Back to Journals » Drug Design, Development and Therapy » Volume 20
Tumor Microenvironment-Responsive Smart Hydrogel: Engineering Next-Generation in situ Tumor Vaccines for Synergistic Tumor Immunotherapy
Received 3 April 2026
Accepted for publication 25 June 2026
Published 8 July 2026 Volume 2026:20 614384
DOI https://doi.org/10.2147/DDDT.S614384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Wenfeng He1,2, Wanlei Sun3
1Department of Medical Genetics, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 2Molecular Medicine of Jiangxi Key Laboratory, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 3Department of Clinical Laboratory, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China
Correspondence: Wanlei Sun, Email [email protected]
Abstract: Tumor vaccines represent a promising approach for tumor immunotherapy, yet their clinical translation is greatly impeded by cumbersome antigen screening, poor adaptation to tumor heterogeneity, inefficient antigen presentation, and insufficient immune activation. Tumor microenvironment (TME)-responsive smart hydrogels have emerged as advanced platforms for constructing next‑generation whole‑cell tumor vaccines, featuring tunable microstructures, spatiotemporally controlled cargo release, and excellent in situ TME adaptability. These hydrogel‑based vaccines directly employ intact tumor tissues as broad‑spectrum antigen reservoirs, avoiding complex antigen isolation and identification to effectively overcome tumor heterogeneity. Hydrogel‑based vaccines enable stimuli‑responsive sequential release of antigens, adjuvants, and bioactive factors, precisely modulating immune cascades to elicit robust systemic antitumor immunity against tumor growth, invasion, and metastasis. This review systematically summarizes the design principles, fabrication strategies, and immunomodulatory mechanisms of TME‑responsive hydrogel‑based whole‑cell vaccines, highlights their structure-efficacy relationships, and discusses key challenges in clinical translation. Furthermore, this review proposes future directions to guide the rational development of high‑performance immunotherapeutic formulation with strong clinical potential for personalized tumor treatment.
Keywords: tumor vaccines, smart hydrogel, stimuli‑responsive, antitumor immunity, whole‑cell vaccines
Introduction
Tumor remains a life-threatening disease that severely endangers human health and survival. Surgical resection, chemotherapy, and radiotherapy fail to fundamentally eradicate tumor cells, which often accompanied by high recurrence rates, distant metastasis, and severe systemic side effects in clinical practice, thus hardly meeting the requirement for curative treatment.1,2 In recent decades, tumor immunotherapy has revolutionized tumor treatment by activating and remodeling the host’s intrinsic immune system to achieve precisely recognition and long-term elimination of tumor cells, emerging as a next-generation therapeutic strategy complementary to traditional approaches.3 Among various immunotherapeutic modalities, tumor vaccines stand out for their unique capacity to induce tumor-specific immune responses and establish long-term immune memory, making them particularly promising for preventing tumor recurrence and metastasis.4
Tumor vaccines exert antitumor effects mainly by initiating innate immune sensing, promoting dendritic cells (DC) maturation, and activating CD8+ cytotoxic T cells and CD4+ helper T cells through major histocompatibility complex-I (MHC-I) and major histocompatibility complex-II (MHC-II) antigen presentation pathways, thereby establishing systemic adaptive immunity and immune surveillance.5,6 However, conventional tumor vaccines are predominantly designed based on single or few defined neoantigens, including peptide vaccines, genetic vaccines, and antibody-based vaccines. And these vaccines relies heavily on high-throughput sequencing and bioinformatic screening to identify effective targets.7 Unfortunately, the high heterogeneity and complexity of tumors lead to low accuracy and success rates of neoantigen identification. Moreover, clonal evolution during tumor progression further reduces the efficacy of neoantigen-based vaccines, resulting in narrow immune spectra and frequent immune escape.8 To address these limitations, in situ tumor vaccines prepared from inactivated autologous tumor tissues have been developed.9 These vaccines retain a full spectrum of tumor-associated antigens (TAAs) and multiple epitopes, enabling simultaneous presentation via both MHC-I and MHC-II pathways to activate comprehensive T cells responses.10–12 Despite these advantages, clinical translation of whole-cell vaccines severely restricted by short in vivo retention and rapid clearance, uncontrolled and burst antigen releasing, insufficient intrinsic adjuvanticity, limited DC cells recruitment and activation, and weak ability to reverse immunosuppression.13 These bottlenecks jointly lead to inadequate immune activation and poor therapeutic outcomes, hindering their clinical application.
To explore feasible therapeutic strategies, it is essential to elucidate the characteristics of tumor microenvironment (TME) and its impacts on tumor immunotherapy. Low pH, high glutathione (GSH) levels, overexpressed enzymes, hypoxia, and high reactive oxygen species (ROS) of the TME forms a strongly immunosuppressive niche to inhibit DC cells maturation, inactivate T cells, induce immune cell exhaustion, and promote the proliferation of regulatory T cells (Tregs) and tumor-associated macrophages (TAMs), which plays a decisive physiological and immunological role in tumor progression and therapeutic resistance.14,15 Specifically, acidic pH suppresses T cells, proliferation and cytokine secretion, high GSH scavenges ROS and reduces immunogenic cell death (ICD), overexpressed matrix metalloproteinases (MMPs) degrade extracellular matrix (ECM) to drive invasion and metastasis while further dampening anti-tumor immunity.16 These TME hallmarks not only promote tumor progression but also severely impair the efficacy of tumor vaccines. Given these issues, advanced delivery systems are urgently needed. Compared with liposomes, nanoparticles, micelles, and other delivery platforms suffered from rapid clearance, low loading efficiency, poor controllability, and limited immune-modulating effects.17 Hydrogel possesses unique superiority, (1) high porosity and loading capacity for co-delivering antigens, adjuvants, and functional factors. (2) Injectability and in situ gelation for localized implantation. (3) Prolonged retention to serve as stable antigen depots. (4) Excellent biocompatibility and biodegradability. (5) Precise responsiveness to TME stimuli for on-demand release, and the ability to reshape the immune microenvironment.18
TME-responsive hydrogel can intelligently respond to pathological signals in the TME to achieve spatiotemporally controlled release of antigens and adjuvants. They can establish localized immune-activating niches, enhance DC cells maturation and antigen cross-presentation, and boost T cells infiltration and function, thereby overcoming the core bottlenecks of conventional whole-cell vaccines.19,20 Accordingly, TME-responsive hydrogel-mediated in situ vaccines represent a promising strategy to develop next-generation personalized tumor vaccines. In this review, we systematically summarize the material design principles, fabrication strategies, immunomodulatory mechanism, and recent progress of TME-responsive hydrogel-based in situ tumor vaccines. We highlight the structure-activity relationships and discuss key challenges in clinical translation, aims to provide guidance for developing intelligent and efficient tumor immunotherapies.
Environment-Responsive Hydrogel-Based in situ Tumor Vaccines
Hydrogel-based in situ tumor vaccines have demonstrated substantial potential in improving antigen stability, extending local retention at the tumor sites, enabling controlled antigen release, and potentiating antitumor immune responses. However, the induction of potent and durable antitumor immunity depends on a well-orchestrated immune cascade, including tumor antigen release and recognition, efficient antigen uptake, draining of tumor antigens to lymph nodes, processing and presentation by DC cells, activation and proliferation of cytotoxicity CD8+ T cells, and then kill tumor cells (Figure 1).21 Notably, TME-triggered environment-responsive hydrogel-mediated in situ vaccines have attracted increasing attention, attributed to their superior capacity to spatiotemporally regulate vaccine release and robustly amplify antitumor immune responses by leveraging TME-associated stimuli.
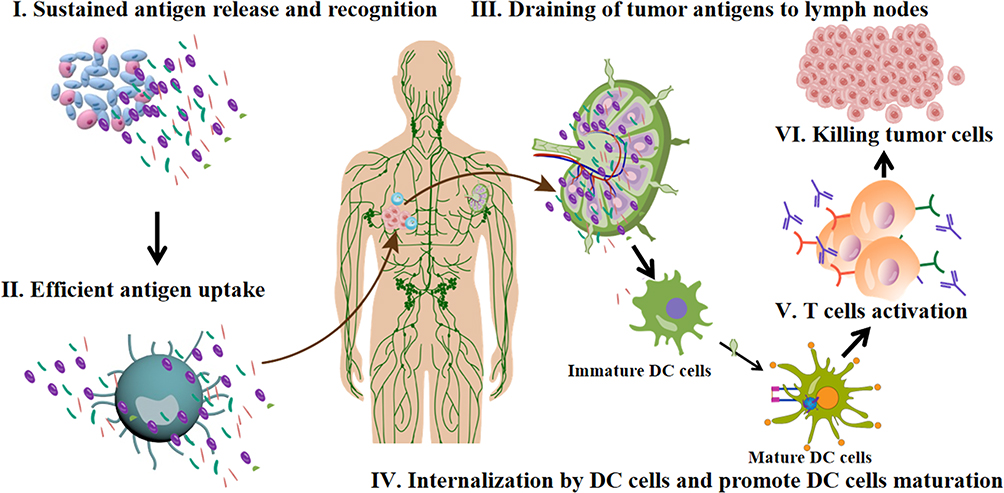 |
Figure 1 Schematic illustration of the systemic antitumor immune cascade activated by TME-responsive hydrogel-based in situ tumor vaccines. (I) The in situ vaccine hydrogel induces tumor ICD to achieve sustained release of TAAs and DAMPs at local tumor site. (II) Peripheral DC cells efficiently uptake the released TAAs and immunostimulatory mediators. (III) TAAs draining into lymph nodes. (IV) Internalized antigens and DAMPs facilitate intracellular antigen processing and promote phenotypic maturation of immature DC cells. (V) Mature DC cells with abundant surface MHC molecules and co-stimulatory signals present processed antigens to naive T lymphocytes to initiate robust T cell activation. (VI) Differentiated cytotoxic effector T cells home to primary and distal tumor lesions to specifically recognize and eradicate malignant tumor cells for systemic anti-tumor immune effect. |
pH-Responsive Hydrogel-Based in situ Tumor Vaccines
Extracellular acidification is a well-recognized hallmark of TME, with a pH value significantly lower than that of normal tissues. This acidic characteristic plays a critical role in promoting malignant progression, mediating immune evasion, and inducing therapeutic resistance.22 The Warburg effect is the primary driver of tumor acidosis, which indicates that tumor cells preferentially rely on aerobic glycolysis for rapid energy supply, accompanied by massive production of lactate and protons even under aerobic conditions.23 Meanwhile, defective tumor angiogenesis and impaired lymphatic drainage hinder the clearance of metabolic wastes, while overexpression of proton pumps and lactate transporters further extrudes acidic metabolites extracellularly, collectively leading to sustained TME acidification.24 Such an acidic TME not only reshapes tumor metabolism and invasiveness but also suppresses antitumor immunity, thus emerging as a pivotal target for precision tumor immunotherapy.
To harness TME acidity for enhanced whole-cell tumor vaccination, Li et al developed a pH-responsive chitosan-boronate ester hydrogel using nordihydroguaiaretic acid (NDGA) as both crosslinker and therapeutic agent. This hydrogel enables acidity-triggered drug release to induce ICD and activate antitumor immunity (Figure 2A).25 This NDGA hydrogel exhibits favorable injectability, self-healing ability, and tumor acidity-triggered controlled drug releasing. In a hepatocellular carcinoma model, the in situ releasing of NDGA from the hydrogel effectively induced ICD of tumor cells without additional ICD inducers, triggering the exposure of damage-associated molecular patterns (DAMPs) including calreticulin (CRT), adenosine triphosphate (ATP), and high mobility group box 1 (HMGB1). These DAMPs further promoted DC cells maturation and CD8+ T cells infiltration, ultimately activating systemic antitumor immunity.25 In contrast to traditional chemotherapeutic-loaded hydrogel that suffered from complex preparation and unsatisfactory controlled release, this design integrates drug and carrier into a single system, endowing the NDGA hydrogel with intrinsic immune-stimulating activity while simplifying fabrication, representing a promising engineering strategy for pH-responsive in situ tumor vaccines.
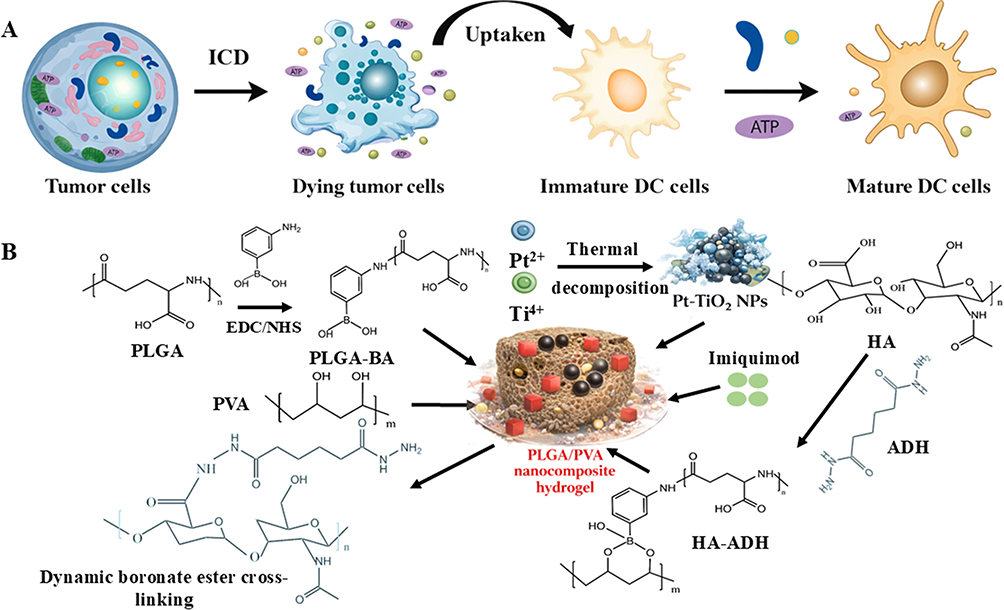 |
Figure 2 Schematic illustration of the construction and mechanism of the injectable nanocomposite hydrogel-based tumor immunotherapy system. (A) Tumor cells undergo ICD to release damage-associated molecular patterns, which are taken up by immature DC cells to promote their maturation and initiate subsequent antitumor immune responses. (B) Injectable pH-responsive PLGA/PVA hydrogel co-loaded with Pt-TiO2 sonosensitizer, IQ, and fluorescent probe for synergistic SDT-immunotherapy and real-time imaging of immunologically cold tumors. |
However, immunologically “cold” solid tumors typically exhibit poor immunogenicity, scarce T cells infiltration, and a profoundly immunosuppressive microenvironment, which collectively undermine the clinical efficacy of single-modal therapy.26 Conventional single-stimulus responsive delivery platform also fails to recapitulate the spatiotemporally complex immune regulatory cascades in vivo, limiting their ability to fully activate antitumor immunity.27 To address these limitations, multi-stimuli-responsive hydrogels have emerged as promising vehicles, which ascribed to their intelligent matrices enable sequential, on-demand release of antigens, adjuvants, and immunomodulators under multiple biological cues, thereby closely mimicking pathogen-elicited innate immune activation.27 Against this background, Qian et al constructed a pH-responsive injectable hydrogel co-loaded with sonosensitizer, immunoadjuvant, and fluorescent probe for synergistic SDT-immunotherapy and imaging (Figure 2B).28 Crosslinked via dynamic boronate ester linkages between boronic acid-modified polyglutamic acid (PLGA-BA) and polyvinyl alcohol (PVA), this hydrogel achieved pH-triggered drug releases in the acidic tumor milieu. Pt-TiO2 nanoparticles (NPs) acted as sonosensitizers to generate cytotoxic reactive oxygen species (ROS) under ultrasound irradiation, eliciting robust oxidative stress and apoptosis for potent sonodynamic therapy (SDT). The immunoadjuvant imiquimod (IQ) further potentiated adaptive antitumor immunity, while HA-ADH-RBITC enabled real-time tumor fluorescence imaging.29 This synergistic platform integrates SDT, immunotherapy, and noninvasive visualization, offers a powerful and translatable strategy for precision theranostics of immunologically cold tumors, which effectively complementing the limitation of single pH-responsive systems in remodeling immunosuppressive TME.
In summary, pH-responsive hydrogel-based in situ tumor vaccines offer distinct advantages for tumor immunotherapy, including tumor acidity-triggered on-demand drug release, efficient induction of ICD, and enhanced antitumor immune activation. These systems enable spatiotemporally controlled co-delivery of whole-cell derived antigens and adjuvants, reduce systemic toxicity, and showed great potential in converting “cold tumors” into “hot immunogenic tumors”. Nevertheless, most current single pH-responsive platforms are limited by their inability to fully mimic complex immune regulatory networks in vivo and achieve deep tumor penetration.30 Although multi-stimuli-responsive and theranostic designs have been explored, challenges remain in achieving sustained ICD, durable immune memory, and reliable clinical translation. Therefore, the development of optimized multifunctional pH-responsive hydrogel-mediated in situ vaccines, such as integrating pH responsiveness with other TME stimuli or combination therapies, holds significant promise for advancing next-generation tumor immunotherapy.
Redox-Responsive Hydrogel-Based in situ Tumor Vaccines
Dysregulated proliferation of tumor cells is accompanied by drastically accelerated metabolism, mitochondrial dysfunction, and excessive ROS production, which collectively maintain tumor tissues in a state of sustained oxidative stress.31 To counteract oxidative damage and support malignant progression, tumor cells upregulate biosynthetic pathways to overexpress GSH antioxidants. Hypoxic, acidic, and inflammatory cues within TME further drive GSH accumulation, resulting in intracellular GSH concentration far higher than those in normal tissues.32 This unique high GSH characteristic not only enhances tumor cells survival, therapeutic resistance, and immune evasion, but also provides a reliable endogenous stimulus for the rational design of redox-responsive drug delivery systems, particularly for in situ tumor vaccines that require precise spatiotemporal control over antigen releasing and immune activation.
Benefiting from this distinct tumor redox imbalance, GSH-responsive hydrogel-based platforms have emerged as promising vehicles for tumor-specific immunotherapy. Among these strategies, Pang et al developed a GSH-responsive photothermal gel vaccine (OA&PG/DOX&NA) via the redox reaction between potassium permanganate and oleic acid, enabling the co-delivery of doxorubicin (chemotherapeutic) and nattokinase (ECM-degrading enzyme) (Figure 3A).33 Following intratumoral injection, the MnO2-containing gel exerted dual functions, which acted as a catalase mimic to decompose H2O2 for TME hypoxia relief, and as an efficient photothermal agent under near-infrared (NIR) irradiation. Local hyperthermia above 45°C induced robust ICD of tumor cells, improved cell membrane permeability to promote drug uptake, and released whole-cell-derived TAAs and DAMPs. Meanwhile, Mn2+ released from GSH-triggered gel degradation directly activated the cyclic GMP-AMP synthase-stimulator of interferon genes (cGAS-STING) pathway, boosted DC cells maturation and antigen cross-presentation, and elicited strong CD8⁺ T cell mediated antitumor immunity.34 Furthermore, nattokinase released during gel degradation degraded the extracellular matrix (ECM), reduced tumor stiffness, and enhanced intratumoral perfusion, synergistically improving drug penetration and immune cell infiltration to suppress tumor recurrence and metastasis. This design fully leverages the GSH-responsive property to integrate chemo-photothermal therapy, ECM remodeling, and whole-cell vaccine-induced immunity, addressing key limitations of conventional whole-cell vaccines (Figure 3B).
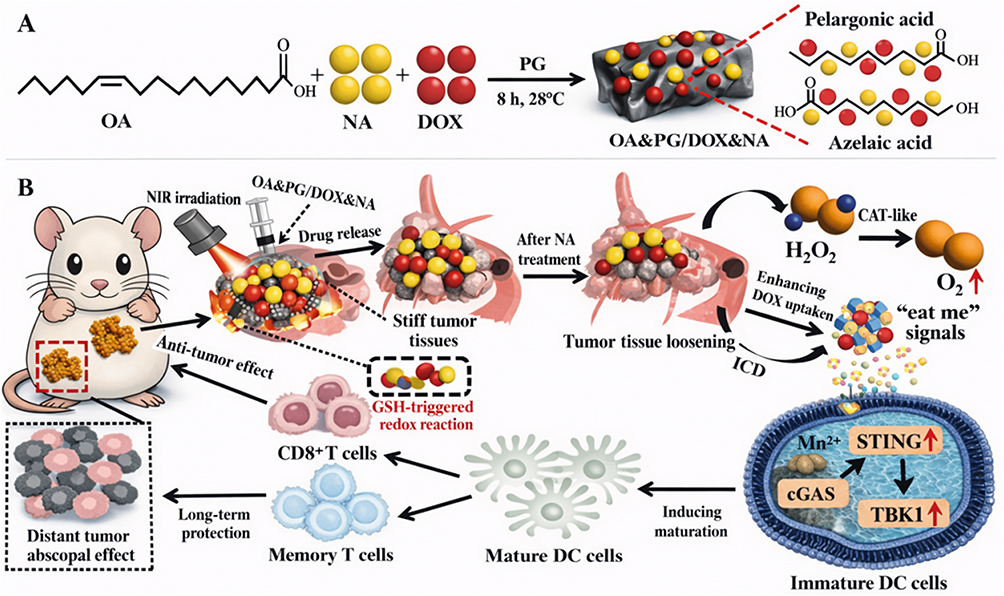 |
Figure 3 Schematic illustration of redox-responsive OA&PG/DOX&NA hydrogel for synergistic tumor chemo-immunotherapy. (A) Synthetic route of OA&PG/DOX&NA nanocomposite hydrogel assembled from OA, NA and DOX with pelargonic acid and azelaic acid as PG crosslinkers. (B) In vivo therapeutic cascade: Upon local NIR irradiation, implanted hydrogel enables on-demand drug release, NA remodels dense tumor extracellular matrix to loosen stiff tumor tissue and boost intracellular DOX uptake, which triggers ICD of tumor cells. Released Mn2+ further activates the cGAS–STING–TBK1 axis within immature DC cells to drive DC cells maturation, sequentially eliciting robust CD8⁺ cytotoxic T cell response and memory T cell formation for primary tumor regression and long-term abscopal anti-tumor efficacy against distant metastatic lesions. Symbol definition: Red upward arrows represent the upregulation/activation of corresponding protein expression or biological pathways; gray dashed boxes mark the core hydrogel nanoparticle region for GSH-responsive redox-triggered drug release. |
Despite the remarkable efficacy of photothermal therapy (PTT), excessive local heating may cause unintended damage to surround normal tissues and limit its clinical applicability.35 To address this issue, ultrasound-based strategies have been explored as a milder alternative to induce ROS dependent tumor cell apoptosis and establish an intratumoral antigen reservoir for whole-cell vaccination. In this regard, Lin et al proposed an injectable carboxymethyl chitosan-oxidized dextran (CMCS-ODEX) hydrogel system co-loading metal-organic framework (MOF)-derived sonosensitizer PCN-224@MnO2@HA (PMH) and antifibrotic agent specific inhibitor of smad 3 (SIS3) for osteosarcoma treatment.36 The MnO2 component in PMH specifically consumed intracellular GSH to disrupt redox homeostasis and alleviate TME hypoxia, thereby amplifying ROS generation and enhancing ICD under ultrasound-mediated SDT. Simultaneously, SIS3 inhibited the TGF-β/SMAD3 pathway to reprogram cancer-associated fibroblasts (CAFs), remodel the tumor stroma, reduce ECM deposition and stiffness, and facilitate T cells infiltration. With sustained local release and favorable biocompatibility, CMCS-ODEX hydrogel system integrated GSH depletion enhanced SDT, CAF reprogramming, and whole-cell antigen presentation, which effectively reverses the immunosuppressive TME and inhibiting tumor growth in vivo. This work highlights the advantage of GSH-responsive hydrogels in synergizes mild physical therapy with whole-cell tumor vaccination, overcoming the bottleneck of single-modal therapies in remodeling TME and activating systemic immunity.
Collectively, GSH-responsive hydrogels represent a versatile and intelligent platform for the development of high-performance in situ tumor vaccines. By exploiting the elevated GSH levels in TME, these hydrogels undergo redox-triggered degradation via disulfide bonds or other redox-labile linkages, enabling controlled and sustained release of whole-cell derived TAAs and immunomodulatory adjuvants.37 The three-dimensional hydrogel network acts as a localized antigen depot, prolonging antigen retention and presentation to promote DC cells maturation and activation. Moreover, GSH depletion by these hydrogels disrupts intracellular redox homeostasis, potentiates ICD, and reverses TME immunosuppression, synergistically enhancing CD8+ T cells responses and establishing long-term immune memory. With excellent biocompatibility, tumor specificity, and on-demand degradability, such hydrogel system provides a safe and efficient strategy for constructing redox-sensitive in situ tumor vaccines, highlight their enormous potential in personalized tumor immunotherapy that overcomes tumor heterogeneity and immune escape.
Enzyme-Responsive Hydrogel-Based in situ Tumor Vaccines
Significantly elevated expression of MMPs, cathepsins, and other proteases is a key hallmark of TME.38 Chronic inflammation, hypoxia, acidic conditions, and aberrant signaling pathways jointly promoting the secretion and activation of these proteases by tumor cells, CAFs, and infiltrating immune cells. These proteases mediate ECM degradation, facilitating tumor invasion and metastasis, and aggravating immunosuppression, thus playing critical roles in malignant progression.39 Importantly, this characteristic overexpression provides an ideal endogenous stimulus for designing intelligent enzyme-responsive drug delivery systems, particularly for in situ tumor vaccines that require site-specific antigen releasing, and TME remodeling to enhance immunogenicity.
Against this background, Tian et al (Figure 4A) developed an injectable MMP-2-responsive hydrogel self-crosslinked from gelatin, oxidized sodium alginate, and borax, which co-loaded DOX and anti-TIGIT monoclonal antibody (immune checkpoint inhibitor).40 Driven by highly expressed MMP-2 in the TME, the hydrogel enabled sequential and controlled release of the two payloads. Specifically, DOX induced robust ICD of tumor cells, releasing whole-cell-derived TAAs and DAMPs, while promoting the infiltration of natural killer (NK) cells and effector T cells. The anti-TIGIT antibody further reversed immune cells exhaustion and synergistically activated innate and adaptive immunity. In the poorly immunogenic 4T1 breast tumor model, this strategy successfully overcame critical limitation of conventional whole-cell vaccines, including insufficient neoantigen exposure, limited immune infiltration, and immune cell dysfunction, which markedly suppressing primary tumor growth and distant metastasis, and eliciting long-term immune memory. This work highlights the value of MMP-2-responsive hydrogel in integrating chemoimmunotherapy with whole-cell vaccine-induced immunity, providing a clinically translatable strategy for safe and efficient local tumor immunotherapy.
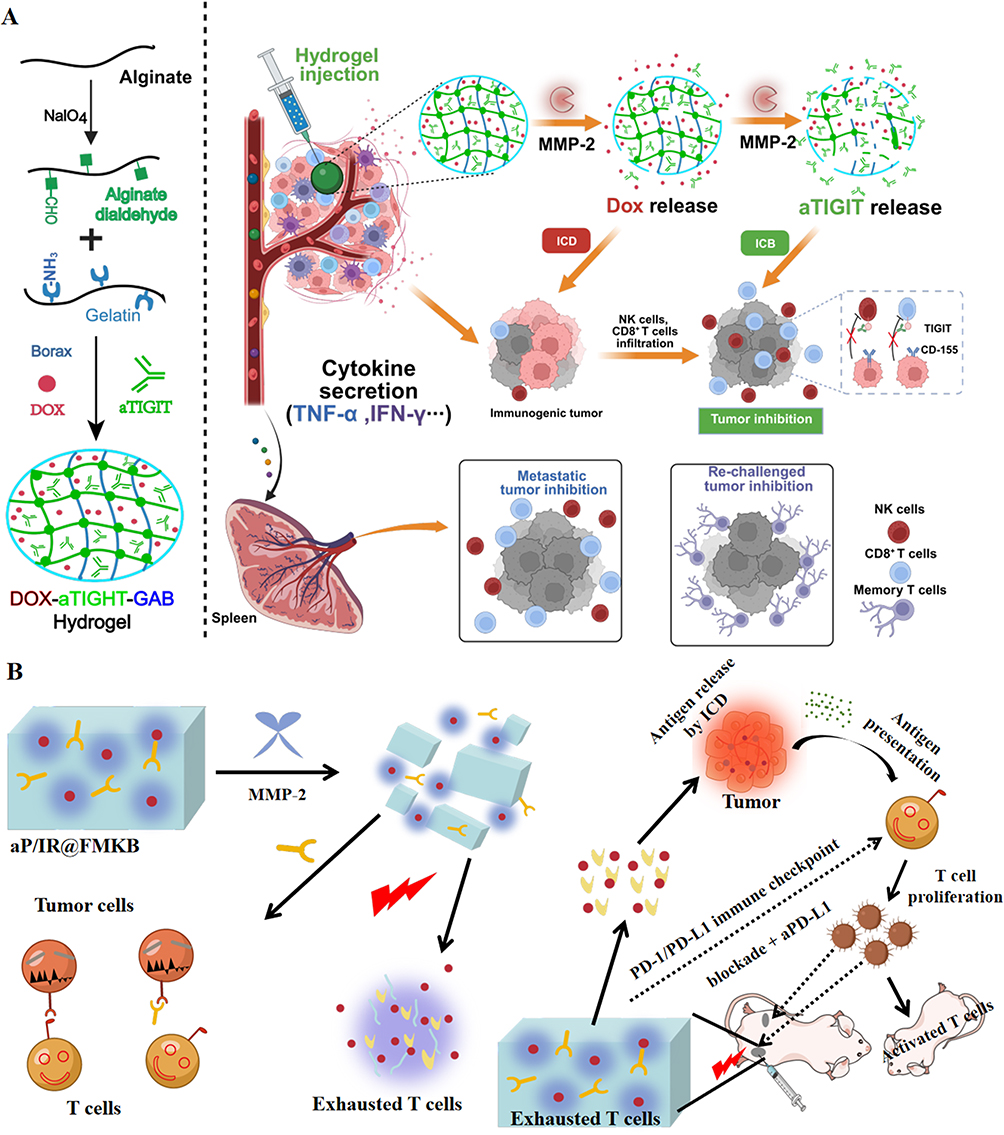 |
Figure 4 Schematic illustration of MMP-2-responsive hydrogel platforms for synergistic chemo-immunotherapy. (A) MMP-2-responsive DOX-αTIGIT hydrogel achieves sequential drug release to induce ICD, block TIGIT checkpoint, and activate NK cells and T cells for breast cancer inhibition. (B) MMP-2-responsive polypeptide hydrogel (aP/IR@FMKB) enables deep tumor penetration, ICD induction, PD-L1 blockade, and amplified systemic antitumor immunity. Symbol definition: Red lightning bolt symbols denote photothermal treatment triggered by the hydrogel system. |
The high complexity of the immune TME and aberrant activation of proliferation-related signaling pathways in tumor and immune cells frequently lead to therapeutic resistance against monotherapy, ultimately resulting in tumor recurrence and clinical failure.41 Therefore, combination therapy that maximizes efficacy through multimodal synergy has become a promising strategy for tumor treatment. To improve tumor penetration and enhance ICD induced whole-cell vaccination, Zhang et al first developed trimethyl chitosan (TMC)-bufalin nanoparticles (TB NPs) by encapsulating bufalin (BF) into TMC-based NPs.42 However, TB NPs are still restricted by the highly immunosuppressive TME, failing to fully exert their potential in inducing ICD and activating antitumor immunity. Accordingly, the group further constructed an intelligent MMP-2 responsive polypeptide hydrogel nanoplatform (aP/IR@FMKB) by covalently conjugating an MMP-2 sensitive peptide with a tumor-penetrating peptide, achieving co-delivery of TB NPs, the photothermal agent IR820, and the immune checkpoint inhibitor aPD-L1 via polypeptide self-assembly.42 This aP/IR@FMKB platform enables deep tumor penetration, MMP-2 triggered responsive drug release, and effective integration of ICD effects (from BF and IR820-mediated photothermal therapy), PD-1/PD-L1 blockade, and whole-cell antigen presentation, precisely remodeling the immunosuppressive TME to amplify systemic antitumor immunity (Figure 4B).
Collectively, highly expressed MMPs and cathepsins in TME provide ideal endogenous stimuli for constructing intelligent enzyme-responsive delivery systems. Enzyme-responsive hydrogels enable specific degradation at tumor sites, achieving precise and sequential release of whole-cell antigens, chemotherapeutics, photosensitizers, and immune checkpoint inhibitors, effectively elevating local drug concentration while reducing systemic toxicity. By inducing ICD, activating NK cells and T cells, and reversing the immunosuppressive TME, these hydrogel systems exert multimodal synergistic antitumor effects. In poorly immunogenic tumors, enzyme-responsive hydrogels exhibit distinct superiorities in deep tumor penetration, long-term local retention, and synergistic enhancement of whole-cell vaccines efficacy, offering a promising direction for developing effective and translatable tumor immunotherapy strategies that overcome tumor heterogeneity and immune escape.
Photothermal-Responsive Hydrogel-Based in situ Tumor Vaccines
PTT emerged as a highly promising strategy for tumor treatment due to its precise targeting, minimal invasiveness, and reduced damage to normal tissues. When combined with photodynamic therapy (PDT), this modality exhibits synergistic immunomodulatory effects, photothermal effects can directly ICD of tumor cells to activate adaptive immune responses against TAAs, while PDT upregulates “eat-me” signals (calreticulin) on dying cells, collectively promoting the recognition and phagocytosis of tumor antigens by DC cells to initiate systemic antitumor immunity.43,44 Hydrogel-based PTT system serves as ideal platforms for in situ tumor vaccines, as they can efficiently induce tumor cell apoptosis, construct in-situ “antigen reservoirs” within tumors, and provide sustained and stable release of whole-cell-derived TAAs, offering a novel approach to address the limitation of conventional whole-cell vaccines such as uncontrolled antigen release and insufficient immune activation.45
The rational design and screening of photothermal agents with high photothermal conversion efficiency are pivotal prerequisites for fabricating high-performance photo-responsive hydrogels.46 Polydopamine nanoparticles (PDA NPs) exhibit broad-spectrum light absorption, efficient photon-to-thermal energy conversion, outstanding biocompatibility, and facile scalable synthesis, which rendering them highly promising photothermal candidates for intelligent hydrogel systems.46 Leveraging these merits, Fang et al fabricated a cascade immune-activating composite hydrogel (M/P-PDA@IQ PHA) as an in-situ in situ tumor vaccines.47 This hydrogel was constructed by crosslinking polyvinyl alcohol-modified PDA nanoassemblies (P-PDA@IQ NPs) with phenylboronic acid-modified hyaluronic acid (PHA) via boronate ester bonds. The P-PDA@IQ NPs were loaded with the TLR7 agonist imiquimod and functionalized with mannose for targeted DC cells delivery. Under NIR irradiation, M/P-PDA@IQ PHA exhibited efficient photothermal conversion to induce tumor photothermal ablation and ICD, releasing whole-cell-derived TAAs to form an in-situ antigen reservoir that alleviates tumor heterogeneity. Meanwhile, the acidic, high ROS, and high GSH of TME can cleave boronate ester bonds to trigger hydrogel degradation, releasing M/P-PDA@IQ NPs. These nanoadjuvants released IQ to reverse immunosuppression, captured TAAs, and targeted lymph nodes, promoting DC cells maturation and antigen cross-presentation via mannose receptor-mediated endocytosis, and ultimately activating CD8+ T cells and CD4+ T cells to elicit robust and long-term antitumor immunity.47 This work highlights the value of PDA-based photothermal hydrogels in integrating in-situ whole-cell vaccination with immune adjuvant delivery, synergistically enhancing antitumor immunity.
However, hydrogel-mediated in situ vaccines relying solely on PTT still exhibit limited efficacy against most solid tumors, primarily due to the highly immunosuppressive and physically dense TME.48 Current strategies mostly focus on biochemical modulation of tumors, while the physical barriers imposed by ECM are largely overlooked. ECM rich in collagen, hyaluronic acid (HA), and elastin increases tumor stiffness and interstitial fluid pressure, compressing tumor vessels, impairing perfusion, and blocking drug/immune cell infiltration.48 Moreover, negatively charged ECM components hinder the penetration of charged nanomedicines, and the collagen network forms a physical shield that protects tumor cells from immune attack. To address these obstacles, Ji et al developed a TME-responsive nattokinase-delivering hydrogel (NS/FPDA@DOX HA) for synergistic physical barrier disruption and whole-cell vaccination (Figure 5A).49 After intratumoral injection, acidic pH, high GSH, and high H2O2 levels in the TME triggered boronate ester cleavage and hydrogel degradation, releasing nattokinase and folate-modified FPDA@DOX NPs. Nattokinase degraded fibronectin in the ECM, loosening the dense matrix, reducing tumor stiffness, and overcoming physical barriers to enhance drug/immune cell infiltration. Meanwhile, FPDA@DOX specifically targeted tumor cells, released DOX in acidic endosomes for precise chemotherapy, and induced ICD under NIR irradiation, promoting DC cells maturation, activating CD8+ T cells and CD4+ T cells, and efficiently inhibiting tumor growth, metastasis, and recurrence. This strategy integrates PPT, chemotherapy, ECM remodeling, and whole-cell vaccination, providing a multifunctional solution to overcome both physical and immune barriers of solid tumors.
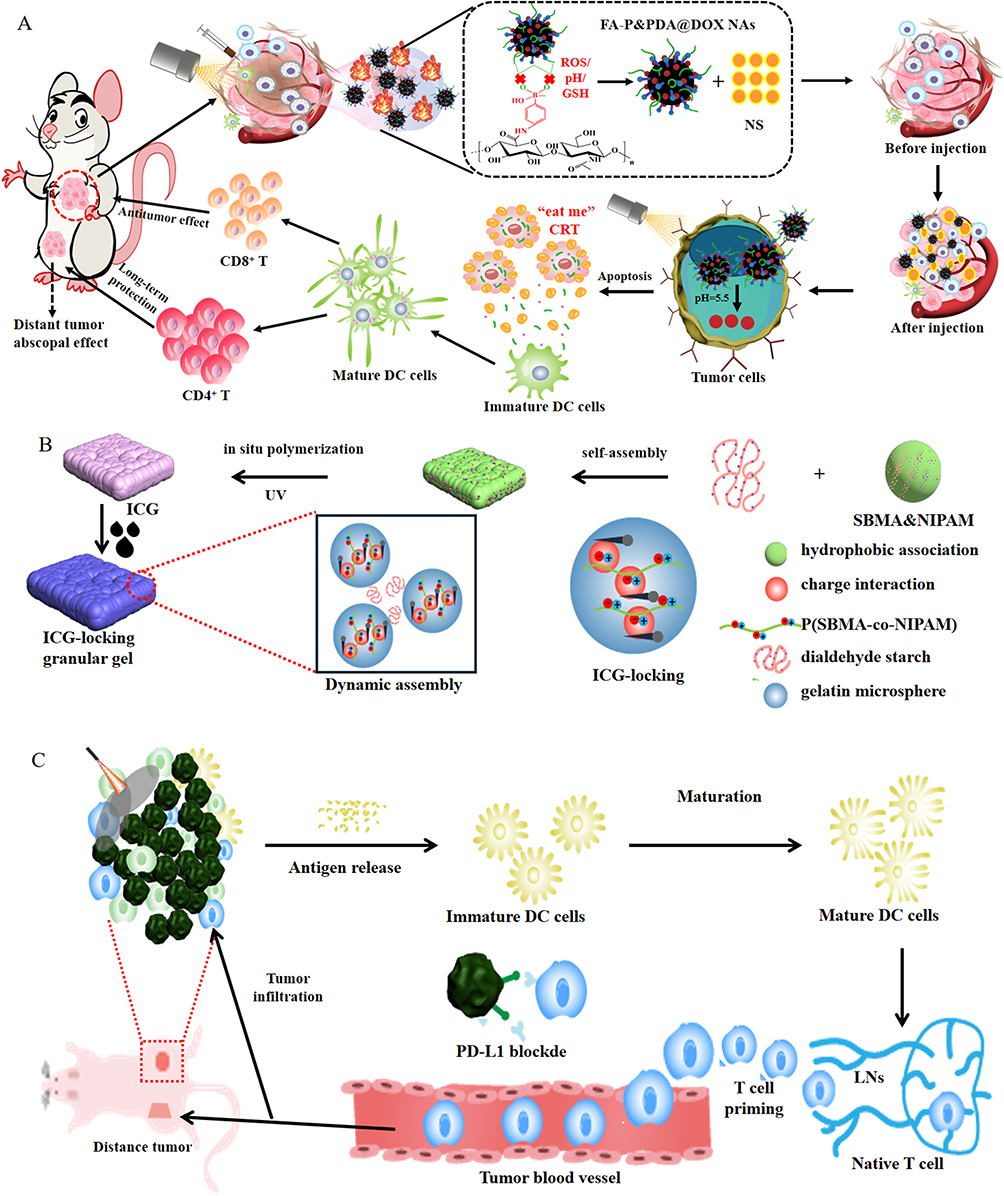 |
Figure 5 Schematic illustrations of photothermal-responsive hydrogel systems for in situ vaccination. (A) TME-responsive nattokinase-loaded hydrogel degrades ECM, releases FPDA@DOX, induces ICD, and promotes DC cells maturation and T cells infiltration. (B) Fabrication of ICG-loaded granular hydrogel via interpenetrating polymer networks for stable photothermal therapy. (C) Hydrogel-based in situ vaccine combined with anti-PD-L1 for postsurgical tumor elimination and metastasis prevention. Symbol definition: Black dashed ovals in (A) denotes the inner nanostructural composition of NS/FPDA@DOX HA. Red filled circles in (B) denotes the inner nanostructural composition of ICG-loaded granular hydrogel. Red dashed box in (C) highlights the abscopal distant tumor site receiving systemic immune-mediated therapeutic effect. |
Indocyanine green (ICG), a clinically approved photosensitizer with favorable biosafety and bioavailability, has also been widely adopted for fabricating photo-responsive hydrogels. Zeting et al established a granular hydrogel system composed of gelatin microgels interpenetrated with in-situ polymerized poly(sulfobetaine methacrylate-co-N-isopropylacrylamide) (P(SBMA-co-NIPAM)) for stable ICG encapsulation in colorectal cancer treatment.50 The zwitterionic copolymer P (SBMA-co-NIPAM) enabled high retention of water-soluble ICG, avoiding rapid diffusion/clearance to guarantee sustained PTT (Figure 5B). This ICG-loaded granular hydrogel exhibits good tissue adhesion, tightly attaching to wet surgical sites in vivo. When combined with anti-PD-L1 immune checkpoint blockade, hydrogel-mediated PTT effectively eliminated residual/metastatic tumor lesions after surgery and prevented long-term recurrence. Mechanistically, the combination therapy promotes DC cells maturation in lymph nodes, enhanced intratumoral infiltration of CD8+ T cells, and elevated CD4+ T cells populations in the spleen, triggering robust systemic antitumor immunity. Thus, this ICG-based granular hydrogel represents a promising PTT strategy for postoperative whole-cell vaccination and recurrence prevention (Figure 5C).
In summary, photothermal-responsive hydrogel-mediated in situ vaccines possess dual advantages of local phototherapy and systemic immunotherapy, selectively kill tumor cells to form in-situ antigen reservoirs, prolong antigen retention, and continuously activate antigen-presenting cells, showing great potential in inhibiting tumor growth and eliminating micrometastases. Nevertheless, these systems still face inherent limitations: (1) NIR light has a limited tissue penetration depth (typically 1–5 cm), making it difficult to achieve sufficient ablation of deep-seated or large-volume tumors, leading to incomplete treatment.51 (2) Some tumor cells exhibit strong thermotolerance, and photothermal effects can induce heat shock protein upregulation, pushing tumors into a protective stress state that lays the foundation for recurrence.52 (3) The targeting and accumulation efficiency of photothermal agents need improvement, as non-specific distribution may cause phototoxic damage to normal tissues.53 In the future, rational integration of ECM degradation, targeted delivery, multi-stimuli-responsive release, and immune activation is expected to develop intelligent light-responsive hydrogel-mediated in situ vaccines with high penetration, precise targeting, and strong immune-modulating capacity, breaking through the physical and immune barriers of solid tumors and providing novel strategies for effective and safe individualized tumor immunotherapy.
Ultrasonic-Responsive Hydrogel-Based in situ Tumor Vaccines
Following the discussion of photothermal-responsive hydrogels, ultrasonic-responsive in situ hydrogel-anchored whole-cell vaccines have emerged as a more clinically translatable alternative for deep-seated tumors, which addressing the critical limitation of NIR light’s shallow tissue penetration.54 Compared with NIR mediated PTT, ultrasound exhibits superior deep tissue penetration (up to 10 cm), excellent spatiotemporal controllability, and real-time imaging guidance, enabling precise ablation of deep lesions with minimal damage to adjacent normal tissues.55 By adjusting ultrasonic intensity, frequency, and focal zone, personalized precision tumor therapy can be achieved. SDT, the core mechanism of this platform, relies on tumor-specific accumulation and prolonged retention of sonosensitizers to generate abundant ROS, inducing oxidative stress and tumor cell apoptosis via ultrasonic cavitation, ROS mediated intracellular damage, and direct apoptotic pathways.56 Importantly, SDT triggers ICD to promote the release of DAMPs and TAAs, enhances DC cells maturation and antigen presentation, and activates effector T cells to elicit systemic antitumor immunity against primary tumors and distant metastases.57 By integrating these advantages, ultrasonic-responsive in situ hydrogels enable localized delivery and sustained release of sonosensitizers, whole-cell-derived TAAs, and immunomodulators, synergizing deep tumor ablation, in situ antigen release, and systemic immune activation to reduce systemic toxicity and enhance therapeutic efficacy for primary and metastatic tumors. This noninvasive, personalized strategy holds great promise for clinically translatable tumor immunotherapy.
To address the critical limitations of conventional endogenous tumor vaccines (transient antigen release and lack of multifunctional immune adjuvants), Guo et al developed an injectable all-in-one alginate-manganese-chlorin e6 (ALG-Mn-Ce6) hydrogel system for ultrasonic-responsive whole-cell vaccination (Figure 6A).58 This hydrogel forms a three-dimensional network via ionic crosslinking between sodium alginate and divalent manganese ions (Mn2+), with the sonosensitizer Ce6 encapsulated in the gel matrix. Upon ultrasound irradiation, Ce6 mediated SDT and Mn2+-mediated chemodynamic therapy synergistically generate abundant ROS, inducing ICD of tumor cells and promoting DAMP release to facilitate DC cells maturation. Meanwhile, Mn2+ acts as a potent immune adjuvant to directly activate the cGAS-STING pathway, promote type I interferon secretion, and enhance T cell-mediated antitumor immune responses. Furthermore, the paramagnetic property of Mn2+ enables real-time magnetic resonance imaging monitoring of drug release at the tumor site. In vivo studies demonstrated that the ultrasound-triggered ALG-Mn-Ce6 hydrogel effectively activates endogenous whole-cell vaccination, markedly suppresses primary tumor growth and metastasis, and reduces tumor recurrence. Featuring facile preparation, low cost, good scalability, favorable injectability, and excellent biosafety, this hydrogel holds great promise for clinical translation in precision immunotherapy against colorectal tumor.
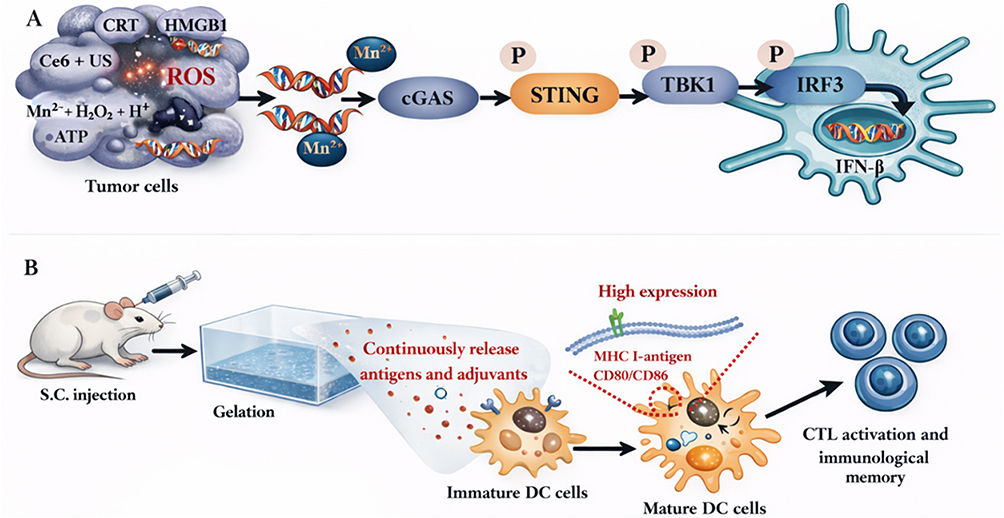 |
Figure 6 Schematic of ultrasound-responsive hydrogel-mediated in situ vaccination and cGAS-STING activation. (A) ALG-Mn-Ce6 hydrogel generates ROS under ultrasound to induce ICD, releases Mn2+ to activate cGAS-STING pathway, and boosts type I interferon secretion for colorectal tumor immunotherapy. (B) Biomembrane-based hydrogel vaccine releases tumor cell membrane antigens and E64 to enhance antigen cross-presentation, driving DC cells maturation and long-term CD8⁺ T cell-mediated immune protection. Red dashed circles in (B) denotes the intracellular antigen MHC-I complex and co-stimulatory molecules (CD80/CD86) highly expressed on mature DC cells surface after antigen uptake. |
Beyond SDT-mediated ICD induction, ultrasonic-responsive hydrogels can also be engineered to optimize whole-cell antigen presentation. Accumulating evidence shows that bacterial outer membrane vesicles (OMVs) retain lipopolysaccharides and lipoproteins from parental bacteria, which activate toll-like receptor 4 and toll-like receptor 2 signaling to promote DC cells maturation, which serving as highly promising immune adjuvants.59 Additionally, the cysteine protease inhibitor E64 can significantly suppress lysosomal degradation of TAAs to enhance antigen cross-presentation.60 Leveraging these insights, Nie et al developed an injectable biomembrane-based hydrogel as a single-shot prophylactic in situ tumor vaccines for comprehensive and durable CD8+ T cells activation (Figure 6B).60 Tumor cell membranes (TCMs) and OMVs were fused into a hybrid cell membrane (HCM) that serves as both a broad-spectrum source of tumor-specific antigens and an immune booster to stimulate DC cells maturation. To enhance DC cells targeting, DSPE-PEG-mannose was incorporated into HCM to generate mannose-modified HCM (MHCM), which specifically binds to mannose receptors on DC cells. MHCM was further modified with oxidized sodium alginate (OSA) to yield the gellable precursor O-MHCM, which rapidly undergoes in situ gelation subcutaneously upon reaction with calcium ions under physiological conditions. Following subcutaneous co-administration of E64 and O-MHCM, the E64@O-MHCM hydrogel was instantly formed with O-MHCM as the crosslinked framework and E64 encapsulated within the porous network. Benefiting from the sustained degradation of OSA, MHCM and E64 were released in a controlled and persistent manner after a single vaccination. The released MHCM efficiently targeted DC cells and promoted their maturation via TCM derived antigens and OMV-mediated adjuvant effects, while E64 inhibited lysosomal degradation of tumor-specific antigens to facilitate efficient antigen cross-presentation and cytotoxic T lymphocyte activation. Consequently, this hydrogel triggered strong and durable T lymphocyte-mediated immune responses, effectively preventing 4T1 breast tumorigenesis with just one dose.
In summary, ultrasonic-responsive in situ hydrogel-mediated in situ vaccines exhibit superior clinical translation potential for deep-seated tumors compared with NIR mediated PTT, owing to ultrasound’s deep tissue penetration, precise spatiotemporal control, and real-time imaging guidance. These platforms integrate SDT with localized controlled release of whole-cell antigens and immunomodulators, enabling deep tumor ablation, in situ antigen reservoir formation, and systemic immune activation. By inducing ICD, promoting DC cells maturation, and activating effector T cells against primary tumors and metastases, ultrasonic-responsive hydrogels represent a promising noninvasive, personalized strategy for clinically translatable tumor immunotherapy, which complementing the strengths of other environment-responsive hydrogel systems discussed earlier.
Reviews and Prospects
Environment-responsive hydrogels have evolved from passive antigen carriers to active immune-regulatory reservoirs that reshape the local immune microenvironment, promoting the recruitment, maturation, and activation of antigen-presenting cells. By sustaining antigen retention and presentation, these hydrogels enhance DC cells maturation, T cells activation, and long-term immune memory formation, addressing the key limitations of conventional in situ tumor vaccines. The co-delivery of immunoadjuvants, targeting ligands, and cytokines enables the seamless integration of antigen delivery, immune activation, and TME modulation, effectively reversing immunosuppression and amplifying antitumor immune responses. Above all, hydrogel-mediated in situ vaccines have demonstrated potent antitumor activity across diverse applications, including primary tumor therapy, postoperative anti-recurrence, anti-metastasis, combination immunotherapy, and personalized vaccination.61 By forming long-term immune depots at the tumor site, these systems delay antigen clearance, increase lymphocyte infiltration, and convert “cold tumor” to “hot tumor”, ultimately suppressing tumor growth and prolonging survival.
Notably, hydrogel-mediated in situ vaccines exhibit exceptional translational potential for addressing postoperative minimal residual disease and distant metastasis. Minimally invasive injectable into the tumor cavity, they not only eliminate residual tumor cells but also sustain to release in situ-released tumor antigens and adjuvants, which triggering systemic antitumor immunity by inducing effector T cells and memory T cells that target circulating tumor cells and distant micrometastases.62 Meanwhile, the favorable biocompatibility, viscoelasticity, and self-healing properties of hydrogels support tissue repairing and wound healing, integrating tumor immunotherapy with tissue regeneration, a unique advantage unattainable by traditional therapeutic modalities. To further enhance efficacy, combinations with immune checkpoint inhibitors achieve synergistic effects by reversing T cells exhaustion, while local sustained co-delivery minimizes systemic toxicity and off-target effects. Besides, personalized hydrogel vaccines fabricated using autologous tumor antigens can be rapidly prepared without complex antigen synthesis or identification, efficiently overcoming tumor heterogeneity and enabling convenient precision immunotherapy.63 Mechanistically, hydrogels stabilize antigens, promoting innate immune cell infiltration, and facilitate antigen presentation via both MHC-I and MHC-II pathways, activating CD8+ T cells and CD4+ T cells.64 Sustained antigen release enhances cross-presentation and tumor killing, while memory T cells establish long-term immune surveillance to prevent tumor recurrence. Endowed with excellent injectability, in situ gelation, high porosity, stimuli-responsive release, and biocompatibility, hydrogel-mediated in situ vaccines represent a highly translatable platform for clinical tumor immunotherapy.
Despite the promising preclinical antitumor efficacy, the clinical translation of TME‑responsive hydrogel‑based whole‑cell tumor vaccines severely restricted by numerous inherent limitations and deficiencies, which have not been systematically discussed in most current studies. (1) Most hydrogel systems rely on single‑stimulus responsiveness, which cannot fully adapt to the highly heterogeneous, dynamic, and complex TME, leading to unstable, untimely, or non‑specific antigen release. (2) The poor deep‑tissue penetration of photothermal/photodynamic hydrogels greatly restricts their applications in deep‑seated solid tumors. (3) Precise control over in vivo degradation kinetics remains difficult, which may cause mismatched release profiles, local inflammation, or long‑term retention. (4) The lack of standardized preparation, scalable production, and quality control hinders large‑scale clinical translation. (5) The in vivo immune regulatory mechanisms and cascade networks induced by hydrogel vaccines remain largely unclear, especially the crosstalk between material properties and immune cell fate. (6) Most studies are limited to preclinical animal models, long‑term biosafety evaluations and clinical trials are still insufficient. (7) High inter‑ and intra‑tumor heterogeneity leads to unstable therapeutic efficacy and poor reproducibility. These key deficiencies must be fully addressed before the widespread clinical application of such vaccine systems.65
To address these bottlenecks, future research efforts should focus on three core directions. Firstly, the development of intelligent multi-stimuli-responsive hydrogel platforms with enhanced biocompatibility, precisely controlled releasing, and adaptive TME remodeling capabilities. Secondly, in-depth mechanistic studies using advanced bioinformatics and single-cell sequencing technologies to delineate vaccines-induced immune networks, including antigen-presenting cells activation, T cells differentiation, and immune memory formation. Thirdly, the rational integration of antigen delivery, immune activation, TME remodeling, and combination immunotherapy to achieve synergistic antitumor effects.
The therapeutic performance of hydrogel-mediated in situ vaccines largely governed by the structure-activity relationship linking hydrogel physicochemical properties, stimuli-responsive characteristics, and immune modulation efficacy.66 Microstructural features, such as porosity and crosslinking density, directly regulate immune cell infiltration, antigen diffusion, and release kinetics, which highlighting the importance of a balanced porous structure and crosslinking degree for sustained antigen presentation and durable immune activation.67 Different stimuli-responsive mechanisms enable site-specific and on-demand cargo release, while multi-stimuli responsive systems further mimic physiological immune cascades and amplify antitumor immunity by integrating multiple TME cues.68 Biodegradability and biocompatibility are critical for clinical safety, requiring a careful balance between natural polymers and synthetic polymers to optimize degradation rates and reduce immunogenicity. Moreover, hydrogel surface charge, wettability, and mechanical stiffness actively regulate immune cells adhesion, antigen uptake, and DC cells maturation, thereby shaping both innate and adaptive immune responses. Collectively, rational design based on a deep understanding of hydrogel structure-performance-immunity relationships will guide the development of next-generation in situ tumor vaccines with high potency, specificity, and translational potential.
Environment-responsive hydrogel based in situ tumor vaccines provide a highly innovative and promising strategy for overcoming tumor heterogeneity, enhancing vaccine immunogenicity, and advancing personalized precision tumor immunotherapy, which leveraging their unique structural advantages and potent immune-modulating capacity. Although several critical challenges remain to be addressed, continuous optimization toward intelligent, multifunctional, and translation-oriented design, coupled with in-depth elucidation of structure-performance-immunity relationships, is expected to drive significant theoretical and technological innovations. With the interdisciplinary integration of materials science, tumor immunology, and clinical medicine, these hydrogel-based vaccine systems will ultimately open new avenues for tackling postoperative recurrence and metastasis, improving the comprehensive therapeutic efficacy of malignant tumors, and offering safer, more effective, and personalized tools for clinical tumor immunotherapy.
Conclusion
In summary, TME-responsive hydrogels have emerged as a versatile and powerful platform for constructing next-generation in situ tumor vaccines, which effectively addressed the bottlenecks of single antigen sources, poor adaptability to tumor heterogeneity, inefficient antigen presentation, and insufficient immune activation. These intelligent hydrogel systems rely on distinct responsive mechanisms to achieve spatiotemporally controlled release of therapeutic agents, thereby inducing ICD in situ and establishing endogenous antigen reservoirs without ex vivo cells loading. pH-responsive hydrogels exploit the acidic TME to trigger on-demand payload release, efficiently inducing ICD and promoting DC cells maturation to convert “cold tumor” into immunologically “hot tumor”. Redox-responsive hydrogels target the high glutathione level in tumors to achieve controlled degradation, disrupting intracellular redox homeostasis, activating the cGAS-STING pathway, and enhancing CD8⁺ T cell-mediated antitumor immunity. Enzyme-responsive hydrogels take advantage of overexpressed proteases such as MMP-2 in TME to realize site-specific and sequential drug release, deep tumor penetration, and synergistic chemo-immunotherapy. PTT-responsive hydrogels convert near-infrared light into local heat to induce tumor ablation and ICD, while remodeling extracellular matrix to improve immune cell infiltration. Ultrasound-responsive hydrogels enable deep-tissue penetration and precise spatiotemporal control, triggering robust SDT-induced ICD and systemic antitumor immune responses with excellent clinical translation potential. Collectively, these hydrogel-based in situ vaccination strategies establish localized immune-activating niches, prolong antigen retention, boost DC cells maturation and antigen cross-presentation, and elicit durable T cells mediated immunity and immune memory. By integrating stimuli-responsive release, TME remodeling, ICD induction, and immune amplification, they effectively suppress tumor growth, inhibit metastasis, and prevent postoperative recurrence. Although challenges remain in precise release control, standardized preparation, and clinical translation, continuous optimization of multi-stimuli-responsive design, structure–activity relationships, and combination immunotherapy will further advance this field. Therefore, TME-responsive hydrogel-mediated in situ tumor vaccination represents a highly promising, personalized, and translatable strategy for next-generation tumor immunotherapy.
Data Sharing Statement
No datasets were generated or analysed during the current study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Natural Science Foundation of Jiangxi Province (20232BAB206055) and Special fund for postgraduate innovation in Jiangxi Province (YC2012-B011).
Disclosure
The authors declare no competing interests in this work.
References
1. Wang G, Dong Y. Novel chemo-photothermal therapy in hepatic cancer using gemcitabine-loaded hyaluronic acid conjugated MoS2/ZnO nanocomposites. Appl Biochem Biotechnol. 2024;196:5181–16. doi:10.1007/s12010-023-04796-0
2. Yang Y, Jianrong W, Bremner DH, et al. A multifunctional nanoplatform based on MoS2-nanosheets for targeted drug delivery and chemo-photothermal therapy. Colloids Surf B Biointerfaces. 2020;185:110585. doi:10.1016/j.colsurfb.2019.110585
3. Liu G, Nana M, Cheng K, et al. Bacteria-derived nanovesicles enhance tumour vaccination by trained immunity. Nat Nanotechnol. 2024;19:387–398. doi:10.1038/s41565-023-01553-6
4. Mistarz A, Komorowski MP, Graczyk MA, et al. Recruitment of intratumoral CD103+ dendritic cells by a CXCR4 antagonist-armed virotherapy enhances antitumor immunity. Mol Ther Oncolytics. 2019;14:233–245. doi:10.1016/j.omto.2019.06.003
5. Liang J, Zhu F, Cheng K, et al. Outer membrane vesicle-based nanohybrids target tumor-associated macrophages to enhance trained immunity-related vaccine-generated antitumor activity. Adv Mater. 2023;35:e2306158. doi:10.1002/adma.202306158
6. Sahin U, Türeci Ö. Personalized vaccines for cancer immunotherapy. Science. 2018;359:1355–1360. doi:10.1126/science.aar7112
7. Kumar A, Dixit S, Srinivasan K, et al. Personalized cancer vaccine design using AI-powered technologies. Front Immunol. 2024;15:1357217.
8. Blass E, Ott PA. Advances in the development of personalized neoantigen-based therapeutic cancer vaccines. Nat Rev Clin Oncol. 2021;18:215–229. doi:10.1038/s41571-020-00460-2
9. von Locquenghien M, Zwicky P, Xie K, et al. Macrophage-targeted immunocytokine leverages myeloid, T, and NK cell synergy for cancer immunotherapy. Cell. 2025;188:7099–7117. doi:10.1016/j.cell.2025.10.030
10. Chen J, Hnath B, Sha CM, et al. Optogenetically engineered Septin-7 enhances immune cell infiltration of tumor spheroids. Proc Natl Acad Sci USA. 2024;121:e2405717121. doi:10.1073/pnas.2405717121
11. Gao Z-L, Wei X, Zheng S-J, et al. Orchestrated cytosolic delivery of antigen and adjuvant by manganese ion-coordinated nanovaccine for enhanced cancer immunotherapy. Nano Lett. 2023;23:1904–1913. doi:10.1021/acs.nanolett.2c04970
12. Shen M, Guo L, Zhang H, et al. Differential reinforcement of cGAS-STING pathway-involved immunotherapy by biomineralized bacterial outer membrane-sensitized EBRT and RNT. J Nanobiotechnology. 2024;22:310. doi:10.1186/s12951-024-02565-7
13. Vos JL, Elbers JBW, Krijgsman O, et al. Neoadjuvant immunotherapy with nivolumab and ipilimumab induces major pathological responses in patients with head and neck squamous cell carcinoma. Nat Commun. 2021;12:7348. doi:10.1038/s41467-021-26472-9
14. Luo S, Yang Y, Chen L, et al. Outer membrane vesicle-wrapped manganese nanoreactor for augmenting cancer metalloimmunotherapy through hypoxia attenuation and immune stimulation. Acta Biomater. 2024;181:402–414. doi:10.1016/j.actbio.2024.05.010
15. Pavelić K. Personalized neoantiged vaccine against cancer. Psychiatry Danub. 2021;33:S331–S335.
16. Yin X, Yaohua K, Liang Y, et al. An immune-enhancing injectable hydrogel loaded with esketamine and DDP promotes painless immunochemotherapy to inhibit breast cancer growth. Adv Healthc Mater. 2024;13:e2401373. doi:10.1002/adhm.202401373
17. Tang H, Wang X, Lili H, et al. An injectable composite hydrogel containing polydopamine-coated curcumin nanoparticles and indoximod for the enhanced combinational chemo-photothermal-immunotherapy of breast tumors. Colloids Surf B Biointerfaces. 2024;244:114130. doi:10.1016/j.colsurfb.2024.114130
18. Wang L, Ramirez A, Felgner J, et al. Development of a single-dose Q fever vaccine with an injectable nanoparticle-loaded hydrogel: effect of sustained co-delivery of antigen and adjuvant. Drug Deliv. 2025;32:2476144. doi:10.1080/10717544.2025.2476144
19. Musaie K, Abbaszadeh S, Nosrati-Siahmazgi V, et al. Metal-coordination synthesis of a natural injectable photoactive hydrogel with antibacterial and blood-aggregating functions for cancer thermotherapy and mild-heating wound repair. Biomater Sci. 2023;11:2486–2503. doi:10.1039/D2BM01965E
20. Liu C, Liao Y, Liu L, et al. Application of injectable hydrogels in cancer immunotherapy. Front Bioeng Biotechnol. 2023;11:1121887. doi:10.3389/fbioe.2023.1121887
21. Kim J, Choi Y, Kim D-H, et al. Injectable hydrogel-based combination cancer immunotherapy for overcoming localized therapeutic efficacy. Pharmaceutics. 2022;14:1908. doi:10.3390/pharmaceutics14091908
22. Zhou Q, Gong N, Zhang D, et al. Mannose-derived carbon dots amplify microwave ablation-induced antitumor immune responses by capturing and transferring “danger signals” to dendritic cells. ACS Nano. 2021;15:2920–2932. doi:10.1021/acsnano.0c09120
23. Zhangzuo L, Wang Q, Huang X, et al. Lactate in the tumor microenvironment: a rising star for targeted tumor therapy. Front Nutr. 2023;10:1113739. doi:10.3389/fnut.2023.1113739
24. Schwartz L, Supuran CT, Alfarouk KO. The warburg effect and the hallmarks of cancer. Anticancer Agents Med Chem. 2017;17:164–170. doi:10.2174/1871520616666161031143301
25. Jing L, Zhao J, Jingjia Y, et al. A versatile chitosan hydrogel crosslinked by boronated diol drug conjugates as anti-tumor immune stimulator for hepatocellular carcinoma treatment. Carbohydr Polym. 2025;369:124244. doi:10.1016/j.carbpol.2025.124244
26. Llovet JM, Castet F, Heikenwalder M, et al. Immunotherapies for hepatocellular carcinoma. Nat Rev Clin Oncol. 2022;19:151–172. doi:10.1038/s41571-021-00573-2
27. Belmontes B, Sawant DV, Zhong W, et al. Immunotherapy combinations overcome resistance to bispecific T cell engager treatment in T cell-cold solid tumors. Sci Transl Med. 2021;13:eabd1524. doi:10.1126/scitranslmed.abd1524
28. Qian Z, Yuan Y, Junhang L, et al. pH-responsive injectable nanocomposite hydrogel based on dynamic boronate ester bonds loading Pt-TiO2 nanoparticles and fluorescence probe for synergistic sonodynamic-immunotherapy and imaging of cancer. J Mater Chem B. 2025;13:13635–13646. doi:10.1039/D5TB01837D
29. Mousavi SM, Kalashgrani MY, Javanmardi N, et al. Recent breakthroughs in graphene quantum dot-enhanced sonodynamic and photodynamic therapy. J Mater Chem B. 2024;12:7041–7062. doi:10.1039/D4TB00767K
30. Zhou J, Yamin L, Wang L, et al. Bifunctional drug delivery system with carbonic anhydrase IX targeting and glutathione-responsivity driven by host-guest amphiphiles for effective tumor therapy. Carbohydr Polym. 2024;326:121577. doi:10.1016/j.carbpol.2023.121577
31. Liu Z, Ling J, Wang N, et al. Redox homeostasis disruptors enhanced cuproptosis effect for synergistic photothermal/chemodynamic therapy. J Colloid Interface Sci. 2025;678:1060–1074. doi:10.1016/j.jcis.2024.08.234
32. Billimoria R, Bhatt P. Chrysin mitigates therapy-induced senescence in breast cancer via cGAS-STING pathway inhibition. Med Oncol. 2025;42:445. doi:10.1007/s12032-025-02993-x
33. Pang J, Yang J, Zhu W, et al. Photosensitive gel vaccine with enzyme-like properties for remodeling tumor microenvironment with STING activation for tumor synergistic therapy. Cancer Nanotechnol. 2026;17:17. doi:10.1186/s12645-026-00369-y
34. Cui M, Tang D, Wang B, et al. Bioorthogonal guided activation of cGAS-STING by AIE photosensitizer nanoparticles for targeted tumor therapy and imaging. Adv Mater. 2023;35:e2305668. doi:10.1002/adma.202305668
35. Zhang L, Zhu P, Wan T, et al. Glutamine coated titanium for synergistic sonodynamic and photothermal on tumor therapy upon targeted delivery. Front Bioeng Biotechnol. 2023;11:1139426. doi:10.3389/fbioe.2023.1139426
36. Lin S, Liu H, Letian L, et al. Hydrogel delivering antifibrotic agent and nano-sonosensitizer enhances efficacy of sonodynamic therapy in osteosarcoma treatment. Bioact Mater. 2025;56:77–94. doi:10.1016/j.bioactmat.2025.10.001
37. Wang A, Fang J, Shuyue Y, et al. Assembly transformation jointly driven by the LAP enzyme and GSH boosting theranostic capability for effective tumor therapy. ACS Appl Mater Interfaces. 2021;13:59787–59802. doi:10.1021/acsami.1c21062
38. Deryugina EI, Quigley JP. Matrix metalloproteinases and tumor metastasis. Cancer Metastasis Rev. 2006;25:9–34. doi:10.1007/s10555-006-7886-9
39. Zong L, Hongliang X, Zhang H, et al. A review of matrix metalloproteinase-2-sensitive nanoparticles as a novel drug delivery for tumor therapy. Int J Biol Macromol. 2024;262:130043. doi:10.1016/j.ijbiomac.2024.130043
40. Tian T, Wang J, Yin F, et al. Activation of cascade-like antitumor immune responses through in situ doxorubicin stimulation and blockade of checkpoint coinhibitory receptor TIGIT. Adv Healthc Mater. 2022;11:e2102080. doi:10.1002/adhm.202102080
41. Zhang B, Ning L, Gao J, et al. Targeting of focal adhesion kinase enhances the immunogenic cell death of PEGylated liposome doxorubicin to optimize therapeutic responses of immune checkpoint blockade. J Exp Clin Cancer Res. 2024;43:51. doi:10.1186/s13046-024-02974-4
42. Zhang Q, Wenjun H, Guo M, et al. MMP-2 responsive peptide hydrogel-based nanoplatform for multimodal tumor therapy. Int J Nanomed. 2024;19:53–71. doi:10.2147/IJN.S432112
43. Cai Y, Chai T, Nguyen W, et al. Phototherapy in cancer treatment: strategies and challenges. Signal Transduct Target Ther. 2025;10:115. doi:10.1038/s41392-025-02140-y
44. Guo Y, Wang M, Zhang Y, et al. Advanced hydrogel material for colorectal cancer treatment. Drug Deliv. 2025;32:2446552. doi:10.1080/10717544.2024.2446552
45. Xu N, Hu A, Ximing P, et al. Cu-Chelated polydopamine nanoparticles as a photothermal medium and “immunogenic cell death” inducer for combined tumor therapy. J Mater Chem B. 2022;10:3104–3118. doi:10.1039/D2TB00025C
46. Ziwei H, Tan H, Yicheng Y, et al. NIR-actuated ferroptosis nanomotor for enhanced tumor penetration and therapy. Adv Mater. 2024;36:e2412227. doi:10.1002/adma.202412227
47. Fang Z, Yan Z, Zhangzuo L, et al. Polydopamine nanoparticles cross-linked hyaluronic acid photothermal hydrogel with cascading immunoinducible effects for in situ antitumor vaccination. Int J Biol Macromol. 2024;269:132177. doi:10.1016/j.ijbiomac.2024.132177
48. Kou Y, Feng R, Chen J, et al. Development of a nattokinase-polysialic acid complex for advanced tumor treatment. Eur J Pharm Sci. 2020;145:105241. doi:10.1016/j.ejps.2020.105241
49. Qing J, Zhu M, Xinyuan L, et al. Environment-responsive polydopamine nanoparticle cross-linked phenylboronic-grafted hyaluronic acid with enzyme-like properties for tumor synergistic therapy. Nanoscale. 2025;17:15988–16002. doi:10.1039/D5NR00964B
50. Zeting Y, Shuli M, Yue L, et al. Tissue adhesive indocyanine green-locking granular gel-mediated photothermal therapy combined with checkpoint inhibitor for preventing postsurgical recurrence and metastasis of colorectal cancer. Bioeng Transl Med. 2023;8:e10576. doi:10.1002/btm2.10576
51. Zhang F, Qingyuan W, Liu H, et al. NIR light-triggered nanomaterials-based prodrug activation towards cancer therapy. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2020;12:e1643. doi:10.1002/wnan.1643
52. Kaneko K, Osada T, Morse MA, et al. Heat shock protein 90-targeted photodynamic therapy enables treatment of subcutaneous and visceral tumors. Commun Biol. 2020;3:226. doi:10.1038/s42003-020-0956-7
53. Lan J, Zeng R, Zhe L, et al. Biomimetic nanomodulators with synergism of photothermal therapy and vessel normalization for boosting potent anticancer immunity. Adv Mater. 2024;36:e2408511. doi:10.1002/adma.202408511
54. Sun Y, Chen Y, Bolin W, et al. Synergistic SDT/cuproptosis therapy for liver hepatocellular carcinoma: enhanced antitumor efficacy and specific mechanisms. J Nanobiotechnology. 2024;22:762. doi:10.1186/s12951-024-02995-3
55. Son S, Kim JH, Wang X, et al. Multifunctional sonosensitizers in sonodynamic cancer therapy. Chem Soc Rev. 2020;49:3244–3261. doi:10.1039/C9CS00648F
56. Wei X, Feng Z, Huang J, et al. Homology and immune checkpoint dual-targeted sonocatalytic nanoagents for enhancing sonodynamic tumor therapy. ACS Appl Mater Interfaces. 2021;13:32810–32822. doi:10.1021/acsami.1c08105
57. Zheng J, Sun Y, Long T, et al. Sonosensitizer nanoplatform-mediated sonodynamic therapy induced immunogenic cell death and tumor immune microenvironment variation. Drug Deliv. 2022;29:1164–1175. doi:10.1080/10717544.2022.2058653
58. Guo S, Xie G, Molin L, et al. Ultrasound-triggered endogenous tumor vaccination for the inhibition of metastasis and recurrence. Chem Eng J. 2026;532:174432. doi:10.1016/j.cej.2026.174432
59. Zhang X-M, Wang H-L, Gemingnuer A, et al. Bacterial outer membrane vesicles as intrinsically immunogenic and highly modifiable nanocarriers for precision tumor therapy. Mol Biol Rep. 2026;53:455. doi:10.1007/s11033-026-11628-x
60. Nie X, Shi C, Chen X, et al. A single-shot prophylactic tumor vaccine enabled by an injectable biomembrane hydrogel. Acta Biomater. 2023;169:306–316. doi:10.1016/j.actbio.2023.08.010
61. Liu X, Wang Y, Han W, et al. Natural polysaccharide hydrogel delivery system remodeling tumor microenvironment to promote postoperative tumor therapy. Int J Biol Macromol. 2025;291:139137. doi:10.1016/j.ijbiomac.2024.139137
62. Chu X, Bobin M, Xiong Y, et al. Bioactive nanocomposite hydrogel enhances postoperative immunotherapy and bone reconstruction for osteosarcoma treatment. Biomaterials. 2025;312:122714. doi:10.1016/j.biomaterials.2024.122714
63. Igarashi Y, Sasada T. Cancer vaccines: toward the next breakthrough in cancer immunotherapy. J Immunol Res. 2020;2020:5825401. doi:10.1155/2020/5825401
64. Cai G, Ren L, Jiali Y, et al. A microenvironment-responsive, controlled release hydrogel delivering embelin to promote bone repair of periodontitis via anti-infection and osteo-immune modulation. Adv Sci. 2024;11:e2403786. doi:10.1002/advs.202403786
65. Wang Y, Geng W, Yang Y, et al. Engineered self-assembling hydrogel systems for advanced guided bone regeneration: structural optimization and biofunctional modulation. J Nanobiotechnology. 2025;23:720. doi:10.1186/s12951-025-03761-9
66. Yang Y, Zhou B, Min L, et al. GO/Cu nanosheet-integrated hydrogel platform as a bioactive and biocompatible scaffold for enhanced calvarial bone regeneration. Int J Nanomed. 2024;19:8309–8336. doi:10.2147/IJN.S467886
67. Wang M, Chen M, Niu W, et al. Injectable biodegradation-visual self-healing citrate hydrogel with high tissue penetration for microenvironment-responsive degradation and local tumor therapy. Biomaterials. 2020;261:120301. doi:10.1016/j.biomaterials.2020.120301
68. Haichang L, Liu Z, Zhang P, et al. The recent research progress in the application of the nanozyme-hydrogel composite system for drug delivery. Drug Deliv. 2024;31:2417986. doi:10.1080/10717544.2024.2417986
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.