAB3 (pathway) GTPase activating Protein; MPDZ, Multiple post synaptic density proteins; NFIB, Polymorphic Nuclear Factor 1B gene; BANP, B cell translocation associated nuclear protein gene; ZNF469, Zinc-Finger protein 469; PPCD, Posterior Polymorphous dystrophy; HGF, Hepatocyte growth factor; MMP, Matrix metallo proteinase; COL A, Collagen Alpha; ECM, Extracellular matrix; CH, Corneal biomechanics; POAG, Primary Open angle glaucoma; CCT, central corneal thickness; MDC, Mothers of DS children; MNC, Mothers of normal children; CXL, Corneal collagens cross linkage with riboflavin; T-CXL, Trans epithelial CXL; SCXL, Standard CXL; ACXL, Accelerated CXL; VKC, Vernal keratoconjunctivitis; GA, general anesthesia; DALK, Deep anterior lamellar keratoplasty; PK, Penetrating keratoplasty; CBI, Corvis biomechanical index; TBI, Tomographic biomechanical index; ICRS, Intracorneal ring segments; ID, Intellectual disability; D, Dioptre; HOA, Higher order aberrations; Z Kmax 3mm, average maximum keratometry value in the 3 mm zone; I-S value, difference between Inferior superior value in the axial curvature map; BAD-D, Belin Ambrosio display-total deviation; AUROC, Area under curve.
Acknowledgments
- Ramakrishnan Rangappa DO, MSAdvisor, Aravind Eye Hospital, Tirunelveli, Tamil Nadu, India
- Meenakshi Ravindran DO, DNBChief medical officer, Aravind Eye Hospital, Tirunelveli, Tamil Nadu, India
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by a grant from the NIH Fogarty International Center (D43AG069077).
Disclosure
Dr Olav Kristianslund reports personal fees from Santen, personal fees from Abbvie, grants from South-Eastern Norway Regional Health Authority, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Abdelaziz L, Barbara R. History of the development of the treatment of keratoconus. Int J Keratoconus Ectatic Corneal Dis. 2013;2:31–33.
2. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. doi:10.1016/S0039-6257(97)00119-7
3. Rajaraman R, Singh S, Raghavan A, Karkhanis A. Efficacy and safety of intracameral perfluoropropane (C3F8) tamponade and compression sutures for the management of acute corneal hydrops. Cornea. 2009;28(3):317–320. doi:10.1097/ICO.0b013e31818ada0b
4. Grzybowski A, McGhee CN. The early history of keratoconus prior to Nottingham’s landmark 1854 treatise on conical cornea: a review. Clin Exp Optom. 2013;96(2):140–145. doi:10.1111/cxo.12035
5. Lopes BT, Ramos IC, Salomão MQ, et al. Enhanced tomographic assessment to detect corneal ectasia based on artificial intelligence. Am J Ophthalmol. 2018;195:223–232. doi:10.1016/j.ajo.2018.08.005
6. Korbel JO, Tirosh-Wagner T, Urban AE. The genetic architecture of Down syndrome phenotypes revealed by high-resolution analysis of human segmental trisomies. Proc Natl Acad Sci U S A. 2009;106(29):12031–12036. doi:10.1073/pnas.0813248106
7. Akoto T, Li JJ, Estes AJ, et al. The underlying relationship between keratoconus and down syndrome. Int J Mol Sci. 2022;23(18):10796. doi:10.3390/ijms231810796
8. Stephenson KAJ, Power B, Malata D, et al. Management of keratoconus in down syndrome and other intellectual disability. Cornea. 2022;41(4):456–461. doi:10.1097/ICO.0000000000002793
9. Woodward MA, Blachley TS, Stein JD. The association between socio demographic factors, common systemic diseases, and keratoconus: an analysis of a nationwide heath care claims database. Ophthalmology. 2016;123(3):457.e452–65. doi:10.1016/j.ophtha.2015.10.035
10. Walsh SZ. Keratoconus and blindness in 469 institutionalised subjects with down syndrome and other causes of mental retardation. J Ment Defic Res. 1981;25:243–251. doi:10.1111/j.1365-2788.1981.tb00114.x
11. Chang HYP, Chodosh J. The genetics of keratoconus. Semin Ophthalmol. 2013;28(5–6):275–280. doi:10.3109/08820538.2013.825295
12. Kristianslund O, Hagem AM, Thorsrud A, et al. Prevalence and incidence of keratoconus in Norway: a nationwide register study. Acta Ophthalmol. 2021;99(5):e694–9. doi:10.1111/aos.14668
13. Hashemi H, Miraftab M, Amanzadeh K, et al. Keratoconus detection by novel indices in patients with down syndrome: a cohort population-based study. Jpn J Ophthalmol. 2020;64(3):285–291. doi:10.1007/s10384-020-00725-4
14. Edwards M, McGhee CN, Dean S. The genetics of keratoconus. Clin Exp Ophthalmol. 2001;29(6):345–351. doi:10.1046/j.1442-9071.2001.d01-16.x
15. Kim WJ, Rabinowitz YS, Meisler DM, et al. Keratocyte apoptosis associated with keratoconus. Exp Eye Res. 1999;69(5):475–481. doi:10.1006/exer.1999.0719
16. Alio JL, Vega-Estrada A, Sanz P, et al. Corneal morphologic characteristics in patients with down syndrome. JAMA Ophthalmol. 2018;136(9):971–978. doi:10.1001/jamaophthalmol.2018.2373
17. Elsheikh A, Wang D, Brown M, et al. Assessment of corneal biomechanical properties and their variation with age. Curr Eye Res. 2007;32(1):11–19. doi:10.1080/02713680601077145
18. Asgari S, Aghamirsalim M, Mehravaran S, et al. Effect of down syndrome and keratoconus on corneal density and volume: a triple comparative study. Sci Rep. 2020;10(1):9098. doi:10.1038/s41598-020-66108-4
19. Haugen OH, Høvding G, Eide GE. Biometric measurements of the eyes in teenagers and young adults with down syndrome. Acta Ophthalmol Scand. 2001;79(6):616–625. doi:10.1034/j.1600-0420.2001.790613.x
20. Bermudez BEBV, de Souza Do Amaral ME, da Silva Gomes C, et al. Ophthalmological abnormalities in down syndrome among Brazilian patients. Am J Med Genet A. 2020;182(11):2641–2645. doi:10.1002/ajmg.a.61845
21. Abu-Amero KK, Al-Muammar AM, Kondkar AA. Genetics of keratoconus: where do we stand? J Ophthalmol. 2014;2014:641708. doi:10.1155/2014/641708
22. McComish BJ, Sahebjada S, Bykhovskaya Y, et al. Association of genetic variation with keratoconus. JAMA Ophthalmol. 2020;138(2):174–181. doi:10.1001/jamaophthalmol.2019.5293
23. Bykhovskaya Y, Rabinowitz YS. Update on the genetics of keratoconus. Exp Eye Res. 2021;202:108398. doi:10.1016/j.exer.2020.108398
24. Kristianslund O, Drolsum L. Prevalence of keratoconus in persons with down syndrome in a national registry in Norway. JAMA Network Open. 2021;4(3):e210814. doi:10.1001/jamanetworkopen.2021.0814
25. Lu Y, Vitart V, Burdon KP, et al. Genome-wide association analyses identify multiple loci associated with central corneal thickness and keratoconus. Nat Genet. 2013;45(2):155–163. doi:10.1038/ng.2506
26. Kymionis GD, Plaka AD, Kontadakis GA. Clinical Signs and Differential Diagnosis of Keratoconus. In: Barbara A, editor. Textbook on Keratoconus New Insights.
27. Maharana PK, Sharma N, Vajpayee RB. Acute corneal hydrops in keratoconus. Indian J Ophthalmol. 2013;61(8):461–464. doi:10.4103/0301-4738.116062
28. Ozcan AA, Ersoz TR. Severe acute corneal hydrops in a patient with down syndrome and persistent eye rubbing. Ann Ophthalmol. 2007;39(2):158–160. doi:10.1007/s12009-007-0009-6
29. Song P, Yang K, Li P, et al. Assessment of corneal pachymetry distribution and morphologic changes in subclinical keratoconus with normal biomechanics. Biomed Res Int. 2019;2019:1748579. doi:10.1155/2019/1748579
30. Hashemi H, Asgari S, Panahi P, et al. Corneal ectasia in mothers of Down syndrome children. Sci Rep. 2021;11(1):22436. doi:10.1038/s41598-021-02035-2
31. Heidari Z, Mohammadpour M, Hashemi H, et al. Early diagnosis of subclinical keratoconus by wavefront parameters using scheimpflug, placido and Hartmann-Shack based devices. Int Ophthalmol. 2020;40(7):1659–1671. doi:10.1007/s10792-020-01334-3
32. Heidari Z, Hashemi H, Mohammadpour M, et al. Evaluation of corneal topographic, tomographic and biomechanical indices for detecting clinical and subclinical keratoconus: a comprehensive three-device study. Int J Ophthalmol. 2021;14(2):228–239. doi:10.18240/ijo.2021.02.08
33. Shetty R, Rao H, Khamar P, et al. Keratoconus screening indices and their diagnostic ability to distinguish normal from ectatic corneas. Am J Ophthalmol. 2017;181:140–148. doi:10.1016/j.ajo.2017.06.031
34. Herber R, Pillunat LE, Raiskup F. Development of a classification system based on corneal biomechanical properties using artificial intelligence predicting keratoconus severity. Eye Vis. 2021;8(1):21. doi:10.1186/s40662-021-00244-4
35. Eliasy A, Chen KJ, Vinciguerra R, et al. Determination of corneal biomechanical behavior in-vivo for healthy eyes using CorVis ST Tonometry: stress-strain index. Front Bioeng Biotechnol. 2019;7:105. doi:10.3389/fbioe.2019.00105
36. Haugen OH. Keratoconus in the mentally retarded. Acta Ophthalmol. 1992;70(1):111–114. doi:10.1111/j.1755-3768.1992.tb02101.x
37. Vinciguerra R, Romano MR, Camesasca FI, et al. Corneal cross-linking as a treatment for keratoconus: four-year morphologic and clinical outcomes with respect to patient age. Ophthalmology. 2013;120(5):908–916. doi:10.1016/j.ophtha.2012.10.023
38. Vinciguerra P, Albé E, Frueh BE, et al. Two-year corneal cross-linking results in patients younger than 18 years with documented progressive keratoconus. Am J Ophthalmol. 2012;154(3):520–526. doi:10.1016/j.ajo.2012.03.020
39. Völker-Dieben HJ, Odenthal MT, D’Amaro J, et al. Surgical treatment of corneal pathology in patients with Down’s syndrome. J Intellect Disabil Res. 1993;37(2):169–175. doi:10.1111/j.1365-2788.1993.tb00584.x
40. Mazzotta C, Traversi C, Baiocchi S, et al. Corneal collagen cross-linking with riboflavin and ultraviolet a light for pediatric keratoconus: ten-year results. Cornea. 2018;37(5):560–566. doi:10.1097/ICO.0000000000001505
41. Hashemi H, Amanzadeh K, Seyedian M, et al. Accelerated and standard corneal cross-linking protocols in patients with down syndrome: a non-inferiority contralateral randomized trial. Ophthalmol Ther. 2020;9(4):1011–1021. doi:10.1007/s40123-020-00303-4
42. Soeters N, Bennen E, Wisse RPL. Performing corneal crosslinking under local anesthesia in patients with down syndrome. Int Ophthalmol. 2018;38(3):917–922. doi:10.1007/s10792-017-0535-1
43. Caporossi A, Mazzotta C, Paradiso AL, et al. Transepithelial corneal collagen crosslinking for progressive keratoconus: 24-month clinical results. J Cataract Refract Surg. 2013;39(8):1157–1163. doi:10.1016/j.jcrs.2013.03.026
44. Faschinger C, Kleinert R, Wedrich A. Corneal melting in both eyes after simultaneous corneal cross-linking in a patient with keratoconus and down syndrome. Ophthalmologe. 2010;107(10):951–2,954–5. doi:10.1007/s00347-009-2127-6
45. Hafezi F, Mrochen M, Iseli HP, et al. Collagen crosslinking with ultraviolet-A and hypoosmolar riboflavin solution in thin corneas. J Cataract Refract Surg. 2009;35(4):621–624. doi:10.1016/j.jcrs.2008.10.060
46. Frantz JM, Insler MS, Hagenah M, et al. Penetrating keratoplasty for keratoconus in down’s syndrome. Am J Ophthalmol. 1990;109:143–147.
47. McElvanney AM, Adhikary HP. Penetrating keratoplasty in the mentally retarded. Eye. 1997;11(Pt 6):786–789.
48. Wroblewski KJ, Mader TH, Torres MF, et al. Long-term graft survival in patients with down syndrome after penetrating keratoplasty. Cornea. 2006;25(9):1026–1028. doi:10.1097/01.ico.0000226053.61884.91
49. Panda A, Aggarwal A, Madhavi P, et al. Management of acute corneal hydrops secondary to keratoconus with intracameral injection of sulfur hexafluoride (SF6). Cornea. 2007;26(9):1067–1069. doi:10.1097/ICO.0b013e31805444ba
50. Olivo-Payne A, Abdala-Figuerola A, Hernandez-Bogantes E, et al. Optimal management of pediatric keratoconus: challenges and solutions. Clin Ophthalmol. 2019;13:1183–1191. doi:10.2147/OPTH.S183347
51. Bull MJ, Trotter T, Santoro SL, et al. Health supervision for children and adolescents with down syndrome. Pediatrics. 2022;149(5):e2022057010. doi:10.1542/peds.2022-057010
52. Koppen C, Leysen I, Tassignon MJ. Riboflavin/UVA cross-linking for keratoconus in Down syndrome. J Refract Surg. 2010;26(9):623–624. doi:10.3928/1081597X-20100824-01
53. Hashemi H, Roberts CJ, Ambrósio R, et al. Comparative contralateral randomized clinical trial of standard (3 mW/cm2) versus accelerated (9 mW/cm2) CXL in patients with down syndrome: 3-year results. J Refract Surg. 2022;38(6):381–388. doi:10.3928/1081597X-20220329-01
54. Weijerman ME, de Winter JP. Clinical practice. The care of children with down syndrome. Eur J Pediatr. 2010;169(12):1445–1452. doi:10.1007/s00431-010-1253-0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.