Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Two Advancement Flaps for Eyelid Margin Reconstruction of Small and Medium Defects and a Novel Design to Reduce Ocular Injury
Authors Dai X ![]() , Ma X, Zhang D
, Ma X, Zhang D ![]() , Zhang D
, Zhang D ![]() , Li J
, Li J ![]() , Xiong Z
, Xiong Z ![]() , Wang B
, Wang B ![]() , Liu G
, Liu G ![]()
Received 2 November 2022
Accepted for publication 23 December 2022
Published 20 January 2023 Volume 2023:16 Pages 173—184
DOI https://doi.org/10.2147/CCID.S394211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Xinyue Dai,1,* Xu Ma,1,* Dongxue Zhang,2 Dapeng Zhang,1 Jiajun Li,1 Zenghui Xiong,3 Bingyu Wang,1 Guofeng Liu1
1Department of Plastic Surgery, the Second Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China; 2Department of Plastic Surgery, Nanjing Maternity and Child Health Care Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 3Department of Plastic Surgery, the Second Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guofeng Liu, Department of Plastic Surgery, the Second Affiliated Hospital of Harbin Medical University, 246 Xuefu Road, Harbin, 150001, People’s Republic of China, Tel +86 15545561122, Email [email protected]
Purpose: The key point of eyelid margin reconstruction is to keep both the support function and aesthetic appearance. The eyelid’s complex anatomical structures make eyelid margin reconstruction demanding. Eyelid margin defects are conventionally classified by their width relative to the eyelid width: small, medium, or large. In this study, we introduce a reconstruction method for small to medium defects.
Patients and Methods: We conducted a single-center case series of patients from the practice of a single experienced plastic surgeon at a tertiary center. We included consecutive outpatients from 2014 to 2021. The inclusion criteria were (1) eyelid margin mass and (2) willingness to receive eyelid margin reconstruction by the reported method. The exclusion criteria were (1) eyelid margin mass involving most or all of the tarsus and (2) less than one year of follow-up. Patients were followed up face to face or online. Patients’ demographics, clinical characteristics and outcomes, and satisfaction were collected. The clinical outcomes were assessed and scored by two plastic surgeons.
Procedure: We reconstructed the anterior lamella with an advancement musculocutaneous flap and repaired the posterior lamella with a specially designed advancement tarsoconjunctival flap, of which a piece of tarsus was shaved and the corresponding remnant conjunctiva was bent forward to cover the tarsus edge to avoid ocular injury.
Results: We included 24 patients (25 lesions). Almost all patients had eyelash discontinuity. One patient presented slight notching of the lower eyelid margin. The other patients reported no complications or recurrence. The average outcome score was 1.23± 0.69, indicating that our method was excellent. All patients were very satisfied with the surgery. The average follow-up time was 5.75 years.
Conclusion: We report a reconstruction method for small to medium eyelid margin defects and a novel design for preventing ocular injury, which is an especially good option for transverse defects.
Keywords: eyelid margin, reconstruction, tarsoconjunctival flap, advancement flap
Introduction
The eyelid is an important facial aesthetic and functional unit. As the most sophisticated structure of the eyelid, the eyelid margin matters greatly. It provides tensional support to make the eyelid cling to the globe. It also lubricates the oculus by secreting meibum that is involved in forming the tear film, distributes tears when blinking, prevents tear overflow, and keeps sebum out of the eye.1,2 In reconstructive surgery, the eyelid is considered a bilamellar structure. The anterior lamella consists of skin, connective tissue, and the orbicularis muscle, and the posterior lamella consists of the tarsus and the palpebral conjunctiva. Besides having the same structure as the eyelid, the eyelid margin has some unique anatomy. Eyelashes emerge from the skin. The gray line is the most superficial portion of the orbicularis muscle, and surgeons usually determine the resection thickness of the lesion based on whether the gray line is invaded. Meibomian gland orifices within the tarsus secrete meibum. The epidermis gradually transitions into the mucosa behind the meibomian gland orifices until the mucocutaneous junction.2 A perfect reconstruction requires suturing each lamella and precisely aligning the eyelash line, gray line, and meibomian gland orifices.
The eyelid is a common site of skin lesions, accounting for 5–10% of all skin tumors because of the multiplicity of tissue and exposure to sunlight. Around 79–84% of eyelid lesions are benign, frequently including nevi, squamous cell papillomas, basal cell papillomas, seborrheic keratoses, and epidermal cysts. Among malignant tumors, basal cell carcinoma is the most common type (around 80%).3–5 Most benign tumor resections leave defects of less than 50% of the eyelid width, whereas malignant tumors always result in larger defects. The classification of eyelid defects is conventionally based on their horizontal width relative to the eyelid width: small defects are less than 25% of the eyelid width, medium defects are 25–50%, and large defects are more than 50%.
In this study, we introduced an alternative eyelid margin reconstruction method for small and medium defects and a novel design for reducing ocular injury. We used a rectangular advancement musculocutaneous flap for anterior lamellar reconstruction and a specially designed rectangular advancement tarsoconjunctival flap for posterior lamellar reconstruction. The novel design was a slice of tarsus pared off from the free edge of the tarsoconjunctival flap, which created a space such that the corresponding remnant conjunctiva could easily bend forward and cover the tarsal edge. The risk of ocular complications was thus decreased. We analyzed 24 patients who had received eyelid margin reconstruction by this method. Data on postoperative clinical outcomes, complications, and patient satisfaction were obtained. All patients were followed up face to face or online for at least one year.
Materials and Methods
This study was a single-center case series of patients from the practice of a single experienced plastic reconstructive surgeon at a tertiary center. We consecutively recruited outpatients in the Department of Plastic Surgery in the Second Affiliated Hospital of Harbin Medical University from 2014 to 2021. The inclusion criteria were (1) eyelid margin mass and (2) willingness to receive eyelid margin reconstruction by the reported method. The exclusion criteria were (1) eyelid margin mass involving most or all of the tarsus and (2) less than one year of follow-up. Patients’ age; gender; lesion location, depth, and size; outcomes; and follow-up time were collected in medical records. Outcomes including asymmetry, eyelid distortion or deformity, eyelash discontinuity, Vancouver Scar Scale (VSS) score, disability of opening and closing the eyelid, ocular discomfort, entropion or ectropion, eyelid retraction, trichiasis, and recurrence were assessed by two plastic surgeons and scored none (0), slight (1), moderate (2), or severe (3). For VSS, 0–3 was none; 4–6 was slight; 7–9 was moderate; and 10–13 was severe.6 Each patient’s total score was classed as excellent (0–10), good (11–20), or poor (21–30). A patient satisfaction survey was conducted, with possible ratings of not satisfied, slightly satisfied, moderately satisfied, or very satisfied. All data were collected in a multiple fashion.
Our study was approved by the Medical Ethics Committee of the Second Affiliated Hospital of Harbin Medical University. Informed consent was obtained from all patients.
Surgical Procedure
Incision
Under 1% lidocaine and 1:100,000 adrenaline, a rectangular resection of mass on the eyelid margin was performed (#11 fine point blade) 1 mm from its edge. For lesions invading the gray line, full-thickness resection was conducted. If the gray line was intact, the posterior lamella was reserved. Hemostasis was then achieved, and lesion tissue was sent for histopathology examination.
Posterior Reconstruction by Tarsoconjunctival Flap with Special Design
For full-thickness eyelid margin defects, we started with posterior lamellar reconstruction using a specially designed advancement tarsoconjunctival flap (Figures 1A–D and 2A–D). We flipped the eyelid inside out with the help of an assistant or sutures with the cheek. We incised the palpebral conjunctiva and tarsus along the extended vertical lines of the rectangular defect. The height of the flap was the same as that of the defect. We bluntly separated the tarsus and muscle and removed a pair of dog triangles. After generating a rectangular tarsoconjunctival flap, we pared off an approximately 0.5-mm-thick piece of tarsus from its free edge (Figure 3A). We first separated the tarsus and conjunctiva using the #11 fine-point blade. By clipping the orbicularis oculi muscle and tarsus together, we immobilized the tarsoconjunctival flap. The other hand made the blade cling to the tarsus and used the reverse technique to separate about 0.5-mm-deep conjunctiva from the tarsus. The blade was at a 45-degree angle from the flap edge. The conjunctiva retracted after separation. We then shaved the tarsus. We swiveled the blade located between the tarsus and conjunctiva into the direction vertical to the tarsus and shaved a 0.5-mm-thick piece of tarsus (Figure 3B). The corresponding remnant conjunctiva flap finally folded forward to cover the tarsus edge after suturing between the anterior and posterior lamellas (Figure 3C and D). This not only prevented tarsus edge abrasion of the cornea and bulbous conjunctiva but also kept the suture away from the eyeball. We then advanced the rectangular tarsoconjunctival flap and sutured under the conjunctiva (7–0 Vicryl undyed braided).
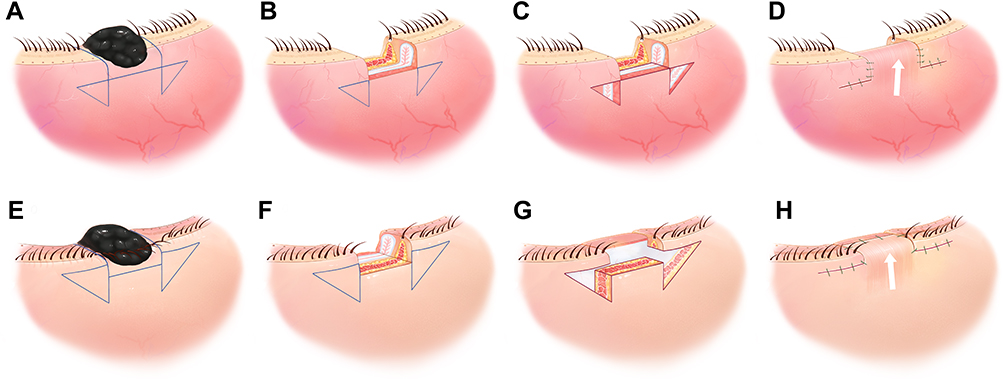 |
Figure 1 (A) The full-thickness mass and the incisions (blue line) designed on the conjunctiva; (B) The full-thickness eyelid margin defect after excising the mass; (C) Excising a pair of dog triangles on the posterior lamellar eyelid; (D) Advancing the tarsoconjunctival flap along the arrow direction and suturing; (E) The full-thickness mass and the incisions (blue line) designed on the skin; (F) The full-thickness eyelid margin defect after excising the mass; (G) Excising a pair of dog triangles on the anterior lamellar eyelid; (H) Advancing the musculocutaneous flap along the arrow direction and suturing. |
 |
Figure 2 (A) The full-thickness eyelid margin mass; (B) The incisions designed on the palpebral conjunctiva; (C) The full-thickness eyelid margin defect after excising the mass; (D) Advancing the tarsoconjunctival flap and suturing under the conjunctiva; (E) The full-thickness eyelid margin mass and the incisions designed on the skin; (F) The full-thickness eyelid margin defect after excising the mass; (G) Excising a pair of dog triangles on the anterior lamellar eyelid; (H) Advancing the orbicularis oculi musculocutaneous flap and suturing. |
 |
Figure 3 (A) A 0.5-mm-thick piece of tarsus pared off from the tarsoconjunctival flap’s free edge; (B) The photograph of the free edge of the tarsoconjunctival and conjunctival flap; (C) The conjunctiva folded forward after suturing (dotted lines), covering the tarsus edge; (D) The photograph shows the edge of the sutured anterior and posterior lamellas. |
Anterior Reconstruction by Musculocutaneous Flap
For anterior lamella defects or full-thickness defects after posterior lamella reconstruction, we used a rectangular advancement orbicularis oculi musculocutaneous flap to reconstruct the anterior lamella (Figures 1E–H, 2E–H, 4 and 5). Vertical incisions were extended to the same height as the defect, and then part or all of the orbicularis oculi muscle was separated bluntly. We often designed the dog triangles at the root of eyelashes for an inconspicuous scar. However, if the lesion was wide and located on the upper eyelid with a double eyelid crease, we also considered incising the dog triangles along the double eyelid crease (Figure 6). We then advanced the orbicularis oculi musculocutaneous flap and sutured it. When suturing the free edges of the musculocutaneous flap and the tarsoconjunctival flap, we guided the needle forward through the root of the conjunctival flap, then downward through the front upper part of the tarsus of the tarsoconjunctival flap and finally through the musculocutaneous flap (7–0 Vicryl undyed braided) (Figure 3C, d). The knot was tied on the surface of the musculocutaneous flap, away from the eyeball and threads were cut short enough to avoid ocular injury or long enough to be immobilized on the cheek.
 |
Figure 4 (A) The anterior lamella eyelid margin mass and incisions (blue line) on the skin; (B) The anterior lamella eyelid margin mass did not invade the gray line; (C) The anterior lamella eyelid margin defect after excising the mass; (D) Excising a pair of dog triangles; (E) Advancing the musculocutaneous flap along the arrow direction and suturing. |
 |
Figure 5 (A) The anterior lamella eyelid margin mass on the skin; (B) The anterior lamella eyelid margin mass did not invade the gray line; (C) The anterior lamella eyelid margin defect and incisions designed on the skin; (D) Excising a pair of dog triangles; (E) After advancing the musculocutaneous flap and suturing when closing the eyes; (F) After advancing the musculocutaneous flap and suturing when opening the eyes. |
 |
Figure 6 (A) Designed incisions of the lesion and dog triangles along the double eyelid crease; (B) Excising the lesion and dog triangles and making the advancement flap; (C) Suturing the advancement flap; (D) The preoperative appearance; (E) The postoperative appearance. |
Postoperative Care
We changed dressings after three days and removed sutures after seven days.
Results
We included 24 consecutive patients (25 lesions). The demographics, clinical characteristics, and outcomes of all patients are shown in Table 1. There were no modifications in participant selection or treatment. All patients were elective cases paid for by themselves. We included four medium lesions and 21 small lesions. Twenty patients received anterior lamellar reconstruction (Figures 7 and 8), and four patients with full-thickness defects received bilamellar reconstruction (Figures 9 and 10). All lesions were benign nevi. Almost all patients experienced eyelash discontinuity. Eyelash discontinuity was noticeable in cases in which lesions lay at the middle of the upper eyelid margin, especially when closing the eyes (Figure 7), and it was unclear for lesions near the canthus. One patient presented slight distortion—notching of the lower eyelid margin—and thus slight asymmetry two months after surgery (Figure 9). The notching improved naturally after one year. Patients reported no distortion or deformity, scar, disability of opening and closing the eyelid, ocular discomfort, eyelid entropion or ectropion, eyelid retraction, trichiasis, or recurrence. For one patient with an upper eyelid marginal lesion (case one), the dog triangles were designed in the double eyelid crease, while others were at the root of the eyelash. It had little effect on the morphology of the double eyelid crease when the dog triangles sat near the double eyelid crease. The outcome scores ranged from 0 to 3, and the average score was 1.23±0.69, indicating that the effect of the reconstruction was excellent. All patients were very satisfied with the surgery. The average follow-up time was 5.75 years.
 |
Table 1 Demographics, Clinical Characteristics and Outcomes |
 |
Figure 7 (A) The preoperative appearance; (B) The postoperative appearance one week after surgery; (C) The postoperative appearance six months after surgery when looking straight ahead; (D) The postoperative appearance six months after surgery when looking down; (E) The postoperative appearance six months after surgery when closing the eyes. |
 |
Figure 8 (A) The preoperative appearance of case 24; (B) The postoperative appearance one week after surgery; (C) The postoperative appearance six months after surgery. |
 |
Figure 9 (A) The preoperative appearance of case 11; (B) The postoperative appearance one week after surgery; (C) The postoperative appearance two months after surgery. |
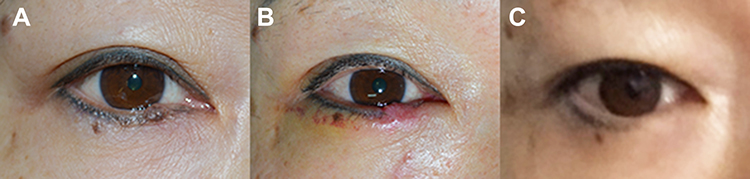 |
Figure 10 (A) The preoperative appearance of case seven; (B) The postoperative appearance one week after surgery; (C) The postoperative appearance six years after surgery. |
Discussion
Some criteria exist for aesthetic eyelid reconstruction: (1) the eyelid margin keeps a proper distance from the scleral limbus, (2) the skin resembles the nearby normal skin, and (3) the lateral scleral triangle and canthal angle are crisp.7 Our method appeared successful in eyelid margin reconstruction for small to medium defects. Most participants obtained satisfactory eyelid margin reconstruction with good aesthetic and functional outcomes. Eyelash discontinuity was acceptable due to its minor effect on aesthetic appearance and could be hidden easily.
One patient had slight lower eyelid notching. We inferred that the reason was that the tarsus height of the tarsoconjunctival flap could not produce sufficient support for a medium lower eyelid margin defect. This defect was the largest among all participants, with a 15-mm width and 1-mm height in the posterior lamella in the lower eyelid. The height of the inferior tarsus was much less than the superior tarsus, only 3.5–5 mm at most. At least 4 mm of tarsus height is required to support the eyelid margin. Another possible reason was much retraction tension from the advancement flaps since we reserved the retractors.
The unique complications of eyelid reconstruction include wound dehiscence, cornea and bulbar conjunctiva injury, eyelid ectropion, entropion, retraction, ptosis, trichiasis, and even lagophthalmos and exposure keratitis.8 Maintaining proper horizontal eyelid margin tension is key. Our method used the remnant tarsus to maintain the original tarsus width, transforming the extra transverse tension into vertical tension. The novelty of our method was a specially designed tarsoconjunctival flap, a tarsoconjunctival, conjunctiva only flap actually, designed to reduce ocular injury. Paring off a 0.5-mm-thick tarsus from its free edge released space to enable the corresponding conjunctiva remnant to be folded forward. Hence, the conjunctiva fully covered the free tarsus edge, and the suture seam was kept away from the eyeball, preventing cornea and bulbar conjunctiva abrasion. Similarly, a Japanese surgeon emphasized the need to suture the conjunctiva as much as possible to reconstruct the complete margin and prevent free tarsus ablation.9 Our concept—the pared tarsus in the tarsoconjunctival flap—could be extended to other posterior lamellar reconstruction procedures. The point is to keep the tarsus or other alternative grafts slightly shorter than the conjunctiva or mucosa.
For small and medium eyelid margin defects, direct closure was the most common and simple strategy, especially in cases of high eyelid skin laxity. Defects were trimmed into triangles or pentagons and closed with various suture techniques.10–12 A vertical scar was inevitable, so some techniques, such as curvilinear pentagonal wedge resection or resection below the musculocutaneous flap, were proposed to diminish its length.13,14 Sometimes combining direct closure with canthotomy and cantholysis was necessary to avoid wound dehiscence or palpebral fissure deformation caused by high horizontal tension. For these cases, surgical complexity and injury to normal tissue increased, and direct closure was not preferred. Second-intention healing of marginal defects could also achieve acceptable outcomes, mainly for small to medium anterior lamella defects, as well as full-thickness defects in the lower eyelid.15,16 Second-intention healing caused minimal trauma and shortened the operation period with compromised aesthetic appearance and healing time. Given that Asians are more prone to scar formation than Europeans, we suggest that second-intention healing should be conducted cautiously as a kind of treatment of exclusion. Recently, laser and radiofrequency ablation have obtained excellent cosmetic results for small eyelid margin lesions, and the rates of recurrence and complications have declined following the development of this technique.17 Compared with other methods, flaps could better maintain the original eyelid margin contour and horizontal tension. For medium and large defects, various flaps and grafts are used independently or cooperatively to achieve eyelid margin reconstruction. The consensus is that the two lamellas of the eyelid should be reconstructed independently. Mainstream practice is that either lamella should possess a vascularized pedicle in the eyelid reconstruction. However, a recent study reported that both free grafts for two lamellas also achieved good blood perfusion and survival.18 The anterior lamella can be repaired by advancement, rotation, and transposition flaps, such as the Tenzel flap, Tripier flap, or Cutler-Beard flap, or by free skin and musculocutaneous grafts. The Tenzel flap is the most common technique used for repairing medium defects or supplementing other techniques to repair large defects. A pedicled nearby transposition flap could provide good mobility and little tension when repairing medium to large marginal defects.19,20 A part of the lower eyelid sometimes has to be compromised to reconstruct the upper eyelid because of the upper eyelid’s greater functional importance.21 The V-Y advancement flap could also be used to repair eyelid marginal defects, despite the significant scar.22 The rectangular advancement flap is a better fit for small and medium or transversal lesions and leaves less significant scars. The posterior lamella can be reconstructed by a pedicled tarsoconjunctival flap, such as the Hughes flap; free tarsoconjunctival graft (Hubner’s tarsomarginal graft); composite grafts combining mucosa with nasal septal cartilage, hard palate, or acellular dermal matrix; or a periosteal flap.23,24 The Hughes flap and Hubner’s tarsomarginal grafts are the most common. The tarsoconjunctival flap of our method is actually a Hughes-type eyelid pedicle flap containing the residual tarsus which could avoid the complications caused by the grafts. Several published studies prove that the tarsoconjunctival flap could repair the eyelid margin defects with any width, even total or near-total eyelid margin, of both the upper and lower eyelid.25–29 However, sufficient remnant tarsus is necessary (at least 3–4 mm) to support the eyelid margin. Given that, we believe this method is more suitable for upper eyelid margin reconstruction due to the higher tarsus than the lower eyelid and is a good option for the transverse defect of which the horizontal width is much greater than the vertical height.
Our method has some limitations. It cannot be used to repair lesions that invade most or all of the tarsus because of the lack of available tarsus for advancement. Although this method could repair the defects with any width, wider defects are usually accompanied by greater vertical height. It was a pity that our report did not include any patient with large eyelid margin defect but sufficient tarsus. Although similar European cases have been reported, we still require the Asian cases to verify the effect of this method for large eyelid margin reconstruction since the Asians have less available eyelid tissue than the Europeans. For large anterior defects, a rotation or transposition flap should be selected first rather than the advancement flap. The advancement flap would undermine a large amount of normal tissue and leave facial scars regardless of skin laxity.
Conclusion
We reviewed 24 patients who received eyelid margin reconstruction by our reported method: anterior lamellar reconstruction by an advancement musculocutaneous flap and posterior lamellar reconstruction by an advancement tarsoconjunctival flap. The tarsoconjunctival flap was specially designed to reduce the risk of ocular complications. Our method seemed successful in aesthetic and functional eyelid margin reconstruction for small and medium defects, with few complications. We believe it is an especially good option for transverse defects. In the future, its strengths and limitations could be obtained from a comparative study with other reconstruction methods. The study on the large eyelid margin defects with sufficient tarsus for the Asians is needed as well.
Abbreviations
VSS, Vancouver Scar Scale.
Data Sharing Statement
The authors do not intend to share individual participant data because all necessary data have been reported in this paper.
Ethics Approval and Informed Consent
Our study was approved by the Medical Ethics Committee of the Second Affiliated Hospital of Harbin Medical University. The permit number is KY-2016005. Informed consent was obtained from all patients.
Consent for Publication
All patients in the figures have been shown the article contents and gave the consent. All figures are original and have not been published elsewhere previously.
Clinical Trials Registration
We have prospectively registered the trial in Chinese Clinical Trial Registry (ChiCTR) and the Clinical Trial Registration number is ChiCTR-ONC-16007886.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the young and middle aged innovative science research foundation of the second affiliated hospital of Harbin medical university (KYCX2018-05), the Heilongjiang provincial postdoctoral science foundation (0202-21042160137), the Heilongjiang province natural science foundation (LH2019H069), the Chinese postdoctoral science foundation (2019M661299).
Disclosure
All authors report no conflicts of interest or competing interests in this work.
References
1. Harvey DT, Taylor RS, Itani KM, Loewinger RJ. Mohs micrographic surgery of the eyelid: an overview of anatomy, pathophysiology, and reconstruction options. Dermatologic Surgery. 2013;39(5):673–697. doi:10.1111/dsu.12084
2. Knop E, Korb DR, Blackie CA, Knop N. The lid margin is an underestimated structure for preservation of ocular surface health and development of dry eye disease. Dev Ophthalmol. 2010;45:108–122.
3. Shimizu N, Oshitari T, Yotsukura J, Yokouchi H, Baba T, Yamamoto S. Ten-year epidemiological study of ocular and orbital tumors in Chiba University Hospital. BMC Ophthalmol. 2021;21(1):344. doi:10.1186/s12886-021-02108-w
4. Wang L, Shan Y, Dai X, et al. Clinicopathological analysis of 5146 eyelid tumours and tumour-like lesions in an eye centre in South China, 2000-2018: a retrospective cohort study. BMJ Open. 2021;11(1):e041854. doi:10.1136/bmjopen-2020-041854
5. Yu -S-S, Zhao Y, Zhao H, Lin J-Y, Tang X. A retrospective study of 2228 cases with eyelid tumors. Int J Ophthalmol. 2018;11(11):1835–1841. doi:10.18240/ijo.2018.11.16
6. Sullivan T, Smith J, Kermode J, McIver E, Courtemanche DJ. Rating the burn scar. J Burn Care Rehabil. 1990;11(3):256–260. doi:10.1097/00004630-199005000-00014
7. Alghoul MS, Bricker JT, Vaca EE, Purnell CA. Lower Eyelid Reconstruction: a New Classification Incorporating the Vertical Dimension. Plast Reconstr Surg. 2019;144(2):443–455. doi:10.1097/PRS.0000000000005882
8. Chang EI, Esmaeli B, Butler CE. Eyelid Reconstruction. Plast Reconstr Surg. 2017;140(5):724e–735e. doi:10.1097/PRS.0000000000003820
9. Yamashita K, Yotsuyanagi T, Sugai A, et al. Full-thickness total upper eyelid reconstruction with a lid switch flap and a reverse superficial temporal artery flap. J Plast Reconstr Aesthet Surg. 2020;73(7):1312–1317. doi:10.1016/j.bjps.2020.02.017
10. Perry JD, Aguilar CL, Kuchtey R. Modified vertical mattress technique for eyelid margin repair. Dermatologic Surgery. 2004;30(12 Pt 2):1580–1582. doi:10.1111/j.1524-4725.2004.30570.x
11. Wessman LL, Demer A, Behshad R, Maher IA. Preparing for and Executing a Pentagonal Wedge Mohs Layer for Tumors of the Marginal Eyelid. Dermatologic Surgery. 2021;47(7):992–994. doi:10.1097/DSS.0000000000002882
12. Burroughs JR, Soparkar CNS, Patrinely JR. The buried vertical mattress: a simplified technique for eyelid margin repair. Ophthal Plast Reconstr Surg. 2003;19(4):323–324. doi:10.1097/01.IOP.0000075013.85905.9B
13. Garcia GA, Nguyen CV, Vo TA, Yonkers MA, Minckler DS, Tao JP. Lazy Pentagonal Wedge Resection of Eyelid Margin Lesions. JAMA Facial Plast Surg. 2018;20(3):251–252. doi:10.1001/jamafacial.2017.1902
14. Dailey RA, Chavez MR. Upper eyelid margin mass excision technique: supraciliary approach. Ophthal Plast Reconstr Surg. 2011;27(1):48–51. doi:10.1097/IOP.0b013e3181dee5df
15. Trieu DN, Drosou A, White LE, Goldberg LH. Outcomes of Second Intention Healing of the Lower Eyelid Margin After Mohs Micrographic Surgery. Dermatologic Surgery. 2019;45(7):884–889. doi:10.1097/DSS.0000000000001951
16. Xu H, Qiu Y, Wang X, et al. Improved Tumor Resection on the Palpebral Margin. J Craniofac Surg. 2019;30(3):907–910. doi:10.1097/SCS.0000000000005161
17. Wang J-X, Li Y-L, Gao Y-M, et al. Radiofrequency ablation micro-dissecting of eyelid nevus with XL-RFA device under operating microscope. Int J Ophthalmol. 2019;12(7):1116–1121. doi:10.18240/ijo.2019.07.10
18. Tenland K, Berggren J, Engelsberg K, et al. Successful Free Bilamellar Eyelid Grafts for the Repair of Upper and Lower Eyelid Defects in Patients and Laser Speckle Contrast Imaging of Revascularization. Ophthal Plast Reconstr Surg. 2021;37(2):168–172. doi:10.1097/IOP.0000000000001724
19. Yoshitatsu S, Shiraishi M. A modified method for upper eyelid reconstruction with innervated orbicularis oculi myocutaneous flaps and lower lip mucosal grafts. JPRAS Open. 2021;28:131–139. doi:10.1016/j.jpra.2021.03.003
20. Yano T, Karakawa R, Shibata T, et al. Ideal esthetic and functional full-thickness lower eyelid “like with like” reconstruction using a combined Hughes flap and swing skin flap technique. J Plast Reconstr Aesthet Surg. 2021. doi:10.1016/j.bjps.2021.03.119
21. Yamashita K, Yotsuyanagi T, Sugai A, et al. Full-thickness total upper eyelid reconstruction with a lid switch flap and a reverse superficial temporal artery flap. J Plastic Reconstructive Aesthetic Surgery. 2020;73(7):1312–1317.
22. Seth D, Scott JF, Bordeaux J. Repair of a Large Full-Thickness Defect of the Lower Eyelid. Dermatologic Surgery. 2021;47(1):117–119. doi:10.1097/DSS.0000000000002622
23. Scott JF, Bordeaux JS, Redenius RA. How We Do It: periosteal Flaps for Full-Thickness Eyelid Defects. Dermatologic Surgery. 2020;46(4):564–566. doi:10.1097/DSS.0000000000001791
24. Vimont T, Arnaud D, Rouffet A, Giot JP, Florczak AS, Rousseau P. Hübner’s tarsomarginal grafts in eyelid reconstruction: 94 cases. J Stomatol Oral Maxillofacial Surgery. 2018;119(4):268–273. doi:10.1016/j.jormas.2018.03.001
25. Moesen I, Paridaens D. A technique for the reconstruction of lower eyelid marginal defects. Br J Ophthalmol. 2007;91(12):1695–1697. doi:10.1136/bjo.2007.123075
26. Harris S, Silkiss RZ. Revisiting the single-eyelid Hughes reconstruction - A report of two cases. Am J Ophthalmol Case Rep. 2022;27:101667. doi:10.1016/j.ajoc.2022.101667
27. Malik A, Shah-Desai S. Sliding tarsal advancement flap for upper eyelid reconstruction. Orbit. 2014;33(2):124–126. doi:10.3109/01676830.2013.814681
28. Irvine F, McNab AA. A technique for reconstruction of upper lid marginal defects. Br J Ophthalmol. 2003;87(3):279–281. doi:10.1136/bjo.87.3.279
29. Jordan DR, Anderson RL, Nowinski TS. Tarsoconjunctival flap for upper eyelid reconstruction. Arch Ophthalmol. 1989;107(4):599–603. doi:10.1001/archopht.1989.01070010613041
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.