Back to Journals » ClinicoEconomics and Outcomes Research » Volume 8
UK-specific cost-effectiveness of tiotropium + olodaterol fixed-dose combination versus other LAMA + LABA combinations in patients with COPD
Authors Tebboth A, Ternouth A, Gonzalez-Rojas N
Received 5 July 2016
Accepted for publication 30 August 2016
Published 7 November 2016 Volume 2016:8 Pages 667—674
DOI https://doi.org/10.2147/CEOR.S116546
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Video abstract presented by Abigail Tebboth.
Views: 776
Abigail Tebboth,1 Andrew Ternouth,1 Nuria Gonzalez-Rojas2
1Boehringer Ingelheim Ltd., Bracknell, UK; 2Boehringer Ingelheim GmBH, Ingelheim, Germany
Objective: The aim of this study is to assess the cost-effectiveness of other long-acting muscarinic antagonist + long-acting β2 agonist combinations in comparison with Spiolto® Respimat® (tiotropium + olodaterol fixed-dose combination [FDC]) for maintenance treatment to relieve symptoms in adult patients with chronic obstructive pulmonary disease.
Methods: A previously published individual-level Markov model was adapted for the perspective of the UK health care system, in line with recommendations from the National Institute for Health and Care Excellence. Individuals progressed through the model based on their forced expiratory volume in 1 second (FEV1) value at baseline and the post-improvement FEV1 value. Changes in FEV1 were taken from a mixed treatment comparison. Costs were obtained from a published cost-utility analysis of tiotropium in the treatment of chronic obstructive pulmonary disease in the UK. Uncertainty was assessed by deterministic and probabilistic sensitivity analysis.
Results: Duaklir® Genuair® (aclidinium bromide + formoterol fumarate FDC) and the free-dose combination of tiotropium + salmeterol were dominated by tiotropium + olodaterol FDC. The quality-adjusted life years and costs were identical for Ultibro® Breezhaler® (indacaterol + glycopyrronium FDC) and Anoro™ Ellipta® (umeclidinium + vilanterol FDC) compared with tiotropium + olodaterol FDC, resulting in identical incremental cost-effectiveness ratios.
Conclusion: This analysis shows tiotropium + olodaterol FDC to be a cost-effective option for the maintenance treatment of adults with chronic obstructive pulmonary disease in the UK.
Keywords: COPD, economic, cost-effectiveness, tiotropium + olodaterol
Introduction
There are around one million people in the UK with a diagnosis of chronic obstructive pulmonary disease (COPD), although it is estimated that a further 2 million are undiagnosed.1 COPD is associated with a considerable clinical burden, with symptoms such as chronic cough and persistent dyspnea, exacerbations, and comorbidities contributing to the burden of disease.2–4 COPD is also associated with a considerable economic burden, with direct costs to the NHS of £800 million per year.5
In the UK, treatment of COPD is based on bronchodilators, including short- and long-acting agents.3,6 Guidelines from the National Institute for Health and Care Excellence (NICE) recommend using short-acting bronchodilators as first-line therapy, followed by either long-acting β2 agonists (LABAs) or long-acting muscarinic antagonists (LAMAs).6 Combination therapy with either LABA + inhaled corticosteroid or LAMA + LABA is recommended if patients have forced expiratory volume in 1 second (FEV1) <50% predicted, or an FEV1 ≥50% predicted with remaining breathlessness or exacerbations despite LABA treatment.
Tiotropium + olodaterol fixed-dose combination (FDC) is available in the UK and is accepted by the Scottish Medicines Consortium for maintenance treatment to relieve symptoms in patients with COPD. A number of other LAMA + LABA combinations are also used, including Ultibro® Breezhaler® (indacaterol + glycopyrronium FDC), Anoro™ Ellipta® (umeclidinium + vilanterol FDC), Duaklir® Genuair® (aclidinium bromide + formoterol fumarate FDC), and a free-dose combination of tiotropium + salmeterol. Since these therapies form a routine part of maintenance treatment for COPD, it is important to understand their relative cost-effectiveness. Several economic evaluations have been published on the subject, including evaluations of combination bronchodilator treatment.7,8 Recently, Selya-Hammer et al reported the structure and design of a model to evaluate tiotropium + olodaterol FDC versus tiotropium in the maintenance treatment of adults with COPD.9 This article presents a country-specific adaptation of this model, with results of an analysis of LAMA + LABA combination treatments in comparison with tiotropium + olodaterol FDC from a UK payer perspective. In doing this, the authors aim to validate the suitability of the model structure for use in the UK, which has some differences in health care decision making compared with Italy, the country reported in the initial publication. The authors also aim to inform UK-specific health care decisions on maintenance treatments in COPD, a chronic condition with considerable clinical and economic impact. This may also be of interest to other global health economies with a similar focus on health technology appraisal and cost-effectiveness.
Materials and methods
An individual-level Markov model was developed assessing the cost-effectiveness of four combination maintenance treatments for COPD in comparison with tiotropium + olodaterol FDC, based on the patient-level characteristics from the TONADO trials.10 Individual patients progressed through the model based on their lung function, starting with their baseline FEV1 value. Patients then experienced a short-term improvement in lung function following treatment, after which lung function declined at a rate based on that seen in the 4-year UPLIFT trial.11 This decline is based on patients with COPD and is dependent on Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage. COPD severity was assessed as percentage predicted in each 1-month cycle following GOLD classification of airflow limitation. Severity classification was used to inform lung function decline, probability of mortality, utility values, and disease management health care resource use. Monthly moderate and severe exacerbation risks were estimated based on a logistic regression analysis of patient-level data from the tiotropium treatment group in the UPLIFT trial.
The outcomes of each individual patient were then aggregated and compared across treatment groups. Results were considered from the perspective of the National Health Service and personal social services. Costs and health outcomes were evaluated over a 15-year time horizon, which can be considered to effectively represent lifetime given the mean age of 66 years in the TONADO trials10 and the high probability of mortality in COPD patients compared with the general population.12,13
The structure and design of this model have been previously reported in Therapeutic Advances in Respiratory Disease,9 including the classification of patients, clinical inputs (lung function, risk of exacerbation, and health state utility values), and how they were estimated. However, some modifications were necessary to present the results from a UK perspective. First, the previous publication describes the cost-effectiveness of tiotropium + olodaterol FDC versus tiotropium, whereas this analysis compares other LAMA + LABA combinations with tiotropium + olodaterol FDC. The initial short-term (treatment-related) improvements in lung function were therefore estimated from mean trough FEV1 responses at 2 weeks relative to tiotropium + olodaterol FDC, and were taken from a mixed treatment comparison (MTC)14 rather than from the TONADO trials. These estimates are available in Table S1. Only statistically significant differences from the MTC were considered in the model; non-statistically significant differences were treated as showing no difference. After 2 weeks, the long-term lung function decline was applied as previously reported.
Utility values were estimated by GOLD stage for patients who had not experienced an exacerbation, based on data from the published literature15 (Table S2). Further utility decrements were then applied for patients who experienced severe or moderate exacerbations (values also reported in Table S2). Exacerbations were defined as an increase or new onset of more than one respiratory symptom (cough, sputum, sputum purulence, wheezing, or dyspnea) lasting for at least 3 days and requiring treatment with an antibiotic, systemic steroid, or both.16 Severe exacerbations were those that resulted in hospital admission. COPD-related mortality was estimated from TIOSPIR16 study data and mortality statistics from the UK Office of National Statistics.
UK-specific costs and resource use data were used in the model to inform the routine cost of management of COPD in the UK. These were obtained from a published cost-utility analysis by Hettle et al15 and are available in Table S3. The costs of LAMA + LABA combinations licensed in the UK (Table S3) were taken from the Monthly Index of Medical Specialties Online. Costs and outcomes were discounted by 3.5%, in line with NICE guidance. Institutional ethical review was not sought as all data were used in anonymized form from previous clinical studies. These were performed in accordance with the Declaration of Helsinki, ICH Harmonised Tripartite Guideline: Guideline for Good Clinical Practice and local regulations. The protocols were approved by the authorities and the ethics committees of the respective institutions, and signed informed consent was obtained from all patients.
Validity of the model
The main model was validated by the Institute for Medical Technology Assessment at Erasmus University, Rotterdam.9
Sensitivity analysis
Uncertainty in the model was assessed using deterministic sensitivity analyses. The variables tested in these analyses are listed below. When confidence intervals were not specified, inputs relating to costs and utilities were modified by ±15%.
- Standard mortality ratio
- Two-week relative improvement in FEV1 relative to tiotropium + olodaterol FDC
- Annual decline in lung function based on a single linear rate (ie, not varying by GOLD stage)
- Fifty-two-week probability of severe and moderate exacerbation, based on estimates from the UPLIFT trial
- Moderate and severe exacerbation risk equation
- Cost of routine COPD management and costs of severe and moderate COPD exacerbation
- Health state utility values and decrements following severe and moderate exacerbations
- Discount rate (0% to 5%)
- Time horizon
The deterministic sensitivity analysis was restricted to aclidinium bromide + formoterol fumarate FDC and tiotropium + salmeterol. This was to maintain consistency with the base case analysis, which assumed that indacaterol + glycopyrronium FDC and umeclidinium + vilanterol FDC had identical quality-adjusted life-years (QALYs) to tiotropium + olodaterol FDC, based on the non-statistically significant differences in treatment effect in the MTC.
The impact of parameter uncertainty was also tested using probabilistic sensitivity analyses; again, analyses were restricted to aclidinium bromide + formoterol fumarate FDC and tiotropium + salmeterol for consistency with the base case analysis. Lung function decline and utility values were varied based on beta distributions; standard mortality ratios were based on lognormal distributions and costs were based on gamma distributions. Exacerbation risks varied based on normal distributions.
Results
The results of the base case analysis indicate that aclidinium bromide + formoterol fumarate FDC is associated with lower increases in quality of life (measured in QALYs) compared with tiotropium + olodaterol FDC, as well as higher costs (Table 1). As a result, aclidinium bromide + formoterol fumarate FDC is dominated by tiotropium + olodaterol FDC. Indacaterol + glycopyrronium FDC and umeclidinium + vilanterol FDC are associated with identical QALYs and costs compared with tiotropium + olodaterol FDC, resulting in identical incremental cost-effectiveness ratios. The free-dose combination of tiotropium + salmeterol is associated with the same QALYs as tiotropium + olodaterol FDC but with higher costs, and is thus dominated by tiotropium + olodaterol FDC.
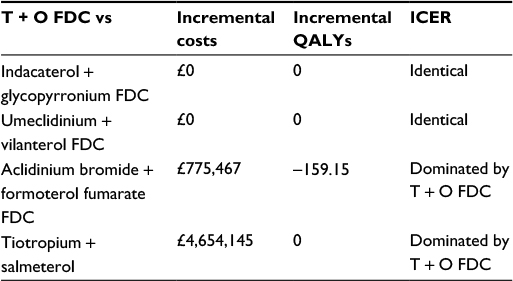 | Table 1 Fifteen-year results – incremental costs and QALYs (discounted) Note: Results are based on 1,029 simulated patients. Abbreviations: FDC, fixed-dose combination; ICER, incremental cost-effectiveness ratio; QALYs, quality-adjusted life-years; T + O, tiotropium + olodaterol. |
Overall, the deterministic analysis found that the estimates from the base case did not significantly change when inputs related to costs or utilities were varied (Table 2). The most sensitive parameters were the treatment-specific short-term FEV1 improvements, as estimated in the MTC: when the 95% confidence intervals included both a positive and negative improvement relative to tiotropium + olodaterol FDC, treatments switched from being dominated to dominating. For example, this is the case for the comparison with tiotropium + salmeterol.
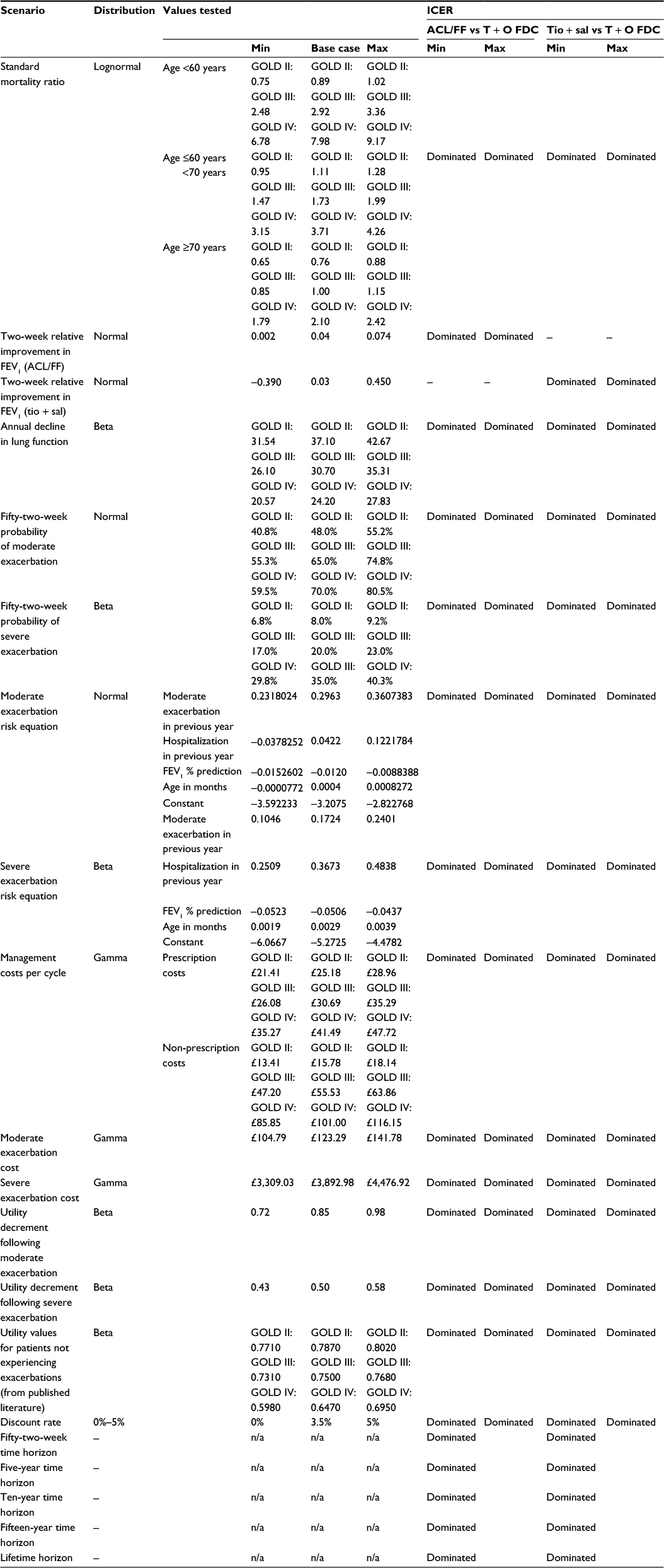 | Table 2 Deterministic sensitivity analysis results Note: Dominated means dominated by T + O FDC. Abbreviations: ACL/FF, aclidinium bromide + formoterol fumarate; FDC, fixed-dose combination; FEV1, forced expiratory volume in 1 second; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICER, incremental cost-effectiveness ratio; Max, maximum; Min, minimum; n/a, not applicable; T + O, tiotropium + olodaterol; tio + sal, tiotropium + salmeterol. |
Probabilistic sensitivity analyses showed that tiotropium + olodaterol FDC was the most cost-effective treatment in 96.5% of simulations at both thresholds of £20,000 and £30,000 per QALYs (Figure 1). In both cases, 200 simulations were run. The probabilistic sensitivity analyses scatterplot can be seen in Figure 2.
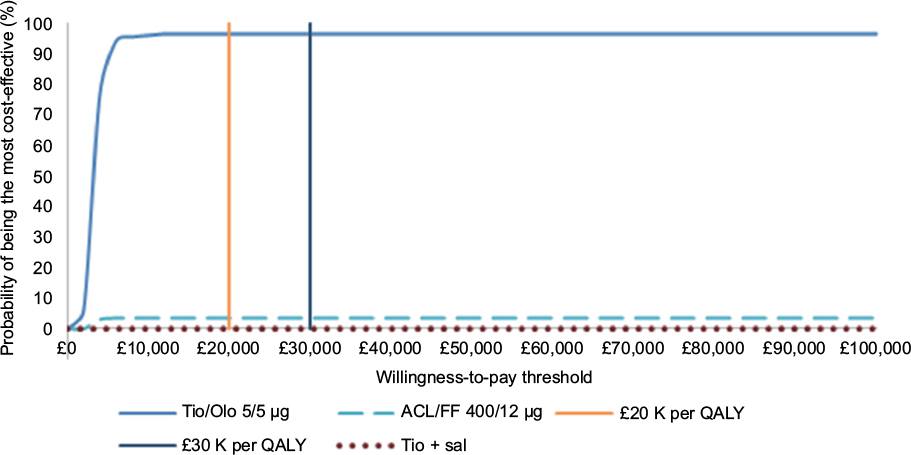 | Figure 1 Cost-effectiveness acceptability curve. Abbreviations: ACL/FF, aclidinium bromide + formoterol fumarate; Tio/Olo, tiotropium + olodaterol; QALY, quality-adjusted life-year; Tio + sal, tiotropium + salmeterol. |
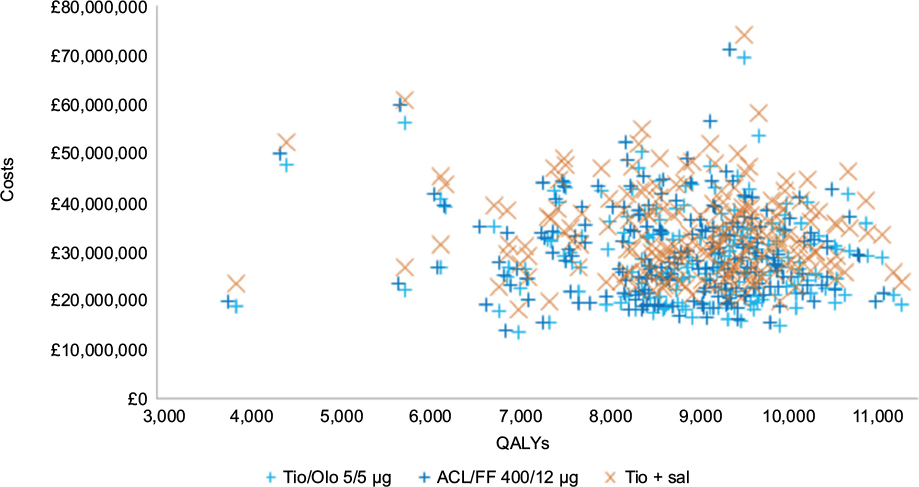 | Figure 2 Probabilistic sensitivity analysis scatterplot. Abbreviations: ACL/FF, aclidinium bromide + formoterol fumarate; QALYs, quality-adjusted life-years; Tio/Olo, tiotropium + olodaterol; Tio + sal, tiotropium + salmeterol. |
Discussion
LAMA + LABA combination therapy is recommended for maintenance treatment of COPD3,6 and has been shown to significantly increase patients’ lung function.3 In the TONADO trials, tiotropium + olodaterol FDC was shown to improve lung function and quality of life and reduce dyspnea compared with the monotherapy components.10 In this analysis, the authors wanted to demonstrate the cost-effectiveness of tiotropium + olodaterol FDC, by comparing other LAMA + LABA combinations available in the UK with this therapy. This analysis suggests that tiotropium + olodaterol FDC is a cost-effective treatment option, dominating aclidinium bromide + formoterol fumarate FDC and tiotropium + salmeterol. Costs and QALYs were identical to the two remaining FDCs, indacaterol + glycopyrronium and umeclidinium + vilanterol. The model was based on a previously reported model, but with adaptations to address a UK payer perspective, and was conducted in line with NICE guidelines for economic analysis.
The results were driven by the relative short-term lung function benefit observed in the MTC, with tiotropium + olodaterol FDC dominating less effective treatments. Varying the other clinical and cost parameters, including health state utility values and utility values following exacerbations, 52-week probability of exacerbations (severe and moderate), relative mortality risk, discount rates, and cost of routine COPD management and exacerbations did not significantly impact on the cost-effectiveness. Similarly, the model was relatively insensitive to differences in the rate of lung function decline following treatment. This highlights the importance of the initial treatment-related improvement in lung function in the model, given the similarity of prices among treatments.
As reported previously, the individualized approach allowed us to more closely estimate the costs and benefits from COPD bronchodilator treatment compared with a more traditional cohort-based Markov model.9 However, the same limitations are also present, such as the exclusion of the impact of adherence on clinical outcomes, the uncertainty around progression of disease beyond the period of the UPLIFT trial, and using GOLD stage and lung function as the only driver for quality of life. However, these are unlikely to affect the direction of the results or interpretation of the model, as there is no indication that the LAMA + LABA combinations are different enough in these aspects to lead to relative changes.
An additional aim of this work was to validate the suitability of the model structure for use in the UK. The main model was first tested in an Italian setting, which has some differences in comparison with the UK. These include variation in the management of COPD as a result of different guidelines and differing recommended methods for assessing cost-effectiveness. Different comparisons to those presented in the previous analysis in order to better reflect NICE guidelines for COPD were included. The results presented here show that the model structure is applicable to the UK, and can be used to provide evidence on the relative cost-effectiveness of LAMA + LABA combinations.
Conclusion
Given the similar acquisition costs of most LAMA + LABA combination therapies in the UK, lung function improvement during treatment is the most important driver of cost-effectiveness. Since tiotropium + olodaterol FDC shows comparable or better improvements in lung function versus other LAMA + LABA combinations, this analysis suggests that it is a cost-effective treatment option for the maintenance of adult patients with COPD from the perspective of the UK health care system.
Acknowledgments
The authors acknowledge Carl Selya-Hammer of Amaris, UK, and James Clark-Wright of Boehringer Ingelheim, UK, for development of the economic model. This work was sponsored by Boehringer Ingelheim Ltd.
Disclosure
A Tebboth, A Ternouth and N Gonzalez-Rojas are employees of Boehringer Ingelheim Ltd., who sponsored the study.
References
NHS Inform. Chronic obstructive pulmonary disease; 2013. Available from: http://www.nhsinform.co.uk/health-library/articles/c/chronic-obstructive-pulmonary-disease/introduction/. Accessed October, 2015. | ||
Schneider C, Bothner U, Jick SS, Meier CR. Chronic obstructive pulmonary disease and the risk of cardiovascular diseases. Eur J Epidemiol. 2010;25(4):253–260. | ||
Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2016. Available from: http://goldcopd.org/. Accessed September 2016. | ||
Rodríguez LA, Wallander MA, Martín-Merino E, Johansson S. Heart failure, myocardial infarction, lung cancer and death in COPD patients: a UK primary care study. Respir Med. 2010;104(11):1691–1699. | ||
NICE. Chronic obstructive pulmonary disease: costing report; 2011. Available from: https://www.nice.org.uk/guidance/cg101/resources/cg101-chronic-obstructive-pulmonary-disease-update-costing-report2. Accessed September 1, 2016. | ||
NICE. NICE guideline CG101: chronic obstructive pulmonary disease in over 16s: diagnosis and management; 2010. Available from: https://www.nice.org.uk/guidance/cg101. Accessed September 1, 2016. | ||
Hertel N, Kotchie RW, Samyshkin Y, Radford M, Humphreys S, Jameson K. Cost-effectiveness of available treatment options for patients suffering from severe COPD in the UK: a fully incremental analysis. Int J Chron Obstruct Pulmon Dis. 2012;7:183–199. | ||
Najafzadeh M, Marra CA, Sadatsafavi M, et al. Cost effectiveness of therapy with combinations of long acting bronchodilators and inhaled steroids for treatment of COPD. Thorax. 2008;63(11):962–967. | ||
Selya-Hammer C, Gonzalez-Rojas Guix N, Baldwin M, et al. Development of an enhanced health-economic model and cost-effectiveness analysis of tiotropium + olodaterol Respimat® fixed-dose combination for chronic obstructive pulmonary disease patients in Italy. Ther Adv Respir Dis. 2016. | ||
Buhl R, Maltais F, Abrahams R, et al. Tiotropium and olodaterol fixed-dose combination versus mono-components in COPD (GOLD 2–4). Eur Respir J. 2015;45(4):969–979. | ||
Tashkin DP, Celli B, Senn S, et al. UPLIFT Study Investigators. A 4-Year Trial of Tiotropium in Chronic Obstructive Pulmonary Disease. N Engl J Med. 2008;359(15):1543–1554. | ||
Office for National Statistics. UK Interim Life Tables, 1980–82 to 2008–10. Available from: http://webarchive.nationalarchives.gov.uk/20160105160709/ http://www.ons.gov.uk/ons/rel/lifetables/interim-life-tables/2008-2010/sum-ilt-2008-10.html. Accessed September 2016. | ||
Wise RA, Anzueto A, Cotton D, et al. Tiotropium respimat inhaler and the risk of death in COPD. N Engl J Med. 2013;369(16):1491–1501. | ||
Schlueter M, Gonzalez-Rojas N, Baldwin M, Groenke L, Voss F, Reason T. Comparative efficacy of fixed-dose combinations of long-acting muscarinic antagonists and long-acting β2-agonists: a systematic review and network meta-analysis. Ther Adv Respir Dis. 2016;10(2): | ||
Hettle R, Wouters H, Ayres J, et al. Cost-utility analysis of tiotropium versus usual care in patients with COPD in the UK and Belgium. Respir Med. 2012;106(12):1722–1733. | ||
Decramer M, Celli B, Kesten S, Lystig T, Mehra S, Tashkin DP; UPLIFT investigators. Effect of tiotropium on outcomes in patients with moderate chronic obstructive pulmonary disease (UPLIFT): a prespecified subgroup analysis of a randomised controlled trial. Lancet. 2009;374(9696):1171–1178. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.