Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Ultra-High-Frequency Ultrasound of Melanoma Excision Scars for Detection of Clinically Occult Local Recurrence: A Single-Center Retrospective Study
Authors Russo A, Patanè V ![]() , Bucciero L, Brunese M, Troiani T, Argenziano G, Franco R
, Bucciero L, Brunese M, Troiani T, Argenziano G, Franco R ![]() , Reginelli A
, Reginelli A
Received 14 November 2025
Accepted for publication 23 February 2026
Published 27 February 2026 Volume 2026:19 580359
DOI https://doi.org/10.2147/CCID.S580359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michela Starace
Anna Russo,1 Vittorio Patanè,1 Lucrezia Bucciero,1 Mario Brunese,1 Teresa Troiani,1 Giuseppe Argenziano,2 Renato Franco,2 Alfonso Reginelli1
1Department of Precision Medicine, University of Campania “luigi Vanvitelli”, Naples, 80138, Italy; 2Department of Mental and Physical Health and Preventive Medicine, University of Campania “Luigi Vanvitelli”, Naples, 80138, Italy
Correspondence: Vittorio Patanè, Department of Precision Medicine, University of Campania “Luigi Vanvitelli”, Piazza Luigi Miraglia 2, Naples, 80138, Italy, Tel +390815665204, Email [email protected]
Background: High- and ultra-high-frequency ultrasound (HFUS/UHFUS) may enhance early detection of clinically occult local recurrence at melanoma excision scars, where postoperative fibrotic or inflammatory changes can obscure subtle dermal–subcutaneous foci.
Methods: This single-center retrospective observational study included all consecutive patients with histologically confirmed cutaneous melanoma who underwent HFUS/UHFUS assessment of the excision scar between November 2024 and October 2025 at a tertiary referral center. Examinations were performed with a Vevo 3100 system using a 48– 70 MHz linear transducer by an experienced radiologist (> 10 years), following a standardized institutional protocol. Scars were classified as benign remodeling, indeterminate, or suspicious/highly suspicious according to predefined morphologic and vascular features. Suspicious/highly suspicious findings were referred for biopsy/excision; indeterminate findings underwent short-interval follow-up; benign-appearing scars were monitored per protocol. Histopathology and/or longitudinal follow-up served as reference standards.
Results: Among 320 patients (730 examinations), 53 scars were categorized as suspicious/highly suspicious; recurrence was histologically confirmed in 50 cases, while 3 represented fibroblast-rich extracellular matrix remodeling. All recurrences were clinically occult at imaging. No false negatives were observed within the available follow-up of ultrasound-negative scars (median 12 months; range 3– 12). Sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy were 100%, 98.9%, 94.3%, 100%, and 99.1%, respectively.
Conclusion: In an expert setting, HFUS/UHFUS provides highly reliable detection of subclinical local recurrence at melanoma excision sites and robust discrimination from benign postoperative changes, supporting its integration as an adjunct tool in specialized follow-up pathways.
Keywords: cutaneous melanoma, excision scars, high-frequency ultrasound, local recurrence, postoperative surveillance, scar imaging, ultra-high-frequency ultrasound
A Letter to the Editor has been published for this article.
Introduction
Cutaneous melanoma is an aggressive malignancy with a steadily increasing incidence worldwide and a disproportionate impact on skin cancer–related mortality.1–5 Complete surgical excision with histologically tumor-free margins, with or without sentinel lymph node biopsy according to stage and risk profile, remains the cornerstone of curative treatment for localized disease.6–10 In this context, structured postoperative surveillance plays a pivotal role in the timely detection of disease recurrence, guiding access to surgical, loco-regional, and systemic therapies that may significantly influence prognosis.11–14
Local recurrence at or near the melanoma excision scar—encompassing true local relapse, pericicatricial intradermal or subcutaneous nodules, and early in-transit deposits—represents a clinically relevant pattern of failure.15–19 These events are often associated with biologically active disease and may herald further regional or distant spread. However, in their early stages, local recurrences are frequently small, located in the superficial soft tissues, and may be clinically subtle or entirely inapparent.20–25 Their detection is further complicated by the dynamic and heterogeneous nature of postoperative wound healing, which includes fibrosis, remodeling of the extracellular matrix, inflammatory responses, and occasional granulomatous or hypertrophic scarring.26–30 Under these circumstances, clinical inspection alone shows limited sensitivity for millimetric or deep dermal–subcutaneous foci, particularly in irregular or thickened scars.
Beyond morphologic ambiguity at the surgical bed, timing is a critical determinant of surveillance design. Large cohort analyses and reviews consistently show that the hazard of melanoma recurrence is highest in the first years after treatment, with stage-dependent distributions in which a substantial proportion of recurrences—particularly in higher-risk stages—occur within the first 2 years.31,32 In high-risk cohorts, median time to first recurrence has been reported in the order of months (eg, approximately 40 weeks), supporting a closer early surveillance interval.33 At the same time, late recurrences can occur, and follow-up duration must be considered when interpreting negative predictive value estimates.34
Dermoscopy has become integral to melanoma diagnosis and follow-up, but it primarily interrogates superficial epidermal and dermal structures and is not designed to systematically assess deeper components of the surgical bed.35–38 Conventional ultrasound has been increasingly adopted for nodal staging and for the evaluation of cutaneous and subcutaneous lesions, yet its performance at the surgical site is constrained by the trade-off between penetration and spatial resolution.39–42 In the setting of recent or complex scars, conventional or standard high-frequency probes may struggle to discriminate between normal or reactive scar tissue and early neoplastic foci, and operator inexperience may further contribute to false reassurance or equivocal findings.43–46 As a result, very early local recurrences may remain undetected until they become clinically evident or reach a greater tumor burden, potentially reducing the window for optimal intervention.
High- and ultra-high-frequency ultrasound (HFUS/UHFUS), operating at significantly higher frequencies than conventional systems, offers markedly improved axial and lateral resolution for the epidermis, dermis, and superficial subcutis.47–51 This enhanced spatial definition allows detailed visualization of the microarchitecture of the excision scar, including the layered organization of cutaneous tissues, subtle focal distortions, and small nodular or infiltrative abnormalities arising in close continuity with the surgical site.52–55 The addition of sensitive Doppler techniques permits assessment of microvascular patterns that may support differentiation between quiescent fibrotic tissue and biologically active lesions.43,54,56,57 These characteristics make HFUS/UHFUS an appealing candidate for refining local surveillance strategies, particularly for the identification of clinically occult recurrences in high-risk or structurally complex scars.58
Despite this theoretical and technical potential, the role of HFUS/UHFUS in postoperative monitoring of melanoma excision scars has not been systematically defined. Recent reviews on sonographic assessment of locally recurring skin cancers emphasize that postoperative scars contain multiple mimickers (fibrosis, inflammatory changes) and that grayscale morphology combined with Doppler vascular patterns may improve discrimination between recurrence and benign remodeling.59,60 In parallel, scoping evaluations of melanoma follow-up guidelines highlight substantial variability in recommended imaging strategies, with nodal ultrasound more consistently discussed than dedicated scar imaging and cross-sectional imaging more often reserved for higher-stage disease.61 Existing data are limited, often derived from small or heterogeneous series, and its use in routine follow-up remains restricted. Key barriers include the limited availability of ultra-high-frequency equipment and the need for operators with specific expertise in dermatologic and postoperative imaging, conditions that are not widely met across centers. Consequently, current guidelines continue to rely predominantly on clinical examination, dermoscopy, and, in selected settings, conventional ultrasound, leaving a gap in evidence regarding the added value of high-resolution ultrasound for early local recurrence at the surgical site.
Within this context, the present study provides a retrospective evaluation of a consecutive series of melanoma patients monitored in a dedicated HFUS/UHFUS outpatient clinic, in which systematic high-resolution assessment of melanoma excision scars forms part of the institutional follow-up strategy. The primary objective is to describe the diagnostic performance of HFUS/UHFUS for the detection of clinically occult local recurrence at the surgical site and to define reproducible sonographic criteria capable of distinguishing true recurrence from benign postoperative changes in a real-world, specialized setting.
Methods
The study was conducted in accordance with the principles of the Declaration of Helsinki.
The research protocol received approval from the local ethics committee at the University Hospital of Campania “L. Vanvitelli” and AORN “Ospedale dei Colli”, Naples, with Protocol Number 4567/i/2024, 15th October 2024). Because the analysis was based on retrospective review of anonymized data obtained from routine clinical practice, the requirement for individual informed consent was waived by the local Ethics Committee.
Study Design
This single-center retrospective observational study was conducted at the University Hospital “Luigi Vanvitelli” in Naples, Italy, and was based on the routine activity of a dedicated high- and ultra-high-frequency ultrasound (HFUS/UHFUS) outpatient clinic for postoperative surveillance of melanoma excision scars. The clinic operates within a tertiary referral melanoma setting and provides standardized high-resolution ultrasound assessment of the surgical site as part of institutional follow-up pathways.
Patient Population
All consecutive patients with histologically confirmed cutaneous melanoma who underwent HFUS/UHFUS examination of the excision scar between November 2024 and October 2025 were eligible for inclusion. Only examinations specifically performed for surveillance of melanoma surgical sites were considered; patients with non-melanoma primary tumors or incomplete clinical or imaging data were excluded. For each patient, clinical information (including primary tumor characteristics and time from surgery) and ultrasound reports and images were retrieved from institutional archives and reviewed.
Ultrasonographic Assessment
All examinations were performed in the same facility using a Vevo 3100 system (FUJIFILM VisualSonics, Toronto, Canada) equipped with a 48–70 MHz linear transducer. This configuration provides high axial and lateral resolution for the epidermis, dermis and superficial subcutis, with a penetration depth suitable for the evaluation of melanoma excision scars and adjacent tissue. A single radiologist with more than 10 years of experience in HFUS/UHFUS and in dermatologic and postoperative imaging performed all scans, ensuring technical consistency and uniform application of the protocol. The operator’s interpretation was based on predefined institutional semeiotic criteria that were used prospectively in the dedicated surveillance clinic. For the purposes of this retrospective analysis, scar-category assignment (benign/indeterminate/suspicious) was performed without reference to subsequent histopathology results; however, as in routine surveillance practice, the operator was aware of the clinical context and time from surgery at the time of image acquisition. Examinations were acquired in longitudinal and transverse planes along and across the scar, using a thin layer of coupling gel and, when necessary, a stand-off pad to optimize acoustic contact with superficial structures. Static B-mode imaging was systematically obtained in all cases; color Doppler assessment was performed when technically feasible to evaluate microvascularity.
Follow-Up Protocol
Ultrasound examinations were integrated into an institutional surveillance schedule that recommended HFUS/UHFUS assessment of the excision scar every 3 months during the first 2 years after surgery and every 6 months from year 3 to year 5. This timing was chosen to mirror the known temporal pattern of recurrence risk, which is typically front-loaded within the first 2–3 years after treatment (especially in higher-risk stages), while maintaining structured surveillance through year 5 to account for later events. Additional examinations could be scheduled in higher-risk patients, as defined by primary tumor stage, Breslow thickness, and multidisciplinary tumor board evaluation, or in the presence of equivocal clinical findings, but all within the framework of this structured protocol. For the purposes of the present study, patients could contribute one or more examinations according to their position along this follow-up pathway.
Ultrasonographic Semeiotic of Scar Findings
For the retrospective analysis, all available HFUS/UHFUS images and reports were systematically reviewed and each surgical site was categorized according to predefined sonographic criteria. Lesions were classified into three diagnostic categories: benign remodeling, indeterminate, and suspicious or highly suspicious for local recurrence. Benign remodeling was defined by linear or band-like hyperechoic scar tissue along the surgical axis, preservation or progressive reconstitution of the layered architecture, absence of discrete nodular components, and minimal or absent intralesional vascular signal. Indeterminate findings included subtle focal thickening or hypoechoic changes with partial architectural distortion but without a well-formed nodular lesion or clearly aberrant vascularity, in keeping with possible active remodeling or inflammatory changes. No absolute size threshold was prespecified for upgrading a finding; rather, categorization relied on morphology (discrete nodular lesion versus non-nodular thickening), degree of architectural disruption, orientation relative to the scar axis, and, when technically feasible, Doppler vascular signal. For indeterminate findings, evolution on short-interval follow-up (progression in size/echotexture/architecture/vascularity) was the prespecified trigger for reclassification as suspicious and referral for histologic verification. Suspicious or highly suspicious lesions were characterized by newly appearing or progressively enlarging hypoechoic or heterogeneous nodules within or immediately adjacent to the scar, disruption of normal cutaneous planes, nodular or ovoid morphology not aligned with the scar, and, when assessable, the presence of internal or peripheral vascular signals inconsistent with a quiescent scar. Classification was performed by the same experienced operator, with knowledge of the clinical context and timing from surgery but independently of subsequent histopathological results and therapeutic decisions.
Management Pathway and Reference Standard
Management decisions were guided by these categories within a predefined pathway. All lesions classified as suspicious or highly suspicious for local recurrence were systematically discussed in a multidisciplinary tumor board and referred for surgical excision or biopsy of the scar region. Histopathological examination of these specimens served as the reference standard to confirm or exclude melanoma recurrence. Indeterminate lesions were scheduled for short-interval HFUS/UHFUS re-evaluation, generally within 3 to 6 months. Lesions in this group that demonstrated progression in size, echotexture, architectural distortion, or vascularity were subsequently treated as suspicious and referred for histological verification; those that stabilized or normalized over time were reclassified as benign postoperative changes (Figure 1). Scars classified as benign remodeling were followed according to the institutional surveillance protocol; the absence of clinical or sonographic evidence of recurrence over a minimum follow-up period of 6 months, or until the end of the study period when shorter, was considered confirmatory for true negative status.
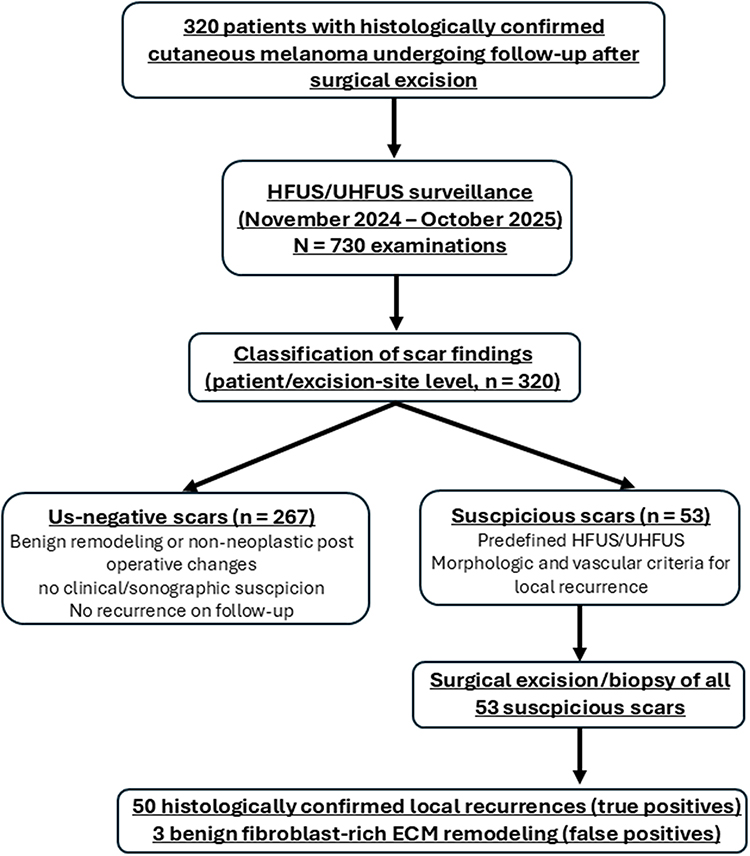 |
Figure 1 HFUS/UHFUS-based management algorithm for melanoma excision scars. Excision scars are systematically evaluated with high- and ultra-high-frequency ultrasound and classified as benign remodeling, indeterminate, or suspicious/highly suspicious for local recurrence according to predefined morphologic and vascular criteria. Benign scars continue routine surveillance. Indeterminate findings undergo short-interval HFUS/UHFUS reassessment (3–6 months), with lesions that progress being upgraded to suspicious. All suspicious/highly suspicious lesions are discussed within a multidisciplinary tumor board and referred for biopsy or re-excision of the scar region. |
For the present analysis, follow-up duration for ultrasound-negative scars (benign and indeterminate lesions that stabilized/regressed) was calculated from the index HFUS/UHFUS examination to the last available clinical and/or ultrasound assessment, and summarized as median (range).
Diagnostic Performance Analysis
For the evaluation of diagnostic performance, melanoma local recurrence at the excision site, as documented by histopathology, represented the target condition. True positives were defined as lesions classified as suspicious/highly suspicious with histologically confirmed recurrence; false positives as suspicious/highly suspicious lesions with benign histology; true negatives as lesions classified as benign (or indeterminate lesions that normalized) with no local recurrence during follow-up; and false negatives as any scar classified as benign or indeterminate that later developed histologically proven local recurrence at the same site. Sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy of HFUS/UHFUS for local recurrence were calculated with corresponding proportions. Diagnostic performance was assessed at the scar level (one observation per excision site), using histopathology and/or longitudinal follow-up as reference standards as described above. Serial ultrasound examinations were used to document stability/regression or progression over time but were not treated as independent observations for performance calculations. We additionally report 95% confidence intervals for all diagnostic estimates using exact binomial methods (Clopper–Pearson), given the limited number of recurrence events. Given the retrospective, exploratory design and single-center setting, no formal sample size calculation was performed.
Results
Study Population and Examinations
During the study period, 320 consecutive patients with histologically confirmed cutaneous melanoma underwent HFUS/UHFUS evaluation of the excision scar in the dedicated outpatient clinic. All examinations were performed exclusively for postoperative surveillance of melanoma surgical sites. According to the institutional follow-up schedule and risk-adapted adjustments, these patients contributed a total of 730 HFUS/UHFUS examinations, reflecting serial assessments at different time points along the surveillance pathway (Figure 2). To contextualize recurrence timing, recurrences detected at the excision site were summarized by time from surgery to ultrasound detection (≤12 months, 13–24 months, and >24 months), and corresponding descriptive performance estimates with confidence intervals are reported where sample size permits.
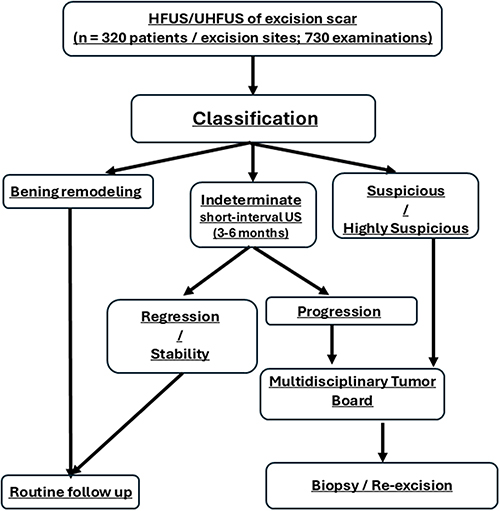 |
Figure 2 HFUS/UHFUS-based management algorithm for melanoma excision scars. The figure depicts the schematic decision pathway used in our dedicated surveillance clinic. HFUS/UHFUS examinations are performed on melanoma excision scars and classified as benign remodeling, indeterminate, or suspicious/highly suspicious according to predefined morphologic and vascular criteria. Indeterminate findings undergo short-interval reassessment (3–6 months): lesions showing regression/stability return to routine follow-up, whereas lesions showing progression are discussed at the multidisciplinary team and managed as suspicious/highly suspicious. Suspicious/highly suspicious findings are triaged to biopsy or re-excision. Counts and denominators are explicitly distinguished at the figure level (n = 320 patients/excision sites; n = 730 examinations), while outcome accounting and denominators by final categories are reported in the study flowchart (Figure 1). |
Distribution of Scar Outcomes
Retrospective review of clinical, sonographic, and histopathological data allowed classification of surgical sites into three principal outcome groups. Histologically confirmed local recurrence at or adjacent to the excision scar was documented in 50 patients during the observation period. One hundred patients showed complicated but non-neoplastic postoperative changes, including hypertrophic or keloid scars, nodular fibrotic remodeling, or inflammatory and granulomatous reactions, without evidence of melanoma recurrence. The remaining 170 patients exhibited uncomplicated scar remodeling, with regular or progressively normalized echotexture and no clinical or imaging suspicion of local recurrence throughout available follow-up.
According to the predefined HFUS/UHFUS criteria, 53 excision sites were prospectively or retrospectively categorized as suspicious or highly suspicious for local recurrence. All such cases were referred for surgical excision or biopsy following multidisciplinary discussion. Histopathological examination confirmed melanoma recurrence in 50 of these lesions, whereas 3 nodular abnormalities corresponded to benign fibroblast-rich extracellular matrix remodeling, and were therefore classified as false-positive ultrasound findings (Figure 3).
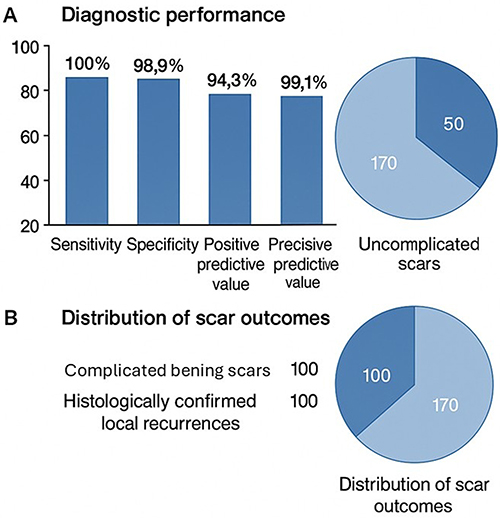 |
Figure 3 Diagnostic performance and outcome distribution. (A) Observed diagnostic performance of HFUS/UHFUS for detection of local recurrence at melanoma excision scars, reported with underlying event counts and exact 95% confidence intervals (Clopper–Pearson): sensitivity 100.0% (50/50; 95% CI 92.9–100.0%), specificity 98.9% (267/270; 95% CI 96.8–99.8%), positive predictive value 94.3% (50/53; 95% CI 84.3–98.8%), negative predictive value 100.0% (267/267; 95% CI 98.6–100.0%), and overall accuracy 99.1% (317/320; 95% CI 97.3–99.8%). Event counts are summarized as TP = 50, FP = 3, TN = 267, FN = 0 (excision-site level). (B) Distribution of final excision-scar outcomes among 320 sites: uncomplicated benign remodeling (n = 170), complicated but non-neoplastic postoperative changes (n = 100), and histologically confirmed local recurrence (n = 50). |
Lesions classified as indeterminate at initial assessment were managed with short-interval HFUS/UHFUS re-evaluation.
Overall, indeterminate findings comprised 53 excision sites. All of these demonstrated progression on short-interval imaging and were upgraded to suspicious and referred for biopsy/excision. For conservatively managed indeterminate scars, final ground truth was established by longitudinal stability/regression on ultrasound and absence of clinical/sonographic recurrence during follow-up.
Those that demonstrated progressive normalization of echotexture and vascularity were ultimately considered benign postoperative changes. None of the scars initially classified as benign remodeling, nor the indeterminate lesions that stabilized or regressed during follow-up, developed histologically proven local recurrence at the same site within the study period.
Diagnostic Performance of HFUS/UHFUS
Using histologically confirmed local recurrence at the surgical site as the reference standard, HFUS/UHFUS correctly identified all 50 recurrent cases among the 53 lesions deemed suspicious or highly suspicious, resulting in 50 true positives and 3 false positives. No false negatives were observed, as no patient with an HFUS/UHFUS classification of benign remodeling or indeterminate (subsequently regressing or stabilizing) experienced a documented local recurrence during follow-up. The median follow-up for ultrasound-negative scars was 12 months (range 3–12). On a per-patient basis, this corresponded to 267 true negatives.
The resulting observed diagnostic performance of HFUS/UHFUS for local recurrence at melanoma excision scars in this dedicated setting was as follows: sensitivity 100%, specificity 98.9%, positive predictive value 94.3%, negative predictive value 100%, and overall accuracy 99.1%. Exact 95% confidence intervals (Clopper–Pearson) were calculated to reflect estimate precision: sensitivity 100.0% (95% CI 92.9–100.0%), specificity 98.9% (95% CI 96.8–99.8%), positive predictive value 94.3% (95% CI 84.3–98.8%), negative predictive value 100.0% (95% CI 98.6–100.0%), and overall accuracy 99.1% (95% CI 97.3–99.8%). All confirmed local recurrences were clinically occult or only minimally apparent at the time of ultrasound detection, underscoring the contribution of high-resolution imaging in revealing early disease that was not confidently identifiable on clinical examination alone (Figure 4).
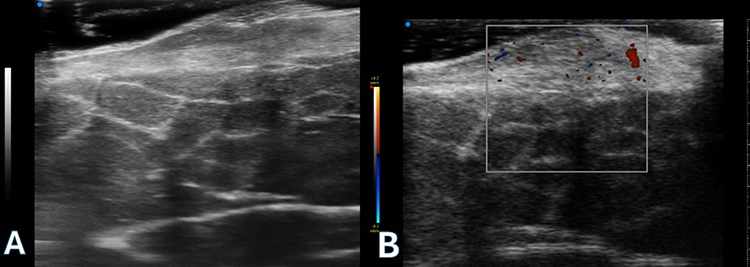 |
Figure 4 Benign postoperative nodular scar mimicking local recurrence on high-frequency ultrasound. (A) HFUS image of the melanoma excision site showing a superficially located, heterogeneously hyperechoic nodular area along the scar, with partial distortion of the normal cutaneous architecture and features initially interpreted as suspicious. (B) Color Doppler assessment demonstrating discrete intralesional vascular signals, further supporting the provisional classification as highly suspicious. White box indicating Region Of Interest for Doppler signal detection. Surgical excision was performed, and histopathological analysis revealed fibroblast-rich collagenous extracellular matrix remodeling without evidence of melanoma, representing one of the HFUS false-positive cases. The blue dot in the upper-left corner denotes the ultrasound probe orientation marker (transducer notch), indicating the screen-left side of the image. |
Sonographic Features and Management of Recurrent Lesions
Recurrent lesions consistently exhibited the predefined sonographic features associated with suspicion for local recurrence (Figures 5 and 6). They appeared as newly detected or progressively enlarging hypoechoic or heterogeneous nodules arising within or immediately adjacent to the scar, with disruption of the normal layered architecture and morphology incongruent with linear fibrotic remodeling. In a relevant proportion of cases, color Doppler interrogation demonstrated internal or peripheral vascular signals supporting the presence of biologically active tissue rather than quiescent scar (Figure 7). Application of these criteria guided triage to surgical excision or biopsy, enabling histopathological confirmation in all suspected cases and supporting the robustness of the HFUS/UHFUS-based classification in discriminating true local recurrence from benign postoperative changes in this specialized clinical context.
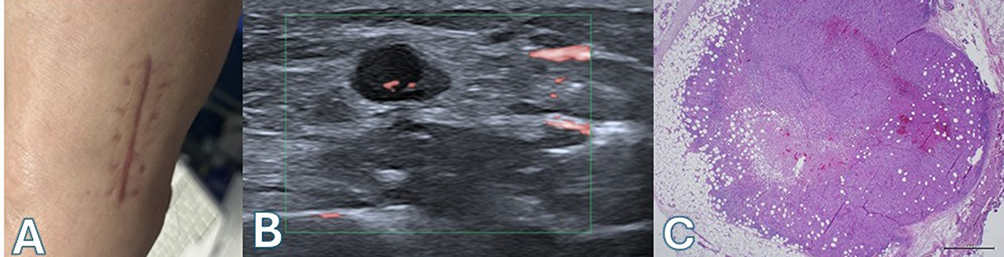 |
Figure 5 Clinically occult local recurrence at a melanoma excision scar detected by high-frequency ultrasound. (A) Clinical appearance of the linear excision scar on the lower limb, without evident nodular recurrence. (B) HFUS image demonstrating a well-defined hypoechoic nodule deep to the scar, with internal vascular signals on color Doppler, fulfilling predefined criteria for a suspicious lesion. (C) Corresponding histopathological section confirming melanoma recurrence within the nodular lesion. The blue dot in the upper-left corner denotes the ultrasound probe orientation marker (transducer notch), indicating the screen-left side of the image. Scale bar = 500 µm: 1cm. The green rectangular box indicates the color Doppler region of interest (ROI) over which flow is sampled. |
 |
Figure 6 High-frequency ultrasound detection of a small nodular local recurrence at a melanoma excision scar. (A) Clinical inspection of the lateral trunk scar reveals no evident nodular recurrence on palpation. (B) HFUS with color Doppler demonstrates a small hypoechoic nodule adjacent to the scar with internal vascular signals, fulfilling predefined criteria for a suspicious lesion; dotted alphabetical labels “A” and “B” in this panel denote measurement reference markers used to identify the lesion’s axial dimensions. (C) Corresponding gray-scale HFUS image confirms a well-defined hypoechoic focus disrupting the normal superficial architecture; the same “A” and “B” markers indicate the axial measurement references. (D) Histopathological section of the excised lesion shows dermal melanoma recurrence, correlating with the ultrasound findings. The blue dot in the upper-left corner denotes the ultrasound probe orientation marker (transducer notch), indicating the screen-left side of the image. The green rectangular box indicates the color Doppler region of interest (ROI) over which flow is sampled. Green dotted lines represent the ultrasound system’s electronic calipers/crosshair used for positioning and measurement; the (+) symbol marks the cursor/intersection point. Scale bar = 500 µm: 1. |
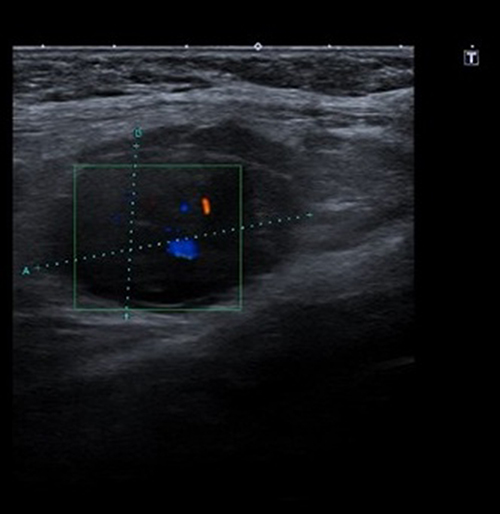 |
Figure 7 High-frequency ultrasound of a suspicious nodular lesion at a melanoma excision site. Gray-scale HFUS shows a well-defined hypoechoic nodule within the superficial soft tissues contiguous with the scar; electronic calipers indicate the maximal long- and short-axis diameters, with dotted alphabetical markers “A” and “B” denoting the measurement reference labels for the lesion’s axial dimensions. Color Doppler demonstrates discrete internal vascular signals, fulfilling predefined criteria for a “suspicious” lesion within our HFUS/UHFUS framework. According to the management algorithm, such findings are triaged to multidisciplinary discussion and referred for biopsy or re-excision of the scar region. The blue dot in the upper-left corner denotes the ultrasound probe orientation marker (transducer notch), indicating the screen-left side of the image. The green rectangular box indicates the color Doppler region of interest (ROI) over which flow is sampled. Green dotted lines represent the ultrasound system’s electronic calipers/crosshair used for positioning and measurement; the (+) symbol marks the cursor/intersection point. |
Discussion
This single-center retrospective experience shows that high- and ultra-high-frequency ultrasound, when implemented within a dedicated outpatient clinic and applied systematically to melanoma excision scars, can reliably detect clinically occult local recurrence with very high diagnostic performance. Across 320 consecutive patients and 730 examinations, HFUS/UHFUS correctly identified all histologically confirmed local recurrences at the surgical site, with three false-positive findings and no documented false negatives during the observation period.
Importantly, these estimates are based on 50 histologically confirmed scar-site recurrences (and three false positives), and we now report exact 95% confidence intervals for sensitivity, specificity, PPV, and NPV to reflect estimate precision. In addition, we clarify that the observed NPV reflects no false negatives observed within the available follow-up of ultrasound-negative scars; the median and range follow-up in benign scars and indeterminate scars that stabilized/regressed, as well as the proportion with ≥12 months follow-up, are reported to support true-negative classification and to contextualize the potential impact of delayed recurrences on NPV. These data support the concept that, under appropriate technical and organizational conditions, high-resolution ultrasound can distinguish true local recurrence from benign postoperative changes in a challenging anatomical and biological context.
The early detection of local recurrence at the melanoma excision site is clinically relevant and non-trivial. Local relapse and pericicatricial or in-transit disease may represent biologically active tumor, are associated with an increased risk of further spread, and can modify both staging and therapeutic strategy. However, the surgical bed is a complex environment: fibrosis, extracellular matrix remodeling, reactive nodularity, suture granulomas, hypertrophic or keloid scars, and low-grade inflammation may all mimic or obscure small foci of recurrent melanoma. Clinical examination and dermoscopy, although essential, are inherently limited in their ability to interrogate deep dermal and superficial subcutaneous compartments, especially in thickened or irregular scars. Conventional ultrasound, in turn, may not provide sufficient spatial resolution at the very superficial layers and is particularly vulnerable to interpretative uncertainty in non-expert hands, which may result in both over-calling and, more critically, false reassurance.
Within this framework, our findings illustrate how HFUS/UHFUS can address part of this unmet need. By offering micrometric resolution of the epidermis, dermis, and superficial subcutis, HFUS/UHFUS enables direct visualization of the fine architecture of the scar and adjacent tissues. In our cohort, recurrent melanoma at the surgical site displayed a consistent set of sonographic features: newly appearing or progressively enlarging hypoechoic or heterogeneous nodules arising within or immediately adjacent to the scar, disruption of normal layered architecture, morphology discordant with linear fibrotic remodeling, and, in many cases, internal or peripheral vascularity suggestive of viable tumor. When these predefined criteria were present, histopathological examination confirmed melanoma recurrence in the vast majority of cases. Conversely, lesions corresponding to benign fibroblast-rich remodeling and other non-neoplastic changes, although sometimes nodular, lacked the full combination of structural and vascular abnormalities and were ultimately classified as false positives in only a very small fraction of patients. Scars with sonographic features of benign remodeling and indeterminate findings that normalized or remained stable during follow-up did not evolve into proven recurrence, supporting the robustness of the classification framework.
A key strength of this study lies in the structured methodology underpinning this experience. All examinations were performed using the same high-end HFUS/UHFUS platform by a single radiologist with specific expertise in dermatologic and postoperative imaging, ensuring technical uniformity and consistent application of diagnostic criteria. The cohort included consecutive melanoma patients undergoing routine institutional surveillance, reducing selection based on suspicion alone and anchoring the findings in real-world clinical practice. The use of explicit, a priori criteria to classify scars into benign, indeterminate, and suspicious/highly suspicious categories, combined with a predefined management algorithm, allowed clear linkage between imaging findings, clinical decisions, and outcomes. Importantly, all lesions categorized as suspicious or highly suspicious for local recurrence were systematically referred for surgical excision or biopsy and underwent histopathological verification, thereby providing a solid reference standard for performance estimates. The absence of observed false negatives within the available follow-up period, although interpreted with due caution, further supports the reliability of HFUS/UHFUS in this dedicated context. The absence of observed false negatives in this cohort is therefore reassuring but cannot be interpreted as an absolute guarantee of perfect sensitivity beyond the observed follow-up. Accordingly, limited follow-up of ultrasound-negative scars could inflate the observed negative predictive value if delayed scar-site recurrences occur beyond the available observation window; this underlines the need for longer prospective follow-up to confirm durability of NPV estimates.
Equally relevant is the ability of HFUS/UHFUS not only to detect recurrence, but also to prevent overtreatment by supporting confident recognition of benign postoperative changes. In a setting where scar irregularities and nodularities are common, the capacity to differentiate reactive or fibrotic remodeling from lesions that warrant excision has tangible clinical and organizational implications. By anchoring management decisions to well-defined sonographic categories, this approach favors targeted biopsy or re-excision of truly suspicious findings and reduces unnecessary procedures in patients with physiologic healing, while maintaining a high level of safety through continued ultrasound-based surveillance.
These strengths, however, also delineate the principal limitations and boundaries of interpretation. The study is retrospective, single-center, and based on the experience of one highly trained operator working in a specialized clinic equipped with ultra-high-frequency technology. The excellent diagnostic metrics observed here must therefore be regarded as “best-case scenario” performance in an optimized environment, not automatically generalizable to centers without similar expertise or resources. Operator dependency is intrinsic to ultrasound, and the learning curve for HFUS/UHFUS in dermatologic applications is non-negligible; it is plausible that both sensitivity and specificity would be lower in less experienced hands or with less standardized protocols. Moreover, while the institutional surveillance schedule was clearly defined, risk-adapted intensification of follow-up for selected patients introduces the possibility of surveillance bias, with closer monitoring in higher-risk individuals potentially favoring earlier detection. The real-world nature of this adaptation reflects good clinical practice but should be acknowledged when extrapolating results.
Another limitation is the restricted temporal window of this analysis. Although scars classified as benign or normalized indeterminate findings were followed for at least several months and, in many cases, longer, the study period does not fully capture very late local recurrences. The absence of false negatives in this cohort is therefore reassuring but cannot be interpreted as an absolute guarantee of perfect sensitivity beyond the observed follow-up. Similarly, although all suspicious lesions underwent histopathological confirmation, not every benign or indeterminate lesion was biopsied, and classification in these groups relies on combined imaging and clinical follow-up as a reference standard, with the inherent, albeit limited, risk of residual misclassification.
Similarly, although all suspicious lesions underwent histopathological confirmation, not every benign or indeterminate lesion was biopsied, and classification in these groups relies on combined imaging and clinical follow-up as a reference standard, with the inherent, albeit limited, risk of residual misclassification.
Finally, this study did not include a formal, parallel-arm comparison with conventional ultrasound, and claims of superiority of HFUS/UHFUS over standard techniques should be made with caution.
Nevertheless, comparison with the existing literature supports the plausibility and clinical relevance of our approach. Reviews focused on ultrasound assessment of local recurrence in skin tumors describe recurrence as a focal mass with architecture distortion and possible low-flow vascularity, while underscoring the interpretative challenge posed by postoperative scarring and inflammatory mimickers—elements directly reflected in our three-category scar framework.59,60 Evidence syntheses on high-resolution ultrasonography during melanoma surveillance also acknowledge heterogeneity and limited high-level data specifically addressing local recurrence/satellite disease near the scar, reinforcing the need for scar-dedicated studies with standardized criteria and clear reference standards.
Alternative modalities provide complementary—but not interchangeable—information. Dermoscopy and reflectance confocal microscopy have been studied mainly for evaluating new pigmentation within/adjacent to melanoma scars, where RCM can support biopsy triage by improving assessment of superficial recurrence patterns; however, these techniques have limited ability to interrogate deeper dermal–subcutaneous compartments, which are central to the clinically occult nodules targeted in our study. Conversely, cross-sectional imaging (CT/MRI/PET/CT) is principally oriented to regional/distant disease detection and is variably recommended across guidelines, more commonly at higher stages, making it less suited to systematic detection of millimetric superficial scar foci.62 Despite these constraints, the present experience has relevant clinical implications. It demonstrates that integration of HFUS/UHFUS into a structured melanoma follow-up program is feasible and highly informative in a specialized setting, and that systematic use of predefined sonographic criteria can translate into accurate triage of scars into benign, reactive, and truly recurrent categories. These findings support the inclusion of HFUS/UHFUS as an adjunct to clinical and dermoscopic examination in tertiary centers, particularly for high-risk patients and in the presence of complex or evolving scars. From an implementation perspective, we propose integrating HFUS/UHFUS scar imaging into routine follow-up as a risk-adapted adjunct, with the strongest justification in patients at increased recurrence risk (eg, stage IIB–IIC and stage III, thick/ulcerated primaries, positive sentinel node, or multidisciplinary-defined high-risk profiles) and in scars that are clinically difficult to assess (hypertrophic/keloid remodeling, graft/flap reconstruction, or anatomically challenging sites). Stage-based melanoma follow-up recommendations support risk-adapted surveillance strategies over uniform imaging, typically extending at least 5 years.63,64 Given that recurrence hazard is often front-loaded in the first few years but remains heterogeneous, we consider scar HFUS/UHFUS at 3-month intervals in years 0–2 and 6-month intervals in years 3–5 a pragmatic schedule in higher-risk patients, while reserving scar ultrasound for selective indications (equivocal clinical findings, symptoms, or complex scars) in lower-risk stages. Recent recurrence-timing data in high-risk cohorts—showing that most recurrences occur within the first few years—support closer early surveillance while acknowledging the possibility of later events.65,66 Future research should focus on multicenter prospective validation of the proposed criteria, assessment of interobserver agreement, evaluation of performance across different levels of expertise and equipment, and formal comparison with conventional ultrasound-based protocols. Such efforts are essential to define the role of HFUS/UHFUS within evidence-based guidelines and to determine under which conditions its routine use is justified.
In conclusion, this retrospective single-center study indicates that HFUS/UHFUS, when applied within a dedicated and experienced clinical environment, provides highly reliable detection of clinically occult local recurrence at melanoma excision scars and robust discrimination from benign postoperative changes. While further validation is required, these findings contribute to bridging an important gap in postoperative surveillance and outline a pragmatic framework for the rational use of high-resolution ultrasound in specialized melanoma care.
Conclusion
This single-center retrospective study suggests that high- and ultra-high-frequency ultrasound, when implemented in a dedicated follow-up clinic and applied using predefined criteria, can support detection of clinically occult local recurrence at melanoma excision scars and differentiation from postoperative changes in a specialized setting. Within this optimized setting, HFUS/UHFUS correctly identified all histologically confirmed local recurrences, with a very limited number of false-positive findings supporting its role as a sensitive and safe imaging tool for surveillance of the surgical site.
These results should be interpreted in light of the specific context in which they were obtained—namely, a tertiary referral center with dedicated technology, a standardized protocol, and an experienced operator—and do not justify uncritical extrapolation to all practice environments. Moreover, the observed negative predictive value is contingent on the duration of longitudinal confirmation in ultrasound-negative scars, and delayed scar-site recurrences beyond the available follow-up could reduce NPV; therefore, broader clinical adoption should await prospective multicenter validation with longer follow-up and multi-operator assessment. However, they provide a coherent and clinically meaningful framework for the use of HFUS/UHFUS as an adjunct to clinical and dermoscopic examination in specialized centers, particularly for high-risk patients and complex scars. Prospective multicenter studies, formal comparison with conventional ultrasound protocols, and assessment of performance across different levels of expertise are warranted to validate these findings and to define the conditions under which high-resolution ultrasound may be incorporated into evidence-based guidelines for postoperative surveillance of cutaneous melanoma.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brown M, Zhou AE, Dunbar D, et al. Requiring all surgeries to be referred to in-house dermatologic surgeons: is it ethical or a profit haven? Clin Dermatol. 2025;43(3):420–14. doi:10.1016/j.clindermatol.2025.02.005
2. Papaoikonomou MA, Pavlidis L, Apalla Z, Papas A. Conjunctival melanoma: a narrative review of current knowledge. Pigment Cell Melanoma Res. 2025;38(2):e70006. doi:10.1111/pcmr.70006
3. Qi H, Hu L, Huang S, et al. Proton therapy for uveal melanoma on a pencil beam scanning gantry. Adv Radiat Oncol. 2025;10(8):101782. doi:10.1016/j.adro.2025.101782
4. Churchill RA, Yu CY, Wang KY, et al. Clinical features and outcomes of melanoma involving eyelid and conjunctiva. Can J Ophthalmol. 2025. doi:10.1016/j.jcjo.2025.06.020
5. Tolino E, Skroza N, Di Guardo A, Proietti I, Bernardini N, Potenza C. Managing atopic dermatitis with dupilumab in special populations: a case series study. Clin Cosmet Invest Dermatol. 2025;18:2859–2868. doi:10.2147/CCID.S508359
6. Seeburruth D, Sood S, Heung M, Mukovozov I. Characteristics, management, and outcomes of cutaneous malignancies arising from necrobiosis lipoidica: a systematic review. J Cutan Med Surg. 2025;12034754251351637. doi:10.1177/12034754251351637
7. Herron ED, Snyder AM, Hull CM, LoBello S, Herron MD. Shave biopsy with purposeful electrodesiccation benefits small nonmelanoma skin cancer. J Cutan Med Surg. 2025;29(3):317–318. doi:10.1177/12034754241308235
8. Sharma N, Rájová J, Mermelekas G, et al. In-depth patient-specific analysis of tumor heterogeneity in melanoma brain metastasis: insights from spatial transcriptomics and multi-region bulk sequencing. Transl Oncol. 2025;59:102468. doi:10.1016/j.tranon.2025.102468
9. Thet Z, Lam AK, Ng SK, et al. Comparison of skin cancer risk between renal transplant recipients and patients with glomerular diseases in rural Queensland. Aust J Rural Health. 2024;32(2):249–262. doi:10.1111/ajr.13081
10. Cao C, Ju W, Li LQ, et al. Prox1 is linked to metastasis and poor prognosis by promoting lymphangiogenesis in melanoma. Clin Cosmet Invest Dermatol. 2025;18:2847–2858. doi:10.2147/CCID.S554709
11. Urraro F, Patanè V, Clemente A, et al. Radiological assessment after pancreaticoduodenectomy for a precision approach to managing complications: a narrative review. J Pers Med. 2025;15(6):220. doi:10.3390/jpm15060220
12. Chu LC, Wang ZJ, Kambadakone A, et al. Postoperative surveillance of pancreatic ductal adenocarcinoma (PDAC) recurrence: practice pattern on standardized imaging and reporting from the society of abdominal radiology disease focus panel on PDAC. Abdom Radiol. 2023;48(1):318–339. doi:10.1007/s00261-022-03693-0
13. Daamen LA, van Goor I, Groot VP, et al. Recurrent disease detection after resection of pancreatic ductal adenocarcinoma using a recurrence-focused surveillance strategy (RADAR-PANC): protocol of an international randomized controlled trial according to the Trials within cohorts design. Trials. 2024;25(1):401. doi:10.1186/s13063-024-08223-5
14. Qiu ZQ, Ye SY, Zhang RD, Cao M, Lifestyle WYABS. Physical activity, and skin cancer among outpatient us adults: evidence from NHANES. Clin Cosmet Invest Dermatol. 2025;18:2439–2450. doi:10.2147/CCID.S545546
15. Stekelenburg I, Laeijendecker AE, van Doorn RC, et al. Reconsidering the surgical approach in cutaneous melanoma: does wide local excision after a complete diagnostic excision reduce the risk of recurrence? Eur J Cancer. 2025;220:115366. doi:10.1016/j.ejca.2025.115366
16. Brown CD, Zitelli JA. The prognosis and treatment of true local cutaneous recurrent malignant melanoma. Dermatol Surg. 1995;21(4):285–290. doi:10.1111/j.1524-4725.1995.tb00174.x
17. Drzewiecki KT, Andersson AP. Local melanoma recurrences in the scar after limited surgery for primary tumor. World J Surg. 1995;19(3):346–349. doi:10.1007/BF00299155
18. Yuan F, Huang Z, Zhang E, Yao D, Sun J. Anti-MDA5 positive dermatomyositis overlapping with rheumatoid arthritis: a case report. Clin Cosmet Invest Dermatol. 2025;18:2371–2376. doi:10.2147/CCID.S537273
19. Liu X, Luan W, Fan S, Liu T. Association between poor lifestyle habits and cutaneous melanoma risk: a mendelian randomization study. Clin Cosmet Invest Dermatol. 2025;18:687–697. doi:10.2147/CCID.S506547
20. Wang S, Li W, Wang Z, et al. Emerging and reemerging infectious diseases: global trends and new strategies for their prevention and control. Signal Transduct Target Ther. 2024;9(1):223. doi:10.1038/s41392-024-01917-x
21. Cates JMM, Coffin CM. Neurogenic tumors of soft tissue. Pediatr Dev Pathol. 2012;15(1_suppl):62–107. doi:10.2350/11-03-1003-PB.1
22. Arya S, Nagarkatti DG, Dudhat SB, Nadkarni KS, Joshi MS, Shinde SR. Soft tissue sarcomas: ultrasonographic evaluation of local recurrences. Clin Radiol. 2000;55(3):193–197. doi:10.1053/crad.1999.0343
23. Ferguson PC, Deshmukh N, Abudu A, Carter SR, Tillman RM, Grimer RJ. Change in histological grade in locally recurrent soft tissue sarcomas. Eur J Cancer. 2004;40(15):2237–2242. doi:10.1016/j.ejca.2004.04.022
24. Cui Q, Wang H. Resveratrol in dermatological therapy: a critical review of mechanisms, delivery innovations, and clinical frontiers. Clin Cosmet Invest Dermatol. 2025;18:2229–2242. doi:10.2147/CCID.S543849
25. Martora F, Tommasino N, Battista T, Potestio L, Megna M. Hidradenitis suppurativa cancer risk: a review of the literature. Clin Cosmet Invest Dermatol. 2025;18:617–626. doi:10.2147/CCID.S512373
26. Gupta R, Cooper PO, Chai W, et al. Endothelial βII spectrin deletion exacerbates inflammation and impairs tissue regeneration in ischemic-diabetic skin wound healing. Wound Repair Regener. 2025;33(6):e70103. doi:10.1111/wrr.70103
27. Wu YF, Sheu SY, Cheng NC, Cheng CM. Promising biomarkers for chronic wound healing: a pilot cohort study on wound cytokines and a novel biofilm detection kit for predicting 90-day outcomes. Wound Repair Regener. 2025;33(5):e70100. doi:10.1111/wrr.70100
28. Riaz M, Iqbal MZ, Klar AS, Biedermann T. Immunomodulatory mechanisms of chronic wound healing: translational and clinical relevance. MedComm. 2025;6(11):e70378. doi:10.1002/mco2.70378
29. de AraújoBoleti AP, Jacobowski AC, Frihling BEF, et al. Wound healing: molecular mechanisms, antimicrobial peptides, and emerging technologies in regenerative medicine. Pharmaceuticals. 2025;18(10):1525.
30. Yang H, Yang J, Zheng H, et al. Multi-omics integration with machine learning and molecular docking reveals crosstalk mechanisms and drug candidates in metastatic melanoma and vitiligo. Clin Cosmet Invest Dermatol. 2025;18:2047–2066. doi:10.2147/CCID.S533281
31. Peirano D, Donoso F, Vargas S, et al. Patterns of recurrence of cutaneous melanoma: a literature review. Dermatol Pract Concept. 2023;13(4):e2023304.
32. Helvind NM, Brinch-møller weitemeyer M, Chakera AH, et al. Stage-specific risk of recurrence and death from melanoma in Denmark, 2008–2021: a national observational cohort study of 25 720 patients with stage IA to IV melanoma. JAMA dermatol. 2023;159(11):1213–1222. doi:10.1001/jamadermatol.2023.3256
33. Von schuckmann LA, Hughes MCB, Ghiasvand R, et al. Risk of melanoma recurrence after diagnosis of a high-risk primary tumor. JAMA Dermatol. 2019;155(6):688–693. doi:10.1001/jamadermatol.2019.0440
34. Sarac E, Wilhelmi J, Thomas I, et al. Late recurrence of melanoma after 10 years – is the course of the disease different from early recurrences? J Eur Acad Dermatol Venereol. 2020;34(5):977–983. doi:10.1111/jdv.16106
35. Taleb E, Yélamos O, Ardigo M, Christensen RE, Geller S. Non-invasive Skin Imaging in Cutaneous Lymphomas. Am J Clin Dermatol. 2024;25(1):79–89. doi:10.1007/s40257-023-00824-1
36. Taleb E, Yélamos O, Ardigo M, Christensen RE, Geller S. Non-invasive skin imaging in cutaneous lymphomas. Am J Clin Dermatol. 2023;25(1):79–89.
37. Goceri E. Evaluation of denoising techniques to remove speckle and Gaussian noise from dermoscopy images. Comput Biol Med. 2023;152:106474. doi:10.1016/j.compbiomed.2022.106474
38. Bozsányi S, Boostani M, Farkas K, et al. Optically guided high-frequency ultrasound to differentiate high-risk basal cell carcinoma subtypes: a single-centre prospective study. J Clin Med. 2023;12(21):6910. doi:10.3390/jcm12216910
39. Argalia G, Reginelli A, Molinelli E, et al. High-frequency and ultra-high-frequency ultrasound in dermatologic diseases and aesthetic medicine. Medicina. 2025;61(2):220. doi:10.3390/medicina61020220
40. Russo A, Patanè V, Nardone V, et al. Anatomical evaluation of gingival tissues using ultra-high-frequency ultrasound: a preliminary study. Periodont Implant Res. 2025;9(1):13. doi:10.1007/s41894-025-00157-8
41. Wang YX, Cui XM, Zhang Q, et al. Pigmented extramammary paget’s disease of the axilla: two case reports and a literature review. Clin Cosmet Invest Dermatol. 2025;18:1909–1915. doi:10.2147/CCID.S535004
42. Russo A, Marinelli L, Patanè V, et al. Whole-body magnetic resonance imaging for cutaneous melanoma staging: a scientific review. World J Clin Oncol. 2025;16(8):109206. doi:10.5306/wjco.v16.i8.109206
43. Russo A, Patanè V, Fusco L, et al. Reliability of ultrasonographic assessment of depth of invasion and tumor thickness in intraoral mucosa lesions: a preliminary experience. J Clin Med. 2024;13(9):2595. doi:10.3390/jcm13092595
44. Russo A, Patanè V, Gagliardi F, et al. Preliminary experience in ultra-high frequency ultrasound assessment of cutaneous primary lymphomas: an innovative classification. Cancers. 2024;16(13):2456. doi:10.3390/cancers16132456
45. Reginelli A, Russo A, Berritto D, Patane V, Cantisani C, Grassi R. Ultra-high-frequency ultrasound: a modern diagnostic technique for studying melanoma. Ultraschall der Medizin. 2023;44(4):360–378. doi:10.1055/a-2028-6182
46. Jin R, Lu J, Cheng S, Shi S. Differential causal associations of chronic gastritis and ulcerative colitis with melanoma risk: a mendelian randomization study using large-sample GWAS data. Clin Cosmet Invest Dermatol. 2025;18:1551–1563. doi:10.2147/CCID.S525937
47. Wang Q, Ren W, Wang L, et al. Role of high-frequency ultrasound in differentiating benign and malignant skin lesions: potential and limitations. Ultrasonography. 2024;43(4):238–249. doi:10.14366/usg.24015
48. Sellyn GE, Lopez AA, Ghosh S, et al. High-frequency ultrasound accuracy in preoperative cutaneous melanoma assessment: a meta-analysis. J Eur Acad Dermatol Venereol. 2024;39(1):86–96. doi:10.1111/jdv.20179
49. Niu Y, Shi S, Chen Y, Yang S, Yan P, Kou J. Association between serum uric acid levels and skin cancer: results from NHANES data and mendelian randomization analysis. Clin Cosmet Invest Dermatol. 2025;18:1437–1452. doi:10.2147/CCID.S517389
50. Li X, Yang S, Du Z, et al. Cathepsins and skin cancer (Malignant Melanoma, Basal Cell Carcinoma, and Squamous Cell Carcinoma): insight from genetic correlation and mendelian randomization. Clin Cosmet Invest Dermatol. 2025;18:553–566. doi:10.2147/CCID.S502013
51. Belfiore MP, Reginelli A, Russo A, et al. Usefulness of high-frequency ultrasonography in the diagnosis of melanoma: mini review. Front Oncol. 2021;11:673026. doi:10.3389/fonc.2021.673026
52. Zhu AQ, Wang Q, Shi YL, et al. A deep learning fusion network trained with clinical and high-frequency ultrasound images in the multi-classification of skin diseases in comparison with dermatologists: a prospective and multicenter study. EClinicalMedicine. 2024;67:102391. doi:10.1016/j.eclinm.2023.102391
53. Chauvel-Picard J, Tognetti L, Cinotti E, et al. Role of ultra-high-frequency ultrasound in the diagnosis and management of basal cell carcinoma: pilot study based on 117 cases. Clin Exp Dermatol. 2023;48(5):468–475. doi:10.1093/ced/llad001
54. Dini V, Iannone M, Michelucci A, et al. Ultra-High Frequency UltraSound (UHFUS) assessment of barrier function in moderate-to-severe atopic dermatitis during dupilumab treatment. Diagnostics. 2023;13(17):2721. doi:10.3390/diagnostics13172721
55. Papulino C, Crepaldi M, Favale G, et al. “Aging and epigenetic implications in radiotherapy: the promise of BNCT”. Ageing Res Rev. 2025;110:102786. doi:10.1016/j.arr.2025.102786
56. Fulvio G, Izzetti R, Aringhieri G, et al. UHFUS: a valuable tool in evaluating exocrine gland abnormalities in sjögren’s disease. Diagnostics. 2023;13(17):2771. doi:10.3390/diagnostics13172771
57. Li X, Wu S, Pan Y, et al. Causal association between skin microbiota and malignant melanoma: genetic insights from mendelian randomization. Clin Cosmet Invest Dermatol. 2025;18:303–310. doi:10.2147/CCID.S500172
58. Wortsman X. Why, how, and when to use color Doppler ultrasound for improving precision in the diagnosis, assessment of severity and activity in morphea. J Scleroderma Relat Disord. 2019;4(1):28–34. doi:10.1177/2397198318799244
59. Wortsman X. Ultrasound in skin cancer: why, how, and when to use it? Cancers. 2024;16(19):3301. doi:10.3390/cancers16193301
60. Catalano O, Crisan D, Díaz CPG, Cavallieri F, Varelli C, Wortsman X. Ultrasound assessment of skin tumors local recurrence. J Ultrasound Med. 2023;42(10):2439–2446. doi:10.1002/jum.16255
61. Johnston L, Starkey S, Mukovozov I, Robertson L, Petrella T, Alhusayen R. Surveillance after a previous cutaneous melanoma diagnosis: a scoping review of melanoma follow-up guidelines. J Cutan Med Surg. 2023;27(5):516–525. doi:10.1177/12034754231188434
62. Reginelli A, Patanè V, Urraro F, et al. Magnetic resonance imaging evaluation of bone metastases treated with radiotherapy in palliative intent: a multicenter prospective study on clinical and instrumental evaluation assessment concordance (MARTE Study). Diagnostics. 2023;13(14):2334. doi:10.3390/diagnostics13142334
63. Committee EG, Amaral T, Ottaviano M, et al. Cutaneous melanoma: ESMO clinical practice guideline for diagnosis, treatment and follow-up☆. Ann Oncol. 2025;36(1):10–30. doi:10.1016/j.annonc.2024.11.006
64. On behalf of the European Association of D-O, the European Dermatology F, and the European Organization for R, et al. European consensus-based interdisciplinary guideline for melanoma. Part 1: diagnostics - update 2024. Eur J Cancer. 215;2025.
65. Farooq MS, Mattfeld V, Beniwal PC, et al. Recurrence patterns and survival outcomes in clinical stage IIB/IIC melanoma: can we stratify patients for consideration of neoadjuvant immunotherapy? Ann Surg Oncol. 2026;33(1):379–388. doi:10.1245/s10434-025-18263-z
66. Effiom D, Aprati T, Karneris A, et al. Real-world outcomes of adjuvant therapy in stage III melanoma and the impact of somatic mutations. Cancer Med. 2025;14(23):e71410. doi:10.1002/cam4.71410
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.