Back to Journals » International Journal of Women's Health » Volume 18
Turning Challenges into Success: Successful Pregnancy in Advanced Maternal Age with Adenomyosis Using Prolonged GnRH Agonist Protocol: A Case Report
Authors Syam HH ![]() , Halim D
, Halim D ![]() , Tasya M, Adrianto N
, Tasya M, Adrianto N ![]()
Received 16 March 2026
Accepted for publication 4 May 2026
Published 19 May 2026 Volume 2026:18 609580
DOI https://doi.org/10.2147/IJWH.S609580
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Hanom Husni Syam,1 David Halim,1 Marissa Tasya,1 Nicholas Adrianto2
1Division of Reproductive Endocrinology and Infertility, Department of Obstetrics and Gynecology, Padjadjaran University, Dr Hasan Sadikin General Hospital, Bandung, West Java, Indonesia; 2School of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, North Jakarta, Daerah Khusus Ibukota Jakarta, Indonesia
Correspondence: Hanom Husni Syam, Division of Reproductive Endocrinology and Infertility, Department of Obstetrics and Gynecology, Padjadjaran University, Dr Hasan Sadikin General Hospital, Bandung, West Java, Indonesia, Email [email protected]
Abstract: Advanced maternal age (AMA) is a major challenge in reproductive medicine, compounded by coexisting conditions such as adenomyosis and endometriosis, which impair oocyte competence and endometrial receptivity. Prolonged gonadotropin-releasing hormone agonist (GnRHa) protocols have been proposed to improve in vitro fertilization-embryo transfer (IVF-ET) outcomes. We report the case of a 41-year-old Indonesian woman with 13 years of primary infertility, AMA, adenomyosis, endometriosis, and male factor infertility. Following laparoscopic excision of endometriosis, she underwent a prolonged GnRH agonist protocol with depot triptorelin, followed by controlled ovarian stimulation using recombinant FSH and LH. Despite an initially modest response, eight oocytes were retrieved and all fertilized via ICSI. Two good-quality day-3 embryos were transferred fresh, and three blastocysts were cryopreserved. Intensive luteal support with hCG, progesterone, dydrogesterone, and estradiol was administered. Serial β-hCG confirmed early pregnancy, and at the time of reporting, she is 35+6 weeks pregnant with a viable singleton and unremarkable antenatal course. This case demonstrates that prolonged GnRHa protocols may offer favorable outcomes in women with AMA and multiple adverse prognostic factors, including adenomyosis, endometriosis, and male factor infertility. While encouraging, such results require cautious interpretation, and further prospective studies incorporating preimplantation genetic testing and cumulative live birth rate are needed to clarify their broader applicability.
Keywords: infertility, fertilization in vitro, gonadotropin-releasing hormone, adenomyosis
Introduction
Adenomyosis is a well recognized contributor to reduced success in in vitro fertilization-embryo transfer (IVF-ET) success. Despite numerous proposed strategies, no stimulation approach has consistently and robustly improved outcomes.1 Prolonged GnRH agonist (GnRHa) protocols have demonstrated favorable effects on IVF outcomes in patients with adenomyosis.2–4 However, their efficacy in advanced maternal age (AMA) remains uncertain with available studies failed to demonstrate consistent or promising results.5 AMA itself has become a critical demographic and clinical challenge, as increasing numbers of women postpone childbearing beyond the age of 35.6,7 It is associated with diminished ovarian reserve, impaired oocyte quality, and reduced IVF success rates. In addition, AMA women may exhibit relative LH deficiency and premature LH surges, further compromising follicular development and implantation.1,8
The management of infertility becomes even more complex when AMA coexists with adenomyosis or endometriosis, as these conditions further impair outcomes through altered endometrial receptivity, chronic pelvic inflammation, and disruption of oocyte quality.9 In such cases, prolonged GnRHa protocols may offer dual benefits: stabilizing LH dynamics in aging ovaries while simultaneously suppressing adenomyotic and endometriotic activity, thereby creating a more favorable reproductive environment.10 By achieving deeper pituitary downregulation and more stable hormonal control, prolonged GnRHa pretreatment may enhance both oocyte maturation and endometrial receptivity in this difficult-to-treat population.9,10
Emerging evidence suggests that prolonged GnRHa protocols may improve oocyte yield and support endometrial receptivity in AMA, though robust data on live birth outcomes remain limited. This highlights the importance of continued evaluation of such strategies.11 Here, we report a case of an AMA patient with adenomyosis and endometriosis, who achieved unexpectedly high mature oocyte yield following a prolonged GnRHa protocol, highlighting its potential role in this challenging population.
Case Presentation
A 41-year-old Indonesian woman, married for thirteen years and nulliparous, presented to our fertility clinic with primary infertility. Her medical history was significant for AMA, posterior adenomyosis (Figure 1), and symptomatic endometriosis previously managed by surgical ablation and excision of superficial lesions across the tubo-ovarian regions, uterine corpus, and peritoneum (laparoscopic surgery performed on December 3, 2024) (Figure 2). Despite prior interventions, her ovarian reserve was within normal limits for age, with anti-Müllerian hormone measuring 2.41 ng/mL both pre- and post-operatively. Her partner was diagnosed with teratozoospermia, as evidenced by sperm analysis showing a normal total count and motility but only 2% normal morphology, contributing a significant male factor to their infertility diagnosis. There was no significant family or psychosocial history.
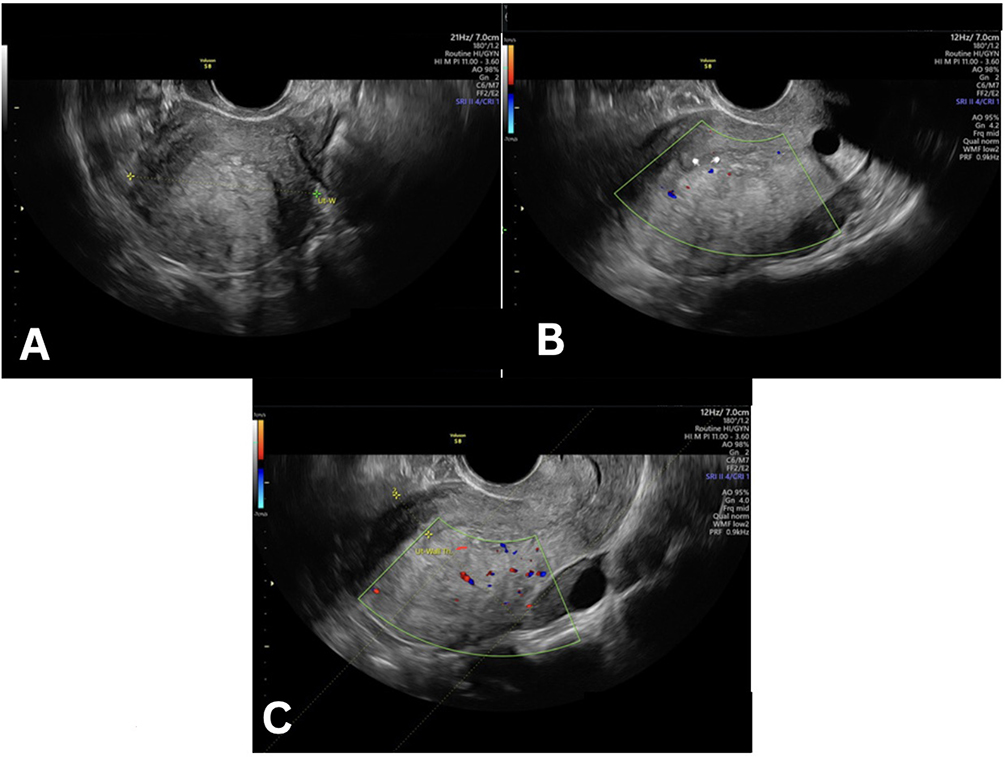 |
Figure 1 Transvaginal ultrasound features of posterior adenomyosis. (A) Coronal transvaginal ultrasound demonstrating posterior myometrial heterogeneity and ill-defined thickening without a discrete focal mass. (B) Transvaginal ultrasound showing characteristic adenomyosis features, including subendometrial echogenic lines and buds extending into the posterior myometrium. (C) Sagittal transvaginal ultrasound illustrating asymmetric posterior myometrial wall thickening with increased translesional vascularity on color Doppler, consistent with posterior adenomyosis. |
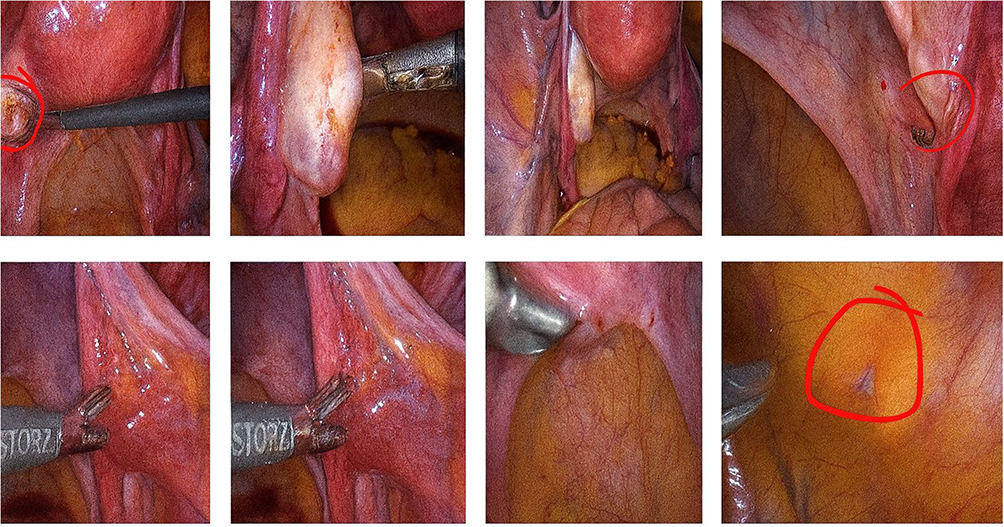 |
Figure 2 Laparoscopic findings demonstrating superficial endometriosis involving the peritoneum, left ovary, and left ovarian fossa, with red-marked areas indicating the superficial lesions. |
Given the challenging context of adenomyosis, endometriosis, AMA, and male factor infertility, a personalized IVF strategy was adopted, employing a prolonged GnRHa protocol aimed at maximizing follicular recruitment and suppressing residual endometriosis activity. Following surgery, the patient received a depot triptorelin acetate 3.75 mg injection on day 2 menstruation, initiating pituitary downregulation for four weeks. Monitoring confirmed complete down-regulation, with a baseline estradiol (E2) of 10.49 pg/mL and endometrial thickness of 3.7 mm. Controlled ovarian stimulation (COS) was then initiated using follitropin alfa 300 IU and lutropin alfa 150 IU (Pergoveris®) during the stimulation phase. On stimulation day (SD) 6, transvaginal ultrasound demonstrated ten developing follicles (six on the left ovary and four on the right, most measuring <11 mm). An additional 75 IU of follitropin alfa was introduced, increasing the daily dose to follitropin alfa 375 IU with lutropin alfa 150 IU. By SD8, follicular growth remained modest (<13 mm), and by SD10 progression had plateaued, necessitating escalation to follitropin alfa 450 IU with lutropin alfa 150 IU. At trigger, the leading follicular diameters measured 15.4–20.5 mm (mean 17.0 mm). At the time of final maturation, E2 was 2903.5 pg/mL and progesterone 0.86 ng/mL. Final oocyte maturation was induced with 250 µg choriogonadotropin alfa (Ovidrel®) (Figure 3). Eight oocytes were retrieved, all underwent intracytoplasmic sperm injection (ICSI), achieving 100% fertilization. Embryo culture was continued to day 3 (D3), yielding seven embryos. Two good-quality D3 embryos were selected for fresh transfer (Figure 4A and B), while the remaining five were cultured to day 5 (D5). Of these, three blastocysts reached sufficient quality, comprising two good-quality and one moderate-quality embryo, which were cryopreserved.
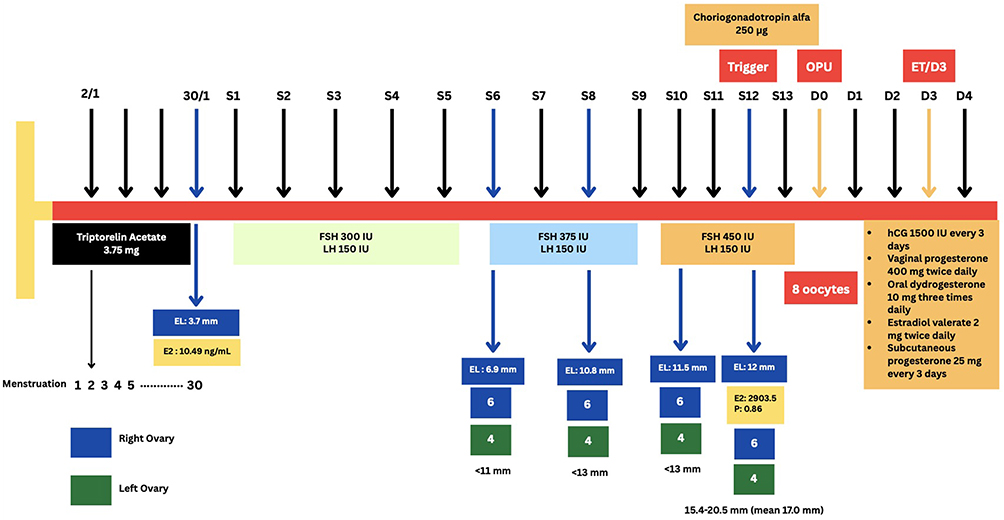 |
Figure 3 Protocol stimulation chart. |
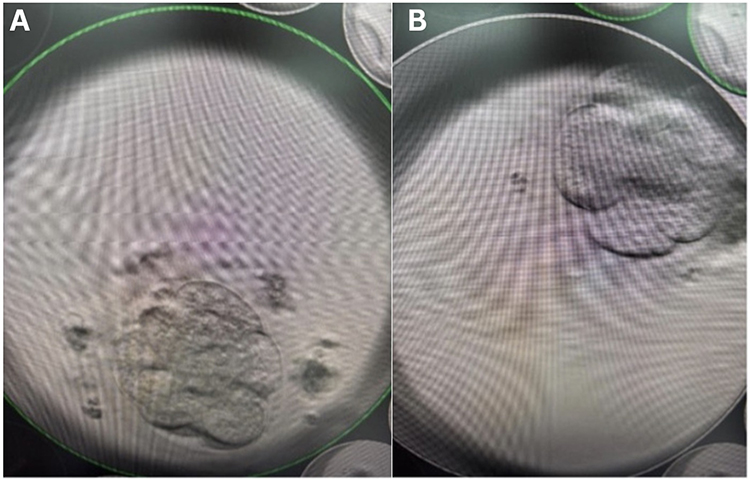 |
Figure 4 Morphology of the two cleavage-stage embryos selected for transfer on day 3. (A) Embryo 1 at the 7-cell stage with good morphological quality. (B) Embryo 2 at the 7-cell stage with good morphological quality. |
The evening after oocyte pickup (OPU), the patient received intensive luteal phase support consisting of hCG 1500 IU every 3 days, vaginal progesterone 400 mg twice daily, oral dydrogesterone 10 mg three times daily, estradiol valerate 2 mg twice daily, and subcutaneous progesterone 25 mg every 3 days, up to 12 weeks of gestation. Serial β-hCG monitoring demonstrated a positive trend, rising from 80 mIU/mL after ET to 1920 mIU/mL one week later, consistent with early pregnancy. The patient was followed with close antenatal surveillance throughout the pregnancy (Figure 5A and B). At the time of reporting, the patient is 35+6 weeks pregnant with a viable singleton fetus; physical examination was unremarkable, with stable vital signs and normal systemic findings.
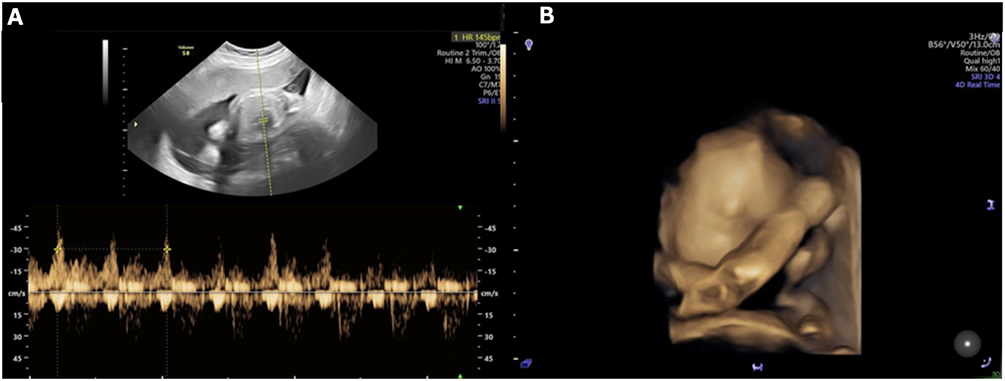 |
Figure 5 Antenatal ultrasound surveillance demonstrating fetal well-being. (A) Pulsed-wave Doppler ultrasound confirming a normal fetal heart rate. (B) Three-dimensional (3D) rendered ultrasound at 26 weeks of gestation showing a healthy singleton fetus with normal surface anatomy and no detectable anomalies. |
Discussion
This case highlights the potential of prolonged GnRHa protocols to overcome multiple reproductive challenges in women with AMA. The achievement of a clinical pregnancy in a patient with coexisting adenomyosis and endometriosis overcame low expectations and offers important insights into strategies for improving IVF outcomes in complex scenarios. Adenomyosis negatively impacts IVF-ET outcomes through impaired folliculogenesis, distorted pelvic anatomy hindering oocyte retrieval, reduced fertilization potential, and decreased implantation rates due to altered endometrial receptivity.12,13
Clinical pregnancy rates decline from approximately half in women without ultrasonographic adenomyosis to markedly lower levels in those with severe disease (42.7% vs. 13.0%), highlighting the prognostic impact of disease severity on IVF/ICSI outcomes. Notably, outcomes are further influenced by the frequent coexistence of endometriosis, reported in 33% to 87% of cases, which compounds the negative impact on reproductive prognosis, as illustrated in this case.14 Adenomyotic lesions are known to express GnRH receptors.3 Prolonged pituitary downregulation with GnRHa protocols induces a hypogonadotropic, hypogonadal state characterized by suppressed E2 levels, depriving lesions of hormonal stimulation.12 Several studies have reported favorable reproductive outcomes, including clinical pregnancies and live births, in women with adenomyosis following the use of prolonged GnRHa protocols.15,16
In addition to adenomyosis and endometriosis, AMA is an independent barrier to fertility, primarily due to a decreased ovarian reserve and diminished oocyte quality. Women over 35 experience a significant increase in embryo aneuploidy, with rates reaching up to 90% in their late 40s. The likelihood of producing a euploid blastocyst drops below 5% after the age of 43.1 Therefore, maximizing ovarian response is crucial for women with AMA, retrieving a larger number of oocytes increases the chances of identifying at least one euploid embryo. The optimal COS response is typically 6–15 oocytes, with LBR maximized at a yield of approximately 15 (12–18).17–20 Suboptimal retrieval reduces embryo availability, while excessive responses increase the risk of supraphysiologic E2 levels, ovarian hyperstimulation syndrome (OHSS), and impaired endometrial receptivity.11,21 Our case demonstrated an unexpectedly favourable response, retrieving eight mature oocytes and achieving 100% fertilization, underscoring how individualized strategies can mitigate the cumulative burden of AMA, adenomyosis, and endometriosis. This aligns with recommendations emphasizing tailoring ovarian stimulation protocols to patient-specific prognostic factors to optimize cumulative LBR in AMA patients.1,22
Conclusion
This case demonstrates that prolonged GnRHa protocols may achieve favorable outcomes in patients with AMA with multiple adverse prognostic factors, including adenomyosis and endometriosis. The achievement of fertilization and ongoing pregnancy in this patient is particularly notable, as these conditions generally result in poor IVF outcomes. While encouraging, such results should be interpreted cautiously, as they may not be generalizable. For patients with adenomyosis and AMA, prolonged downregulation represents a potential strategy to optimize both follicular recruitment and endometrial receptivity. These findings highlight the need for further prospective studies, ideally including preimplantation genetic testing and cumulative LBR as primary endpoints, to clarify the broader applicability of prolonged GnRHa protocols in such complex infertility cases.
Abbreviations
AMA, Advanced Maternal Age; COS, Controlled Ovarian Stimulation; D3, Day 3 (embryo culture stage); D5, Day 5 (embryo culture stage); E2, Estradiol; ET, Embryo Transfer; FSH, Follicle Stimulating Hormone; GnRH, Gonadotropin-Releasing Hormone; GnRHa, Gonadotropin-Releasing Hormone Agonist; hCG, Human Chorionic Gonadotropin; ICSI, Intracytoplasmic Sperm Injection; IVF-ET, In Vitro Fertilization–Embryo Transfer; LBR, Live Birth Rate; LH, Luteinizing Hormone; OPU, Oocyte Pick-Up; r-FSH, Recombinant Follicle Stimulating Hormone; SD, Stimulation Day.
Ethics Approval and Consent to Participate
Institutional review board approval was waived for this case report, as written informed consent for publication was obtained from the patient.
Consent for Publication
Written informed consent was obtained from the patient for publication of the case and the accompanying images.
Acknowledgement
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ubaldi FM, Cimadomo D, Vaiarelli A, et al. Advanced Maternal Age in IVF: still a Challenge? The Present and the Future of Its Treatment. Front Endocrinol. 2019;10. doi:10.3389/fendo.2019.00094
2. Hou X, Xing J, Shan H, et al. The effect of adenomyosis on IVF after long or ultra-long GnRH agonist treatment. Reprod Biomed Online. 2020;41(5):845–7. doi:10.1016/j.rbmo.2020.07.027
3. Park C, Mh C, Yang KM, Song IO. Pregnancy rate in women with adenomyosis undergoing fresh or frozen embryo transfer cycles following gonadotropin-releasing hormone agonist treatment. Clin Exp Reprod Med. 2016;43(3):169–173. doi:10.5653/cerm.2016.43.3.169
4. Niu Z, Chen Q, Sun Y, Feng Y. Long-term pituitary downregulation before frozen embryo transfer could improve pregnancy outcomes in women with adenomyosis. Gynecol Endocrinol. 2013;29(12):1026–1030. doi:10.3109/09513590.2013.824960
5. Ganer Herman H, Feferkorn I, Dahan MH, Reinblatt S, Demirtas E, Buckett W. A meta-analysis and systematic review of advanced maternal age patients in IVF. Hum Reprod Update. 2025; 31(6):dmaf020.
6. Schmidt L, Sobotka T, Bentzen JG, Nyboe Andersen A. on behalf of the ESHRE Reproduction and Society Task Force. Demographic and medical consequences of the postponement of parenthood. Hum Reprod Update. 2012;18(1):29–43. doi:10.1093/humupd/dmr040
7. Mills M, Rindfuss RR, McDonald P, te Velde E. ESHRE Reproduction and Society Task Force. Why do people postpone parenthood? Reasons and social policy incentives. Hum Reprod Update. 2011;17(6):848–860. doi:10.1093/humupd/dmr026
8. Bielfeld AP, Schwarze J-E, Verpillat P, et al. Effectiveness of recombinant human FSH: recombinant human LH combination treatment versus recombinant human FSH alone for assisted reproductive technology in women aged 35–40 years. Reprod Biomed Online. 2024;48(6):103725. doi:10.1016/j.rbmo.2023.103725
9. Somigliana E, Li Piani L, Paffoni A, et al. Endometriosis and IVF treatment outcomes: unpacking the process. Reprod Biol Endocrinol RBE. 2023;21(1):107. doi:10.1186/s12958-023-01157-8
10. Latif S, Kastora S, Wattar BHA, Yasmin E, Saridogan E, Mavrelos D. The effectiveness of prolonged downregulation with gonadotrophin-releasing hormone analogue (GnRHa) treatment in women with adenomyosis undergoing IVF/ICSI: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2024;301:87–94. doi:10.1016/j.ejogrb.2024.07.063
11. Tian L, Xia L, Wu Q. Retrospective analysis of GnRH-a prolonged protocol for in vitro fertilization in 18,272 cycles in China. J Ovarian Res. 2022;15(1):110. doi:10.1186/s13048-022-01044-7
12. Jaafar SH, Sallam HN, Arici A, Garcia-Velasco JA, Abou-Setta AM. Long-term GnRH agonist therapy before in vitro fertilization (IVF) for improving fertility outcomes in women with endometriosis. Cochrane Database Syst Rev. 2019;2019(11):CD013240. doi:10.1002/14651858.CD013240.pub2
13. Ren J, Sha A, Han D, Li P, Geng J, Ma C. Does prolonged pituitary down-regulation with gonadotropin-releasing hormone agonist improve the live-birth rate in in vitro fertilization treatment? Fertil Steril. 2014;102(1):75–81. doi:10.1016/j.fertnstert.2014.03.030
14. Chapron C, Tosti C, Marcellin L, et al. Relationship between the magnetic resonance imaging appearance of adenomyosis and endometriosis phenotypes. Hum Reprod. 2017;32(7):1393–1401. doi:10.1093/humrep/dex088
15. Silva PD, Perkins HE, Schauberger CW. Live birth after treatment of severe adenomyosis with a gonadotropin-releasing hormone agonist*. Fertil Steril. 1994;61(1):171–172. doi:10.1016/S0015-0282(16)56471-1
16. Huang FJ, Kung FT, Chang SY, Hsu TY. Effects of short-course buserelin therapy on adenomyosis. A report of two cases. J Reprod Med. 1999;44(8):741–744.
17. Ji J, Liu Y, Tong XH, Luo L, Ma J, Chen Z. The optimum number of oocytes in IVF treatment: an analysis of 2455 cycles in China. Hum Reprod Oxf Eng. 2013;28(10):2728–2734. doi:10.1093/humrep/det303
18. van der Gaast MH, Eijkemans MJC, van der Net JB, et al. Optimum number of oocytes for a successful first IVF treatment cycle. Reprod Biomed Online. 2006;13(4):476–480. doi:10.1016/S1472-6483(10)60633-5
19. Stanger JD, Yovich JL. Follicle recruitment determines IVF productivity rate via the number of embryos frozen and subsequent transfers. Reprod Biomed Online. 2013;27(3):286–296. doi:10.1016/j.rbmo.2013.05.015
20. Law YJ, Zhang N, Kolibianakis EM, et al. Is there an optimal number of oocytes retrieved at which live birth rates or cumulative live birth rates per aspiration are maximized after ART? A systematic review. Reprod Biomed Online. 2021;42(1):83–104. doi:10.1016/j.rbmo.2020.10.008
21. Ko DS, Lee SH, Park DW, Yang KM, Lim CK. Pregnancy and fertilization potential of immature oocytes retrieved in intracytoplasmic sperm injection cycles. Clin Exp Reprod Med. 2015;42(3):118–125. doi:10.5653/cerm.2015.42.3.118
22. Duan X, Li Z, Li M, Ma X. Analysis of controlled ovarian hyperstimulation protocols in women over 35 years old with poor ovarian response: a real-world study. BMC Pregnancy Childbirth. 2023;23(1):813. doi:10.1186/s12884-023-06112-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.