Back to Journals » Clinical Ophthalmology » Volume 11
Trifocal intraocular lenses: a comparison of the visual performance and quality of vision provided by two different lens designs
Authors Gundersen KG ![]() , Potvin R
, Potvin R ![]()
Received 5 March 2017
Accepted for publication 11 May 2017
Published 8 June 2017 Volume 2017:11 Pages 1081—1087
DOI https://doi.org/10.2147/OPTH.S136164
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Kjell G Gundersen,1 Rick Potvin2
1IFocus Øyeklinikk AS, Haugesund, Norway; 2Science in Vision, Akron, NY, USA
Purpose: To compare two different diffractive trifocal intraocular lens (IOL) designs, evaluating longer-term refractive outcomes, visual acuity (VA) at various distances, low contrast VA and quality of vision.
Patients and methods: Patients with binocularly implanted trifocal IOLs of two different designs (FineVision [FV] and Panoptix [PX]) were evaluated 6 months to 2 years after surgery. Best distance-corrected and uncorrected VA were tested at distance (4 m), intermediate (80 and 60 cm) and near (40 cm). A binocular defocus curve was collected with the subject’s best distance correction in place. The preferred reading distance was determined along with the VA at that distance. Low contrast VA at distance was also measured. Quality of vision was measured with the National Eye Institute Visual Function Questionnaire near subset and the Quality of Vision questionnaire.
Results: Thirty subjects in each group were successfully recruited. The binocular defocus curves differed only at vergences of −1.0 D (FV better, P=0.02), −1.5 and −2.00 D (PX better, P<0.01 for both). Best distance-corrected and uncorrected binocular vision were significantly better for the PX lens at 60 cm (P<0.01) with no significant differences at other distances. The preferred reading distance was between 42 and 43 cm for both lenses, with the VA at the preferred reading distance slightly better with the PX lens (P=0.04). There were no statistically significant differences by lens for low contrast VA (P=0.1) or for quality of vision measures (P>0.3).
Conclusion: Both trifocal lenses provided excellent distance, intermediate and near vision, but several measures indicated that the PX lens provided better intermediate vision at 60 cm. This may be important to users of tablets and other handheld devices. Quality of vision appeared similar between the two lens designs.
Keywords: FineVision, Panoptix, multifocal, defocus curve, contrast sensitivity
Plain language summary
This study was performed to see if there was a difference in the vision provided by a new trifocal lens (Panoptix [PX] lens) and a previously studied trifocal lens (FineVision [FV] lens). The new lens was designed to provide better vision at 60 cm (~24 inches). The researchers examined 60 subjects; 30 were implanted with the PX lens in both eyes and 30 were implanted with the FV lens in both eyes. The ability to read an eye chart (visual acuity) was tested at distance (4 m), intermediate (80 and 60 cm) and near (40 cm) and subjects completed a questionnaire regarding the quality of their vision. Low contrast vision (ability to see gray letters) was also examined. The results showed that both of the trifocal lenses studied provide similar vision at distance and near and provided about the same quality of vision. However, the PX lens appeared to provide better vision at an intermediate distance of 60 cm. These results mean that the PX trifocal lens may be a more suitable lens than the FV trifocal lens for people who prefer an intermediate viewing distance of 60 cm. Computer screens and handheld devices are generally found 40–60 cm from most users.
Introduction
The goal of multifocal intraocular lenses (IOLs) is to provide clear and comfortable vision to patients at all viewing distances; this is often difficult to achieve. Current multifocal IOLs include diffractive bifocal lenses with various add powers; these appeared to provide better near vision with fewer visual disturbances than earlier lens designs.1 Visual acuity (VA) at near and distance has been generally reported to be satisfactory, but intermediate vision was often problematic.2 Intermediate vision has become an increasing concern for patients as a result of the proliferation of handheld devices and the increasing use of computers and tablets in daily life.
Trifocal diffractive lenses were developed to address the intermediate vision limitations of bifocal IOL designs. To reduce the likelihood of increasing visual disturbances the designs were such that the dioptric power of the near focal point was twice the dioptric power of the intermediate focal point. In this way the second harmonic of the intermediate focal point contributed to the usable light energy at the near point. The FineVision® (FV) IOL (PhysIOL, Liège, Belgium) is an example of this trifocal design.3,4 The toric version of the lens has one haptic design while the non-toric version has another (MicroF). A study comparing the two models showed that they provided comparable visual outcomes.5
A new trifocal lens has recently been introduced, the AcrySof® Panoptix® IOL (Alcon, Fort Worth, TX, USA).6 An optical bench study indicated peak IOL performance at 42 cm for near and at ~60 cm for intermediate with this new trifocal lens.4
The purpose of the current study was to compare the clinical performance of the new Panoptix (PX) IOL with a commonly used trifocal lens, the FV trifocal IOL, with particular attention to the binocular defocus curve and the quality of vision provided. This is the first in vivo study that we are aware of comparing the two lenses.
Patients and methods
This study was a double-arm comparative noninterventional study of visual outcomes after successful bilateral trifocal IOL implantation. Subjects were assessed during a single diagnostic visit between 6 and 24 months after their surgery; 6 months allowed sufficient time for refractive stability and 24 months limited the likelihood of any pathological changes after surgery, such as posterior capsular opacification. Patients signed an informed consent that outlined the nature of the study, acknowledging their willingness to participate and permitting use of their de-identified data. Regional ethical committee approval was obtained before patients were enrolled (Regionale komiteer for medisinsk og helsefaglig forskningsetikk, Norway).
A sample size calculation indicated that 30 subjects in each group would be sufficient to detect the desired differences in IOL performance. Subjects were recruited for enrollment in the study 1 month or more after uncomplicated cataract surgery. IOL implantation performed by one surgeon at a single site. Surgery had to include bilateral implantation of either the FV or PX trifocal IOL. The patients self-selected a trifocal IOL, with the advice of the surgeon. Trifocal implantation was performed based on the patient’s interest in a higher degree of spectacle freedom at far, intermediate and near distances after cataract surgery. The only specific diagnostic criterion used to decide which lens to implant was preoperative astigmatism, because the FV lens was available as a toric lens. No other criteria were used, so selection bias was expected to be minimal. Enrollment criteria included uncomplicated bilateral IOL implantation and good ocular health with no pathology that could compromise VA (outside of residual refractive error). Inclusion criteria also included an uncorrected binocular distance VA of 20/40 or better; this was to ensure that quality of vision responses were not likely a function of residual refractive error or visually significant ocular pathology, such as posterior capsular opacification. Patients with previous ocular surgery, including LASIK or photorefractive keratectomy, were excluded.
The primary outcome measure was the best distance-corrected binocular defocus curve where logMAR VA was recorded for each defocus step. A binocular defocus curve was obtained with the manifest distance refraction in place in a phoropter, and in photopic conditions. An over-correction starting at +1.0 D was placed in the phoropter and binocular VA was recorded. The correction was then reduced by 0.5 D (ie, +0.5 over-correction) and VA was retested. An over-correction of −4.0 D was then placed in the phoropter and removed in 0.5 D increments, testing VA at each step. The procedure ends with VA testing with a 0.0 D over-correction (best-corrected distance refraction). Testing was conducted using proprietary computer software designed to simplify the procedure and to record results. LogMAR VA was recorded for each defocus step. VA was tested from worse to better focus to reduce the likelihood of letter memorization; in addition, three letter charts were used as the vergences changed.
Secondary outcome measures included uncorrected and best distance-corrected binocular VA at distance (4 m), intermediate (80 and 60 cm) and near (40 cm). All VA testing was with logMAR charts specifically designed for the four test distances. In addition, two surveys were included: the National Eye Institute (NEI) near vision subscale7 and the Quality of Vision (Q of V) questionnaire. The latter is a validated, Rasch-scored visual quality questionnaire;8 questions relate to the frequency, severity and the degree to which the subject is bothered by various possible visual disturbances, such as glare and halos. Additional secondary measures included the uncorrected and best-corrected low contrast binocular distance VA (using a 5% contrast early treatment diabetic retinopathy study [ETDRS] chart under photopic lighting conditions) and a measure of the preferred reading distance and binocular VA at that distance for all subjects in their uncorrected state. The near testing was conducted with a logarithmic ETDRS VA chart scaled for 40 cm, and held at the patient’s preferred reading distance. VA determined with the chart was recorded and scored. Results were adjusted for the distance that the chart was read to determine the corrected logMAR VA.
The lenses included in the current study were:
- Physiol FV IOL: This is a hydrophilic acrylic IOL with a 6.15 mm optical diameter which has 26 diffractive rings across the entire optic; the lens provides 1.75 and 3.5 D add powers.3 An optical bench study showed that the peak performance for this lens was at 40 cm for near and 80 cm for intermediate.4
- AcrySof PX IOL: This lens is made from a hydrophobic acrylic material with a 6.0 mm optical diameter, comprising a central 4.5 mm region with 15 diffractive rings and an outer annulus that is refractive only.6 The lens is actually a quadrafocal diffractive design, but the light from the first diffractive order is redistributed to the distance (refractive order) and second diffractive order using proprietary technology. The lens has the necessary diffractive design feature of multiple harmonics, with lens add powers of ~1.1, 2.2 and 3.3 D at the IOL plane; it is the 1.1 D diffractive order that is redistributed. This lens design provides approximate focal points of 60 and 40 cm for the intermediate and near foci, respectively.
The data were recorded in an Excel spreadsheet which was then imported into an MS Access database for data checking, collation and preliminary analysis (both Microsoft Corp., Redmond, WI, USA). Statistical analyses were performed using the Dell Statistica data analysis software system, version 13 (Dell, Inc., Round Rock, TX, USA). Statistical testing was completed using an analysis of variance on continuous variables and appropriate non-parametric tests on categorical data. Statistical significance was set at P=0.05.
Results
Thirty binocularly implanted subjects were successfully recruited for both trifocal groups. Eleven FV subjects received toric IOLs in both eyes, whereas another two received a toric IOL in one eye. All other FV eyes, and all PX eyes, were implanted with non-toric IOLs. Table 1 shows the preoperative demographics of each group. The only significant difference between the two groups, aside from the use of the toric IOL, was the higher number of refractive lens exchange subjects in the FV group.
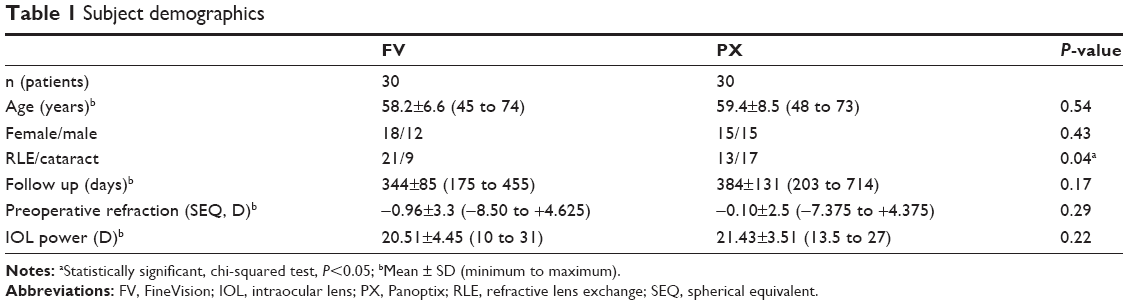 | Table 1 Subject demographics |
Table 2 shows the distribution of postoperative sphere and cylinder by IOL type. There was a statistically significantly higher likelihood of being within 0.25 or 0.50 D of emmetropia with the PX lenses relative to the FV lenses (chi-squared test, P<0.02 and P<0.01, respectively). There was no statistically significant difference in the distribution of postoperative refractive cylinder between lenses.
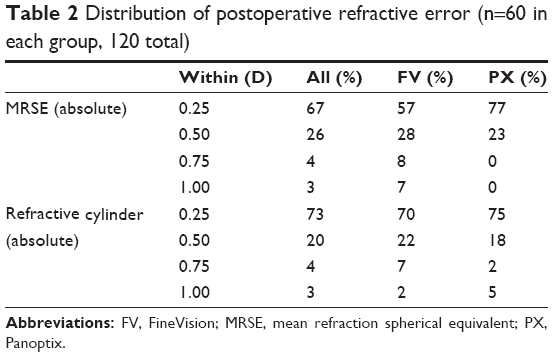 | Table 2 Distribution of postoperative refractive error (n=60 in each group, 120 total) |
Figure 1 shows the binocular defocus curve for the two lenses, with all subjects best-corrected for distance acuity (4 m). There were only three vergences where there was any statistically significant difference between the two lenses. At −1.00 D (corresponding to a viewing distance of ~80 cm, after accounting for the 4 m chart distance), the VA with the FV lens was statistically significantly better, by ~2 letters or nearly half a logMAR line (P=0.02). At vergences of −1.50 and −2.00 D (corresponding to viewing distances of ~60–45 cm) the VA with the PX lens was statistically significantly better, by ~3 letters or just over half a logMAR line (P<0.01 in both cases).
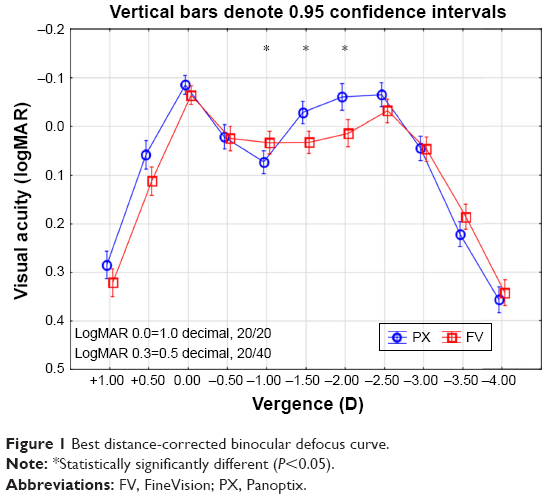 | Figure 1 Best distance-corrected binocular defocus curve. |
The binocular best distance-corrected VA at various reading distances appeared consistent with the findings in the defocus curve, though the differences between the two lenses were somewhat lower, as can be seen in Figure 2. Only the VA at 60 cm was statistically significantly different, with the PX lens having a mean VA about half a line better than the FV lens (P<0.01). Results were similar for uncorrected VA, with a statistically significant difference only at the 60 cm test distance, where the acuity with the PX lens was about half a line better (P=0.01).
 | Figure 2 Best distance-corrected visual acuity at different distances. |
Table 3 contains the summary clinical outcomes data for both of the lens groups. The postoperative refractions were not statistically significantly different between groups. Mean residual refractive cylinder was near 0.25 D in both groups.
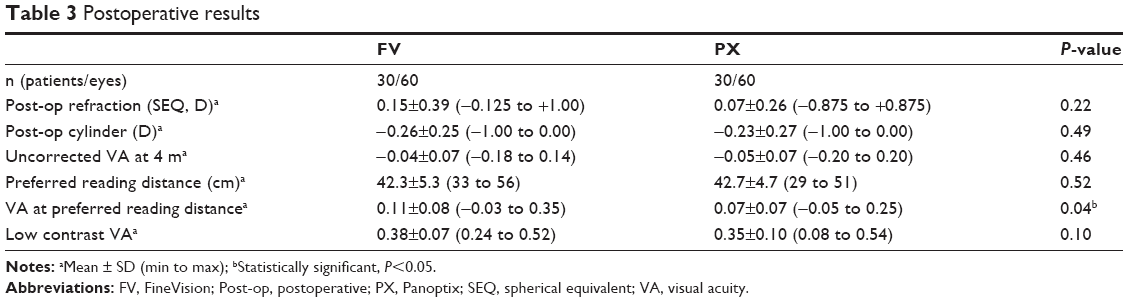 | Table 3 Postoperative results |
The preferred reading distance was tested for all subjects, along with their VA at that distance. LogMAR acuities were corrected for the actual reading distance vs the chart distance. There was no statistically significant difference in the preferred reading distance (P=0.52); subjects in both lens groups had a mean preferred reading distance between 42 and 43 cm. There was a statistically significant difference in the VA at that preferred distance, with the PX group having one letter better acuity (P=0.04), but this result is unlikely to be clinically significant. All PX subjects and all but two FV subjects had a preferred reading VA of 0.1 logMAR (20/25). The two remaining subjects had a reading VA better than 0.2 logMAR (20/32).
Binocular distance low contrast VA was also tested. There was no statistically significant difference between the groups (P=0.10). Both groups had a mean low contrast VA between 0.3 and 0.4 logMAR (20/40–20/50).
Results from the Quality of Vision questionnaire are shown in Figure 3, where lower values are better. The distribution appears to indicate the PX lenses have slightly better performance than the FV lenses, but there was no statistically significant difference between lens groups in terms of the frequency of visual disturbances (P=0.39), the severity of visual disturbances (P=0.44) or the degree to which visual disturbances bothered subjects (P=0.39). Halos were the most frequently reported phenomenon. Sixty percent (18/30) of subjects in both groups reported some degree of halos, but only four subjects (3 FV, 1 PX) reported that they were more than “a little” bothersome. That difference was not statistically significant (chi-squared test, P=0.29).
 | Figure 3 Quality of Vision results by lens. |
The NEI-Visual Function Questionnaire near vision subscale was also completed by all subjects. There was no statistically significant difference in the responses by lens group for any of the questions in that questionnaire (Mann–Whitney U-test, P>0.3 in all cases).
The potential for confounding factors to influence results was evaluated. Time since surgery was not significantly correlated to any of the outcomes above (P>0.05). There was no statistically significant difference in refractive cylinder between groups (Table 3, P=0.49), which suggests the use of toric IOLs in one group was not a significant factor. Distance best-corrected vision was also not statistically significantly different by surgery type (refractive lens exchange [RLE] or cataract surgery, P=0.14).
Discussion
The clinical results reported here were excellent for both trifocal lens designs. The acuities reported here are somewhat higher than we have seen in a previous study with the FV lens using the same procedures.9 With that noted, the VA data were collected from several different charts and appear fairly consistent (eg, the VA data collected using near cards is similar to the defocus data at near vergences, collected using the 4 m distance chart). We also confirmed using a magnified image that the 0.0 logMAR letter size was correct on the 40 cm near card. We attribute the excellent results for both lenses here to the inclusion requirement that uncorrected binocular VA be 0.3 logMAR or better, and to careful preoperative patient selection.
Previous clinical results have shown that the FV trifocal lens provides good distance, intermediate and near vision.10,11 Optical bench studies have suggested that the PX IOL might exhibit slightly better overall performance when compared with the FV lens.4,12 A correlation between optical bench image quality and VA has been demonstrated in prior research.13 On balance, results from optical bench studies should be interpreted with caution and carry less weight than prospective comparative clinical studies. Kohnen reported excellent outcomes using the PX lens in four patients with reports of low adaptation time and similar contrast sensitivity results to spherical monofocal lenses.6 Our results indicate that, except for VA at 60 cm, the clinical performance of both lenses is very similar.
The defocus curve of the FV lens is at least 0.1 logMAR better than previously reported in another study.10 That study also showed similar results with the FV lens to another bifocal lens, both showing a reduction in intermediate vision. Another study examining the FV lens found a more similar defocus curve to the current results and significantly better intermediate VA, especially at the −1.0 and −1.5 D vergences when compared with a low add bifocal lens placed in the dominant eye and a higher add bifocal lens placed in the nondominant eye.14 The disparity in results is likely at least partially explained by patient selection. Given the earlier results published by Gundersen and Potvin,14 it is likely that the results with the current trifocal lenses are significantly better than bifocal lenses alone at the intermediate vision range.
The better VA at the 60 cm intermediate distance was evident with the PX lens in both the defocus curve (at a vergence of −1.50) and the binocular corrected and uncorrected VA measured using the 60 cm chart. This appears to corroborate the expectations related to the lens design and the optical bench testing. Although the FV trifocal is constrained to have a near add which is twice that of the intermediate add, as a function of its pure trifocal design, the quadrafocal-based design of the PX lens allows for closer intermediate viewing. This may provide more visual comfort for patients using handheld devices or working with computers. Better VA between 40 and 60 cm will be more helpful to these individuals, as 80 cm is generally beyond arm’s reach for most people and greater than the highest end (30 inches or 76.2 cm) of the range generally recommended by the National Institute for Occupational Safety and Health.15 However, moving the intermediate add closer in a standard trifocal design such as the FV would require a closer near add (eg, 1.5 and 3.0 D, which would provide a near focus near 33 cm); this level of near add may not be well-tolerated by most patients.
It has been noted that the addition of a third focal point with a trifocal lens may increase halos but is unlikely to increase visual disturbances or reduce mesopic contrast sensitivity function when compared with bifocal IOLs.14,16,17 In our study, halos were the most common phenomenon reported by subjects. Halos were mostly mild in the current study so were not considered to impact quality of life significantly. However, the low contrast visual acuities reported here were similar to those we found when evaluating a variety of bifocal IOLs.9 Both of these findings appear consistent with expectation. Visual disturbances may be mitigated by the high level of light use in both trifocals; ~86% of available light is focused by the FV lens and ~88% of available light is focused by the PX lens.18
Although there were statistically more RLE cases in the FV group compared to the PX group, the age and gender were not significantly different between groups and ocular disorders were controlled by careful preoperative selection. As such, one would expect similar objective outcomes although subjective patient reporting might be expected to be slightly worse for the RLE cases, since they have been reported to have higher expectations relative to their vision after IOL implantation.19 We did not see any subjective differences in our study.
Conclusion
In summary, the two trifocal lens designs tested here provided excellent distance, intermediate and near vision, with similar quality of vision. However, the PX design provided significantly better intermediate vision at 60 cm, a distance that may be very important to users of tablets and other handheld devices.
Acknowledgments
The study was supported by an investigator-initiated study grant to IFocus Øyeklinikk AS from Alcon, Fort Worth, Texas, USA. IFocus Øyeklinikk AS provided funding to Science in Vision to assist with data analysis and preparation of this manuscript. Sarah Y Makari, OD, a consultant to Science in Vision, received compensation for providing writing assistance to the authors in preparation of the manuscript.
Preliminary findings of the study described in this paper were presented at the Winter Meeting of the European Society of Cataract and Refractive Surgeons (ESCRS) in Maastricht, The Netherlands, February 10–12, 2017. https://issuu.com/eurotimes/docs/escrsmaastricht17_finalprogramme_pr.
Disclosure
Rick Potvin is an employee of Science in Vision. The authors report no other conflicts of interest in this work.
References
Cochener B, Lafuma A, Khoshnood B, Courouve L, Berdeaux G. Comparison of outcomes with multifocal intraocular lenses: a meta-analysis. Clin Ophthalmol. 2011;5:45–56. | ||
Alfonso JF, Fernández-Vega L, Amhaz H, Montés-Micó R, Valcárcel B, Ferrer-Blasco T. Visual function after implantation of an aspheric bifocal intraocular lens. J Cataract Refract Surg. 2009;35(5):885–892. | ||
Cochener B. Prospective clinical comparison of patient outcomes following implantation of trifocal or bifocal intraocular lenses. J Refract Surg. 2016;32(3):146–151. | ||
Carson D, Xu Z, Alexander E, Choi M, Zhao Z, Hong X. Optical bench performance of 3 trifocal intraocular lenses. J Cataract Refract Surg. 2016;42(9):1361–1367. | ||
Poyales F, Garzón N, Rozema JJ, Romero C, de Zárate BO. Stability of a novel intraocular lens design: comparison of two trifocal lenses. J Refract Surg. 2016;32(6):394–402. | ||
Kohnen T. First implantation of a diffractive quadrafocal (trifocal) intraocular lens. J Cataract Refract Surg. 2015;41(10):2330–2332. | ||
National Eye Institue (NEI) [homepage on the internet]. National Eye Institute Visual Functioning Questionnaire – 25 (VFQ-25) [cited 2017 April 25]. Available from: https://nei.nih.gov/sites/default/files/nei-pdfs/vfq_sa.pdf. Accessed May 5, 2017. | ||
McAlinden C, Pesudovs K, Moore JE. The development of an instrument to measure quality of vision: the Quality of Vision (QoV) questionnaire. Invest Ophthalmol Vis Sci. 2010;51(11):5537–5545. | ||
Gundersen KG, Potvin R. Comparison of visual outcomes after implantation of a diffractive trifocal toric intraocular lens and a diffractive apodized bifocal toric intraocular lens. Clin Ophthalmol. 2016;10:455–461. | ||
Cochener B, Vryghem J, Rozot P, et al. Clinical outcomes with a trifocal intraocular lens: a multicenter study. J Refract Surg. 2014;30(11):762–768. | ||
Plaza-Puche AB, Alio JL. Analysis of defocus curves of different modern multifocal intraocular lenses. Eur J Ophthalmol. 2016;26(5):412–417. | ||
Lee S, Choi M, Xu Z, Zhao Z, Alexander E, Liu Y. Optical bench performance of a novel trifocal intraocular lens compared with a multifocal intraocular lens. Clin Ophthalmol. 2016;10:1031–1038. | ||
Plaza-Puche AB, Alió JL, MacRae S, Zheleznyak L, Sala E, Yoon G. Correlating optical bench performance with clinical defocus curves in varifocal and trifocal intraocular lenses. J Refract Surg. 2015;31(5):300–307. | ||
Gundersen KG, Potvin R. Comparison of visual outcomes and subjective visual quality after bilateral implantation of a diffractive trifocal intraocular lens and blended implantation of apodized diffractive bifocal intraocular lenses. Clin Ophthalmol. 2016;10:805–811. | ||
CDC.gov [homepage on the internet]. Health Hazard Evaluation Report September 2012 [cited February 8, 2017]. Available from: https://www.cdc.gov/niosh/hhe/reports/pdfs/2011-0149-3165.pdf. Accessed February 20, 2017. | ||
Carson D, Hill WE, Hong X, Karakelle M. Optical bench performance of AcrySof(®) IQ ReSTOR(®), AT LISA(®) tri, and FineVision(®) intraocular lenses. Clin Ophthalmol. 2014;8:2105–2113. | ||
Plaza-Puche AB, Alio JL, Sala E, Mojzis P. Impact of low mesopic contrast sensitivity outcomes in different types of modern multifocal intraocular lenses. Eur J Ophthalmol. 2016;26(6):612–617. | ||
Sheppard AL, Shah S, Bhatt U, Bhogal G, Wolffsohn JS. Visual outcomes and subjective experience after bilateral implantation of a new diffractive trifocal intraocular lens. J Cataract Refract Surg. 2013;39(3):343–349. | ||
Westin O, Koskela T, Behndig A. Epidemiology and outcomes in refractive lens exchange surgery. Acta Ophthalmol. 2015;93(1):41–45. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.