Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
Uncontrolled hyperlipidemia in Chinese patients who experienced acute coronary syndrome: an observational study
Authors Jiang J ![]() , Zhou YJ, Li JJ, Ge JB, Feng YQ, Huo Y
, Zhou YJ, Li JJ, Ge JB, Feng YQ, Huo Y
Received 26 June 2018
Accepted for publication 16 October 2018
Published 16 November 2018 Volume 2018:14 Pages 2255—2264
DOI https://doi.org/10.2147/TCRM.S178318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor De Yun Wang
Jie Jiang,1 Yu-Jie Zhou,2 Jian-Jun Li,3 Jun-Bo Ge,4 Ying-Qing Feng,5 Yong Huo1
On behalf of ASAP Study Investigators
1Department of Cardiology, Peking University First Hospital, Xicheng District, Beijing 100034, China; 2Department of Cardiology, Beijing Anzhen Hospital, Chaoyang District, Beijing 100029, China; 3Department of Cardiology, Fuwai Hospital, Xicheng District, Beijing 100037, China; 4Department of Cardiology, Fudan University Zhongshan Hospital, Xuhui District, Shanghai 200032, China; 5Department of Cardiology, Guangdong General Hospital, Yuexiu District, Guangzhou, Guangdong Province 510080, China
Objective: Despite current standard of care, the overall lipid goal attainment rate for hyperlipidemia patients, especially those who have experienced acute coronary syndrome (ACS), is suboptimal, which predisposes them to a higher residual risk of atherothrombotic events. This study aimed to describe characteristics of Chinese patients who recently experienced an ACS event and were on lipid-lowering treatment, yet failing to reach targeted goal.
Methods: A multicenter, cross-sectional study was conducted to recruit 2,034 Chinese patients who experienced an ACS (ST segment elevation myocardial infarction [STEMI], non-STEMI, or unstable angina) event within the past 4–40 weeks and were on statin treatment (>2 weeks) from March 2015 to December 2016. All eligible patients underwent a fasting lipid test after enrollment and data on medical history were collected.
Results: The mean age of 1,994 eligible patients was 61.0±9.84 years. Among them, 1,493 (74.9%) patients received intensive statin therapy (defined as atorvastatin 40 or 80 mg, or rosuvastatin 20 mg per protocol) and 499 (25.0%) patients were on maximum tolerated dose statin. Of the 1,994 eligible subjects, 1,273 (63.8%) patients did not achieve the lipid goal at the time of enrollment. Among the not-at-goal patients, 910 (71.5%) received intensive statin therapy; the majority (73.4%) of them were male; the mean age was 61.2±10.1 years old; 699 (54.9%) patients had a history of hypertension; 25.3% had diabetes mellitus; and 29.5% were current smokers. The mean low-density lipoprotein-cholesterol (LDL-C), non-high-density lipoprotein-cholesterol (non-HDL-C), and ApoB levels at enrollment of this group of patients were 2.460±0.7139 mmol/L, 3.094±0.8861 mmol/L, and 0.840±0.3015 g/L, respectively.
Conclusion: The study result demonstrates that overall more than half of the patients who recently (4–40 weeks) experienced ACS who were treated did not reach the guideline-recommended LDL-C and non-HDL-C goal. These results highlight the potential necessity for a new drug beyond statins to further reduce disease burden in the future.
Keywords: acute coronary syndrome, intensive statin treatment, lipid goal attainment, lipid-lowering treatment
Introduction
Patients who have experienced recent acute coronary syndrome (ACS) events are at very high risk of recurrent coronary events in the near term. The recently updated American College of Cardiology/American Heart Association guidelines include several major changes in favor of an emphasis on the high intensity of statin treatment, regardless of low-density lipoprotein-cholesterol (LDL-C) levels.1 The 2013 Chinese expert consensus also emphasized that regardless of the baseline cholesterol levels, all patients with ACS events should immediately initiate and maintain intensive statin therapy long-term after discharge.2,3 Based on the results of large-scale clinical trials, early intensive statin therapy has been recommended for patients with recent ACS events. Both epidemiological and interventional clinical trials have shown a strong association between elevated LDL-C level and cardiovascular events.4,5
A large observational study (DYSIS-China) showed that although the majority (88.9%) of dyslipidemia patients in China were treated with statins, the overall attainment of LDL-C target was 61.5% and that for very high-risk ACS patients was 54.8%,6 and the overall attainment of high-density lipoprotein-cholesterol (HDL-C) goal was 68.1% and that for triglycerides (TG) was 58.2%. However, even in patients with normal LDL-C levels, a high residual risk of atherothrombotic events remains.5,7 In the DYSIS-China study, 14.2% of patients at LDL-C goal had decreased HDL-C and/or elevated TG levels. Meanwhile, despite stable lipid-lowering therapy, high cardiovascular (CV) risk patients still had one or more manifestations of dyslipidemia and only approximately 10% of patients received a high dose of statins.7 The overall lipid goal (defined by 2016 Chinese guideline for the management of dyslipidemia in adults:8 LDL <1.8 mmol/L for very high-risk patients, LDL-C <2.6 mmol/L for high-risk patients, LDL-C <3.4 mmol/L for low-moderate risk patients) attainment rate for hyperlipidemia patients, especially those who have experienced ACS who have been treated under standard of care is suboptimal, which predisposes them to a high residual risk of atherothrombotic events. Thus, alternative treatment beyond statins for LDL-C reduction may be necessary in order to achieve target levels not only for LDL-C but also for non-HDL-C.
Therefore, it is important to better understand current, real-world practice in China when it comes to lipid management in high-risk patients such as those who have recently (4–40 weeks) experienced ACS but are not reaching the therapeutic goal. This information will provide an up-to-date view of the unmet needs for the care of post-ACS patients in China.
Methods
Objectives
The primary objective of the study was to describe patient characteristics and use of intensive statin treatment in Chinese patients who recently experienced an ACS event and were on active lipid treatment but not at the therapeutic goal. The secondary objective was to identify medical reasons why patients could not adopt intensive statin treatment when the therapeutic goal had not been achieved.
Not achieving the therapeutic goal was defined as LDL-C ≥1.81 mmol/L (70 mg/dL), or ApoB ≥0.8 g/L, or non-HDL-C ≥2.59 mmol/L (100 mg/dL).
Study design and participants
This study was a multicenter cross-sectional study conducted in 52 tertiary hospitals in China. Patients who had experienced an ACS event within the previous 4–40 weeks were enrolled if they had received active lipid-lowering treatment with a stable (>2 weeks) regimen. Patients needed to be at least 40 years old and had to provide written informed consent to be included.
The ACS event included hospitalization for ST segment elevation myocardial infarction (STEMI), non-STEMI (NSTEMI), or high-risk unstable angina (UA). Patients should have had ischemic symptoms with an unstable pattern occurring at rest or minimal exertion within 72 hours of an unscheduled hospital admission due to presumed or proven obstructive coronary disease and at least one of the following: elevated cardiac biomarkers, resting electrocardiogram changes consistent with ischemia, or infarction together with additional evidence of obstructive coronary disease.
Active lipid-lowering regimen was limited to statin-intensive (defined as atorvastatin 40 or 80 mg per day or rosuvastatin 20 mg per day) therapy, maximum tolerated dose of statins or other non-statin lipid-lowering therapy if patients had documented intolerance to at least two statins, at physician’s discretion.
To be enrolled, patients’ lipid level must not have been tested regardless of level of lipid parameters or tested but not at goal after stable active lipid-lowering treatment, which is defined as LDL-C ≥1.81 mmol/L (70 mg/dL), or ApoB ≥0.8 g/L, or non-HDL-C ≥2.59 mmol/L (100 mg/dL), Figure 1.
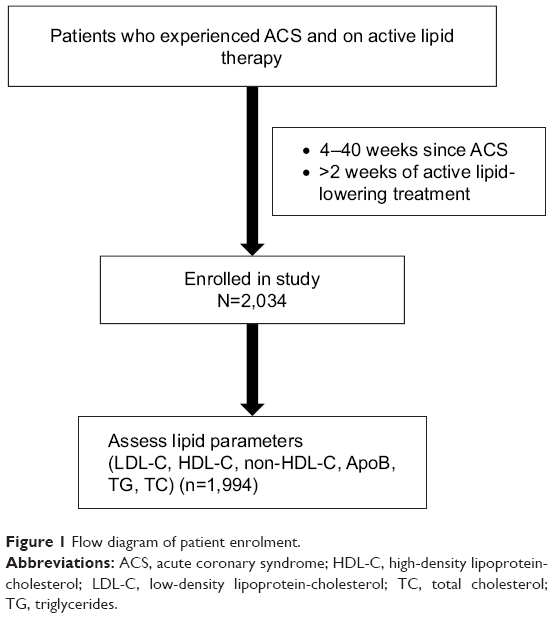 | Figure 1 Flow diagram of patient enrolment. |
Exclusion criteria included inability or unwillingness to provide informed consent, cognitive or language barriers to comprehension, participation in any clinical trial at the time of enrollment, and life expectancy <1 year.
Study process
A site feasibility questionnaire was used to evaluate study feasibility at site level. The study protocol was approved by the ethics committee at each participating center according to the Declaration of Helsinki (Table S1). All patients gave written informed consent to participate in this study. Each site was given approximately 6 months to enroll their allocation of patients. Each selected site had to include consecutive subjects who met the inclusion criteria.
Lipid profile including total cholesterol, LDL-C, HDL-C, ApoB, and TG was compiled for every eligible participant after enrollment. The medical records for the index ACS event during hospitalization were reviewed to collect all the baseline clinical information, including demographics, medical history, physical examination, ACS classification, and in-hospital reperfusion therapies, which included percutaneous coronary intervention with or without stent, coronary artery bypass surgery, or thrombolytic therapy. Blood lipid profile after the index ACS event during hospitalization was also collected. Lipid-lowering pharmacotherapy after the index ACS event was recorded during the visit. Patients were divided into intensive statin therapy (defined as atorvastatin 40 or 80 mg per day or rosuvastatin 20 mg per day per protocol) and maximum tolerated dose statin therapy and non-statin therapy (if patients had documented intolerance to at least two statins at physician’s discretion) groups. Reasons for not using intensive statin in patients on maximum tolerated dose statin therapy or other non-statin therapy were also collected during this visit.
Data collection
Data were collected through use of paper Case Report Forms. The computerized handling of the data generated additional requests to which the participating investigator was obliged to respond by confirming or modifying the data questioned.
Sample size and statistical analysis
The primary objective of this study was to identify patient characteristics and the use of lipid-lowering therapy in patients with recent ACS events (4–40 weeks) who received standard lipid-lowering therapy but did not achieve the therapeutic goal. The sample size was determined based on a non-probabilistic sampling approach to obtain sufficient exposure data from patients in various risk groups.
The analysis was mainly descriptive. For continuous variables, number of non-missing subjects, mean, SD, median, interquartile range, and maximum and minimum values were used to describe the variables. For categorical variables, number of patients and proportions were adopted, and “0” was displayed when the count was zero. The proportions were all based on the non-missing data, except when there were additional instructions.
Results
A total of 2,034 subjects from 52 sites were enrolled in this registry study from March 2015 to December 2016. Three subjects were not assigned to any treatment group. Of the 2,031 subjects, 1,994 who met the main inclusion/exclusion criteria were included in the eligible population.
Patient characteristics, cardiovascular risk profile, and in-hospital therapy for all eligible patients are summarized in Table 1. The mean age of the eligible population was 61.0±9.84 years. Among them, 1,505 (75.5%) were male and 489 (24.5%) were female. Overall, 1,133 (56.8%) patients had a history of hypertension and 515 (25.8%) patients had a history of diabetes mellitus. The number of patients who were currently smoking and physically inactive was 588 (29.5%) and 172 (8.6%), respectively. As for the index ACS event, a total of 1,068 (53.6%) patients had experienced STEMI, 454 (22.8%) had NSTEMI, and 461 (23.1%) had high-risk UA. Also, 1,752 (87.9%) underwent percutaneous coronary intervention with or without stent during the index ACS hospitalization (Table 1).
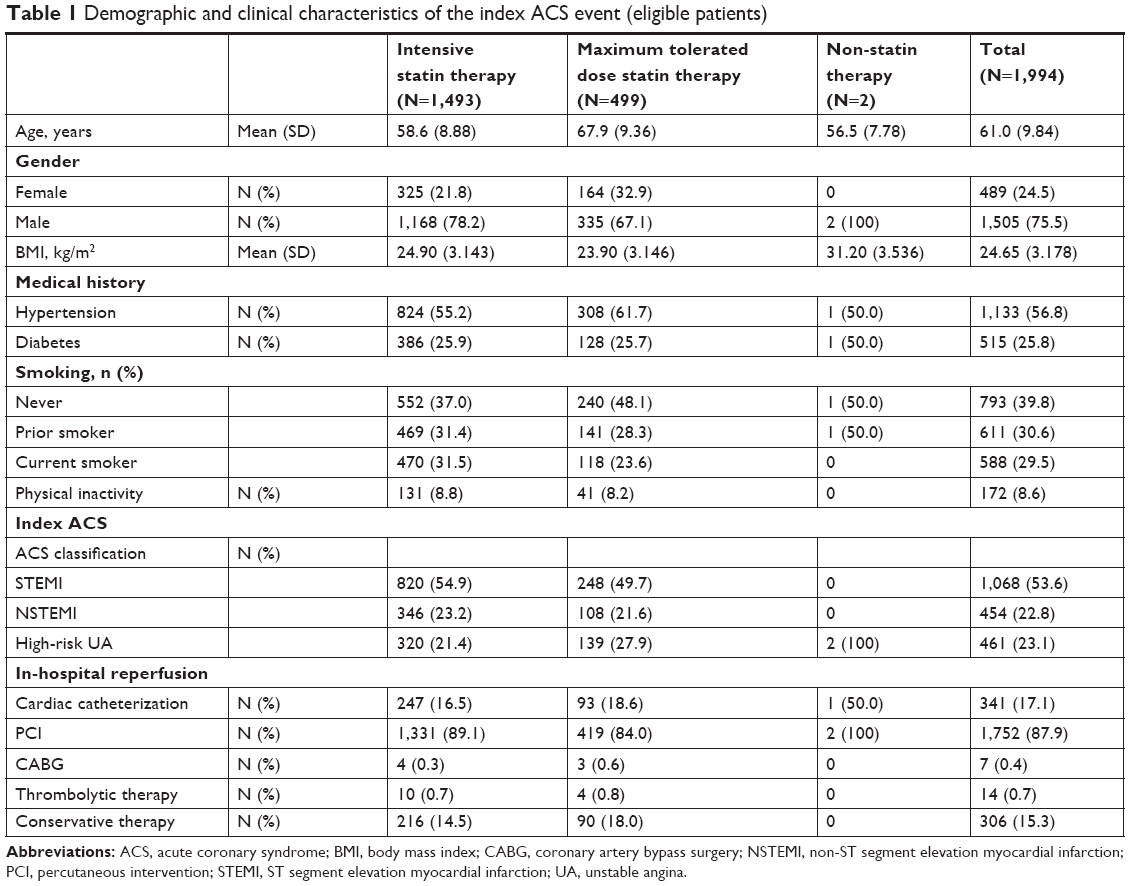 | Table 1 Demographic and clinical characteristics of the index ACS event (eligible patients) |
A total of 1,493 patients were treated with intensive statin therapy, 499 were treated with maximum tolerated dose statin, and two were on non-statin therapy. Numerically, patients who were on intensive statin therapy before enrollment were younger, the majority were male, and had STEMI as the index ACS event.
Lipid profiles during the index ACS hospitalization and at time of enrollment are shown in Figure 2A and B. Lipid profile improved from the index hospitalization to enrollment with numerically decreased LDL-C, non-HDL-C, and ApoB, irrespective of the lipid-lowering treatment pattern.
 | Figure 2 Sequential graph representing the lipid profiles of study population on different lipid-lowering therapies. |
Of the 1,994 eligible subjects, 1,273 (63.8%) patients did not achieve the lipid goal at the time of enrollment. Among them, 71.5% adopted intensive statin therapy. The most frequently used lipid-lowering agents were atorvastatin and rosuvastatin. The mean doses of atorvastatin and rosuvastatin in this group of patients at enrollment were 35.3±8.94 mg and 18.8±3.80 mg, respectively.
Of the 1,273 subjects who were not-at-goal, the majority (73.4%) were male, mean age was 61.2±10.1 years, 54.9% of patients had hypertension, 25.3% had diabetes mellitus, and 40.8% were non-smokers (Table 2). Lipid profiles during the index ACS hospitalization and at time of enrollment are shown in Figure 3A and B. The mean LDL-C, non-HDL-C, and ApoB level of this group of patients after enrollment were 2.460±0.7139 mmol/L (94.5±27.56 mg/dL), 3.094±0.8861 mmol/L (119.45±34.21 mg/dL), and 0.840±0.3015 g/L, respectively (Figure 3B).
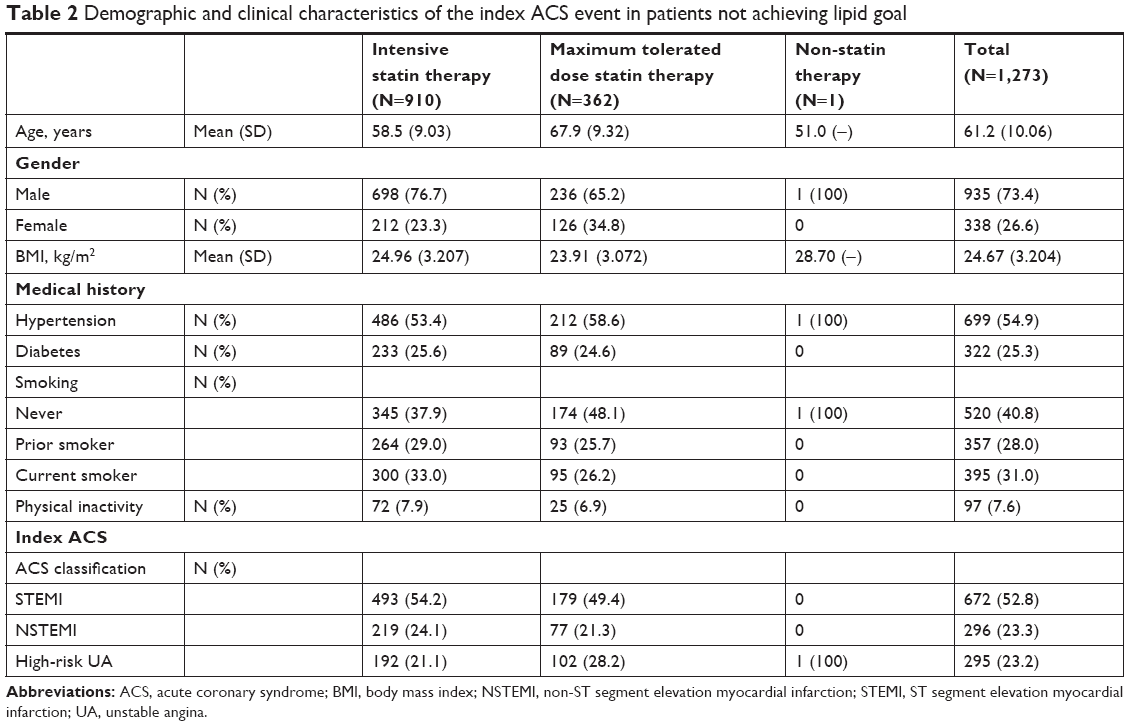 | Table 2 Demographic and clinical characteristics of the index ACS event in patients not achieving lipid goal |
 | Figure 3 Sequential graph representing the lipid profiles of patients not achieving target lipid levels on different statin therapies. |
Among patients with maximum tolerated dose statin or non-statin therapy, 362 patients provided the reason for not adopting intensive statin treatment. Of them, 75 (20.7%) patients claimed elevated liver enzyme, eleven (3.0%) claimed myopathy, and 282 (77.9%) claimed other reasons (ie, advanced age and lower body mass index [BMI]).
Discussion
This study demonstrated that the proportion of post-ACS patients who had been treated but were not reaching the lipid goal was still high. Among those patients who were not-at-goal, 71.5% adopted intensive statin therapy and 28.5% were administered the maximum tolerated dose of statins or non-statin therapy. Furthermore, the risk of developing major CV events is increasingly higher for those patients not-at-goal. Therefore, there is still room for improvement in terms of lipid goal attainment for post-ACS patients.
In this study, the overall rate of lipid goal attainment was only 35.5%. The reasons could be as follows: first, approximately 25% of patients did not adopt intensive statins for various reasons, which may have led to lower lipid goal attainment rate in those patients; second, the duration of intensive statin treatment was at least 2 weeks prior to enrollment, and a proportion of patients’ statin plasma concentrations might not have reached the therapeutic level which may have led to the underestimated treatment effect for those patients. In addition, the LDL-C value was the only criterion to assess goal attainment in previous studies,7,9,10 while this study also assessed non-HDL-C and ApoB level. As non-HDL-C is a strong independent risk factor, and ApoB should be considered as an alternative risk marker whenever available, especially in subjects with high TG, the “not-at-goal” in this study was defined as not only LDL-C level but also non-HDL-C or ApoB level higher than normal. In this regard, the proportion of not-at-goal was increased, which may indicate that some patients were “missed” in clinical practice because assessing the lipid-lowering treatment effect was based purely on the LDL-C level.
In the DYSIS II ACS cohort,11 although 94.6% of patients still used statins 4 months after discharge, the statin dosage decreased from 37 mg during the hospital stay to 32±21 mg/day by the follow-up visit. Despite this comparatively high dose of statin, attainment of the LDL-C target <1.8 mmol/L (70 mg/dL) only increased from 19.0% to 37.0%. Among the patients who were at-goal, 71.7% adopted intensive statin therapy, and the treatment dosage was slightly higher than that for the cohort in the DYSIS II ACS study, but the lipid goal attainment rate was similar to that observed in the DYSIS II ACS study.11
On the contrary, although intensive statin therapy was recommended in the inclusion criteria and all investigators were encouraged to follow study protocol, 25% of patients were not administered intensive statin therapy. When we investigated the reason why these patients could not use intensive statins, it was found that many of these patients did not have a definite adverse event related to the statins. Thus, clinical inertia might play an important role in choosing a treatment strategy. The other factors that will mainly impact adherence include reported adverse events related to statins, advanced age, and lower BMI of patients. In addition, those patients with multiple medical conditions often require the use of multidrug therapy, which may result in increased risk of adverse effects, drug–drug interactions, and medication non-adherence as well as increased costs for both patients and payers. Last but not least, cost of the drug is a barrier to adopting intensive statins in the long run. Hence, in these patients who cannot adopt intensive statin therapy, other lipid-lowering treatment options other than statins are needed to reach the target. Previous studies reported adverse events such as myopathy and muscle and liver toxicity during intensive statin therapy, which has led to further discontinuation of statins.12,13 Furthermore, the adoption rate of ezetimibe alone or combined with statins was very low in this study as ezetimibe was not reimbursed at the time of study. This study provides an up-to-date view of characteristics and lipid profiles of those ACS patients treated but not-at-goal in China. These findings are supported by the DYSIS-China study. However, it still has several limitations that should be addressed. First, it was an observational cross-sectional study that did not assess long-term outcomes. Hence, a long-term longitudinal study is required to establish the temporality of LDL-C lowering and CV outcomes and mortality in ACS patients in China in the future. Second, lipid parameters were not measured in a central laboratory. Finally, given that receiving active lipid-lowering treatment (>2 weeks) was a patient eligibility criterion, we may have overestimated the proportion of intensive/maximum tolerated dose statin usage.
Conclusion
The lipid goal attainment rate of post-ACS (4–40 weeks) patients was still suboptimal. Among patients who were not-at-goal, a proportion of patients did not take intensive statins. The risk of recurrent CV events is increased for those patients not-at-goal. The reasons for not taking intensive statins were mainly advanced age and low BMI. Therefore, intensive lipid-lowering treatment should be reinforced and other treatment options other than statins are needed for those patients who are not reaching the lipid goal, but cannot adopt intensive statin therapy.
Acknowledgments
Sanofi was the sponsor of the study, and was responsible for the design of the study, collecting and managing data, and performing all statistical analyses. The authors are grateful to all the investigators and patients who participated in this study. Medical writing support under authors’ direction was provided by Dhanya Mukundan, MDS and Priyanka Bannikoppa, PhD (Indegene, Bangalore) as funded by Sanofi, China.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Wang WT, Hellkamp A, Doll JA, et al. Lipid testing and statin dosing after acute myocardial infarction. J Am Heart Assoc. 2018;7(3):e006460. | ||
Eisen A, Cannon CP, Braunwald E, et al. Predictors of nonuse of a high-potency statin after an acute coronary syndrome: insights from the stabilization of plaques using darapladib-thrombolysis in myocardial infarction 52 (SOLID-TIMI 52) trial. J Am Heart Assoc. 2017;6(1):e004332. | ||
Schiele F, Farnier M, Krempf M, Bruckert E, Ferrières J; French Group. A consensus statement on lipid management after acute coronary syndrome. Eur Heart J Acute Cardiovasc Care. 2018;7(6):532–543. | ||
Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the european atherosclerosis society consensus panel. Eur Heart J. 2017;38(32):2459–2472. | ||
Sampson UK, Fazio S, Linton MF. Residual cardiovascular risk despite optimal LDL cholesterol reduction with statins: the evidence, etiology, and therapeutic challenges. Curr Atheroscler Rep. 2012;14(1):1–10. | ||
Zhang W, Ji F, Yu X, Wang X. Factors associated with unattained LDL-cholesterol goals in Chinese patients with acute coronary syndrome one year after percutaneous coronary intervention. Medicine (Baltimore). 2017;96(1):e5469. | ||
Zhao S, Wang Y, Mu Y, et al; DYSIS-China Study Investigators. Prevalence of dyslipidaemia in patients treated with lipid-lowering agents in China: results of the DYSlipidemia International Study (DYSIS). Atherosclerosis. 2014;235(2):463–469. | ||
Joint committee issued Chinese guideline for the management of dyslipidemia in adults. 2016 Chinese guideline for the management of dyslipidemia in adults. Zhonghua Xin Xue Guan Bing Za Zhi. 2016;44(10):833–853. | ||
Zheng W, Zhang Y-J, Bu X-T, et al. LDL-cholesterol goal attainment under persistent lipid-lowering therapy in northeast China. Medicine (Baltimore). 2017;96(46):e8555. | ||
Perez de Isla L, Alonso R, Watts GF, et al; SAFEHEART Investigators. Attainment of LDL-Cholesterol treatment goals in patients with familial hypercholesterolemia: 5-Year SAFEHEART registry follow-Up. J Am Coll Cardiol. 2016;67(11):1278–1285. | ||
Gitt AK, Lautsch D, Ferrières J, et al. Cholesterol target value attainment and lipid-lowering therapy in patients with stable or acute coronary heart disease: Results from the Dyslipidemia International Study II. Atherosclerosis. 2017;266:158–166. | ||
Jose J. Statins and its hepatic effects: Newer data, implications, and changing recommendations. J Pharm Bioallied Sci. 2016;8(1):23–28. | ||
Arca M, Pigna G. Treating statin-intolerant patients. Diabetes Metab Syndr Obes. 2011;4:155–166. |
Supplementary material
 | Table S1 Ethics committees which provided approval |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.