Back to Journals » Clinical Ophthalmology » Volume 20
Two-Year Real-World Outcomes of Faricimab in Treatment-Resistant Neovascular Age-Related Macular Degeneration
Authors Ahmed E ![]() , Goodchild C
, Goodchild C ![]() , Bisoukis A, Salvatore S
, Bisoukis A, Salvatore S
Received 21 February 2026
Accepted for publication 13 April 2026
Published 9 June 2026 Volume 2026:20 596406
DOI https://doi.org/10.2147/OPTH.S596406
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Eslam Ahmed,1 Christine Goodchild,2 Anastasios Bisoukis,1 Serena Salvatore1
1Department of Ophthalmology, University Hospitals of Bristol and Weston NHS Foundation Trust, Bristol, UK; 2Department of Ophthalmology, St Vincent’s University Hospital and Hermitage Medical Clinic, Dublin, Ireland
Correspondence: Christine Goodchild, Email [email protected]
Objective: To evaluate long-term visual and anatomical outcomes of faricimab (Vabysmo®) in patients with neovascular age-related macular degeneration (nAMD) showing suboptimal response to aflibercept 2mg (Eylea®) in a real-world setting.
Methods: This retrospective cohort study evaluated 152 eyes from 126 patients switched to faricimab. All received four loading doses, then a treat-and-extend regimen with ≥ 20-month follow-up. Primary outcomes were changes in non-refracted best-recorded visual acuity (BRVA) and central subfield thickness (CST). Secondary outcomes: fluid status, treatment interval, and safety.
Results: Baseline mean BRVA was 69.91 ± 13 letters, maintained at year 2 (65.9 ± 17.1, p = 0.622). CST decreased from 301.5 ± 86.9 μm at baseline to 222.2 ± 49.2 μm at year 2 (p < 0.001). Complete fluid resolution rose from 12.5% at baseline to 50.7% and 49.3% in years 1 and 2 respectively. Subretinal fluid decreased from 79% to 34% (p < 0.001), while intraretinal fluid improved post-loading (30% to 18%, p=0.005) but remained detectable in 25.7% by year 2 (p=0.36). Treatment intervals were extended from 5.8 ± 1.4 weeks to 9.7 ± 3.1 weeks at year 2 (p < 0.001). By year 2, 18% of eyes achieved ≥ 12-week intervals; 7% achieved ≥ 16-week intervals. No cases of endophthalmitis, vasculitis, or retinal artery occlusion were observed, and ocular adverse events occurred in 3% of eyes.
Conclusion: In treatment-resistant nAMD, switching from aflibercept 2mg to faricimab maintained vision, improved anatomical outcomes, enabled extended treatment intervals, and showed a favorable safety profile over 2 years.
Keywords: neovascular age-related macular degeneration, anti-VEGF resistance, treatment intervals, real-world efficacy, faricimab
Introduction
Neovascular age-related macular degeneration (nAMD) is one of the leading causes of irreversible vision loss in older adults. Although anti-vascular endothelial growth factor (anti-VEGF) therapies have significantly improved outcomes, some patients exhibit a suboptimal response, characterized by persistent or recurrent intraretinal and/or subretinal fluid and/or the necessity for frequent, high-burden injections to control disease activity.1,2 Patients with resistant nAMD often remain dependent on frequent injections3 placing a considerable burden on both the individuals and the healthcare system. The recognition of treatment resistance underscores the need for alternative therapeutic approaches or agents, such as faricimab, which targets additional disease pathways and may offer improved anatomical stability, reduced injection burden, and sustained visual outcomes.
Faricimab is the first bispecific antibody targeting both VEGF-A and Angiopoietin-2 (Ang-2), designed to achieve greater vascular stability and extended treatment durability. Pivotal trials (TENAYA/LUCERNE) demonstrated non-inferior visual outcomes compared to aflibercept 2mg, successfully extending dosing intervals up to 16 weeks for approximately 59% to 66.9% of treatment-naïve patients at two years.4
Although encouraging, these findings may not fully reflect real-world practice. The trials included only treatment-naïve nAMD patients, whereas clinicians often switch those with persistent disease despite anti-VEGF therapy to faricimab to lessen treatment burden. Real-world data, which capture variations in practice and broader patient populations, are therefore essential to confirm the applicability of these results.
Emerging real-world evidence increasingly highlights faricimab’s anatomical benefits in patients who have shown resistance to previous anti-VEGF therapies. Notably, these reports consistently document substantial reductions in central subfield thickness (CST) and retinal fluid, all while preserving visual acuity. Despite these promising indications, the body of long-term data on the sustained efficacy and durability of faricimab in this challenging, pretreated population remains sparse, with most studies limited to follow-up periods of 12 months or less.5–7
Addressing this gap, our study examines faricimab’s efficacy, durability, and safety over an extended 24-month period in eyes with nAMD that exhibited a suboptimal response to aflibercept 2 mg. Building on our earlier publication,7 which focused on initial real-world outcomes post-switch, the present analysis offers a robust assessment of faricimab’s long-term impact. These extended follow-up data provide valuable clinical insights into anatomical stability, visual maintenance, and reduced treatment burden—critical considerations for both patients and clinicians managing treatment-resistant nAMD. Our findings advance the understanding of faricimab’s role, moving beyond short-term observations and contributing important evidence for long-term treatment strategies.
Materials and Methods
Study Design and Participants
A retrospective observational cohort study was conducted at a single tertiary referral center, Bristol Eye Hospital, University Hospitals of Bristol and Weston, United Kingdom (UK). A total of 152 eyes from 126 consecutive patients with nAMD were included. All patients were switched to intravitreal faricimab (Vabysmo®, Roche, 6 mg/0.05 mL intravitreal injection) following a suboptimal response to aflibercept 2 mg (Eylea® 2mg, Bayer). A suboptimal response was defined as patients who have disease activity (persistent/ new intraretinal fluid (IRF) and/or sub-retinal fluid (SRF)) at a treatment interval of 8 weeks or less or, patients who achieve disease control at treatment interval of 6 weeks or less.
Patients were eligible for inclusion in this study when they had received 4 loading doses of faricimab and had a minimum of 20 months of follow-up.
Exclusion criteria included: treatment-naïve nAMD or other retinal diseases, incomplete medical records, and inadequate follow-up duration.
Treatment Protocol
After four loading doses of faricimab at monthly intervals, patients were reviewed 8 weeks after the fourth loading dose. At this point, the patient’s treatment interval was individualised based on the disease activity using a treat-and-extend pathway. Treatment intervals were lengthened or shortened in 2–4-week steps (to a minimum of 4-week interval) based on retinal fluid status (see below). All injections were performed under aseptic conditions using standard protocols.
Assessments
At every visit, patients would undergo non-refracted Early Treatment of Diabetic Retinopathy Study (ETDRS) best-recorded visual acuity (BRVA) testing, slit-lamp biomicroscopy, dilated fundus examination, and spectral-domain optical coherence tomography (OCT) [Topcon, 3D OCT-1 Maestro2, 2019]. Retinal fluid, including intraretinal (IRF) and subretinal (SRF) fluid, was assessed on OCT scans. Grading of IRF and SRF was performed by the treating physicians in accordance with established clinical practice, using standardized OCT interpretation criteria to ensure consistency across assessments. Information collected included demographics, frequency and number of previous anti-VEGF treatments, adverse events, BRVA, central subfield thickness (CST), presence of intraretinal (IRF) and/or subretinal (SRF) fluid. CST was measured from Bruch’s membrane to the inner limiting membrane (ILM) to account for pigment epithelial detachments (PED). Complete fluid resolution was defined as absence of both IRF and SRF. Pre-switch treatment interval was calculated as the average of the patient’s past 3 treatment intervals immediately before the treatment switch. Both eyes from the same patient were eligible for inclusion if they met the study criteria. The potential non-independence of observations arising from this was addressed in the statistical analysis using mixed-effects modelling.
Treat-and-Extend Criteria
Treatment intervals were adjusted according to functional and anatomical markers of disease activity, based on BRVA and OCT findings. Treatment intervals were extended when BRVA was stable (no loss of ≥5 ETDRS letters attributable to disease activity) and OCT demonstrated no intraretinal or subretinal fluid. Extension was also permitted in cases of persistent fluid that remained stable despite shorter treatment intervals, provided there had been no unsuccessful attempt to extend the interval within the preceding 6 months. Treatment intervals were maintained when BRVA remained stable and OCT findings were unchanged. This included eyes with no fluid, stable intraretinal fluid (IRF) or subretinal fluid (SRF), or fluid that had shown no variability despite shorter treatment intervals. Intervals were also maintained where prior extension attempts had resulted in recurrence or worsening of disease activity, limiting confidence to extend further. Treatment intervals were shortened when disease activity was detected, which was defined as a decrease of ≥5 ETDRS letters caused by the disease and/or worsening anatomical features observed on OCT. These included new or increased IRF or SRF, new or increased macular haemorrhage, or new or worsening subretinal hyperreflective material.
Safety
All ocular and systemic adverse events were recorded at each visit and summarized as counts and frequencies.
Statistical Analysis
Statistical analysis was performed using Stata (StataCorp, College Station, TX, USA) [version 15.1]. Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range [IQR]) as appropriate, and categorical variables as counts (percentages).
For continuous outcomes (best-recorded visual acuity [BRVA] and central subfield thickness [CST]), changes across timepoints (baseline, post-loading, year 1, and year 2) were assessed using paired t-tests and analysis of variance (ANOVA), with Tukey post hoc testing for multiple comparisons. Pairwise comparisons were performed between baseline and each follow-up timepoint.
Categorical outcomes, including the presence of intraretinal fluid (IRF) and subretinal fluid (SRF), were analyzed using McNemar’s test to assess changes between baseline and each follow-up timepoint.
Additional longitudinal analyses were performed using mixed-effects models to account for repeated measurements over time and the inclusion of both eyes from some patients. For continuous outcomes (BRVA and CST), linear mixed-effects models were fitted with timepoint as a categorical fixed effect and random intercepts for patient and eye nested within patient. For binary outcomes (IRF and SRF), mixed-effects logistic regression models with the same hierarchical structure were used. Marginal means and pairwise comparisons between time points were estimated from these models.
All statistical tests were two-sided, and a p-value <0.05 was considered statistically significant. No formal sample size or power calculation was performed, as this was a retrospective observational study.
Outcome Measures
The primary outcomes were the changes in BRVA and CST from baseline (time of switch) to the last follow-up. Secondary outcomes included the proportion of eyes with IRF and/or SRF, the maximum treatment interval achieved under the treat-and-extend protocol, and the frequency and nature of ocular or systemic adverse events, including intraocular inflammation and retinal pigment epithelium (RPE) tears.
Results
Study Population
A total of 152 eyes from 126 patients with treatment-resistant neovascular age-related macular degeneration (nAMD) were included. All eyes completed four initial loading injections of faricimab and had at least 20 months of follow-up (mean 22.0 ± 1.78 months; range 20–28). The mean age at baseline was 82.9 ± 7.36 years, and 63.5% of patients were female. The majority (89.9%) self-identified as White.
Before switching, eyes had received a mean of 8.0 ± 1.72 aflibercept 2mg injections in the preceding year. The mean duration of nAMD at the time of switch was 4.08 years (49 ± 36.70 months; range 3–179), during which eyes had undergone a cumulative 33 ± 25.23 intravitreal injections (range 3–137).
Visual Acuity Outcomes
Mean BRVA at baseline was 69.91 ± 12.96 ETDRS letters. Following faricimab loading, vision was maintained (67.71 ± 14.11 letters) and remained stable at year 1 (68.63 ± 13.57; p = 0.973 vs baseline) and year 2 (65.90 ± 17.09; p = 0.622 vs baseline). Despite the chronic, treatment-resistant nature of the cohort, vision was preserved over year 2.
Anatomical Outcomes
Mean CST decreased significantly from 301.45 ± 86.88 µm at baseline to 246.84 ± 76.95 µm after loading (p < 0.001), 235.09 ± 47.86 µm at year 1 (p < 0.001), and 222.18 ± 49.15 µm at year 2 (p < 0.001 vs baseline), demonstrating a sustained anatomical response through year 2.
Complete resolution of IRF and SRF was present in 12.5% of eyes (19/152) at baseline, increasing to 48.7% after loading, 50.7% at year 1, and 49.3% at year 2. Subretinal fluid prevalence declined from 79% (120/152) at baseline to 42% after loading, 39% at year 1, and 34% at year 2 (p < 0.001 for all time points vs baseline). IRF prevalence decreased from 30% (45/152) at baseline to 18% post-loading (p = 0.005) and 18.4% at year 1 (p = 0.011). By year 2, IRF was present in 25.7% of eyes (39/152, p = 0.36). This is illustrated in Table 1.
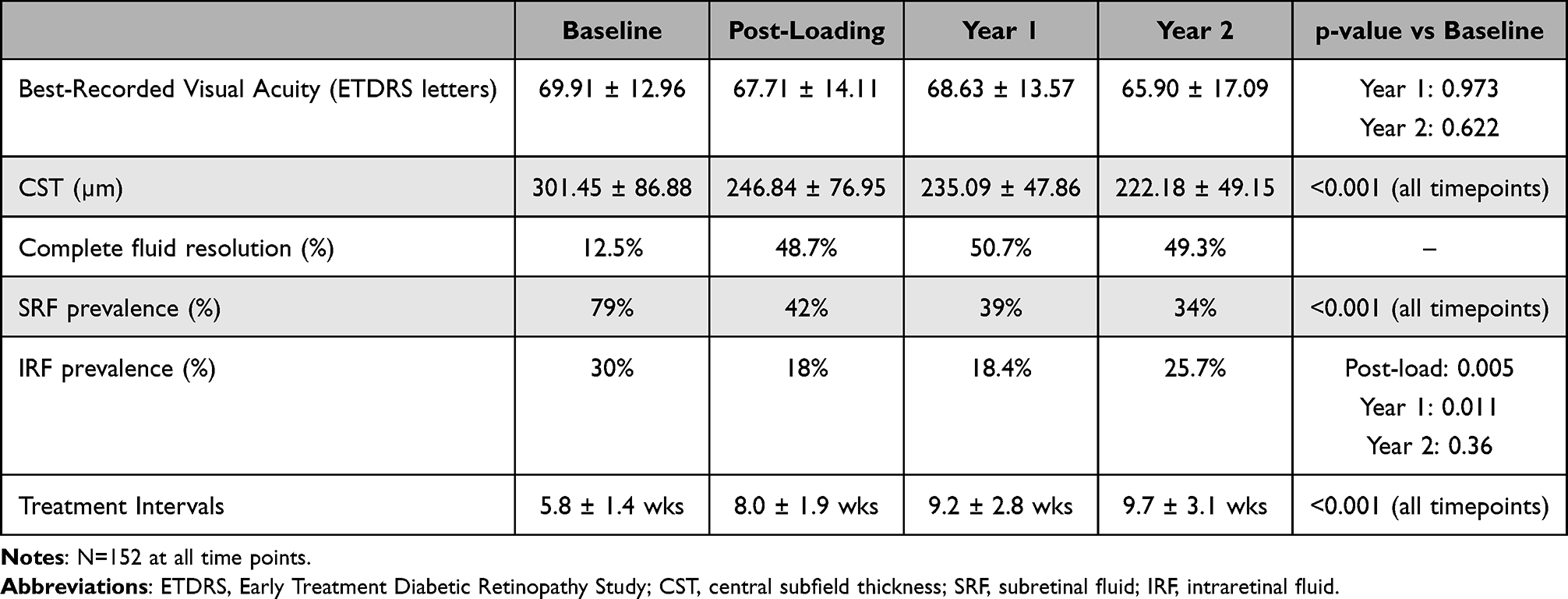 |
Table 1 Two-Year Visual and Anatomical Outcomes with Faricimab |
Additional mixed-effects modelling, accounting for repeated measurements and intra-patient correlation, demonstrated no statistically significant overall change in BRVA over time, although a borderline reduction was observed at year 2 compared with baseline (p = 0.053). In contrast, CST decreased significantly across all post-baseline timepoints (p < 0.001). The proportion of eyes with IRF was significantly reduced following loading and at year 1, whereas SRF was significantly reduced at all post-baseline timepoints (both p < 0.05).
Treatment Exposure
Eyes received a mean of 8.0 ± 0.93 faricimab injections in year 1 (which includes 4 loading doses) and 5.0 ± 1.18 in year 2, for a cumulative mean of 13.43 ± 1.56 injections over 2 years. The number of outpatient visits was also reduced when compared to attendance prior to switching. Patients averaged 8 ± 1.55 reviews in the year before switching to faricimab, which decreased to 5 ± 1.18 (p< 0.001) in the second year. Outpatient appointments were conducted in a one-stop treatment clinic.
Treatment intervals increased significantly from a mean of 5.77 ± 1.42 weeks at baseline to 8.04 ± 1.89 weeks after the loading phase (p < 0.001), 9.24 ± 2.80 weeks at year 1 (p < 0.001 vs baseline), and 9.72 ± 3.07 weeks at year 2 (p < 0.001 vs baseline). At baseline, 31% (n=47) of eyes required 4-weekly dosing; by year 2, this had decreased to 1.3%. Notably, of the original 47 eyes on 4-weekly treatment, 83% (n = 39) were able to extend to intervals of eight weeks or longer by year 2. Extended dosing became increasingly achievable: at year 2, 25% of eyes were maintained at 12-week or longer intervals, including 7% at ≥16-week intervals. See Figure 1.
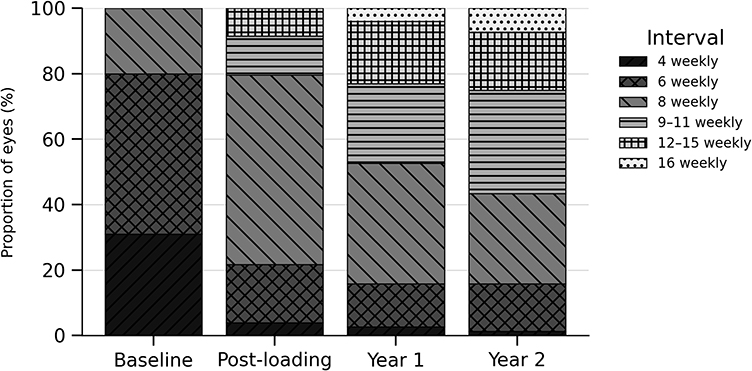 |
Figure 1 Distribution of treatment intervals over time. |
At the two-year time point, 14% of eyes required injections every 6 weeks, 28% every 8 weeks, 32% every 9–11 weeks, 18% every 12 to 15 weeks, and 7% at intervals of 16 weeks or longer. Detailed distributions of treatment intervals over time are illustrated in Figure 1.
Over the two-year period, 4 patients (2.6%) were switched from faricimab to aflibercept 8 mg owing to suboptimal response. Nineteen eyes (19/152, 12.5%) underwent additional ocular procedures, including cataract surgery (n = 12; 63%), minor laser interventions (4 posterior Nd:YAG laser capsulotomies and 2 selective laser trabeculoplasty (n = 6; 31.5%), and retinal bleeding displacement surgery secondary to nAMD (n = 1; 5.2%).
Safety
A total of 2042 injections were given to this cohort of patients. No cases of endophthalmitis, retinal vasculitis, or retinal artery occlusion were observed. Ocular adverse events occurred in four eyes/events (2.6% of patients, 0.2% of events): one RPE tear, one case of anterior chamber inflammation, one retinal detachment, and one new fourth nerve palsy. No systemic adverse events were attributed to faricimab; two patients experienced intercurrent systemic events (limb cellulitis and myocardial infarction), both judged unrelated to treatment. While the overall findings support a favorable safety profile in this cohort, it is important to note that the study was not specifically powered to detect rare adverse events; therefore, the safety outcomes should be interpreted with appropriate caution.
Discussion
In this study, we report the two-year visual and anatomical outcomes for eyes with treatment-resistant neovascular age-related macular degeneration (nAMD) after switching from aflibercept 2mg to faricimab. In a cohort of AMD patients with chronic and refractory disease, the switch to faricimab demonstrated a favourable outcome, primarily demonstrated by a reduction in CST and an extension in treatment interval.
Although mean BRVA showed minor fluctuations over time, mixed-effects modelling demonstrated no statistically significant overall change, with a small borderline reduction observed at year 2. Given the lack of statistical significance, this was considered to represent overall visual stability. Preservation of vision in this heavily pre-treated population is noteworthy, particularly given that the natural history of treatment-resistant nAMD is typically characterized by progressive visual decline due to irreversible photoreceptor damage.8 The literature on this topic reflects a spectrum of outcomes, with reports of visual improvement, stability, and deterioration, likely influenced by varying study criteria and the duration of prior anti-VEGF therapy.5,9 Our findings align with a growing body of real-world evidence demonstrating that switching to faricimab can stabilize vision while improving anatomic markers of disease activity, although the magnitude and durability of these effects may vary. Short-term studies10,11 reported better visual acuity shortly after switching to faricimab in patients with fewer prior injections compared to our cohort, which averaged 33 injections before switching to faricimab. The absence of visual improvement in our study may suggest a “ceiling effect,” consistent with SEVEN-UP’s findings of stable outcomes after long-term therapy.12 Machida et al13 found that roughly one-third of aflibercept-refractory nAMD eyes achieved extended treatment intervals at six months, with baseline characteristics affecting success; however, visual acuity stayed stable, indicating structural improvements do not always lead to functional gains. Our results similarly show stable vision despite anatomical changes. Jones et al14 also reported stable visual acuity with significant CST reduction and modestly extended treatment intervals.14 In our group, interval extensions were more pronounced, likely due to longer follow-up and a higher number of faricimab injections.
Our analysis demonstrated that the most notable benefits of faricimab were observed anatomically. This outcome echoes the observations by Tamiya et al15 however, a key distinction in our approach was the inclusion of a loading dose and a considerably longer follow-up period, providing a more comprehensive perspective.15 CST declined significantly following the treatment switch and continued to improve over two years, indicating a durable therapeutic effect. Fluid resolution rates also increased substantially, with nearly half of the eyes remaining dry at both year 1 and year 2. A consistent pattern was observed in fluid dynamics: SRF prevalence declined steadily, whereas IRF proved more resistant, showing a modest rebound at year 2. These findings are consistent with previous reports linking higher IRF burden to worse visual outcomes and greater ellipsoid zone thinning.16,17
A major advantage of faricimab was its ability to extend dosing intervals, valuable in routine care. Treatment intervals lengthened from around 6 weeks at baseline to almost 10 weeks by year 2, with some patients reaching 16-week intervals. Monthly dosing dropped from nearly one-third to just 1% of eyes by study end, with over 80% of those initially on monthly injections extending to eight weeks or more. Saito et al6 reported similar interval extension, though their cohort was smaller and less diverse.6
Compared to treatment-naïve patients in TENAYA and LUCERNE,4 fewer eyes in our treatment-resistant cohort achieved extended intervals (25% ≥12 weeks vs ~79%), underscoring the chronicity of disease for our cohort as well as real-world relevance versus clinical trial outcomes.
Capacity shortfalls in ophthalmic services threaten the timely delivery of intravitreal injections, a failure that can lead to irreversible vision loss. Studies have shown that treatment interruptions of three months or longer can cause visual declines that are not recovered even after therapy is restarted.18,19 The burden of intensive injection schedules compounded by treatment-related anxiety, fear of injections, and the logistical challenges of frequent clinic attendance weighs heavily on patients and their caregivers. Each appointment can consume hours, a significant commitment for an elderly population often managing other comorbidities. Unsurprisingly, patients consistently prefer treatment protocols that minimize injection frequency without compromising visual outcomes.20
Beyond the patient experience, the real-world non-drug costs associated with high-frequency treatment regimens place an immense strain on healthcare systems. These costs encompass clinic operations, staffing, emergency appointments, diagnostic monitoring, and resources for vision loss management, creating a vicious cycle of financial strain, patient burden, clinical deterioration, and diminished well-being.21 With extended treatment intervals, faricimab reduces the ongoing burden for patients and caregivers, while also improving clinic efficiency and supporting sustainable healthcare.
Throughout our study, faricimab demonstrated a favorable safety profile. These outcomes align with the established safety profile of faricimab in both clinical trial and real-world settings.4,22
Our study is not without limitations. Its retrospective design may introduce selection bias, and the lack of a contemporaneous control group limits direct comparison with ongoing aflibercept treatment. Although follow-up extended to two years, longer-term data are needed to fully establish durability and safety. Furthermore, while visual acuity was successfully maintained, it was not significantly improved in most eyes, reflecting the advanced stage of disease and potential ceiling effects in a cohort that had relatively good vision at baseline.
Conclusion
Switching to faricimab in patients with treatment-resistant nAMD is associated with sustained anatomical improvement, stable visual acuity, and an extension of treatment intervals over a two-year period, all within a favorable safety profile. These findings support the potential of faricimab to lessen treatment burden and improve disease management in a challenging real-world patient group, providing an option to maintain vision, enhance quality of life, and ease clinic capacity pressures.
Abbreviations
Ang-2, Angiopoietin-2; Anti-VEGF, anti-vascular endothelial growth factor; BRVA, best-recorded visual acuity; CST, central subfield thickness; ETDRS, Early Treatment of Diabetic Retinopathy Study; IRF, intraretinal fluid; nAMD, neovascular age-related macular degeneration; OCT, optical coherence tomography; PED, pigment epithelial detachments; RPE, retinal pigment epithelium; SRF, sub-retinal fluid; UK, United Kingdom.
Ethics Approval and Informed Consent
The study adhered to the tenets of the Declaration of Helsinki and received approval by the University Hospitals of Bristol and Weston NHS Foundation Trust clinical audit group (reference MEDRET/CA/2023-24/02). Owing to the retrospective design and use of fully deidentified clinical data, the requirement for individual informed consent was waived.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Serena Salvatore: Advisory board member for Advanz Pharma, Bayer, Alimera Sciences, and Roche; has received speaker honoraria from AbbVie, Alimera Sciences, Bayer, Roche and Sandoz; and travel support from Alimera Sciences, Bayer, and Roche. Christine Goodchild: Travel support from Alimera Sciences, AbbVie, Santen and Roche. Speaker honoraria from Roche and Scope. The authors report no other conflicts of interest in this work.
References
1. Lotery A, Griner R, Ferreira A, et al. Real-world visual acuity outcomes between ranibizumab and aflibercept in treatment of neovascular AMD in a large US data set. Eye. 2017;31(12):1697–8. doi:10.1038/eye.2017.143
2. Amoaku WM, Chakravarthy U, Gale R, et al. Defining response to anti-VEGF therapies in neovascular AMD. Eye (Lond). 2015;29(6):721–731. doi:10.1038/eye.2015.48
3. Leung EH, Oh DJ, Alderson SE, et al. Initial real-world experience with faricimab in treatment-resistant neovascular age-related macular degeneration. Clin Ophthalmol. 2023;17:1287–1293. doi:10.2147/OPTH.S409822
4. Khanani AM, Kotecha A, Chang A, et al. TENAYA and LUCERNE: two-year results from the Phase 3 neovascular age-related macular degeneration trials of faricimab with treat-and-extend dosing in year 2. Ophthalmology. 2024;131(8):914–926. doi:10.1016/j.ophtha.2024.02.014
5. Löw K, Sitnilska V, Tang Y, et al. Real-life treatment intervals and morphological outcomes following the switch to faricimab therapy in neovascular age-related macular degeneration. J Pers Med. 2025;15(5):189. doi:10.3390/jpm15050189
6. Saito M, Imaizumi K. Two-year results of switching to intravitreal administration of faricimab in patients with aflibercept-refractory neovascular age-related macular degeneration. Sci Rep. 2025;15(1):30699. doi:10.1038/s41598-025-15194-3
7. Goodchild C, Bailey C, Soto Hernaez J, Ahmed E, Salvatore S. Real world efficacy and durability of faricimab in patients with neovascular AMD (nAMD) who had sub-optimal response to prior anti-VEGF therapy. Eye. 2024;38(16):3059–3064. doi:10.1038/s41433-024-03218-7
8. Broadhead GK, Hong T, Chang AA. Treating the untreatable patient: current options for the management of treatment-resistant neovascular age-related macular degeneration. Acta Ophthalmol. 2014;92(8):713–723. doi:10.1111/aos.12463
9. Schneider M, Bjerager J, Hodzic-Hadzibegovic D, et al. Short-term outcomes of treatment switch to faricimab in patients with aflibercept-resistant neovascular age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 2024;262:2153–2162. doi:10.1007/s00417-024-06421-0
10. Yufeng X, Ningxi H, Mingzhi S, et al. Real-world outcomes of a loading phase with intravitreal faricimab in refractory Neovascular Age-Related Macular Degeneration (nAMD) patients. BMC Ophthalmol. 2025;25(1):347. doi:10.1186/s12886-025-04212-7
11. Kin A, Mizukami T, Ueno S, Mishima S, Shimomura Y. Short-term comparison of switching to brolucizumab or faricimab from aflibercept in neovascular AMD patients. Medicina. 2024;60(7):1170. doi:10.3390/medicina60071170
12. Bhisitkul RB, Mendes TS, Rofagha S, et al. Macular atrophy progression and 7-year vision outcomes in subjects from the ANCHOR, MARINA, and HORIZON studies: the SEVEN-UP study. Am J Ophthalmol. 2015;159(5):915–24.e2. doi:10.1016/j.ajo.2015.01.032
13. Machida A, Oishi A, Ikeda J, et al. Factors associated with success of switching to faricimab for neovascular age-related macular degeneration refractory to intravitreal aflibercept. Life. 2024;14(4):476. doi:10.3390/life14040476
14. Jones N, Gore C, Saedon H, et al. Efficacy of treatment with faricimab for patients with refractory nAMD. Eur J Ophthalmol. 2025;35(5):1695–1702. doi:10.1177/11206721251328097
15. Tamiya R, Hata M, Tanaka A, et al. Therapeutic effects of faricimab on aflibercept-refractory age-related macular degeneration. Sci Rep. 2023;13(1):21128. doi:10.1038/s41598-023-48190-6
16. Gualino V, Sohier C, Sibert M, et al. Real-world faricimab switch in France: artificial intelligence-based detection of changes in exudative signs in difficult-to-treat neovascular age-related macular degeneration. BMJ Open Ophthalmol. 2025;10(1):e002267. doi:10.1136/bmjophth-2025-002267
17. Patil NS, Mihalache A, Dhoot AS, et al. Association between visual acuity and residual retinal fluid following intravitreal anti–vascular endothelial growth factor treatment for neovascular age-related macular degeneration: a systematic review and meta-analysis. JAMA Ophthalmol. 2022;140(6):611–622. doi:10.1001/jamaophthalmol.2022.1357
18. Gale R, Cox O, Keenan C, et al. Health technology assessment of new retinal treatments; the need to capture healthcare capacity issues. Eye. 2022;36(12):2236–2238. doi:10.1038/s41433-022-02149-5
19. Greenlee TE, Wang VY, Kang H, et al. Consequences of lapses in treatment with vascular endothelial growth factor inhibitors in neovascular age-related macular degeneration in routine clinical practice. Retina. 2021;41(3):581–587. doi:10.1097/IAE.0000000000002888
20. Sivaprasad S, Oyetunde S. Impact of injection therapy on retinal patients with diabetic macular edema or retinal vein occlusion. Clin Ophthalmol. 2016;10:939–946. doi:10.2147/OPTH.S100168
21. Sivaprasad S, Bailey C, Downey L, et al. Real-world service costs for neovascular-AMD clinics in the United Kingdom: structured literature review and scenario analysis. Curr Med Res Opin. 2024;40(7):1221–1233. doi:10.1080/03007995.2024.2362278
22. Khanani AM, Aziz AA, Khan H, et al. The real-world efficacy and safety of faricimab in neovascular age-related macular degeneration: the TRUCKEE study – 6-month results. Eye. 2023;37:3574–3581. doi:10.1038/s41433-023-02553-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.