Back to Journals » International Medical Case Reports Journal » Volume 17
Uncommon Coexistence of Eosinophilic Colitis, Asthma, and Elevated IgG4 Levels: A Case Report
Authors Nguyen QH ![]() , Pham TQN, Lam HT
, Pham TQN, Lam HT ![]() , Huynh TM
, Huynh TM ![]() , Vu NTH, Vo TTL, Vo TD
, Vu NTH, Vo TTL, Vo TD ![]()
Received 10 June 2024
Accepted for publication 29 October 2024
Published 7 November 2024 Volume 2024:17 Pages 939—943
DOI https://doi.org/10.2147/IMCRJ.S482180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Qui Huu Nguyen,1,* Tram Que Nguyen Pham,1,* Huong Tu Lam,1 Tien Manh Huynh,1 Nhu Thi Hanh Vu,1 Tran Thi Luong Vo,1 Thong Duy Vo1,2
1Department of Internal Medicine, Faculty of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 2Department of Gastroenterology, University Medical Center Ho Chi Minh City, Ho Chi Minh City, Vietnam
*These authors contributed equally to this work
Correspondence: Thong Duy Vo, Department of Internal Medicine, Faculty of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, University Medical Center Ho Chi Minh City, 217 Hong Bang, Ward 11, Dis. 5, Ho Chi Minh City, 71724, Vietnam, Tel +84 932039888, Email [email protected]; [email protected]
Purpose: Eosinophilic gastrointestinal diseases represent a rare and diverse group of conditions. Given that the pathogenesis of EoC is not well understood and is often linked to allergic conditions, this case underscores the necessity for further research into such unique presentations. The patient’s prolonged gastrointestinal symptoms presented a significant diagnostic challenge, emphasizing the importance of ruling out various potential causes for elevated blood eosinophils. This exploration aims to enhance the understanding of such rare clinical scenarios and improve diagnostic accuracy in similar cases.
Case Description: We present a unique case of a 57-year-old patient with a medical history of asthma and allergic rhinitis who presented recurrent abdominal pain, significant blood eosinophilia, and elevated levels of Immunoglobulin G4. After ruling out hematological and secondary causes of eosinophilia, a biopsy of the colon mucosa revealed an excess of tissue eosinophils, confirming the diagnosis of EoC. The patient responded well to corticosteroids and was subsequently maintained on montelukast, with no recurrence of symptoms over 3 months.
Conclusion: This rare confluence of EoC, asthma, and high levels of serum IgG4 in a single patient contributes to our understanding of these complex and interconnected disorders.
Keywords: Eosinophilic colitis, IgG4, Asthma
Introduction
Eosinophilic colitis (EoC) is the least common eosinophilic gastrointestinal disease (EGID), characterized by eosinophil infiltration in the colon.1 Its pathogenesis remains largely unknown and is often associated with allergic conditions.1 In this case, the presence of EoC, asthma and high IgG4 is a rare combination that requires further exploration. The patient’s prolonged gastrointestinal symptoms posed a diagnostic challenge due to the need to rule out various causes of elevated blood eosinophils.
Case Report
A 57-year-old woman with a 14-year history of asthma and allergic rhinitis, on salmeterol/fluticasone, was hospitalized for recurrent abdominal pain that began two months earlier. The pain was intermittent and dull, accompanied by nausea, anorexia, malaise, and a weight loss of 5 kg. There was no fever, blood / mucus in the stool, or respiratory symptoms (rhinorrhea, wheezing, coughing). She had no history of alcohol/tobacco use or traditional herbal medicines. Six weeks before admission, she was diagnosed with an intestinal infection in a local clinic after a complete blood count (CBC) revealed leukocytosis and significant eosinophilia (25.61 G/L, 77.8% eosinophils). She received antibiotics and mebendazole without relief of symptoms. At presentation, the patient was alerted and oriented with stable vitals (BP 110/70 mmHg, T 37°C, HR 88 bpm, RR 18 bpm). She had a BMI of 16.6 kg/m² and sarcopenia, but no skin rash, lymphadenopathy, or edema. The abdominal exam showed tenderness in the epigastric and umbilical regions without guarding. CBC revealed leukocytosis and significant eosinophilia (20.8 G/L, with a total white blood cell count of 26.8 G/L, comprising 77.8% eosinophils). Peripheral blood film examination showed normal eosinophils. Bone marrow aspiration reveals 48% eosinophils without blasts, atypical cells. Fluorescence in situ hybridization (FISH) for CHIC2 deletion as a surrogate marker for FIP1L1-PDGFRA showed no rearrangements of the PDGFRA gene. Autoimmune and vasculitis screenings (ANA, anti-dsDNA, p-ANCA, c-ANCA) were negative. Elevated serum IgG (2760 mg/dL; normal range, 700–1600 mg/dL) and IgG4 (1260 mg/dL; normal range, 3.9–86.4 mg/dL), slightly elevated IgE (137.5 IU/mL; normal range, <100 IU/mL) and high RF (144.4 IU/mL; normal range, <20 IU/mL) were observed. Other parameters were normal, including aminotransferase, blood urea nitrogen, serum creatinine, complement C3, complement C4, vitamin B12, serum cortisol, and NT-proBNP. ECG and echocardiogram were normal. Chest CT scans showed mild fibrosis and bronchiectasis (Figure 1). Sputum AFB smears and bronchoscopy were negative. The cytology of the bronchoalveolar lavage fluid showed 35% neutrophils, no eosinophils. Spirometry indicated severe obstruction with bronchodilator response. The fractional exhaled nitric oxide (FeNO) level was 15 ppb. Stool samples were tested positive for leukocytes, with no signs of ova or parasites. Serology tests were positive for toxocariasis (positive IgG of Toxocara canis at 54.2 NovaTec-Units) but negative for Strongyloides stercoralis, Fasciola sp., Toxoplasma gondii, Trichinella spiralis, Ancylostoma sp., Angiostrongylus cantonensis, Ascaris lumbricoides, Clonorchis sinensis, Paragonimus sp., Gnathostoma sp., Entamoeba histolytica, cysticercosis, filariasis, and HIV. An abdominal contrast-enhanced computed tomography scan revealed gallbladder stones without acute cholecystitis and showed no gastrointestinal tract abnormalities. The upper gastrointestinal endoscopy showed unremarkable results with a normal appearance. Colonoscopy showed mucosal inflammation in the sigmoid, left, transverse, and right colon with systemic biopsy (Figure 2). A five-day course of albendazole (400 mg twice daily) for suspected toxocariasis was ineffective. Colonic biopsies revealed significant eosinophilic infiltration (>85 eosinophils/High-power field (HPF) in the left colon, >100 eosinophils/HPF in the transverse and right colon) (Figure 3). Given the patient’s nonresponse to toxocariasis treatment and the significant eosinophilic infiltration observed in the colon mucosa biopsy, a diagnosis of eosinophilic colitis was confirmed. The patient was treated with oral methylprednisolone (16 mg) and montelukast (5 mg). Symptoms resolved in two weeks and eosinophil counts normalized (0.3 G/L). The corticosteroid was reduced and discontinued, and the patient was maintained on montelukast for three months without symptom recurrence (Table 1).
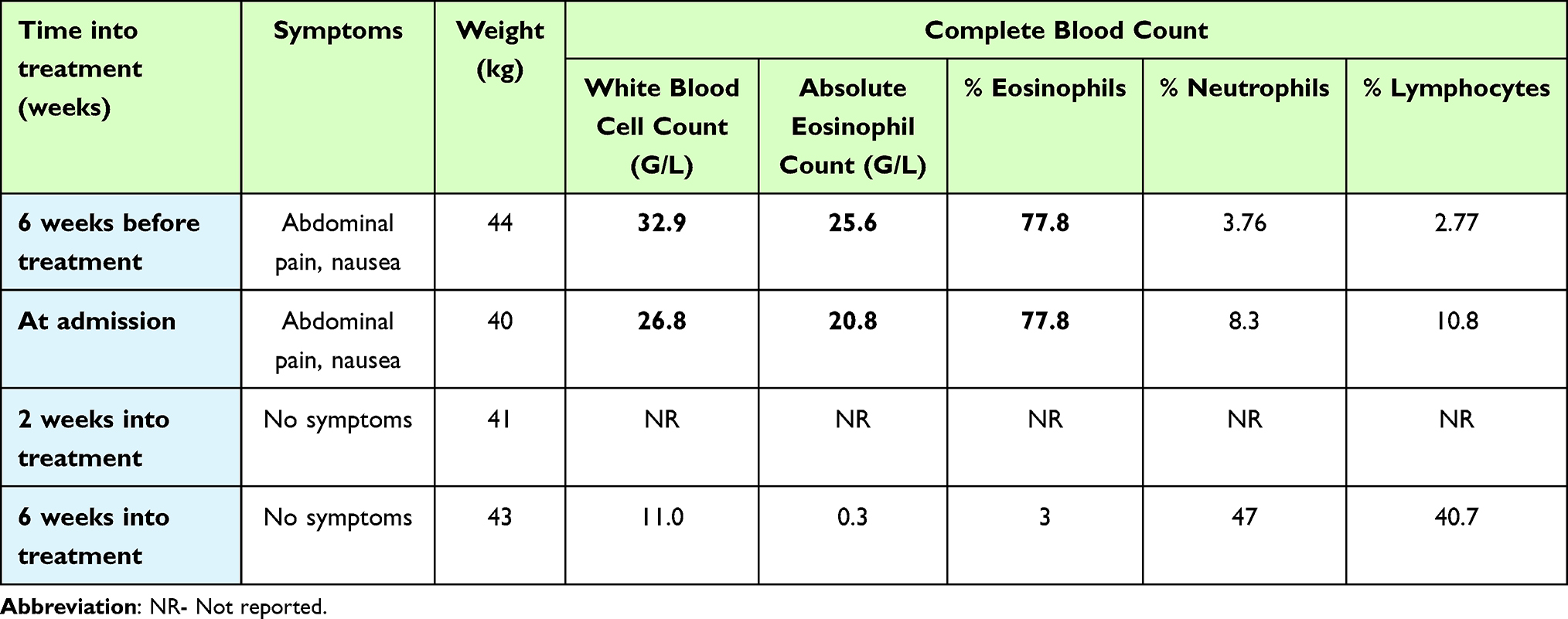 |
Table 1 Patient’s Clinical Progression During Treatment |
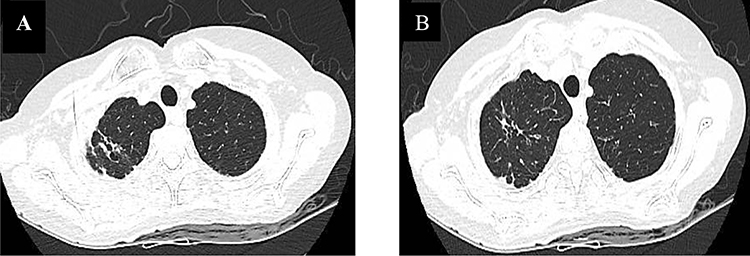 |
Figure 1 Bronchiectasis and fibrosis in the upper lobes of both lungs. (A) Computed tomography (CT) scan showing bronchiectasis in the upper lobes. (B) CT scan revealing fibrosis in the same regions. |
 |
Figure 2 Colitis without ulceration. Colonoscopy images demonstrating mucosal inflammation in the sigmoid, left, transverse, and right colon, indicative of colitis but without evidence of ulcer formation. |
 |
Figure 3 Eosinophilic infiltration in the colon. Histopathological examination of colon mucosa biopsy with hematoxylin and eosin (H&E) staining showing significant eosinophilic infiltration in the lamina propria (A) (HEx40) and (B) (HEx100). |
Discussion
EGIDs encompass a spectrum of rare diseases characterized by eosinophilic infiltration of the gastrointestinal tract.1 Eosinophilic colitis (EoC) is the least common among EGIDs, with a prevalence of 2.1 to 3.3 cases per 100,000 people.2 Despite its rarity, EoC is increasingly recognized due to increased awareness and improved diagnostic techniques.3 EoC can affect both adults and children, presenting in varying degrees depending on the depth and extent of eosinophilic infiltration. The pathophysiology of EoC is thought to be related to atopic processes, presenting primarily as a food allergy in infants and T-lymphocyte-mediated (ie, non-IgE related) in older patients.4 EoC can be classified as primary, with secondary forms related to infections (mainly parasitic infections), inflammatory bowel disease, celiac disease, drug-induced reactions, neoplasia, connective tissue diseases, hypereosinophilic syndrome, and other etiology.5
Clinical manifestations of EoC are nonspecific and depend on the site and depth of eosinophilic infiltration.1 Klein’s classification describes three clinical forms based on the involved layer: mucosal, muscular, and serosal.6 Muscular involvement can cause intestinal obstruction, and serosal involvement may result in ascites.7 Our patient presented with abdominal pain, diarrhea, vomiting, and weight loss, reflecting a primarily mucosal pattern. This nonspecific symptomatology initially led to a misdiagnosis of gastrointestinal infection and inappropriate antibiotic treatment without symptomatic relief.
Peripheral eosinophilia is observed in two-thirds of patients with EoC. Elevations in serum IgE levels are typical in these patients. Atopic illnesses such as asthma and eczema may coexist.8 Our patient had an absolute blood eosinophil count of 20.8 G/L, slightly elevated IgE but with a high IgG4 level. Although the serum IgG4 level has been described as the most sensitive and specific laboratory test for the diagnosis of IgG4-related disease, it is recognized that elevated serum IgG4 level can be encountered in other diseases.9 IgG4 antibodies inhibit allergen binding to IgE and attenuate mast cell degranulation, followed by inhibition of eosinophil infiltration. Therefore, the discrepancy between IgG4 levels and eosinophil counts observed in some patients may be due to this anti-inflammatory response. Diffuse IgG4 deposition in the gastrointestinal tract is a new characteristic of EGIDs and may be associated with their pathogenesis.10 Blood and stool tests were performed to check for parasite infestation. With a positive result for toxocariasis from a serology test, 400 mg of albendazole was administered twice a day for five days. However, she did not experience any improvement in her symptoms. A bone marrow aspiration and peripheral blood smear were performed to rule out hypereosinophilic syndrome and other hematologic malignancies. Despite her history of asthma, she did not exhibit any symptoms of neuropathy or nasal polyps and the results of her ANCA test were negative. She also underwent a bronchoscopy, which revealed no abnormalities. The cytology of the bronchoalveolar lavage fluid revealed the absence of eosinophils, making Churg-Strauss syndrome improbable.
In patients with EoC, endoscopic changes are rather modest and are not characteristic. These may include patchy areas of mucosal edema, punctate erythema, elevated lesions, pale granular mucosa, and aphthous ulceration. However, these findings are uncommon and in most cases, the mucosa appears normal during endoscopy.11 Histological examination of colon biopsies remains a key to diagnosis despite the absence of a universally accepted histological threshold for EoC. While the authors advocate a cutoff of 15 to 25 eosinophils per HPF without specifying the segment, others propose higher thresholds depending on the colonic segment.4,12 In our case, significant eosinophilic infiltration (exceeding 85 eosinophils/HPF in the left colon and more than 100 eosinophils/HPF in the transverse and right colon) confirmed the diagnosis of EoC.
The management of EoC lacks standardized guidelines, relying primarily on case reports and small series.1,3 Corticosteroids, such as prednisolone (20–40 mg/day), with rapid absorption, constitute the mainstay of treatment and are effective in both children and adults.13 Some individuals may require prolonged therapy or long-term, low-dose maintenance.14 Immunomodulatory agents such as azathioprine or 6-mercaptopurine can be considered for severe, refractory, or steroid-dependent EoC.13 Montelukast, a leukotriene receptor antagonist, has shown promise as a steroid-sparing agent.15 Our patient responded well to an initial oral methylprednisolone and montelukast regimen, with symptom resolution and a significant reduction in eosinophil count within two weeks. After absorption of corticosteroids, the patient remained symptom-free on montelukast for three months.
Conclusion
This case report highlights the rare coexistence of EoC, asthma, and elevated IgG4 levels. EoC should be suspected in patients with unexplained gastrointestinal symptoms and extreme peripheral eosinophilia despite a relatively normal appearing mucosa on colonoscopy. The co-occurrence of these conditions underscores the need for a comprehensive diagnostic approach, especially in patients with atopic diseases. The patient’s positive response to corticosteroids and maintenance of montelukast suggests effective treatment strategies.
Abbreviations
EGID, Eosinophilic Gastrointestinal Disease; EoC, Eosinophilic colitis; IgG4, Immunoglobulin subclass 4.
Ethical Approval and Consent for Publication
Written informed consent was obtained from the patient for the publication of this paper. Approval to publish the case details was not required in our institution.
Funding
There is no funding to report.
Disclosure
Qui Huu Nguyen and Tram Que Nguyen Pham are co-first authors. The authors declare they have no competing interest for this study.
References
1. Li K, Ruan G, Liu S, et al. Eosinophilic gastroenteritis: pathogenesis, diagnosis, and treatment. Chin Med J. 2023;136(8):899–909. doi:10.1097/cm9.0000000000002511
2. Mansoor E, Abou Saleh M, Cooper GS. Prevalence of eosinophilic gastroenteritis and colitis in a population-based study, from 2012 to 2017. Clin Gastroenterol Hepatol. 2017;15(11):1733–1741. doi:10.1016/j.cgh.2017.05.050
3. Uppal V, Kreiger P, Kutsch EJ. Eosinophilic gastroenteritis and colitis: a comprehensive review. Clin Rev Allergy Immunol. 2016;50:175–188. doi:10.1007/s12016-015-8489-4
4. Yan BM, Shaffer EA. Primary eosinophilic disorders of the gastrointestinal tract. Gut. 2009;58(5):721–732. doi:10.1136/gut.2008.165894
5. Alfadda AA, Storr MA, Shaffer EA. Eosinophilic colitis: epidemiology, clinical features, and current management. Ther Adv Gastroenterol. 2011;4(5):301–309. doi:10.1177/1756283x10392443
6. Sunkara T, Rawla P, Yarlagadda KS, Gaduputi VJ. Eosinophilic gastroenteritis: diagnosis and clinical perspectives. Clinical Exp Gastroenterol. 2019;12:239–253. doi:10.2147/CEG.S173130
7. Talley NJ, Shorter RG, Phillips SF, Zinsmeister AR. Eosinophilic gastroenteritis: a clinicopathological study of patients with disease of the mucosa, muscle layer, and subserosal tissues. Gut. 1990;31(1):54–58. doi:10.1136/gut.31.1.54
8. Kinoshita Y, Sanuki T. Review of non-eosinophilic esophagitis-eosinophilic gastrointestinal disease (Non-EoE-EGID) and a case series of twenty-eight affected patients. Biomolecules. 2023;13(9):1417. doi:10.3390/biom13091417
9. Ryu JH, Horie R, Sekiguchi H, Peikert T, Yi ES. Spectrum of disorders associated with elevated serum IgG4 levels encountered in clinical practice. Int J Rheumatol. 2012;2012:1–6. doi:10.1155/2012/232960
10. Ming B, Zhong J, Dong L. Role of eosinophilia in IgG4-related disease. Clinical Exp Rheumatol. 2022;40(5):1038–1044. doi:10.55563/clinexprheumatol/l7se2n
11. Turner KO, Sinkre RA, Neumann WL, Genta RM. Primary colonic eosinophilia and eosinophilic colitis in adults. Am J Surg Pathol. 2017;41(2):225–233. doi:10.1097/pas.0000000000000760
12. Collins MH. Histopathologic features of eosinophilic esophagitis and eosinophilic gastrointestinal diseases. Gastroenterol Clin North Am. 2014;43(2):257–268. doi:10.1016/j.gtc.2014.02.007
13. Alfadda AA, Storr MA, Shaffer EA. Eosinophilic colitis: an update on pathophysiology and treatment. Br Med Bull. 2011;100:59–72. doi:10.1093/bmb/ldr045
14. Chen MJ, Chu CH, Lin SC, Shih SC, Wang TE. Eosinophilic gastroenteritis: clinical experience with 15 patients. World J Gastroenterol. 2003;9(12):2813–2816. doi:10.3748/wjg.v9.i12.2813
15. Wang NW, Hsieh H, Yang YJ. Successful montelukast treatment in an infant with steroid-resistant eosinophilic colitis. Case Rep Gastroenterol. 2021;15(1):389–394. doi:10.1159/000513146
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.