Back to Journals » Clinical Interventions in Aging » Volume 15
Trunk Skeletal Muscle Mass and Phase Angle Measured by Bioelectrical Impedance Analysis are Associated with the Chance of Femoral Neck Fracture in Very Elderly People
Authors Chen J, Lu K, Chen H, Hu N, Chen J, Liang X, Qin J, Huang W
Received 20 February 2020
Accepted for publication 19 May 2020
Published 12 June 2020 Volume 2020:15 Pages 889—895
DOI https://doi.org/10.2147/CIA.S250629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Jia Chen,1,* Kai Lu,2,* Hong Chen,3 Ning Hu,3 Jie Chen,3 Xi Liang,3 Jian Qin,1 Wei Huang3
1Department of Clinical Nutrition, The First Affiliated Hospital of Chongqing Medical University, Chongqing 400016, People’s Republic of China; 2Department of Cardiology, The First Affiliated Hospital of Chongqing Medical University, Chongqing 400016, People’s Republic of China; 3Department of Orthopedic Surgery, The First Affiliated Hospital of Chongqing Medical University, Chongqing 400016, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Huang
Department of Orthopedic Surgery, The First Affiliated Hospital of Chongqing Medical University, No. 1, Youyi Road, Chongqing 400016, People’s Republic of China
Tel +86-13883383330
Fax +86-23 89011211
Email [email protected]
Background: The study aimed to investigate the potential association of trunk skeletal muscle mass (tSM) and phase angle measured by bioelectrical impedance analysis (BIA) with the chance of femoral neck fractures in very elderly people.
Patients and Methods: This case-control study enrolled 78 femoral neck fracture patients aged over 75 years (29 males) and 1:2 matched healthy controls. All participants were subjected to BIA examination by specialists. tSM, the corrected values by height squared of tSM (tSMI) and phase angle were compared between fracture patients and controls. Multivariate logistic regression was performed to explore the strength of association of femoral neck fracture with tSM, tSMI, and phase angle.
Results: tSM (kg) of fracture patients was significantly lower than those of controls in all participants (women: 13.49± 0.42 vs 15.44± 0.39, p< 0.05; men: 15.30± 0.71 vs 17.54± 0.78, p< 0.05). In the sarcopenic subgroup, fracture patients also got a lower tSM than controls (women: 12.58± 0.21 vs 13.62± 0.16, p< 0.05; men:14.41± 0.29 vs 16.07± 0.21, p< 0.05). The comparison of tSMI between the two groups was similar to that of tSM. Phase angle (°) at 50 kHz in fracture patients was significantly lower than that of controls in women and men (women: 3.70± 0.32 vs 4.61± 0.21, p< 0.05; men: 3.50± 0.20 vs 3.84± 0.22, p< 0.05). Multivariate logistic regression analysis demonstrated higher fracture chance with significantly associated decreased tSM [women: OR (95% CI): 0.78(0.67– 0.91); men: 0.74(0.64– 0.86)] and tSMI [women: OR (95% CI): 0.72(0.61– 0.85); men: 0.69 (0.59– 0.81)]. In addition, per 1° increase of phase angle in the trunk could decrease the fracture risk by 14% for women [OR (95% CI): 0.86 0.79– 0.94)] and 29% for men [OR (95% CI): 0.71 (0.64– 0.79)].
Conclusion: This study indicates a decrease in tSM, tSMI, and phase angle measured by BIA is significantly related to the increased chance of femoral neck fracture in people aged over 75 years. Strengthening the mass and strength of trunk skeletal muscles may help reduce the risk of femoral neck fracture in elderly patients.
Keywords: bioelectrical impedance analysis, skeletal muscle mass, phase angle, femoral neck fracture
Introduction
The incidence of femoral neck fracture in the elderly population is continuously increasing due to the increase in average life expectancy worldwide.1,2 Prevention of femoral neck fracture is still crucial due to its many complications and high mortality, although the prognosis of femoral neck fracture has been much improved in the past decades.3 Identifying relevant risk factors is the first step in preventing femoral neck fractures.
Sarcopenia is one common form of malnutrition in the elderly population and its prevalence increases along with age.4 Decreased muscle mass often leads to weakened muscle strength, making it difficult to maintain body posture and leading to an increased incidence of falls,5,6 one of the most important factors for femoral neck fracture.7,8 Previous studies have indicated that sarcopenia is one strong risk factor for femoral neck fracture.9–11 According to the definition of sarcopenia by the Asia Working Group for Sarcopenia (AWGS),12 only appendicular lean mass (aLM) or its corrected values of the human body is used to evaluate whether sarcopenia is combined. Actually, skeletal muscles of the trunk also play an important role in maintaining posture and preventing falls. However, whether the decrease in muscle mass or strength in the trunk area increases the risk of femoral neck fractures has not been reported in the literature.
In recent years, bioelectrical impedance technology (BIA) which can estimate body composition by measuring the body’s impedance has been widely used in various clinical fields. Instruments based on BIA can estimate the skeletal muscle mass in whole body as well as in one segment such as limbs or trunk.13 Only measuring muscle mass to determine muscle status has drawbacks because decreased muscle mass does not always lead to weakened skeletal muscle strength. BIA can also measure phase angle which to some extent can reflect the functional status of muscles.14–16 The potential association of phase angle of trunk muscle with the chance of femoral neck fracture has not been reported so far.
In the current study, we aimed to investigate the potential association of trunk skeletal muscle mass and phase angle measured by BIA with the chance of femoral neck fracture in the very elderly population.
Patients and Methods
Study Design and Population
This case-control study was conducted from September 2017 to December 2018 in the orthopedic department of the First Affiliated Hospital of Chongqing Medical University. A total of 78 patients (29 males) aged more than 75 years who were admitted into hospital due to femoral neck fracture after falls were consecutively enrolled. Critical exclusion criteria included: pathologic fracture; malignant tumor; a history of previous hip fracture requiring surgery with metal prosthesis; chronic drug use which may affect the body fluid balance and skeletal mass; significant sensory or balance impairments such as noticeable vision loss, ataxia, etc.; alanine transaminase (ALT) or glutamic-oxalacetic transaminase (GOT) >3 times the upper limit of normal or estimated glomerular filtration rate (eGFR) <30 mL/(min·1.73m2) or other concomitant severe diseases; inability to cooperate to finish BIA test and other conditions which were inappropriate for enrollment judged by the researchers. Then 1:2 gender-, age- and body mass index (BMI)-matched control participants were chosen from the volunteers with no major diseases history.
The contents and purposes of this study were thoroughly explained to the participants prior to the study, and written consents were obtained from all of them. The study protocols were in accordance with the Declaration of Helsinki and ethical approval was obtained from the First Affiliated Hospital of Chongqing Medical University.
Measurements
All participants were subjected to BIA testing by Direct Segmental Multi-Frequency Bioelectrical Impedance Analyzer (DSM-BIA, Inbody S10, Korea). BIA was performed the day the participant was admitted to hospital before any fluid treatment began. And, for volunteers, BIA testing was completed in 2 weeks. BIA measurements in the present study were performed following the manufacturer’s instructions. All participants were asked not to take any foods or drinks and to avoid strenuous activity within 2 hours before the testing. All parameters of BIA testing were obtained using a standard montage of outer and inner electrodes on the right hand and foot while patients lay down with legs apart. Body composition indicators including skeletal muscle mass (SMM), soft lean mass (SLM), percentage of body fat (PBF), fat free mass (FFM), fat mass (FM), intracellular water (ICW), extracellular water (ECW), total body water (TBW), mineral content and protein content were measured and recorded. The parameters of resistance and reactance were determined using an electric alternating current flow of 800 mA and multiple frequencies of 5 kHz, 50 kHz and 250 kHz. Phase angle was calculated using the following equation: phase angle (°) = arctan (reactance/resistance) (180/ω). The BIA device used in the present study could measure phase angle of the whole body as well as a particular body segment such as the trunk.
Statistics
Continuous variables were presented as mean ± stand deviation (SD). Paired t test or Wilcoxon rank-sum test was used for comparison between groups for continuous variables according to whether the distribution of the data was normal. Categorical variables were presented as frequency (proportions) and compared with χ2 test. To further test the strength of association of femoral neck fracture with tSM, tSMI, and phase angle, multivariate logistic regression was performed and confounding effects such as traditional nutritional indicators and parameters from BIA including albumin, prealbumin, blood urea nitrogen, SMM, SLM, PBF, FFM, FM, mineral, and protein were adjusted. For all the comparisons, the level of statistical significance was set at p<0.05 two-sided. SPSS 19.0 was used for all statistical analyses.
Results
Basic Characteristics of Femoral Neck Fracture Patients and Healthy Controls
As shown in Table 1, significant differences were observed between fracture patients and healthy controls with regarding to certain BIA indicators including SMM, SLM, PBF, FFM, FM, mineral, and protein (p<0.05). In addition, albumin, prealbumin, and blood urea nitrogen which were classical indicators of nutritional status also showed significant differences between the two groups. As to hemoglobin, ICW, ECW and TCW, no obvious differences were detected.
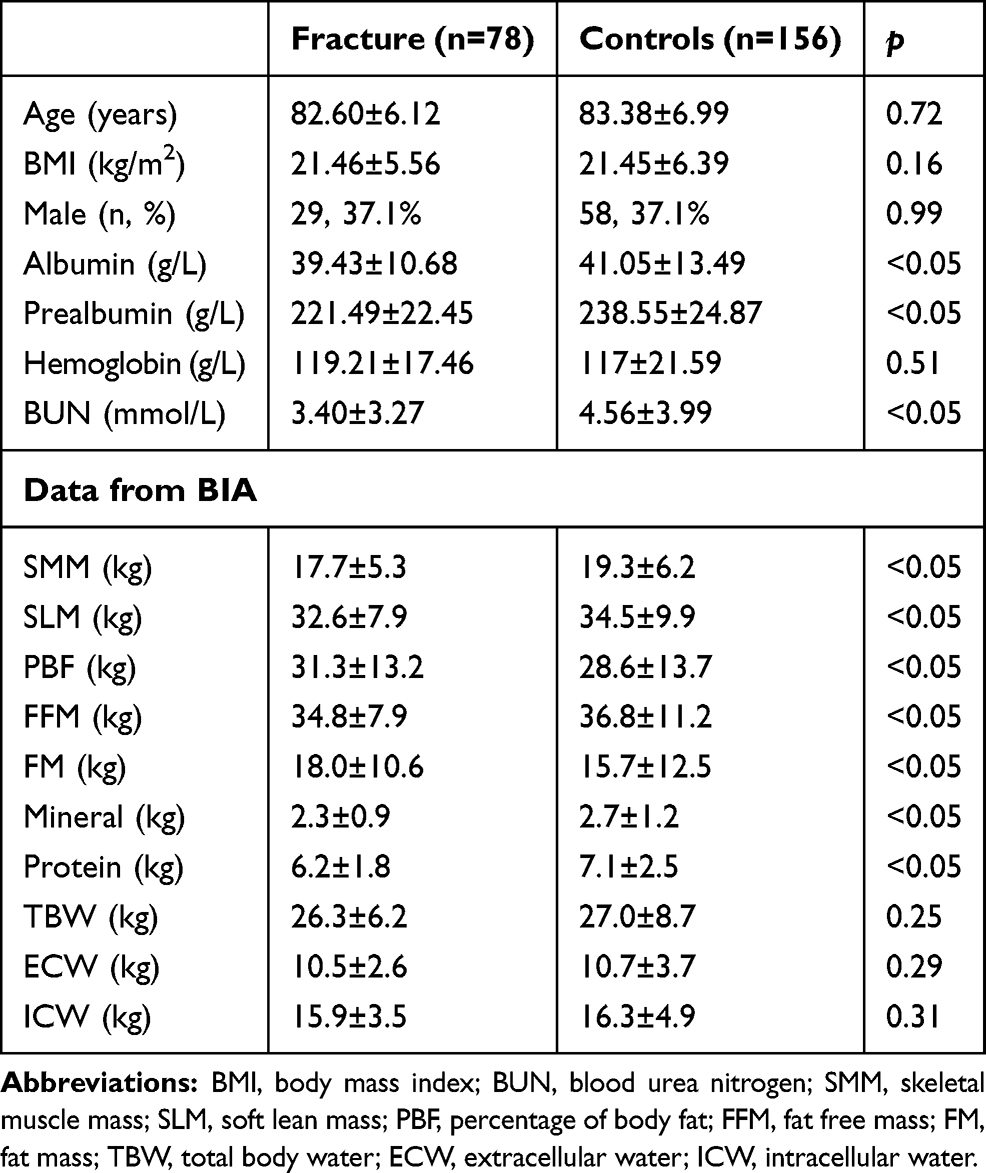 |
Table 1 The Basic Characteristics of Femoral Neck Fracture Patients and Healthy Controls |
Appendicular Lean Mass and Trunk Skeletal Muscle Mass is Lower in Fracture Patients Than Healthy Controls
Appendicular lean mass (aLM) corrected by height squared (appendicular skeletal muscle mass index, aSMI) below 5.4 kg/m2 in women and below 7.0 kg/m2 in men were identified as sarcopenia according to the criteria based on the Asia Working Group for Sarcopenia (AWGS). As shown in Table 2, both aLM and aSMI of fracture patients were significantly lower than those of healthy controls in men and women. The prevalence of sarcopenia in fracture patients was 69.4% in women and 65.5% in men, values which were significantly higher than their counterparts of 52.0% and 42.1% in healthy controls (p<0.05). Similarly, trunk skeletal muscle mass (tSM) was also significantly lower in fracture patients than healthy controls in both women (13.5±2.8 vs 15.4±4.0, p<0.05) and men (15.3±3.8 vs 17.5±6.1, p<0.05). To rule out the confounding effect of height, we corrected tSM by height squared which was named as trunk skeletal muscle mass index (tSMI). The comparative results of tSMI between fracture patients and controls were similar to those of tSM as shown in Table 2.
 |
Table 2 Comparison of Skeletal Muscle Mass in Limbs and Trunk Measured by BIA Between Femoral Neck Fracture Patients and Healthy Controls |
Trunk Skeletal Muscle Mass Is Lower in Fracture Patients Than Controls in the Sarcopenic Subgroup
tSM and its corrected values and tSMI were also compared in sarcopenic participants with or without femoral neck fracture (Figure 1). We observed that both tSM and tSMI were significantly lower in fracture patients than controls in both women (tSM 12.6±0.6 vs 13.6±0.6, p<0.05; tSMI 5.4±0.2 vs 6.0±0.3, p<0.05) and men (tSM 14.4±0.6 vs 16.1±0.4, p<0.05; tSMI 5.4±0.4 vs 6.3±0.2, p<0.05). However, the difference of aSMI between the two groups (women: 4.1±0.2 vs 4.3±0.3, p>0.05; men: 5.9±0.4 vs 6.1±0.4, p>0.05) was not significant. The above result indicated loss of trunk skeletal muscle may not be parallel to loss of appendicular skeletal muscle in elderly fracture patients.
 |
Figure 1 Comparison of trunk skeletal muscle mass measured by BIA and its corrected values by height2 in sarcopenic participants with or without femoral neck fracture. *p<0.05 versus the control group for tSM; **p<0.05 versus the control group for tSMI. Abbreviations: tSM, trunk skeletal muscle mass (kg); tSMI, trunk skeletal muscle mass index which was defined as tSM/height2(kg/m2). |
Phase Angle of Trunk Skeletal Muscle is Lower in Participants with Fracture Than Those Without
As to the value of phase angle at frequency of 5 kHz and 50 kHz, significant differences were found between fracture patients and controls in both men and women (Table 3). However, the statistical significance of phase angle no longer existed at a frequency of 250 kHz in neither men nor women.
 |
Table 3 Comparison of Phase Angle of Trunk at Multiple Frequencies from BIA in Femoral Neck Fracture Patients and Healthy Controls |
Logistic Regression Analysis of the Association of Femoral Neck Fracture with tSM, tSMI, and Phase Angle
As shown in Table 4, multivariate logistic regression was performed to evaluate the strength of the association of femoral neck fracture with tSM, tSMI, and phase angle. After adjusting the confounding effect of albumin, prealbumin, blood urea nitrogen, SMM, SLM, PBF, FFM, FM, mineral, and protein, we found increased tSM was significantly associated with decreased femoral neck fracture risk in both men and women with odds ratio as well as 95% confidence interval of 0.78 (0.67–0.91) for women and 0.74 (0.64–0.86) for men. For tSMI, the association strength was even stronger than tSM [OR (95% CI): 0.72 (0.61–0.85) for women; 0.69 (0.59–0.81) for men]. As to phase angle of trunk, we found per 1° increase of phase angle of trunk could bring down the femoral neck fracture risk by 14% for women [OR (95% CI): 0.86 (0.79–0.94)] and 29% for men [OR (95% CI): 0.71 (0.64–0.79)].
 |
Table 4 Univariate and Multivariate Logistic Regression About the Potential Association of tSM, tSMI and Phase Angle of Trunk at Frequency of 50 kHz with the Incidence of Femoral Neck Fracture |
Discussion
In the present study, we explored the potential association of body composition indicators from BIA with the chance of femoral neck fracture in very elderly people. The result demonstrated that loss of trunk skeletal muscle mass measured by BIA was significantly associated with the risk of femoral neck fracture in people aged more than 75 years. The result also showed obvious differences about the phase angle of trunk between fracture and non-fracture people, which indicated phase angle of trunk could perhaps be a potential predictor of femoral neck fracture.
In the past decade, BIA was widely used in analyzing body composition including segmental skeletal muscle mass with fast and non-invasive advantages,17,18 and many of the BIA indicators were found to be valuable in helping clinicians better diagnose diseases and judge the prognosis.19 Many previous studies have confirmed reduced aLM measured by BIA had a good correlation with increased risk of femoral neck fracture,9–11 which is consolidated by our results that aLM in fracture patients is much lower than the controls. Loss of trunk skeletal muscle may be parallel to loss of appendicular skeletal muscle as people age, in which case no obvious differences can be found in fracture and controls with regarding to tSM. Under this premise, measuring tSM cannot provide more predictive information of fracture than sarcopenia. However, in the present study significantly lower tSM is still observed in fracture patients than controls in the sarcopenic subgroup, which reverses the above assumptions and indicates measuring tSM could perhaps provide additional predictive information for femoral neck fracture.
Obviously, it is not appropriate to evaluate the overall functional status of trunk skeletal muscle by measuring muscle mass only, because muscle mass is not necessarily parallel to other muscle functional status indicators such as strength. Phase angle is mainly determined by the membrane permeability of human body cells which indicates the trunk phase angle can evaluate the quality of trunk skeletal muscle at least in part. This viewpoint is supported by some previous reports in the literature. It has been reported that phase angle was significantly associated with the muscle quality index in older women and it could be improved after resistance training.16 Furthermore, phase angle has been proved to be associated with handgrip strength but not with sarcopenia,15 suggesting phase angle may reflect muscle status from another side different from muscle mass. Another recently published study supported our result which revealed older adults with lower phase angles were more likely to experience prospective falls compared with those with normal-high phase angles,20 although the significance of the overall phase angle was explored in their research rather than the individual trunk phase angle. Our study suggests a correlation between the trunk phase angle and the risk of femoral neck fractures. If this is confirmed by more studies, regular BIA testing may identify high-risk populations for femoral neck fractures at an early stage. Providing timely patient education to this population may help reduce the incidence of femoral neck fractures.
According to the following formula,
phase angle (°) = arctan (reactance/resistance) (180/ω)
reactance (Ω) = 1/(2 π*frequency* capacitance)
Choosing appropriate frequency is crucial to avoid the measured values of phase angle becoming too small, especially considering that systematic error of BIA testing cannot be ignored at this stage. Our result shows that the significant differences of phase angle between fracture and control people can only be observed when the frequency used is 5 kHz or 50 kHz. We speculate that a frequency as high as 250 kHz may reduce the value of reactance too much to make the calculated phase angle relatively stable and repeatable. After an extensive literature review, we found 50 kHz frequency was used the most when measuring phase angle by BIA, which is also consistent with our result.21–23
Limitations
Our study has several limitations. Firstly, although BIA is recommended to measure skeletal muscle mass by European Working Group on Sarcopenia in Older People, the accuracy of BIA is still controversial compared with dual energy X-ray absorptiometry (DXA), computed tomography (CT) and magnetic resonance imaging (MRI).12 Secondly, in addition to sarcopenia, there are many factors that can cause falls in the elderly, such as impaired sensorium, multimorbidity, vitamin D deficiency, polypharmacy, and house hazards. Although the elderly with impaired sensorium, multimorbidity, and polypharmacy were excluded from this study as much as possible, we have not been able to rule out the effects of house hazards and vitamin D deficiency on the results. Thirdly, the phase angle of the trunk area may be affected by the soft tissue inside the chest cavity, but it is not clear to us about the extent of the impact. However, even considering the impact of soft tissue on trunk phase angle, the significant difference in trunk phase angle between the fractured and the control group is still largely due to the difference in function and quality of the muscle itself. Of course, this needs more research to confirm. And last but not least, the swelling of the muscle after the bone fracture may cause the muscle mass to be overestimated which would cause a certain degree of bias to the results. However, the injury caused by femoral neck fracture is mainly limited to the joint capsule, and the degree of muscle edema is less severe than that caused by femoral shaft or intertrochanteric fracture. Therefore, the bias of muscle edema on the results should be very weak, and will not have a significant impact on the conclusion of this study.
Conclusions
In the present study, we find decreased trunk skeletal muscle mass and phase angle measured by BIA are significantly associated with increased risk of femoral neck fracture in people aged more than 75 years. In addition, the attenuation of trunk skeletal muscle is not parallel to the limb muscles, indicating that measuring the trunk skeletal muscle mass and phase angle can provide additional information to help determine the risk of femoral neck fracture. If there are cohort studies in future that can confirm a reduction in trunk muscle mass and phase angle can indeed lead to an increased risk for femoral neck fracture in the elderly, regular BIA testing may be a simple but promising tool for predicting femoral neck fracture in the elderly.
Abbreviations
aLM, appendicular lean mass; ALT, alanine transaminase; aSM, appendicular skeletal muscle mass; aSMI, appendicular skeletal muscle mass index; BIA, bioelectrical impedance analysis; ECW, extracellular water; eGFR, estimated glomerular filtration rate; FFM, fat free mass; FM, fat mass; GOT, glutamic-oxalacetic transaminase; ICW, intracellular water; PBF, percentage of body fat; SE, standard error; SMM, skeletal muscle mass; SLM, soft lean mass; TBW, total body water; tSMI, trunk skeletal muscle mass index; tSM, trunk skeletal muscle mass.
Ethics Approval and Informed Consent
The contents and purposes of this study were thoroughly explained to the participants prior to the study, and written consents were obtained from all of them. The study protocols were in accordance with the Declaration of Helsinki and the ethical approval was obtained from the First Affiliated Hospital of Chongqing Medical University.
Acknowledgments
The authors express their sincere gratitude to Mrs Mele Vaikoloa Fonua from the Graduate College of Chongqing Medical University, People's Republic of China, for her work to improve the language and style of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ju DG, Rajaee SS, Mirocha J, Lin CA, Moon CN. Nationwide analysis of femoral neck fractures in elderly patients: a receding tide. J Bone Joint Surg Am. 2017;99(22):1932–1940. doi:10.2106/JBJS.16.01247
2. Kang JS, Jeon YS, Ahn CH, Roh TH. Osteosynthesis versus endoprosthesis for the treatment of femoral neck fracture in Asian elderly patients. BMC Musculoskelet Disord. 2016;17:264. doi:10.1186/s12891-016-1123-7
3. Florschutz AV, Langford JR, Haidukewych GJ, Koval KJ. Femoral neck fractures: current management. J Orthop Trauma. 2015;29(3):121–129. doi:10.1097/BOT.0000000000000291
4. Ethgen O, Beaudart C, Buckinx F, Bruyere O, Reginster JY. The future prevalence of sarcopenia in Europe: a claim for public health action. Calcif Tissue Int. 2017;100(3):229–234. doi:10.1007/s00223-016-0220-9
5. Landi F, Liperoti R, Russo A, et al. Sarcopenia as a risk factor for falls in elderly individuals: results from the ilSIRENTE study. Clin Nutr. 2012;31(5):652–658. doi:10.1016/j.clnu.2012.02.007
6. Moreland JD, Richardson JA, Goldsmith CH, Clase CM. Muscle weakness and falls in older adults: a systematic review and meta-analysis. J Am Geriatr Soc. 2004;52(7):1121–1129. doi:10.1111/j.1532-5415.2004.52310.x
7. Freiberger E, Blank WA, Salb J, et al. Effects of a complex intervention on fall risk in the general practitioner setting: a cluster randomized controlled trial. Clin Interv Aging. 2013;8:1079–1088. doi:10.2147/CIA.S46218
8. Yip JL, Khawaja AP, Broadway D, et al. Visual acuity, self-reported vision and falls in the EPIC-Norfolk Eye study. Br J Ophthalmol. 2014;98(3):377–382. doi:10.1136/bjophthalmol-2013-304179
9. Hars M, Biver E, Chevalley T, et al. Low lean mass predicts incident fractures independently from FRAX: a prospective cohort study of recent retirees. J Bone Miner Res. 2016;31(11):2048–2056. doi:10.1002/jbmr.2878
10. Kim BJ, Ahn SH, Kim HM, Lee SH, Koh JM. Low skeletal muscle mass associates with low femoral neck strength, especially in older Korean women: the Fourth Korea National Health and Nutrition Examination Survey (KNHANES IV). Osteoporos Int. 2015;26(2):737–747. doi:10.1007/s00198-014-2959-z
11. Elhakeem A, Hartley A, Luo Y, et al. Lean mass and lower limb muscle function in relation to hip strength, geometry and fracture risk indices in community-dwelling older women. Osteoporos Int. 2019;30(1):211–220. doi:10.1007/s00198-018-4795-z
12. Chen LK, Liu LK, Woo J, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc. 2014;15(2):95–101. doi:10.1016/j.jamda.2013.11.025
13. Ward LC. Bioelectrical impedance analysis for body composition assessment: reflections on accuracy, clinical utility, and standardisation. Eur J Clin Nutr. 2019;73(2):194–199. doi:10.1038/s41430-018-0335-3
14. Norman K, Stobaus N, Pirlich M, Bosy-Westphal A. Bioelectrical phase angle and impedance vector analysis – clinical relevance and applicability of impedance parameters. Clin Nutr. 2012;31(6):854–861. doi:10.1016/j.clnu.2012.05.008
15. Dos Reis AS, Santos HO, Limirio LS, de Oliveira EP. Phase angle is associated with handgrip strength but not with sarcopenia in kidney transplantation patients. J Ren Nutr. 2018.
16. Nunes JP, Ribeiro AS, Silva AM, et al. Improvements in phase angle are related with muscle quality index after resistance training in older women. J Aging Phys Act. 2019;1–6.
17. Pfeifer M, Begerow B, Minne HW, et al. Vitamin D status, trunk muscle strength, body sway, falls, and fractures among 237 postmenopausal women with osteoporosis. Exp Clin Endocrinol Diabetes. 2001;109(2):87–92. doi:10.1055/s-2001-14831
18. Sinaki M. Exercise for patients with osteoporosis: management of vertebral compression fractures and trunk strengthening for fall prevention. PMR. 2012;4(11):882–888. doi:10.1016/j.pmrj.2012.10.008
19. Lukaski HC, Kyle UG, Kondrup J. Assessment of adult malnutrition and prognosis with bioelectrical impedance analysis: phase angle and impedance ratio. Curr Opin Clin Nutr Metab Care. 2017;20(5):330–339. doi:10.1097/MCO.0000000000000387
20. Uemura K, Yamada M, Okamoto H. Association of bioimpedance phase angle and prospective falls in older adults. Geriatr Gerontol Int. 2019;19(6):503–507. doi:10.1111/ggi.13651
21. Alves FD, Souza GC, Aliti GB, Rabelo-Silva ER, Clausell N, Biolo A. Dynamic changes in bioelectrical impedance vector analysis and phase angle in acute decompensated heart failure. Nutrition. 2015;31(1):84–89. doi:10.1016/j.nut.2014.05.004
22. Gupta D, Lammersfeld CA, Vashi PG, et al. Bioelectrical impedance phase angle as a prognostic indicator in breast cancer. BMC Cancer. 2008;8(1):249. doi:10.1186/1471-2407-8-249
23. Lee SY, Lee YJ, Yang JH, Kim CM, Choi WS. The association between phase angle of bioelectrical impedance analysis and survival time in advanced cancer patients: preliminary study. Korean J Fam Med. 2014;35(5):251–256. doi:10.4082/kjfm.2014.35.5.251
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.