Back to Journals » International Medical Case Reports Journal » Volume 14
Turmeric-Induced Hepatotoxicity: Report of 2 Cases
Authors Sohal A, Alhankawi D, Sandhu S, Chintanaboina J
Received 2 October 2021
Accepted for publication 8 December 2021
Published 22 December 2021 Volume 2021:14 Pages 849—852
DOI https://doi.org/10.2147/IMCRJ.S333342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Aalam Sohal,1 Dhuha Alhankawi,2 Sunny Sandhu,1 JayaKrishna Chintanaboina2
1Department of Internal Medicine, UCSF Fresno, Fresno, CA, USA; 2Department of Gastroenterology and Hepatology, UCSF Fresno, Fresno, CA, USA
Correspondence: Aalam Sohal 155 N Fresno Street, Fresno, CA, USA
Email [email protected]
Abstract: The use of herbal and dietary supplements is rising in the United States. Turmeric has been one of the most popular supplements recently, used widely for various conditions such as arthritis, digestive disorder, and liver conditions. Although rarely reported, hepatotoxicity can happen with turmeric use. Here, we present 2 cases of drug-induced liver injury due to turmeric use with the complete resolution after cessation.
Keywords: turmeric, DILI, liver injury
Introduction
The use of herbal and dietary supplements (HDS) has significantly increased over the recent years.1 About 50% of the US population currently reports using at least one dietary supplement.1 Data have shown a concurrent increase in the incidence of drug-induced liver injury (DILI), which excluding acetaminophen has risen to 17%. Turmeric being one of the most popular HDS in the United States, and it had $32 million in sales between 2013 and 2017.2 Although turmeric is widely used for various conditions such as arthritis, digestive disorders and liver conditions, hepatotoxicity is a rare adverse effect only described in a few case reports. We present 2 cases of drug-induced liver injury (DILI) due to turmeric use, with the resolution of injury after cessation of turmeric use.
Case 1
A 57-year-old female with no significant past medical history presented with nausea, bloating, and jaundice for two weeks. She denied any alcohol or acetaminophen use. Physical examination was remarkable for right upper quadrant tenderness. She reported taking an over-the-counter supplement containing turmeric 2000 mg and black pepper daily for three months for back pain. Her other medications included omeprazole, metoprolol, atorvastatin, aspirin, fish oil, tamsulosin, and Vitamin D. Laboratory workup was remarkable for alanine transaminase (ALT) 1414 U/L, aspartate transaminase (AST) 1335 U/L, total bilirubin 8.6 mg/dl, and direct bilirubin 6.7mg/dl. Prothrombin time and INR were unremarkable.
Further laboratory workup including acute hepatitis serologies, anti-smooth muscle antibody and anti-mitochondrial antibody were unremarkable. Liver ultrasound revealed a normal liver with patent portal and hepatic veins. Liver biopsy revealed hepatocyte ballooning and necrosis, with an absence of periportal necrosis, steatosis, or fibrosis – overall suggestive of acute hepatitis. Serologies and immunostains on liver biopsy for cytomegalovirus, Epstein Barr virus and herpes simplex virus were negative. Ceruloplasmin and alpha-1-antitrypsin levels were also normal. The patient was advised to stop turmeric use, and her liver enzymes progressively down-trended (Figure 1). The patient was closely monitored in the outpatient setting by trending the liver enzymes as the patient’s nausea improved. Her symptoms ultimately resolved. Atorvastatin was initially held and then restarted at a low dose. She remained asymptomatic with normal liver enzymes six months after stopping the turmeric use.
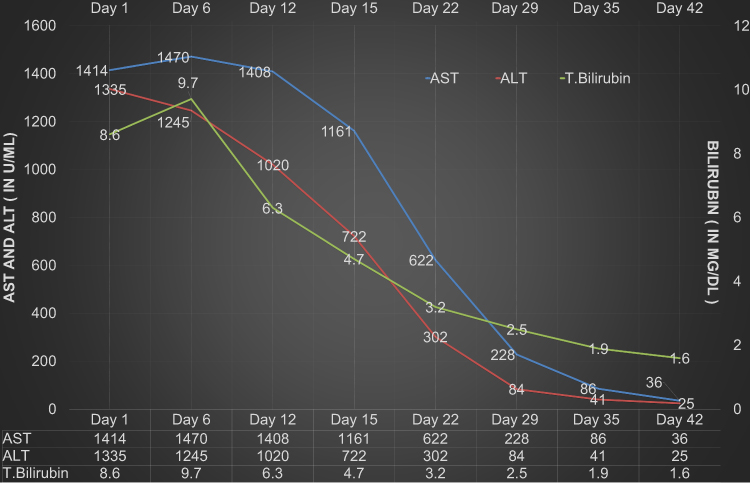 |
Figure 1 Trend of ALT, AST and bilirubin after stopping turmeric use in Case 1. |
Case 2
A 53-year-old female with no past medical history was sent to the emergency department by her primary care physician after abnormal liver function tests were noted on her routine laboratory workup. At the time of presentation, she complained of abdominal pain and nausea. The patient denied using alcohol or any prescribed medications. She was taking apple cider vinegar for over 5 years and had recently started taking turmeric tablets two times a day, and subsequently developed abdominal pain and nausea. Physical examination was unremarkable. Complete blood count was unremarkable. Laboratory tests were remarkable for ALT of 733 U/L, AST of 324 U/L, total bilirubin 1.8 mg/dl, and direct bilirubin 0.8mg/dl. Prothrombin time and INR were normal. Further laboratory workup including acute hepatitis serologies, anti-smooth muscle antibody and anti-mitochondrial antibody were unremarkable. Antinuclear antibody (ANA) titre was 1:40. Computed tomography (CT) triphasic of the liver revealed a cavernous hemangioma and hepatic steatosis.
The decision was made to follow up with the patient closely in the outpatient setting. Repeat liver function tests were done 20 days after the presentation, which revealed ALT of 74 IU/mL, AST of 52 IU/mL and total bilirubin of 0.6 mg/dl. The patient had a liver biopsy done two months after the initial presentation, which revealed nonspecific patchy, predominantly mononuclear portal inflammation without readily identifiable interface activity and clusters of ceroid-laden macrophages, suggesting a response to prior hepatocellular injury. Her Liver function tests were checked a month after the discontinuation and were completely normal.
Discussion
Drug-induced liver injury (DILI) is defined as a liver injury caused by medications, herbal supplements, or other xenobiotics leading to abnormalities in liver enzymes.3 Based on clinical presentation, it is classified into hepatocellular and cholestatic.4 The hepatocellular pattern of injury can be intrinsic (dose-dependent) or idiosyncratic (dose-independent).5 In our case, both the patients had a hepatocellular pattern of injury after taking turmeric as an over-the-counter medication in case 1 and food supplement in case 2.
European Food Safety Authority (EFSA) has established an Acceptable Daily Intake (ADI) for curcumin of 3 mg/kg/day.6 Our patient in Case 1 was taking a very high dose of turmeric, suggesting that injury from turmeric may likely be dose-dependent. Additionally, the patient in case one was taking a supplement of turmeric combined with black pepper (piperine) which has been known to enhance the absorption of turmeric use by 2000%.7 This increased bioavailability may have led to hepatotoxicity in this case. However, the possibility that piperine contributed to hepatotoxicity cannot be ruled out. Furthermore, the dose of turmeric that the patient took in case 2 was unclear.
DILI is typically diagnosed after the exclusion of other etiologies of liver dysfunction. In both cases, the common causes of acute liver injury such as hepatitides, alcohol, other hepatotoxic medications and autoimmune etiology were ruled out. The Roussel Uclaf Causality Assessment Method (RUCAM) scale is a tool used to assess the likelihood of hepatic dysfunction due to a specific drug.8 In the first case, the RUCAM score was 7, which correlates to “probable” (Table 1). In Case 1, the possibility of atorvastatin-induced hepatotoxicity was considered; however, it was deemed less likely as the patient was taking atorvastatin for more than 5 years. In addition, liver enzymes continued to stay normal after initiating atorvastatin. The above mentioned points went against the diagnosis of atorvastatin-induced hepatotoxicity. In the second case, the RUCAM score was six which correlates to “probable cause” of turmeric-induced liver injury. In both cases, the temporal relationship between turmeric use and transaminitis, positive de-challenge, and exclusion of common causes of liver injury supported turmeric use as the culprit for DILI. There have also been cases that report turmeric causing autoimmune hepatitis; however, neither of our patients had this presentation.9,10
 |
Table 1 RUCAM Scores in Cases 1 and 2 |
These findings of turmeric-induced liver injury are interesting as turmeric has recently gained popularity due to its antioxidant and anti-inflammatory properties.11 It is also used as a dietary supplement and a common additive in the food industry. A small study of 50 patients revealed that the use of curcumin, an active compound in turmeric, reduced the fibrosis scores in non-alcoholic fatty liver disease patients.12 However, there have also been less than 40 cases in the literature revealing that turmeric can cause liver damage.13 This case series adds to the growing evidence that turmeric use can lead to liver damage. Further research and regulation of dietary supplements is needed so that the physicians and the general population can make an educated decision about their use.
Conclusions
Our cases emphasize the need to recognize turmeric as one of the causes of DILI. They also highlight the importance of thorough history-taking regarding any over-the-counter medication use in a patient presenting with acute liver injury.
Ethics and Consent Statements
Informed Consent was obtained from both the patients prior to the manuscript submission for publication of the case details and any accompanying images. Therefore, IRB approval was not obtained for this study to publish the case details.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mishra S, Stierman B, Gahche JJ, Potischman N. Dietary supplement use among adults: United States, 2017–2018. NCHS Data Brief, no 399. Hyattsville, MD: National Center for Health Statistics; 2021. doi:10.15620/cdc:101131
2. Food Industry Executive. Turmeric Equals Sales Gold as Consumer Demand Grows. Available from: https://foodindustryexecutive.com/2020/06/turmeric-equals-sales-gold-as-consumer-demand-grows/vcv.
3. Suk KT, Kim DJ. Drug-induced liver injury: present and future. Clin Mol Hepatol. 2012;18(3):249–257. doi:10.3350/cmh.2012.18.3.249
4. Hussaini SH, Farrington EA. Idiosyncratic drug-induced liver injury: an overview. Expert Opin Drug Saf. 2007;6(6):673–684. doi:10.1517/14740338.6.6.673
5. Roth RA, Ganey PE. Intrinsic versus idiosyncratic drug-induced hepatotoxicity - two villains or one? J Pharmacol Exp Ther. 2010;332(3):692–697. doi:10.1124/jpet.109.162651
6. EFSA Panel on Food Additives and Nutrient Sources added to Food (ANS). Scientific opinion on the re-evaluation of curcumin (E 100) as a food additive. EFSA J. 2010;8(9):1679.
7. Shoba G, Joy D, Joseph T, Majeed M, Rajendran R, Srinivas PSSR. Influence of piperine on the pharmacokinetics of curcumin in animals and human volunteers. Planta Med. 1998;64(4):353–356. PMID: 9619120. doi:10.1055/s-2006-957450
8. LiverTox. RUCAM Causality Assessment. LiverTox; 2014.
9. Lee BS, Bhatia T, Chaya CT, Wen R, Taira MT, Lim BS. Autoimmune hepatitis associated with turmeric consumption. ACG Case Rep J. 2020;7(3):e00320. doi:10.14309/crj.0000000000000320
10. Funk J, Alfafara C, McEvoy S, Strom M, Lukefahr A. Turmeric dietary supplement-induced autoimmune hepatitis: a case report. FASEB J. 2017;31:lb354. doi:10.1096/fasebj.31.1_supplement.lb354
11. Menon VP, Sudheer AR. Antioxidant and anti-inflammatory properties of curcumin. Adv Exp Med Biol. 2007;595:105–125. PMID: 17569207. doi:10.1007/978-0-387-46401-5_3
12. Saadati S, Sadeghi A, Mansour A, et al. Curcumin and inflammation in non-alcoholic fatty liver disease: a randomized, placebo controlled clinical trial. BMC Gastroenterol. 2019;19(1):133. PMID: 31345163; PMCID: PMC6659284. doi:10.1186/s12876-019-1055-4
13. Lombardi N, Crescioli G, Maggini V, et al. Acute liver injury following turmeric use in Tuscany: an analysis of the Italian Phytovigilance database and systematic review of case reports. Br J Clin Pharmacol. 2021;87(3):741–753. PMID: 32656820. doi:10.1111/bcp.14460
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.