Back to Journals » International Journal of Women's Health » Volume 18
Treatment Sequencing in Platinum-Resistant Epithelial Ovarian Cancer After MIRASOL, KEYNOTE-B96, and ROSELLA
Authors Liu Y, Xu M, Ma J, Zhu Y, Gao M
Received 12 May 2026
Accepted for publication 25 June 2026
Published 10 July 2026 Volume 2026:18 624084
DOI https://doi.org/10.2147/IJWH.S624084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Yuling Liu,1,* Meng Xu,2,* Jiao Ma,1 Yu Zhu,2 Meiling Gao1
1Department of Gynecology, the First Hospital of China Medical University, Shenyang, 110001, People’s Republic of China; 2Department of Obstetrics, the First Hospital of China Medical University, Shenyang, 110001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Zhu, Department of Obstetrics, the First Hospital of China Medical University, No. 155 Nanjing North Street, Heping District, Shenyang, Liaoning Province, People’s Republic of China, Email [email protected] Meiling Gao, Department of Gynecology, the First Hospital of China Medical University, No. 155 Nanjing North Street, Heping District, Shenyang, Liaoning Province, People’s Republic of China, Email [email protected]
Abstract: Platinum-resistant epithelial ovarian cancer has long been managed as a clinically defined state with limited therapeutic differentiation. This narrative review aims to clarify how recent Phase III evidence should inform treatment allocation and sequencing after the MIRASOL, KEYNOTE-B96, and ROSELLA trials. Historically, treatment relied on non-platinum single-agent chemotherapy, with bevacizumab added for selected patients after AURELIA; however, this approach did not overcome short progression-free survival, limited response durability, cumulative toxicity, and the absence of robust biological selection. Recent randomized evidence has changed this landscape. MIRASOL established mirvetuximab soravtansine as a folate receptor alpha (FRα)-directed antibody-drug conjugate (ADC) for assay-defined FRα-positive platinum-resistant disease. KEYNOTE-B96 showed that pembrolizumab added to weekly paclitaxel, with or without bevacizumab, improves outcomes in programmed death ligand 1 (PD-L1) combined positive score (CPS)-positive platinum-resistant recurrent epithelial ovarian cancer. ROSELLA demonstrated that relacorilant, a selective glucocorticoid receptor (GR) antagonist, improves the activity of nanoparticle albumin-bound paclitaxel (nab-paclitaxel) in a population selected by clinical criteria rather than by a conventional tumor biomarker. Together, these trials define three distinct evidence anchors: FRα-targeted ADC therapy, PD-L1 CPS-selected chemoimmunotherapy, and tumor-biomarker-independent GR antagonism with nab-paclitaxel. They do not establish a simple hierarchy of preferred regimens. Instead, treatment sequencing should integrate biomarker eligibility, prior bevacizumab and poly (ADP-ribose) polymerase inhibitor exposure, taxane feasibility, ocular and immune-related toxicity risks, corticosteroid requirements, disease tempo, and patient priorities. The central challenge is to convert these validated options into rational, patient-specific sequencing strategies across biomarker-directed and tumor-biomarker-independent treatments.
Keywords: platinum-resistant ovarian cancer, treatment sequencing, folate receptor alpha, antibody-drug conjugate, mirvetuximab soravtansine, pembrolizumab, relacorilant, glucocorticoid receptor
Introduction
Epithelial ovarian cancer is commonly responsive to first-line platinum-based chemotherapy, but recurrence is frequent and recurrent disease often evolves toward treatment resistance.1 Unless otherwise specified, this review focuses on platinum-resistant epithelial ovarian, fallopian tube, and primary peritoneal cancers, which correspond to the disease populations represented in the pivotal trials discussed here. Rare ovarian cancer subtypes and non-epithelial ovarian cancers are outside the scope of this review because their biology, evidence base, and treatment advances may differ substantially. Platinum sensitivity has historically been defined by the platinum-free interval, with recurrence within six months after completion of platinum-based chemotherapy classified as platinum-resistant disease.2,3 Although this time-based definition remains useful for trial eligibility and treatment classification, it groups biologically heterogeneous tumors within a single clinical category.3 Resistance may involve restoration of homologous recombination, altered intracellular drug exposure, clonal selection, and microenvironmental remodeling, none of which is fully captured by a time-based platinum-free interval definition.4,5
Historically, treatment for platinum-resistant ovarian cancer has relied largely on non-platinum single-agent chemotherapy, with progress more incremental than transformative. Pegylated liposomal doxorubicin, topotecan, gemcitabine, and weekly paclitaxel remain active options, but their response rates and durability have generally been limited in platinum-resistant disease.6 AURELIA became a key pre-biomarker benchmark for combination therapy in this setting, showing improved progression-free survival and objective response rate with bevacizumab plus chemotherapy versus chemotherapy alone, together with patient-reported abdominal and gastrointestinal symptom benefit in selected analyses.7,8 Nevertheless, the absence of a statistically significant overall survival advantage in the original randomized comparison, together with post-progression bevacizumab exposure among patients initially assigned to chemotherapy alone, complicated interpretation of long-term benefit.9
Three trial-to-practice developments now make a more structured sequencing discussion necessary. First, mirvetuximab soravtansine has established folate receptor alpha (FRα)-directed antibody–drug conjugate therapy in FRα-positive platinum-resistant ovarian cancer. The trajectory from FORWARD I to SORAYA and MIRASOL further indicates that, for this antibody-drug conjugate (ADC) platform, clinical benefit depends on biomarker assay definition and patient enrichment rather than payload delivery alone.10–12 Second, KEYNOTE-B96 provided phase III evidence for an immunotherapy-containing regimen in platinum-resistant disease. Earlier immune checkpoint inhibitor monotherapy and alternative chemoimmunotherapy approaches did not establish a standard, whereas pembrolizumab added to weekly paclitaxel, with or without bevacizumab, improved progression-free and overall survival in patients with programmed death ligand 1(PD-L1) combined positive score (CPS) ≥1 tumors.13–16 Third, ROSELLA supports relacorilant plus nanoparticle albumin-bound paclitaxel (nab-paclitaxel) as a clinically selected, tumor-biomarker-independent strategy built on glucocorticoid receptor (GR) antagonism and taxane sensitization.17–20
These advances have shifted platinum-resistant epithelial ovarian cancer from empirical cytotoxic substitution toward treatment selection based on biomarkers, clinical eligibility, regimen feasibility, and toxicity. The aim of this review is to clarify how MIRASOL, KEYNOTE-B96, and ROSELLA should inform treatment allocation and sequencing in routine practice. We therefore examine these trials not as isolated positive trials, but as evidence anchors for FRα-targeted ADC therapy, PD-L1 CPS-selected chemoimmunotherapy, and tumor-biomarker-independent GR antagonism with nab-paclitaxel. Key efficacy results, biomarker or clinical selection criteria, toxicity considerations, and sequencing implications for the major regimens discussed in this review are summarized in Table 1.
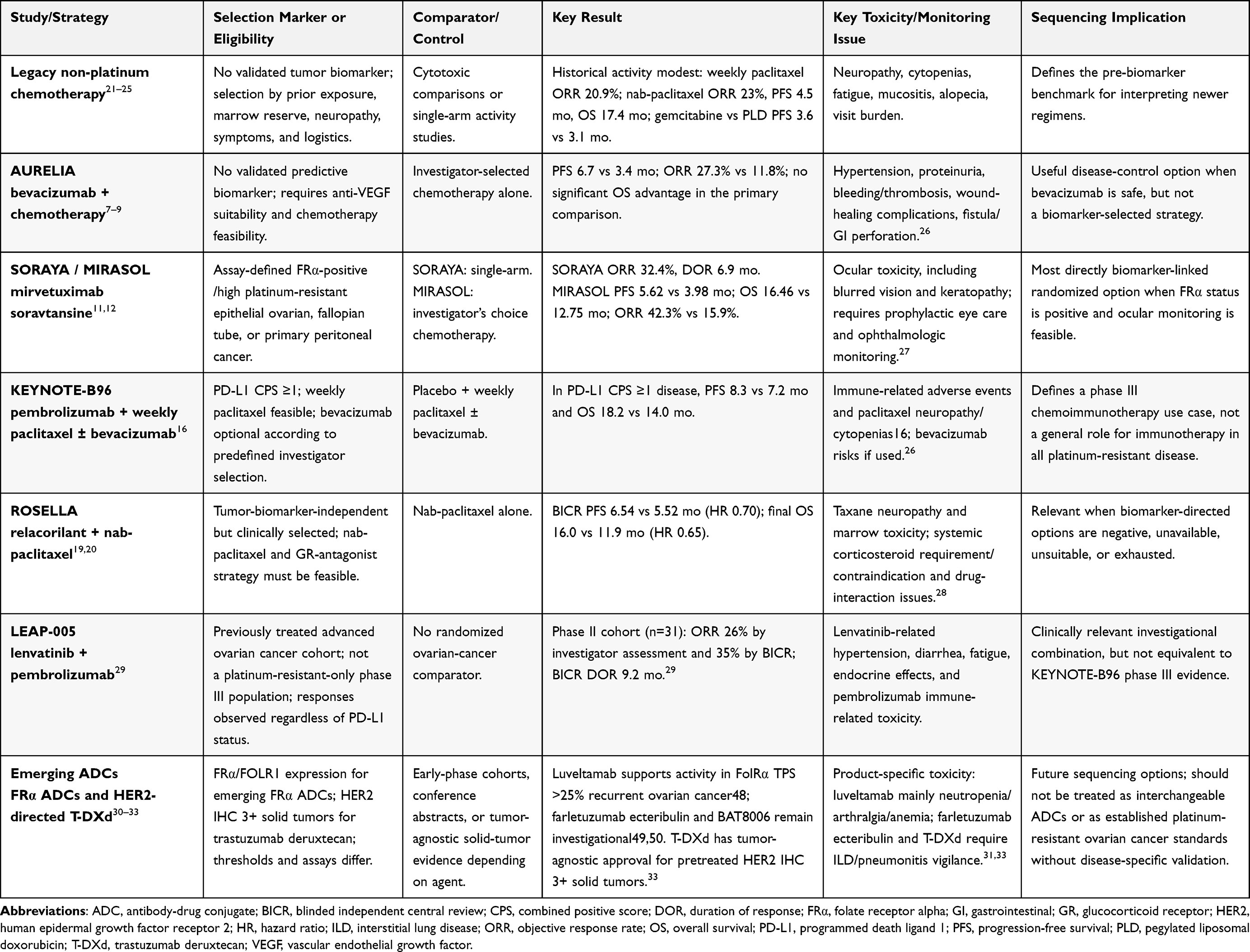 |
Table 1 Key Evidence Anchors and Selection Features for Treatment Sequencing in Platinum-Resistant Epithelial Ovarian Cancer |
The Legacy Platform: Chemotherapy and Bevacizumab Before Biomarker-Informed Selection
Before biomarker-informed treatment selection, the platinum-resistant ovarian cancer platform was shaped by randomized comparisons of non-platinum cytotoxic agents and by subsequent phase II/III studies of alternative schedules and formulations. Early randomized data compared topotecan with paclitaxel in recurrent epithelial ovarian cancer, followed by phase III comparisons involving pegylated liposomal doxorubicin and gemcitabine, as well as phase II evidence supporting weekly paclitaxel and nab-paclitaxel activity.21–25 These studies established measurable activity for several non-platinum agents without producing a biologically selected standard. The magnitude of benefit with these legacy cytotoxic options was generally modest. In an early randomized comparison of topotecan versus paclitaxel in recurrent epithelial ovarian cancer, response rates in the platinum-resistant subgroup were 13.3% versus 6.7%, respectively, and median time to progression in the overall population was 23 versus 14 weeks.21 In a phase III comparison of pegylated liposomal doxorubicin versus topotecan, overall response rates were 19.7% versus 17.0%, and median overall survival was 60.0 versus 56.7 weeks, respectively.22 In a phase II Gynecologic Oncology Group study, weekly paclitaxel produced an objective response rate of 20.9% in a platinum- and paclitaxel-resistant population.25 Nab-paclitaxel showed an objective response rate of 23%, a median progression-free survival of 4.5 months, and a median overall survival of 17.4 months in recurrent or persistent platinum-resistant ovarian, fallopian tube, or primary peritoneal cancer.24 In a randomized phase III comparison of gemcitabine versus pegylated liposomal doxorubicin in platinum-resistant disease, median progression-free survival was 3.6 versus 3.1 months, median overall survival was 12.7 versus 13.5 months, and objective response rates were 6.1% versus 8.3%, respectively.23 These outcomes provide the clinical benchmark against which more recent biomarker-directed or mechanism-defined strategies should be interpreted. In practice, treatment selection largely depended on prior exposure, residual neuropathy, marrow reserve, alopecia and mucositis considerations, expected toxicity, and treatment logistics.6
Pegylated liposomal doxorubicin gained a durable place in recurrent ovarian cancer after randomized comparison with topotecan. In the pivotal phase III study, pegylated liposomal doxorubicin showed efficacy comparable to topotecan with a distinct toxicity profile, and longer follow-up suggested an overall-survival advantage in the broader recurrent/refractory epithelial ovarian cancer population, with the clearest survival separation reported in platinum-sensitive disease.22,34 Gemcitabine was later compared with pegylated liposomal doxorubicin in platinum-resistant or short platinum-free interval recurrent populations, but these studies did not establish a clearly superior cytotoxic option.23,35 Weekly paclitaxel remained clinically useful because of its documented single-agent activity in platinum- and paclitaxel-resistant ovarian and primary peritoneal cancers.25 Nab-paclitaxel provided an active solvent-free taxane formulation in platinum-resistant ovarian cancer and, by avoiding routine corticosteroid premedication, later became a mechanistically coherent partner for relacorilant development.17,24
Bevacizumab established the principal pre-biomarker combination benchmark in platinum-resistant ovarian cancer. Early phase II data showed activity in platinum-resistant ovarian or peritoneal serous cancer, while gastrointestinal perforation emerged as a clinically important safety signal.36 AURELIA then randomized patients with platinum-resistant recurrent ovarian cancer to chemotherapy alone or chemotherapy plus bevacizumab; chemotherapy consisted of weekly paclitaxel, pegylated liposomal doxorubicin, or topotecan, selected before randomization.7 The addition of bevacizumab improved median progression-free survival from 3.4 to 6.7 months and increased Response Evaluation Criteria in Solid Tumors (RECIST) objective response from 11.8% to 27.3%.7 Patient-reported outcomes supported symptomatic benefit, with a higher proportion of patients achieving clinically meaningful improvement in abdominal/gastrointestinal symptoms during bevacizumab-containing chemotherapy.8 Exploratory analyses by chemotherapy cohort suggested benefit across backbones, with numerically prominent activity in the weekly paclitaxel cohort; however, these analyses were not designed as formal head-to-head comparisons between chemotherapy partners.37
AURELIA also defined the limitations of the pre-biomarker framework. The primary comparison did not show a statistically significant overall survival advantage, and interpretation was complicated by post-progression bevacizumab use among patients initially assigned to chemotherapy alone.7,9 AURELIA established bevacizumab-containing chemotherapy as an active disease-control regimen, although its durability and survival implications remained less clearly defined. AURELIA also showed the limits of the pre-biomarker era: anti- vascular endothelial growth factor (VEGF) therapy improved disease-control endpoints, but patient selection remained predominantly clinical rather than molecular. Bevacizumab rechallenge or continuation beyond progression has also been evaluated, but the most relevant randomized evidence comes from the platinum-sensitive rather than platinum-resistant setting. In MITO16B-MaNGO OV2B-ENGOT OV17, patients with platinum-sensitive recurrent ovarian cancer after first-line platinum-based chemotherapy plus bevacizumab had longer progression-free survival with a carboplatin-based doublet plus continued bevacizumab than with chemotherapy alone, although overall survival was not improved.38 This distinction is important because MITO16B supports the clinical relevance of bevacizumab reuse in selected platinum-sensitive recurrence, but it does not redefine bevacizumab as a biomarker-selected standard for platinum-resistant disease. Because no validated tumor biomarker predicts bevacizumab benefit in this setting, routine bevacizumab eligibility is determined mainly by clinical safety and feasibility, including blood pressure and renal toxicity risk, bleeding or thromboembolic risk, bowel involvement or obstruction, fistula/perforation risk, and recent or planned surgery.26
This historical context is essential for interpreting MIRASOL, KEYNOTE-B96, and ROSELLA, which entered a field already benchmarked by weekly paclitaxel, pegylated liposomal doxorubicin, topotecan, nab-paclitaxel, and bevacizumab-containing regimens. A credible new regimen in this setting must therefore show more than endpoint improvement; it must define the patients and treatment circumstances in which its benefit justifies use over chemotherapy alone, bevacizumab-containing therapy, or another validated option.
Biological and Clinical Heterogeneity Behind the Platinum-Resistant Label
Platinum-resistant ovarian cancer is a clinical state rather than a single biological entity. The six-month threshold remains useful for trial eligibility and therapeutic classification, but it does not define a biologically uniform disease state.3 A substantial fraction of primary high-grade serous ovarian cancers shows homologous recombination-deficient features, whereas recurrent disease may acquire resistance through restoration of DNA repair, altered intracellular drug exposure, and selection of resistant subclones.4,5,39–42
Whole-genome characterization of chemoresistant ovarian cancer demonstrated the diversity of resistance mechanisms, including structural variants, gene-disrupting events, and alterations affecting treatment sensitivity.4 Multidrug resistance can emerge through ABCB1 fusions and related mechanisms that increase drug efflux and reduce intracellular exposure to P-glycoprotein substrates, potentially limiting sensitivity to taxanes and anthracyclines.43 Restoration of homologous recombination through secondary mutations in BRCA1, BRCA2, RAD51C, or RAD51D has been repeatedly described and is clinically important because it can mediate acquired resistance to platinum agents and poly(ADP-ribose) polymerase (PARP) inhibitors.5,39–41 Circulating tumor DNA analyses have further shown that BRCA reversion mutations can be detected in association with primary or acquired PARP inhibitor resistance, supporting their use as dynamic markers of restored homologous recombination in post-PARP treatment contexts.5
This platinum-resistant biology now has direct therapeutic relevance. A tumor progressing after platinum and PARP inhibitor exposure should not be described simply as “chemotherapy-resistant”; its clinical context is better defined as platinum-resistant disease shaped by prior DNA damage-directed therapy. It may have restored DNA repair proficiency,5 acquired drug-efflux or taxane-modifying resistance pathways,43 remain eligible for antigen-directed ADC therapy if assay-defined FRα positivity is demonstrated,12 or be considered for combination strategies whose clinical benefit depends on the chemotherapy backbone, anti-angiogenic context, immune-biomarker status, and prior-treatment setting.16 Patients without an actionable surface antigen or immune biomarker may still be eligible for clinically selected, tumor-biomarker-independent approaches such as GR antagonism combined with nab-paclitaxel.17–20
Surface-antigen and immune-marker assessment further complicates this picture. FRα expression identifies patients eligible for mirvetuximab soravtansine, and the clinical trajectory from FORWARD I through SORAYA to MIRASOL underscores the importance of assay definition, expression threshold, and biomarker enrichment.10–12,44 Earlier NaPi2b-directed ADC development, particularly lifastuzumab vedotin, provides a useful counterpoint: target expression and early response signals did not translate into a definitive practice-changing regimen, reinforcing that ADC clinical utility depends on response durability, therapeutic index, payload-linker design, cutoff definition, and randomized validation.45 PD-L1 CPS has gained practical clinical relevance after KEYNOTE-B96, although its use should be interpreted within the specific trial context of weekly paclitaxel, optional bevacizumab, and defined prior-treatment exposure.16 GR signaling represents a distinct therapeutic axis, targeting stress-survival pathways linked in ovarian cancer models and early clinical development to chemotherapy resistance and taxane sensitization rather than selecting patients by tumor antigen or immune biomarker.17,46,47
Clinically, this heterogeneity argues against a single linear treatment ladder for platinum-resistant disease and supports a structured treatment-allocation assessment before each new line of therapy. At minimum, a pragmatic allocation assessment should consider FRα testing, PD-L1 CPS testing, histology, prior bevacizumab and PARP inhibitor exposure, number of prior systemic lines, taxane feasibility, residual neuropathy, ocular comorbidity, bowel involvement, and the need for systemic corticosteroids. The practical shift is from empiric chemotherapy substitution toward mechanism-informed treatment selection. The decision is no longer simply which cytotoxic agent to use next, but which combination of mechanism, eligibility profile, toxicity burden, and patient priorities best fits the next treatment line.
FRα-Targeted ADC Therapy: From FORWARD I to SORAYA and MIRASOL
FRα-targeted ADC therapy is the most clinically validated example of biomarker-directed treatment in platinum-resistant ovarian cancer, with randomized phase III evidence now supporting progression-free survival, objective response, and overall survival benefit for mirvetuximab soravtansine in assay-defined FRα-positive disease.12 FRα is frequently expressed in high-grade serous ovarian carcinoma, whereas its expression in normal tissues is comparatively limited and anatomically restricted, supporting its use as a therapeutic target.48,49 Mirvetuximab soravtansine is an FRα-targeting antibody–drug conjugate composed of an FRα-binding antibody, a cleavable linker, and the tubulin-directed maytansinoid payload DM4.44
The clinical development path was instructive rather than linear. FORWARD I was a randomized open-label phase III trial comparing mirvetuximab soravtansine with investigator’s choice chemotherapy in platinum-resistant epithelial ovarian cancer. The study did not meet its primary progression-free survival endpoint in either the intention-to-treat population or the prespecified FRα-high population. Secondary-endpoint signals in the FRα-high subgroup nevertheless supported a more stringent biomarker-enrichment strategy, making FORWARD I central to the interpretation of SORAYA and MIRASOL.10
SORAYA then evaluated mirvetuximab soravtansine in FRα-high platinum-resistant ovarian cancer in a single-arm phase II design. SORAYA required prior bevacizumab exposure, positioning mirvetuximab soravtansine in a clinically relevant post-bevacizumab platinum-resistant population. Its clinically meaningful confirmed objective responses in FRα-high disease provided the principal clinical basis for the initial accelerated-approval pathway.11 Final overall-survival and post hoc subgroup analyses from SORAYA provided descriptive support for activity across prior-treatment categories, including patients with multiple prior lines and prior PARP inhibitor exposure.50 The Clinical Cancer Research FDA approval summary remains useful for documenting the original regulatory rationale, the VENTANA FOLR1 companion-diagnostic framework, and the initial accelerated-approval context; this evidence should be distinguished from the later randomized confirmation provided by MIRASOL.44
MIRASOL provided the randomized phase III confirmation. In assay-defined FRα-positive platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer, mirvetuximab soravtansine improved progression-free survival, objective response rate, and overall survival compared with investigator’s choice chemotherapy: median progression-free survival was 5.62 versus 3.98 months, median overall survival was 16.46 versus 12.75 months, and objective response rate was 42.3% versus 15.9%, respectively.12 These results established mirvetuximab soravtansine as a marker-defined treatment with randomized evidence of survival benefit over standard single-agent chemotherapy in platinum-resistant disease.12
The value of mirvetuximab also depends on implementation. FRα testing should be completed early enough to inform next-line treatment allocation, because mirvetuximab eligibility depends on assay-defined FRα expression using an approved diagnostic framework. In practice, this requires coordination between gynecologic oncology, pathology, and molecular diagnostics.44 The therapeutic decision also requires attention to mirvetuximab-associated ocular adverse events, particularly blurred vision, keratopathy, and dry eye, which are usually manageable with supportive care and dose modification but require anticipatory eye-care planning.27 Patient-reported outcome analyses from MIRASOL help contextualize the efficacy advantage, showing broadly similar quality-of-life outcomes between mirvetuximab soravtansine and investigator’s choice chemotherapy rather than a clear patient-reported outcome superiority signal.51 In platinum-resistant disease, the combination of survival benefit, manageable toxicity, and broadly preserved patient-reported quality of life makes mirvetuximab soravtansine clinically more meaningful than a response-rate signal alone.12,27,51
Combination development is ongoing. Mirvetuximab soravtansine plus bevacizumab has shown activity in FRα-expressing platinum-resistant ovarian cancer.52 Mirvetuximab plus pembrolizumab has also been evaluated in an early-phase, non-randomized setting, although the incremental contribution of pembrolizumab remains uncertain.53 These studies do not replace MIRASOL; their current value is hypothesis-generating, with potential relevance for combination development, biomarker-overlap questions, and post-mirvetuximab sequencing strategies that still require prospective validation.52,53 Together, FORWARD I, SORAYA, and MIRASOL define the central development lesson for this platform: target expression alone is insufficient; standardized antigen testing, biologically coherent enrichment, and randomized confirmation are required to translate FRα expression into reliable clinical benefit.10–12
Other FRα-targeted ADCs are also in clinical development, but they should not be regarded as interchangeable with mirvetuximab soravtansine. Luveltamab tazevibulin (STRO-002) and farletuzumab ecteribulin (MORAb-202) illustrate how the same surface target can be paired with different antibody formats, linker technologies, payloads, dosing strategies, and toxicity profiles.30,31 Farletuzumab ecteribulin, for example, uses an eribulin payload and has required particular attention to interstitial lung disease/pneumonitis risk in ongoing development, whereas mirvetuximab soravtansine is most clearly associated with ocular toxicities requiring prophylactic eye care and ophthalmologic monitoring.31 BAT8006 is another FRα-directed ADC under clinical evaluation, with early reports suggesting antitumor activity and a toxicity profile that may differ from currently approved mirvetuximab-based therapy.32 These agents may eventually broaden FRα-directed treatment beyond the current MIRASOL-defined use case, but at present they remain investigational and should be interpreted as product-specific development programs rather than evidence-equivalent alternatives to mirvetuximab soravtansine.
Chemoimmunotherapy: From Negative Immune Checkpoint Trials to KEYNOTE-B96
Immune checkpoint blockade has produced limited and inconsistent benefit in ovarian cancer. The biological rationale is clear, with immune infiltration in a subset of high-grade serous tumors, PD-L1–related immune escape, and suppressive tumor microenvironmental programs, but these features have not translated into reliable clinical predictiveness.54 Clinical activity with single-agent PD-1 blockade, however, has generally been modest. Early nivolumab and pembrolizumab studies produced responses in only a minority of patients, with occasional durable benefit but no basis for replacing chemotherapy in an unselected platinum-resistant population.55,56
KEYNOTE-100 evaluated pembrolizumab monotherapy in advanced recurrent ovarian cancer and showed modest objective response, with higher PD-L1 CPS associated with a greater likelihood of response.13 The NINJA trial provided a direct randomized test in platinum-resistant disease by comparing nivolumab with gemcitabine or pegylated liposomal doxorubicin. Nivolumab did not improve overall survival and was associated with shorter progression-free survival than chemotherapy, although it was better tolerated.15 JAVELIN Ovarian 200 tested avelumab alone or with pegylated liposomal doxorubicin against pegylated liposomal doxorubicin alone in platinum-resistant or refractory ovarian cancer. Neither avelumab monotherapy nor avelumab plus pegylated liposomal doxorubicin improved progression-free or overall survival compared with pegylated liposomal doxorubicin alone.14 These data do not support single-agent checkpoint inhibition as a replacement for chemotherapy in unselected platinum-resistant ovarian cancer.
This limited monotherapy activity shifted attention toward combination strategies. Chemotherapy may increase immunogenic tumor-cell death and antigen presentation, whereas anti-angiogenic therapy may facilitate immune-cell trafficking through vascular normalization and remodeling of the suppressive tumor microenvironment.57 A nonrandomized phase II study of pembrolizumab with bevacizumab and oral metronomic cyclophosphamide showed clinical activity in recurrent ovarian cancer and provided a clinical signal supporting further evaluation of immunotherapy combinations.58 However, nonrandomized phase II activity was insufficient to define a standard of care.
Another relevant combination strategy is pembrolizumab plus lenvatinib, evaluated in the Phase 2 multicohort LEAP-005 study. In the ovarian cancer cohort, lenvatinib plus pembrolizumab demonstrated antitumor activity in previously treated advanced ovarian cancer without unexpected safety signals, and responses were observed regardless of PD-L1 status.29 However, this evidence differs from KEYNOTE-B96 in important ways: LEAP-005 was a phase 2, nonrandomized, later-line study, used a VEGF/FGF receptor tyrosine kinase inhibitor partner rather than a weekly paclitaxel backbone, and carries a toxicity profile shaped by lenvatinib-related adverse events such as hypertension, fatigue, diarrhea, and endocrine effects. LEAP-005 therefore supports pembrolizumab–lenvatinib as a biologically and clinically relevant investigational combination strategy, but it does not replace the randomized phase III evidence supporting pembrolizumab plus weekly paclitaxel, with or without bevacizumab, in the KEYNOTE-B96-defined PD-L1 CPS-positive population.
KEYNOTE-B96 was important because it tested pembrolizumab on the clinically familiar weekly paclitaxel backbone in a randomized, double-blind phase III design. Participants with platinum-resistant recurrent ovarian cancer after one to two prior systemic regimens received pembrolizumab or placebo plus weekly paclitaxel, with bevacizumab used according to preplanned investigator selection. In the PD-L1 CPS≥1 population, pembrolizumab improved progression-free survival and overall survival when added to weekly paclitaxel, with or without bevacizumab, compared with placebo plus the same chemotherapy backbone. Median progression-free survival was 8.3 versus 7.2 months, and median overall survival was 18.2 versus 14.0 months.16
KEYNOTE-B96 defines a specific chemoimmunotherapy use case rather than a general role for immunotherapy in all platinum-resistant ovarian cancer. Its contribution is to show that pembrolizumab can add benefit to weekly paclitaxel, with or without bevacizumab, in a PD-L1 CPS-selected population. It also supports weekly paclitaxel as a clinically effective partner for pembrolizumab in this trial context, in contrast to earlier negative monotherapy and PLD-based checkpoint-inhibitor strategies. Within this regimen, PD-L1 CPS has practical relevance as an enrichment tool, although it remains an incomplete predictor of individual benefit.
Several practical issues remain unresolved. Because bevacizumab was optional rather than mandatory in KEYNOTE-B96, pembrolizumab plus weekly paclitaxel remains the relevant backbone when bevacizumab is clinically unsuitable; bowel involvement, fistula or perforation risk, uncontrolled hypertension, and major vascular risk should weigh against bevacizumab use.26 Immune-related adverse events remain an important constraint, particularly in patients with autoimmune disease, chronic steroid exposure, frailty, or limited capacity for early symptom reporting. KEYNOTE-B96 therefore establishes a defined pembrolizumab–weekly paclitaxel strategy for selected patients with platinum-resistant recurrent ovarian cancer, with treatment allocation shaped by PD-L1 testing, paclitaxel tolerance, bevacizumab eligibility, and immune-toxicity risk.
GR Antagonism and Relacorilant: Chemotherapy Sensitization without Conventional Biomarker Selection
Relacorilant differs from FRα-directed ADC therapy and PD-1–based chemoimmunotherapy because its rationale lies in GR signaling and chemotherapy resistance rather than tumor-antigen or immune-biomarker selection. Glucocorticoid signaling can blunt chemotherapy-induced cell death in ovarian cancer models, while glucocorticoid exposure in ovarian cancer tissues has been associated with rapid upregulation of anti-apoptotic genes including SGK1 and DUSP1/MKP1.46,47,59 High tumor GR expression has been associated with shorter progression-free survival in ovarian cancer, and abnormal diurnal cortisol patterns have been linked to decreased survival in epithelial ovarian cancer.60,61 These findings supported selective GR antagonism as a taxane-sensitizing strategy.
The taxane backbone is central to this strategy. Solvent-based paclitaxel commonly requires corticosteroid premedication to reduce hypersensitivity reactions, creating a practical and pharmacologic conflict with a GR -antagonist strategy. Nab-paclitaxel is a solvent-free taxane formulation that does not require routine corticosteroid premedication and has shown single-agent activity in recurrent platinum-resistant ovarian cancer, making it a pharmacologically coherent partner for relacorilant.17,24
Preclinical work and a Phase I solid-tumor study showed that relacorilant could be combined with nab-paclitaxel and supported further ovarian cancer-specific evaluation.17 A three-arm randomized phase II study then compared intermittent relacorilant plus nab-paclitaxel, continuous relacorilant plus nab-paclitaxel, and nab-paclitaxel monotherapy in recurrent platinum-resistant ovarian cancer. The intermittent schedule improved progression-free survival and duration of response compared with nab-paclitaxel alone and generated a favorable overall-survival signal, without a substantial increase in toxicity.18 These findings led directly to the confirmatory ROSELLA trial.
ROSELLA was an open-label, randomized, controlled phase III trial comparing intermittently dosed relacorilant plus nab-paclitaxel with nab-paclitaxel alone in clinically selected, tumor-biomarker-independent platinum-resistant ovarian cancer. The combination improved blinded independent central review-assessed progression-free survival, with median progression-free survival of 6.54 versus 5.52 months and a hazard ratio of 0.70 for relacorilant plus nab-paclitaxel versus nab-paclitaxel alone.19 The final overall-survival analysis subsequently confirmed a significant survival advantage, with median overall survival of 16.0 months for relacorilant plus nab-paclitaxel versus 11.9 months for nab-paclitaxel alone and a hazard ratio for death of 0.65.20 This clinically selected but tumor-biomarker-independent design separates relacorilant from FRα-directed mirvetuximab soravtansine and PD-L1 CPS-enriched pembrolizumab-based therapy.
The absence of a tumor-biomarker requirement broadens eligibility, but patient selection remains clinically constrained. This matters when FRα- or PD-L1-directed options are negative, unavailable, unsuitable, or already exhausted, or when rapid disease progression makes additional assay turnaround clinically impractical. Selection therefore depends on prior treatment, residual toxicity, and taxane feasibility. Nab-paclitaxel may be limited by neuropathy, marrow reserve, and cumulative taxane exposure. Clinical use therefore requires attention to systemic corticosteroid requirements, potential drug-interaction considerations, endocrine context, and overlapping taxane-related toxicities. Patients requiring chronic or frequent systemic glucocorticoids were excluded from ROSELLA, and current prescribing information includes a contraindication for patients who require corticosteroids for a lifesaving indication.28 In this sense, relacorilant is tumor-biomarker-independent rather than selection-free: selection shifts from tumor assay status to treatment history, endocrine context, neuropathy risk, marrow reserve, and taxane feasibility.
ROSELLA also broadens the concept of progress in platinum-resistant ovarian cancer beyond new tumor targets. Modulating GR-mediated stress-survival signaling and chemotherapy tolerance pathways can generate clinically meaningful benefit when paired with an appropriate cytotoxic platform. This is especially relevant after PARP inhibitor and bevacizumab exposure, when subsequent treatment is often constrained by resistance biology, cumulative toxicity, and limited biomarker-matched options.
Lessons from Negative Trials and Non-Confirmatory Strategies
The recent positive trials are best interpreted against a long history of negative or non-confirmatory studies in platinum-resistant ovarian cancer. This history provides a benchmark for judging whether randomized evidence shows benefits that are clinically meaningful and implementable.62
Several biologically plausible strategies failed to improve outcomes in phase III or did not progress to practice-changing evidence. Ofranergene obadenovec (ofra-vec/VB-111), a vascular-targeted gene-based anticancer therapy, was tested with weekly paclitaxel in the placebo-controlled phase III OVAL/GOG-3018 trial. Adding ofra-vec did not improve blinded independent central review-assessed progression-free survival or overall survival versus weekly paclitaxel alone.63 The result was instructive: a familiar weekly-paclitaxel backbone did not compensate for an ineffective partner drug.
ADC development has produced similar cautionary evidence. NaPi2b-directed lifastuzumab vedotin showed that target expression and early activity do not necessarily yield a practice-changing regimen. In a randomized open-label phase II study of platinum-resistant ovarian cancer, lifastuzumab vedotin was compared with pegylated liposomal doxorubicin but did not establish a definitive practice-changing regimen despite target-directed activity.45 This experience reinforces that ADC activity in platinum-resistant ovarian cancer is product-specific and biomarker-definition dependent, not a class effect. ADCs should therefore not be treated as interchangeable therapeutic platforms when their targets, assay thresholds, construct designs, dosing strategies, and toxicity profiles differ substantially.
DNA damage response strategies remain active areas of investigation. Berzosertib, an ATR inhibitor, combined with gemcitabine produced a progression-free survival signal in a randomized phase II study of platinum-resistant high-grade serous ovarian cancer.64 Adavosertib, a WEE1 inhibitor, combined with gemcitabine also improved progression-free survival in platinum-resistant or refractory recurrent ovarian cancer in a randomized phase II setting.65 An earlier phase II study of adavosertib plus carboplatin provided clinical proof-of-concept for WEE1 inhibition in TP53-mutated ovarian cancer.66 These data are biologically coherent, particularly in high-grade serous ovarian cancer with replication-stress vulnerability, but they remain phase II signals rather than phase III standards.
Other targeted combinations have had mixed results. Pertuzumab development provides a more nuanced example: earlier gemcitabine–pertuzumab data suggested activity in platinum-resistant ovarian, fallopian tube, or primary peritoneal cancer,67 but the biomarker-selected phase III PENELOPE trial did not show a statistically significant progression-free survival improvement when pertuzumab was added to chemotherapy in low-HER3 mRNA platinum-resistant ovarian cancer.68 Cediranib–olaparib combinations have mainly informed the clinical development of anti-angiogenic/PARP inhibitor combinations in platinum-sensitive recurrent ovarian cancer, rather than defining a direct treatment standard for platinum-resistant disease.69,70 Their relevance here is interpretive: they illustrate how resistance state, biomarker context, prior therapy, and comparator choice shape whether a biologically coherent regimen becomes clinically relevant. These examples separate biological plausibility from clinical utility, showing how resistance state, biomarker selection, prior therapy, and comparator choice shape clinical relevance.
The broader lesson is that platinum-resistant ovarian cancer is an unforgiving test of drug development. A new strategy in this setting must clear a higher bar than biological plausibility. The distinction of MIRASOL, KEYNOTE-B96, and ROSELLA is that each moved beyond early activity signals into randomized phase III evidence with clinically recognizable comparators and well-defined eligibility constraints. Their value is to raise the evidentiary standard in platinum-resistant ovarian cancer while leaving sequencing, biomarker overlap, and real-world implementation unresolved.
Clinical Allocation and Sequencing of FRα-Targeted ADCs, Chemoimmunotherapy, and GR Antagonism
Current randomized evidence defines several use cases, but direct head-to-head sequencing data are lacking. Because some patients will be eligible for more than one regimen, next-line treatment must be selected according to biomarker status, prior exposure, feasibility, toxicity, disease tempo, and patient priorities. A schematic overview of this biomarker- and feasibility-based allocation approach is shown in Figure 1.
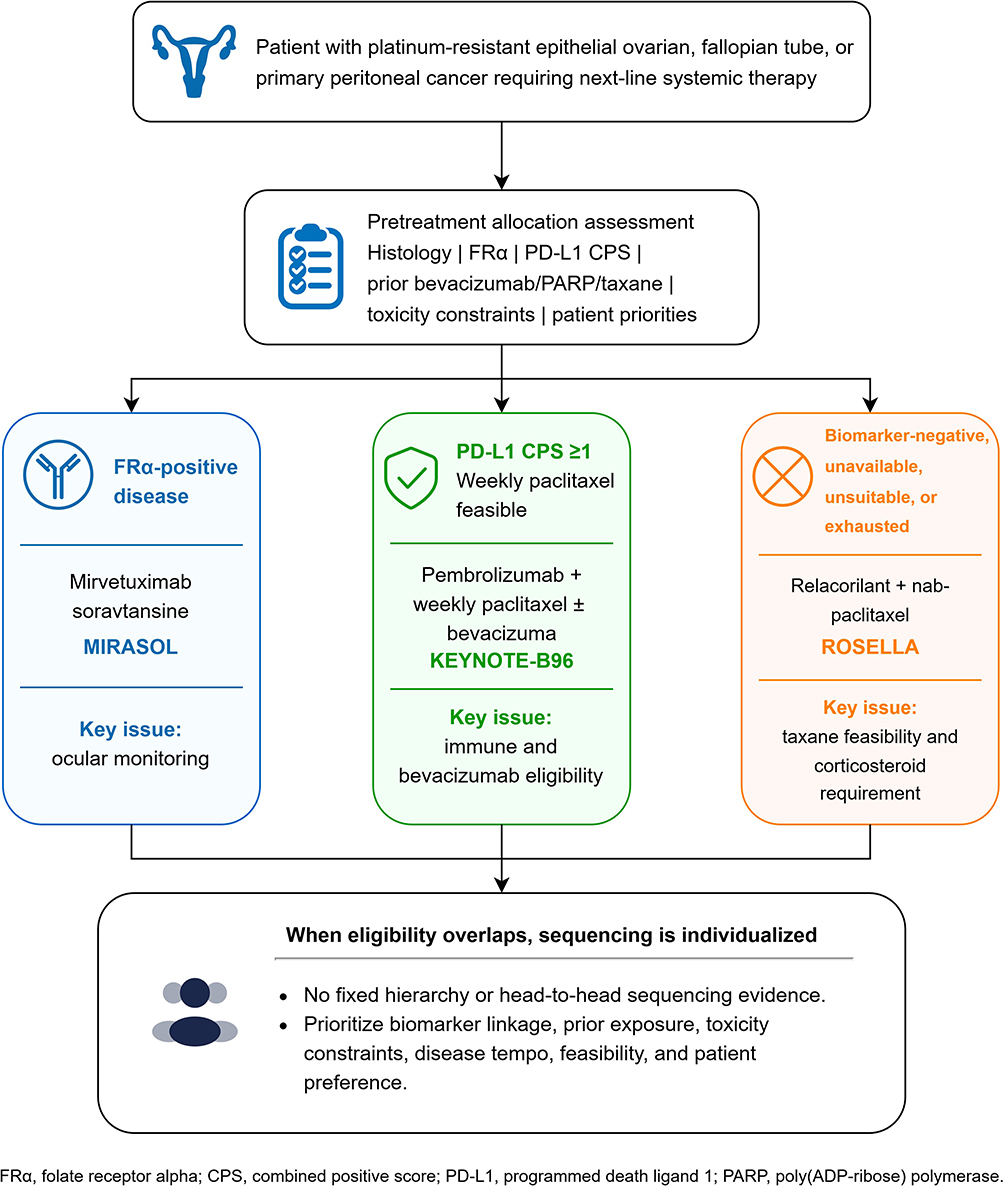 |
Figure 1 Biomarker- and feasibility-based treatment allocation after MIRASOL, KEYNOTE-B96, and ROSELLA in platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer. The schematic summarizes how recent phase III evidence has expanded treatment options according to FRα status, PD-L1 CPS status, taxane feasibility, bevacizumab suitability, corticosteroid requirements, toxicity constraints, and patient priorities. It is intended as a conceptual allocation framework rather than a fixed treatment hierarchy. Abbreviations: CPS, combined positive score; FRα, folate receptor alpha; PARP, poly(ADP-ribose) polymerase; PD-L1, programmed death ligand 1. |
FRα testing should be available before next-line treatment selection because it identifies the most directly biomarker-linked option among the regimens discussed here.44 In patients with FRα-positive platinum-resistant high-grade serous ovarian cancer after one to three prior lines, mirvetuximab soravtansine represents the most directly biomarker-linked randomized option in this setting. In MIRASOL, it improved progression-free survival, objective response rate, and overall survival compared with investigator’s choice chemotherapy.12 It is most compelling when FRα status is already documented, ocular risk is acceptable, and ophthalmologic monitoring with prophylactic eye care is feasible. Baseline corneal disease, poor adherence to eye-care measures, or limited access to timely ocular monitoring may reduce its feasibility.27 These factors do not necessarily preclude treatment, but they affect feasibility.
PD-L1 CPS testing should be incorporated into the pretreatment work-up when pembrolizumab plus weekly paclitaxel is being considered, because KEYNOTE-B96 and the subsequent regulatory indication define the demonstrated benefit in tumors with PD-L1 CPS ≥1, assessed using an authorized diagnostic framework.16 In PD-L1 CPS≥1 platinum-resistant recurrent disease after one to two prior systemic regimens, pembrolizumab plus weekly paclitaxel, with or without bevacizumab, is supported by randomized phase III evidence.16 This option is most appropriate when weekly paclitaxel is feasible and there is no major contraindication to immune checkpoint blockade. Bevacizumab can be incorporated when bowel, vascular, renal, wound-healing, and blood-pressure risks are acceptable.26 Because KEYNOTE-B96 did not separately randomize bevacizumab use, the incremental contribution of bevacizumab cannot be isolated from the pembrolizumab–weekly paclitaxel backbone.16
Relacorilant plus nab-paclitaxel occupies a different position because its use does not depend on FRα or PD-L1 status, although ROSELLA should be interpreted in relation to prior bevacizumab exposure and taxane feasibility.19 It becomes particularly relevant when biomarker-directed approaches are negative, unavailable, unsuitable, or already exhausted, provided that taxane-based therapy remains appropriate. It offers a tumor-biomarker-independent strategy supported by randomized phase III evidence.19 Its nab-paclitaxel backbone is pharmacologically coherent with GR antagonism because routine corticosteroid premedication is avoided.17,24 The main clinical constraints are residual neuropathy, marrow reserve, prior taxane intolerance, need for systemic glucocorticoids, and potential drug-interaction considerations.
Prior bevacizumab exposure informs selection but should not determine it alone. SORAYA and ROSELLA specifically studied post-bevacizumab populations, whereas MIRASOL was less restrictive with respect to prior bevacizumab exposure.11,12,19 KEYNOTE-B96 addressed a different question by incorporating bevacizumab as an optional regimen component according to preplanned investigator selection.16 The key issue is not simply whether bevacizumab has been used before, but whether anti-VEGF therapy is safe and useful now, whether the regimen under consideration depends on bevacizumab eligibility, and whether prior exposure changes the risk–benefit balance of reuse or alternative treatment.
Prior PARP inhibitor exposure is increasingly important because contemporary recurrent ovarian cancer cohorts include more patients previously treated with PARP inhibitor maintenance. In BRCA- or HRR-deficient disease, post-treatment selection can include reversion events that restore homologous recombination and reduce sensitivity to subsequent DNA damage-directed strategies. These resistance mechanisms should be distinguished from eligibility for FRα-directed ADC therapy, PD-1–based chemoimmunotherapy, or GR antagonism, but prior PARP inhibitor exposure should be captured because it affects resistance biology, prognosis, and cross-trial comparability.5,41 Subgroup analyses by prior PARP inhibitor exposure should therefore be routine in future studies.
Toxicity is a core component of treatment selection. Mirvetuximab requires ocular monitoring and adherence to prophylactic eye-care measures.27 Pembrolizumab-containing therapy requires vigilance for immune-mediated toxicities, including pneumonitis, colitis, endocrinopathies, and hepatitis.16 Bevacizumab adds clinically relevant risks of hypertension, proteinuria, thromboembolism, bleeding, wound-healing complications, fistula, and gastrointestinal perforation.26 Weekly paclitaxel and nab-paclitaxel require attention to neuropathy, alopecia, cytopenias, fatigue, and visit burden.19,24
Patient-reported outcomes are particularly important in this setting. AURELIA showed improvement in selected abdominal/gastrointestinal symptom measures with bevacizumab-containing therapy.8 MIRASOL PRO analyses further show how patient experience can be incorporated into evaluation of an efficacy-positive regimen, while avoiding overinterpretation of quality-of-life superiority.51 Platinum-resistant ovarian cancer treatment often continues across multiple lines. When efficacy differences are modest or competing options are clinically close, preservation of functional status, clinic burden, and persistent or function-limiting toxicity become decisive elements of regimen selection. Future comparisons should measure ocular symptoms, neuropathy, fatigue, abdominal symptoms, global quality of life, treatment burden, and financial toxicity with the same rigor as RECIST response.
Future Directions: Sequencing Evidence, Biomarker Overlap, and Real-World Implementation
The next evidentiary gap is sequencing. MIRASOL, KEYNOTE-B96, and ROSELLA each define an option against a control, but none establishes how these regimens should be ordered when eligibility overlaps.12,16,19 A patient with FRα-positive and PD-L1 CPS-positive disease, particularly in the context of prior bevacizumab exposure and preserved taxane feasibility, may fall within the trial-defined eligibility space for more than one validated option, including mirvetuximab soravtansine, pembrolizumab plus weekly paclitaxel, and relacorilant plus nab-paclitaxel. Until head-to-head data are available, prioritization will rely on biomarker linkage, prior exposure, disease tempo, toxicity constraints, and patient preference rather than comparative sequencing evidence. Future studies need to move beyond single-regimen efficacy toward biomarker overlap, cross-resistance, post-ADC sequencing, post-immunotherapy outcomes, prior PARP inhibitor exposure, and patient-centered trade-offs across treatment lines. The conventional six-month platinum-free interval remains useful for trial eligibility, but it should not be treated as a biologically absolute boundary.3 Patients close to the six-month threshold, those with a longer interval after the last platinum exposure, prior durable platinum benefit, slow disease tempo, limited non-platinum options, and acceptable marrow, renal, neurologic, and patient-preference considerations may still be considered for platinum rechallenge on an individualized basis.71 This issue is increasingly relevant because the new post-chemotherapy strategies discussed here—MIRASOL, KEYNOTE-B96, and ROSELLA—were developed within trial-defined platinum-resistant populations, whereas real-world recurrence often lies on a continuum between platinum-resistant and partially platinum-sensitive disease. Therefore, treatment allocation should not be framed as platinum rechallenge versus MIRASOL-, KEYNOTE-B96-, or ROSELLA-based strategies in a rigid binary manner. Instead, clinicians should integrate platinum-free interval, prior platinum response, biomarker eligibility, toxicity constraints, urgency of disease control, and patient goals when deciding whether a selected patient might reasonably receive platinum rechallenge or should instead proceed to a validated non-platinum, biomarker-directed, or mechanism-defined regimen.
Overlap between FRα expression and PD-L1 CPS deserves systematic study because the two biomarkers direct different therapeutic choices and may create sequencing dilemmas when both are present. FRα status currently points toward targeted payload delivery, while PD-L1 CPS supports chemoimmunotherapy. Whether use of one class alters the efficacy of the other remains unknown. Early non-randomized combination data support the feasibility of pairing FRα-directed ADC therapy with PD-1 blockade, but they do not establish whether prior ADC exposure alters subsequent immunotherapy efficacy, or whether chemoimmunotherapy changes FRα expression or ADC susceptibility.53 These sequencing hypotheses require prospective clinical or high-quality translational evaluation. Beyond FRα-directed development, other ADC classes may also affect future sequencing. Trastuzumab deruxtecan is a HER2-directed ADC with a tumor-agnostic accelerated approval for previously treated unresectable or metastatic HER2-positive (IHC 3+) solid tumors when no satisfactory alternative options exist.33 Its relevance to platinum-resistant ovarian cancer will depend on HER2 testing, tumor histology, prior therapy, access, and careful management of ADC-specific risks, particularly interstitial lung disease/pneumonitis.33 This example further supports the need to treat ADCs as target-, payload-, and toxicity-specific agents rather than as a single therapeutic class.
Testing infrastructure will determine whether these options can be used at the right time. FRα testing should be built around a validated immunohistochemistry framework, reproducible scoring, and pragmatic specimen-selection guidance when only older archival tissue is available or when tumor heterogeneity is suspected.44,72 PD-L1 CPS testing has become operationally relevant in this setting after KEYNOTE-B96, but its integration into platinum-resistant ovarian cancer workflows will still require coordination among oncology, pathology, and treatment-scheduling teams. Turnaround time is clinically important because platinum-resistant disease often progresses quickly. A clinically useful testing pathway should return FRα and PD-L1 results early enough to inform next-line allocation rather than after treatment fitness or regimen feasibility has already narrowed.
Prior PARP inhibitor exposure should be incorporated more explicitly into trial design and reporting. Many older platinum-resistant studies enrolled patients before widespread frontline PARP inhibitor maintenance. Current patients may have different resistance biology, including post-treatment reversion events that restore homologous recombination, as well as different treatment histories and cumulative-toxicity profiles.5 Future trials should prespecify and report prior PARP inhibitor exposure, prior bevacizumab exposure, taxane-free interval, and number of prior lines wherever feasible, because these variables increasingly affect both trial comparability and clinical interpretation.
Cost and access will shape how much of this trial benefit reaches routine practice. ADC therapy requires antigen testing, drug access, infusion resources, ocular monitoring, and toxicity management. Chemoimmunotherapy requires PD-L1 testing and long-term management of immune-related adverse events. In settings where relacorilant-based treatment is approved and accessible, implementation will require access to an oral GR antagonist, coordination with nab-paclitaxel delivery, and attention to corticosteroid-related contraindications and endocrine-risk management. These regimens therefore impose different diagnostic, monitoring, toxicity-management, and access burdens. Health-economic analyses will be necessary, but they cannot substitute for clinical selection. The first task remains to identify which patient is most likely to benefit from which regimen.
Negative and non-confirmatory studies should remain part of the field’s interpretive framework. VB-111, early immune-checkpoint strategies, and selected targeted combinations all carried plausible rationales but did not establish practice-changing benefit in platinum-resistant ovarian cancer.14,15,63,68 Their limitations are instructive because they reinforce the need for randomized validation, reproducible biomarker frameworks, acceptable tolerability, and clinically meaningful patient-centered outcomes in platinum-resistant ovarian cancer.
Conclusion
Platinum-resistant epithelial ovarian cancer should no longer be approached only as a setting for empiric non-platinum chemotherapy substitution. Single-agent chemotherapy and bevacizumab-containing therapy remain clinically relevant options, but MIRASOL, KEYNOTE-B96, and ROSELLA have clarified three distinct evidence-based strategies: FRα-directed antibody-drug conjugate therapy, PD-L1 CPS-selected chemoimmunotherapy, and tumor-biomarker-independent GR antagonism combined with nab-paclitaxel. These trials do not establish a fixed hierarchy of preferred regimens; rather, they show that treatment sequencing should be individualized according to biomarker eligibility, prior bevacizumab and PARP inhibitor exposure, taxane feasibility, ocular and immune-related toxicity risks, corticosteroid requirements, disease tempo, and patient goals. Future work should define optimal sequencing, biomarker overlap, post-ADC and post-immunotherapy outcomes, and practical testing pathways so that these validated regimens can be matched to the right patient at the right treatment line.
AI Declaration
Authors declare no use of generative AI in the manuscript preparation process.
Abbreviations
ADC, antibody-drug conjugate; CPS, combined positive score; FRα, folate receptor alpha; GR, glucocorticoid receptor; nab-paclitaxel, nanoparticle albumin-bound paclitaxel; PD-L1, programmed death ligand 1; PD-1, programmed cell death 1; PARP, poly(ADP-ribose) polymerase; RECIST, Response Evaluation Criteria in Solid Tumors; VEGF, vascular endothelial growth factor.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Lheureux S, Gourley C, Vergote I, Oza AM. Epithelial ovarian cancer. Lancet. 2019;393(10177):1240–17. doi:10.1016/s0140-6736(18)32552-2
2. Eisenhauer EA, Vermorken JB, van Glabbeke M. Predictors of response to subsequent chemotherapy in platinum pretreated ovarian cancer: a multivariate analysis of 704 patients. Ann Oncol. 1997;8(10):963–968. doi:10.1023/a:1008240421028
3. Davis A, Tinker AV, Friedlander M. “Platinum resistant” ovarian cancer: what is it, who to treat and how to measure benefit? Gynecol Oncol. 2014;133(3):624–631. doi:10.1016/j.ygyno.2014.02.038
4. Patch AM, Christie EL, Etemadmoghadam D, et al. Whole-genome characterization of chemoresistant ovarian cancer. Nature.;521(7553):489–494. doi:10.1038/nature14410.
5. Lin KK, Harrell MI, Oza AM, et al. BRCA reversion mutations in circulating tumor DNA predict primary and acquired resistance to the PARP inhibitor rucaparib in high-grade ovarian carcinoma. Cancer Discov. 2019;9(2):210–219. doi:10.1158/2159-8290.Cd-18-0715
6. St Laurent J, Liu JF. Treatment approaches for platinum-resistant ovarian cancer. J Clin Oncol. 2024;42(2):127–133. doi:10.1200/jco.23.01771
7. Pujade-Lauraine E, Hilpert F, Weber B, et al. Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: the AURELIA open-label randomized phase III trial. J Clin Oncol. 2014;32(13):1302–1308. doi:10.1200/jco.2013.51.4489
8. Stockler MR, Hilpert F, Friedlander M, et al. Patient-reported outcome results from the open-label phase III AURELIA trial evaluating bevacizumab-containing therapy for platinum-resistant ovarian cancer. J Clin Oncol. 2014;32(13):1309–1316. doi:10.1200/jco.2013.51.4240
9. Bamias A, Gibbs E, Khoon Lee C, et al. Bevacizumab with or after chemotherapy for platinum-resistant recurrent ovarian cancer: exploratory analyses of the AURELIA trial. Ann Oncol. 2017;28(8):1842–1848. doi:10.1093/annonc/mdx228
10. Moore KN, Oza AM, Colombo N, et al. Phase III, randomized trial of mirvetuximab soravtansine versus chemotherapy in patients with platinum-resistant ovarian cancer: primary analysis of FORWARD I. Ann Oncol. 2021;32(6):757–765. doi:10.1016/j.annonc.2021.02.017
11. Matulonis UA, Lorusso D, Oaknin A, et al. Efficacy and safety of mirvetuximab soravtansine in patients with platinum-resistant ovarian cancer with high folate receptor alpha expression: results from the SORAYA study. J Clin Oncol. 2023;41(13):2436–2445. doi:10.1200/jco.22.01900
12. Moore KN, Angelergues A, Konecny GE, et al. Mirvetuximab soravtansine in FRα-positive, platinum-resistant ovarian cancer. N Engl J Med. 2023;389(23):2162–2174. doi:10.1056/NEJMoa2309169
13. Matulonis UA, Shapira-Frommer R, Santin AD, et al. Antitumor activity and safety of pembrolizumab in patients with advanced recurrent ovarian cancer: results from the phase II KEYNOTE-100 study. Ann Oncol.;30(7):1080–1087. doi:10.1093/annonc/mdz135.
14. Pujade-Lauraine E, Fujiwara K, Ledermann JA, et al. Avelumab alone or in combination with chemotherapy versus chemotherapy alone in platinum-resistant or platinum-refractory ovarian cancer (JAVELIN Ovarian 200): an open-label, three-arm, randomised, Phase 3 study. Lancet Oncol. 2021;22(7):1034–1046. doi:10.1016/s1470-2045(21)00216-3
15. Hamanishi J, Takeshima N, Katsumata N, et al. Nivolumab versus gemcitabine or pegylated liposomal doxorubicin for patients with platinum-resistant ovarian cancer: open-label, randomized trial in Japan (NINJA). J Clin Oncol. 2021;39(33):3671–3681. doi:10.1200/jco.21.00334
16. Colombo N, Zsiros E, Parma G, et al. Pembrolizumab plus weekly paclitaxel in platinum-resistant recurrent ovarian cancer (ENGOT-ov65/KEYNOTE-B96): a multicentre, randomised, double-blind, phase 3 study. Lancet. 2026;407(10538):1525–1537. doi:10.1016/s0140-6736(26)00602-1
17. Munster PN, Greenstein AE, Fleming GF, et al. Overcoming taxane resistance: preclinical and phase 1 studies of relacorilant, a selective glucocorticoid receptor modulator, with nab-paclitaxel in solid tumors. Clin Cancer Res. 2022;28(15):3214–3224. doi:10.1158/1078-0432.Ccr-21-4363
18. Colombo N, Van Gorp T, Matulonis UA, et al. Relacorilant + Nab-Paclitaxel in patients with recurrent, platinum-resistant ovarian cancer: a three-arm, randomized, controlled, open-label phase II study. J Clin Oncol. 2023;41(30):4779–4789. doi:10.1200/jco.22.02624
19. Olawaiye AB, Gladieff L, O’Malley DM, et al. Relacorilant and nab-paclitaxel in patients with platinum-resistant ovarian cancer (ROSELLA): an open-label, randomised, controlled, phase 3 trial. Lancet. 2025;405(10496):2205–2216. doi:10.1016/s0140-6736(25)01040-2
20. Lorusso D, Gladieff L, O’Malley DM, et al. Overall survival with relacorilant and nab-paclitaxel in patients with platinum-resistant ovarian cancer (ROSELLA): a phase 3 randomised controlled trial. Lancet. 2026;407(10538):1513–1524. doi:10.1016/s0140-6736(26)00462-9
21. Ten Bokkel Huinink W, Gore M, Carmichael J, et al. Topotecan versus paclitaxel for the treatment of recurrent epithelial ovarian cancer. J Clin Oncol. 1997;15(6):2183–2193. doi:10.1200/jco.1997.15.6.2183
22. Gordon AN, Fleagle JT, Guthrie D, Parkin DE, Gore ME, Lacave AJ. Recurrent epithelial ovarian carcinoma: a randomized phase III study of pegylated liposomal doxorubicin versus topotecan. J Clin Oncol. 2001;19(14):3312–3322. doi:10.1200/jco.2001.19.14.3312
23. Mutch DG, Orlando M, Goss T, et al. Randomized phase III trial of gemcitabine compared with pegylated liposomal doxorubicin in patients with platinum-resistant ovarian cancer. J Clin Oncol. 2007;25(19):2811–2818. doi:10.1200/jco.2006.09.6735
24. Coleman RL, Brady WE, McMeekin DS, et al. A phase II evaluation of nanoparticle, albumin-bound (nab) paclitaxel in the treatment of recurrent or persistent platinum-resistant ovarian, fallopian tube, or primary peritoneal cancer: a Gynecologic Oncology Group study. Gynecol Oncol. 2011;122(1):111–115. doi:10.1016/j.ygyno.2011.03.036
25. Markman M, Blessing J, Rubin SC, Connor J, Hanjani P, Waggoner S. Phase II trial of weekly paclitaxel (80 mg/m2) in platinum and paclitaxel-resistant ovarian and primary peritoneal cancers: a Gynecologic Oncology Group study. Gynecol Oncol. 2006;101(3):436–440. doi:10.1016/j.ygyno.2005.10.036
26. Randall LM, Monk BJ. Bevacizumab toxicities and their management in ovarian cancer. Gynecol Oncol. 2010;117(3):497–504. doi:10.1016/j.ygyno.2010.02.021
27. Moore KN, Lorusso D, Oaknin A, et al. Safety and tolerability of mirvetuximab soravtansine monotherapy for folate receptor alpha-expressing recurrent ovarian cancer: an integrated safety summary. Gynecol Oncol. 2024;191:249–258. doi:10.1016/j.ygyno.2024.10.013
28. Olawaiye AB, Kim JW, Bagameri A, et al. Clinical Trial Protocol for ROSELLA: a phase 3 study of relacorilant in combination with nab-paclitaxel versus nab-paclitaxel monotherapy in advanced platinum-resistant ovarian cancer. J Gynecol Oncol. 2024;35(4):e111. doi:10.3802/jgo.2024.35.e111
29. González-Martín A, Chung HC, Saada-Bouzid E, et al. Lenvatinib plus pembrolizumab for patients with previously treated advanced ovarian cancer: results from the phase 2 multicohort LEAP-005 study. Gynecol Oncol. 2024;186:182–190. doi:10.1016/j.ygyno.2024.04.011
30. Oaknin A, Fariñas-Madrid L, García-Duran C, et al. Luveltamab tazevibulin (STRO-002), an anti-folate receptor alpha (FolRα) antibody drug conjugate (ADC), safety and efficacy in a broad distribution of FolRα expression in patients with recurrent epithelial ovarian cancer (OC): update of STRO-002-GM1 phase 1 dose expansion cohort. J Clin Oncol. 2023;41(16_suppl):5508. doi:10.1200/JCO.2023.41.16_suppl.5508
31. Yonemori K, Yunokawa M, Matsumoto K, et al. Clinical trial of safety and antitumor activity of farletuzumab ecteribulin in patients with platinum-resistant ovarian cancer: phase I expansion results. Int J Gynaecol Obstet. 2026;173(3):1334–1342. doi:10.1002/ijgo.70676
32. Zhang S, Jia H, Liu J, et al. Safety and efficacy of BAT8006, a folate receptor α (FRα) antibody drug conjugate, in patients with platinum-resistant ovarian cancer: update on the dose optimization/expansion cohort of BAT-8006-001-CR trial. J Clin Oncol. 2025;43(16_suppl):5517. doi:10.1200/JCO.2025.43.16_suppl.5517
33. U.S. Food and Drug Administration. FDA grants accelerated approval to fam-trastuzumab deruxtecan-nxki for unresectable or metastatic HER2-positive solid tumors. Internet. U.S. Food and Drug Administration. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-fam-trastuzumab-deruxtecan-nxki-unresectable-or-metastatic-her2.
34. Gordon AN, Tonda M, Sun S, Rackoff W. Long-term survival advantage for women treated with pegylated liposomal doxorubicin compared with topotecan in a phase 3 randomized study of recurrent and refractory epithelial ovarian cancer. Gynecol Oncol. 2004;95(1):1–8. doi:10.1016/j.ygyno.2004.07.011
35. Ferrandina G, Ludovisi M, Lorusso D, et al. Phase III trial of gemcitabine compared with pegylated liposomal doxorubicin in progressive or recurrent ovarian cancer. J Clin Oncol. 2008;26(6):890–896. doi:10.1200/jco.2007.13.6606
36. Cannistra SA, Matulonis UA, Penson RT, et al. Phase II study of bevacizumab in patients with platinum-resistant ovarian cancer or peritoneal serous cancer. J Clin Oncol. 2007;25(33):5180–5186. doi:10.1200/jco.2007.12.0782
37. Poveda AM, Selle F, Hilpert F, et al. Bevacizumab combined with weekly paclitaxel, pegylated liposomal doxorubicin, or topotecan in platinum-resistant recurrent ovarian cancer: analysis by chemotherapy cohort of the randomized Phase III AURELIA trial. J Clin Oncol. 2015;33(32):3836–3838. doi:10.1200/jco.2015.63.1408
38. Pignata S, Lorusso D, Joly F, et al. Carboplatin-based doublet plus bevacizumab beyond progression versus carboplatin-based doublet alone in patients with platinum-sensitive ovarian cancer: a randomised, phase 3 trial. Lancet Oncol. 2021;22(2):267–276. doi:10.1016/s1470-2045(20)30637-9
39. Norquist B, Wurz KA, Pennil CC, et al. Secondary somatic mutations restoring BRCA1/2 predict chemotherapy resistance in hereditary ovarian carcinomas. J Clin Oncol. 2011;29(22):3008–3015. doi:10.1200/jco.2010.34.2980
40. Sakai W, Swisher EM, Karlan BY, et al. Secondary mutations as a mechanism of cisplatin resistance in BRCA2-mutated cancers. Nature. 2008;451(7182):1116–1120. doi:10.1038/nature06633
41. Kondrashova O, Nguyen M, Shield-Artin K, et al. Secondary somatic mutations restoring RAD51C and RAD51D associated with acquired resistance to the PARP inhibitor rucaparib in high-grade ovarian carcinoma. Cancer Discov. 2017;7(9):984–998. doi:10.1158/2159-8290.Cd-17-0419
42. Network CGAR. Integrated genomic analyses of ovarian carcinoma. Nature. 2011;474(7353):609–615. doi:10.1038/nature10166.
43. Christie EL, Pattnaik S, Beach J, et al. Multiple ABCB1 transcriptional fusions in drug resistant high-grade serous ovarian and breast cancer. Nat Commun. 2019;10(1):1295. doi:10.1038/s41467-019-09312-9
44. Dilawari A, Shah M, Ison G, et al. FDA approval summary: mirvetuximab Soravtansine-Gynx for FRα-positive, platinum-resistant ovarian cancer. Clin Cancer Res. 2023;29(19):3835–3840. doi:10.1158/1078-0432.Ccr-23-0991
45. Banerjee S, Oza AM, Birrer MJ, et al. Anti-NaPi2b antibody-drug conjugate lifastuzumab vedotin (DNIB0600A) compared with pegylated liposomal doxorubicin in patients with platinum-resistant ovarian cancer in a randomized, open-label, phase II study. Ann Oncol. 2018;29(4):917–923. doi:10.1093/annonc/mdy023
46. Sui M, Chen F, Chen Z, Fan W. Glucocorticoids interfere with therapeutic efficacy of paclitaxel against human breast and ovarian xenograft tumors. Int J Cancer. 2006;119(3):712–717. doi:10.1002/ijc.21743
47. Stringer-Reasor EM, Baker GM, Skor MN, et al. Glucocorticoid receptor activation inhibits chemotherapy-induced cell death in high-grade serous ovarian carcinoma. Gynecol Oncol. 2015;138(3):656–662. doi:10.1016/j.ygyno.2015.06.033
48. Kalli KR, Oberg AL, Keeney GL, et al. Folate receptor alpha as a tumor target in epithelial ovarian cancer. Gynecol Oncol. 2008;108(3):619–626. doi:10.1016/j.ygyno.2007.11.020
49. O’Shannessy DJ, Somers EB, Wang LC, Wang H, Hsu R. Expression of folate receptors alpha and beta in normal and cancerous gynecologic tissues: correlation of expression of the beta isoform with macrophage markers. J Ovarian Res. 2015;8:29. doi:10.1186/s13048-015-0156-0
50. Coleman RL, Lorusso D, Oaknin A, et al. Mirvetuximab soravtansine in folate receptor alpha (FRα)-high platinum-resistant ovarian cancer: final overall survival and post hoc sequence of therapy subgroup results from the SORAYA trial. Int J Gynecol Cancer. 2024;34(8):1119–1125. doi:10.1136/ijgc-2024-005401
51. Van Gorp T, Moore KN, Konecny GE, et al. Patient-reported outcomes from the MIRASOL trial evaluating mirvetuximab soravtansine versus chemotherapy in patients with folate receptor α-positive, platinum-resistant ovarian cancer: a randomised, open-label, phase 3 trial. Lancet Oncol. 2025;26(4):503–515. doi:10.1016/s1470-2045(25)00021-x
52. Gilbert L, Oaknin A, Matulonis UA, et al. Safety and efficacy of mirvetuximab soravtansine, a folate receptor alpha (FRα)-targeting antibody-drug conjugate (ADC), in combination with bevacizumab in patients with platinum-resistant ovarian cancer. Gynecol Oncol. 2023;170:241–247. doi:10.1016/j.ygyno.2023.01.020
53. Matulonis UA, Vergote I, Moore KN, et al. Safety and efficacy of mirvetuximab soravtansine, a folate receptor alpha (FRα)-targeting antibody-drug conjugate (ADC), in combination with pembrolizumab in patients with platinum-resistant ovarian cancer. Gynecol Oncol. 2025;200:96–104. doi:10.1016/j.ygyno.2025.06.016
54. Leary A, Tan D, Ledermann J. Immune checkpoint inhibitors in ovarian cancer: where do we stand? Ther Adv Med Oncol. 2021;13:17588359211039899. doi:10.1177/17588359211039899
55. Hamanishi J, Mandai M, Ikeda T, et al. Safety and antitumor activity of anti-PD-1 antibody, nivolumab, in patients with platinum-resistant ovarian cancer. J Clin Oncol.;33(34):4015–4022. doi:10.1200/jco.2015.62.3397.
56. Varga A, Piha-Paul S, Ott PA, et al. Pembrolizumab in patients with programmed death ligand 1-positive advanced ovarian cancer: analysis of KEYNOTE-028. Gynecol Oncol. 2019;152(2):243–250. doi:10.1016/j.ygyno.2018.11.017
57. Fukumura D, Kloepper J, Amoozgar Z, Duda DG, Jain RK. Enhancing cancer immunotherapy using antiangiogenics: opportunities and challenges. Nat Rev Clin Oncol. 2018;15(5):325–340. doi:10.1038/nrclinonc.2018.29
58. Zsiros E, Lynam S, Attwood KM, et al. Efficacy and safety of pembrolizumab in combination with bevacizumab and oral metronomic cyclophosphamide in the treatment of recurrent ovarian cancer: a Phase 2 nonrandomized clinical trial. JAMA Oncol. 2021;7(1):78–85. doi:10.1001/jamaoncol.2020.5945
59. Melhem A, Yamada SD, Fleming GF, et al. Administration of glucocorticoids to ovarian cancer patients is associated with expression of the anti-apoptotic genes SGK1 and MKP1/DUSP1 in ovarian tissues. Clin Cancer Res. 2009;15(9):3196–3204. doi:10.1158/1078-0432.Ccr-08-2131
60. Veneris JT, Darcy KM, Mhawech-Fauceglia P, et al. High glucocorticoid receptor expression predicts short progression-free survival in ovarian cancer. Gynecol Oncol. 2017;146(1):153–160. doi:10.1016/j.ygyno.2017.04.012
61. Schrepf A, Thaker PH, Goodheart MJ, et al. Diurnal cortisol and survival in epithelial ovarian cancer. Psychoneuroendocrinology. 2015;53:256–267. doi:10.1016/j.psyneuen.2015.01.010
62. Martorana F, Pavone G, Sessa C, Treglia G, Lheureux S, Colombo I. Can we learn from failures? A systematic review of phase III trials in platinum-resistant ovarian cancer. Int J Gynecol Cancer. 2025;35(1):100009. doi:10.1016/j.ijgc.2024.100009
63. Arend RC, Monk BJ, Shapira-Frommer R, et al. Ofranergene obadenovec (Ofra-Vec, VB-111) with weekly paclitaxel for platinum-resistant ovarian cancer: randomized controlled phase III trial (OVAL Study/GOG 3018). J Clin Oncol. 2024;42(2):170–179. doi:10.1200/jco.22.02915
64. Konstantinopoulos PA, Cheng SC, Wahner Hendrickson AE, et al. Berzosertib plus gemcitabine versus gemcitabine alone in platinum-resistant high-grade serous ovarian cancer: a multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2020;21(7):957–968. doi:10.1016/s1470-2045(20)30180-7
65. Lheureux S, Cristea MC, Bruce JP, et al. Adavosertib plus gemcitabine for platinum-resistant or platinum-refractory recurrent ovarian cancer: a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet. 2021;397(10271):281–292. doi:10.1016/s0140-6736(20)32554-x
66. Leijen S, van Geel RM, Sonke GS, et al. Phase II study of WEE1 inhibitor AZD1775 plus carboplatin in patients with TP53-mutated ovarian cancer refractory or resistant to first-line therapy within 3 months. J Clin Oncol. 2016;34(36):4354–4361. doi:10.1200/jco.2016.67.5942
67. Makhija S, Amler LC, Glenn D, et al. Clinical activity of gemcitabine plus pertuzumab in platinum-resistant ovarian cancer, fallopian tube cancer, or primary peritoneal cancer. J Clin Oncol. 2010;28(7):1215–1223. doi:10.1200/jco.2009.22.3354
68. Kurzeder C, Bover I, Marmé F, et al. Double-blind, placebo-controlled, randomized phase iii trial evaluating pertuzumab combined with chemotherapy for low tumor human epidermal growth factor receptor 3 mRNA-expressing platinum-resistant ovarian cancer (PENELOPE). J Clin Oncol. 2016;34(21):2516–2525. doi:10.1200/jco.2015.66.0787
69. Liu JF, Barry WT, Birrer M, et al. Combination cediranib and olaparib versus olaparib alone for women with recurrent platinum-sensitive ovarian cancer: a randomised phase 2 study. Lancet Oncol. 2014;15(11):1207–1214. doi:10.1016/s1470-2045(14)70391-2
70. Liu JF, Brady MF, Matulonis UA, et al. Olaparib with or without cediranib versus platinum-based chemotherapy in recurrent platinum-sensitive ovarian cancer (NRG-GY004): a randomized, open-label, Phase III trial. J Clin Oncol. 2022;40(19):2138–2147. doi:10.1200/jco.21.02011
71. Valenza C, Mongillo M, Visconti MV, et al. Rechallenge with platinum-based chemotherapy in patients with platinum-resistant ovarian carcinoma: a cohort study. Gynecol Oncol. 2025;194:11–17. doi:10.1016/j.ygyno.2025.01.014
72. Martin LP, Konner JA, Moore KN, et al. Characterization of folate receptor alpha (FRα) expression in archival tumor and biopsy samples from relapsed epithelial ovarian cancer patients: a phase I expansion study of the FRα-targeting antibody-drug conjugate mirvetuximab soravtansine. Gynecol Oncol. 2017;147(2):402–407. doi:10.1016/j.ygyno.2017.08.015
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.