Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Treatment Challenges in Refractory Urticarial Vasculitis
Received 8 November 2025
Accepted for publication 25 January 2026
Published 7 February 2026 Volume 2026:19 579985
DOI https://doi.org/10.2147/CCID.S579985
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Lisha Sun,1 Qiao Yu,2 Xinlong Chen2
1Department of Endocrinology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Department of Dermatology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China
Correspondence: Xinlong Chen, Department of Dermatology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China, Email [email protected]
Abstract: Urticarial vasculitis, a rare autoimmune disease, is characterized by inflammation of the small blood vessels. It presents with skin lesions that resemble hives, but unlike ordinary hives, these lesions last longer than 24 hours, may leave behind bruise-like discoloration or purpura, and can be associated with systemic symptoms. This case reports details a middle-aged female patient, who exhibited extensive urticarial lesions persisting for two weeks and severe reactions to initial treatments.
Keywords: refractory urticarial vasculitis, omalizumab, immunosuppressants
Introduction
Urticarial vasculitis (UV), a rare autoimmune disease, is characterized by inflammation of the small blood vessels. It presents with skin lesions that resemble hives, but unlike ordinary hives, these lesions last longer than 24 hours, may leave behind bruise-like discoloration or purpura, and can be associated with systemic symptoms.1 Diagnostic complexity in UV arises from its clinical mimicry of other conditions, particularly chronic urticaria and autoimmune disorders, posing a significant challenge for effective clinical management.2
The diagnostic process typically involves a clinical evaluation. A skin biopsy can confirm the diagnosis by demonstrating histopathological features of vasculitis.3 Studies have shown that the incidence of UV in patients with chronic urticaria is 2.7%.4 The treatment measures include corticosteroids, antihistamines, chloroquine, non-steroidal anti-inflammatory drugs, colchicine and azathioprine, omalizumab.4,5
Significant clinical amelioration in severe UV with omalizumab treatment has been documented, stemming from its underlying pathway of IgE binding and subsequent modulation of mast cell degranulation.5,6 The development of innovative treatments and combination strategies remains crucial, as scientific knowledge of UV continues to advance. Cyclosporine exerts its effect by forming a complex with cyclophilin, which leads to the inhibition of calcineurin and consequently suppresses the initial stage of the immune response. Although its initial indication was the prevention of organ transplant rejection, its use has since expanded to include various inflammatory dermatoses.7
Case Presentation
The patient is a 56-year-old female, with a height of 150 cm and a weight of 60 kg, who presented to the clinic on June, 2025, with a chief complaint of generalized urticaria persisting for two weeks. Her skin manifestations were observed as shown in Figure 1a–d. Upon admission, a comprehensive workup was conducted, including complete blood count, urinalysis, stool analysis, liver function tests, renal function tests, electrolyte levels, and screenings for hepatitis B, hepatitis C, syphilis, HIV, and tuberculosis (t-spot), all of which returned normal results. The patient’s medical history is notable for a 10-year history of psoriasis, for which she has been treated with Ixekizumab two months ago. The patient’s psoriasis lesions have completely disappeared and are well controlled. The clinical evaluation led to a consideration of UV as the potential diagnosis for her symptoms. Initially, the patient took loratadine tablets for treatment, but the effect was not satisfactory. The patient was administered intravenous methylprednisolone sodium succinate at a dose of 60 mg. However, during the infusion, the patient experienced a worsening of her rash, raising the suspicion of a possible allergic reaction to the methylprednisolone. Consequently, this medication was discontinued. The treatment regimen was then changed to intravenous administration of dexamethasone sodium phosphate at a dose of 10 mg, but the patient’s rash continued to exacerbate during this infusion. Given the unsatisfactory response to the corticosteroid treatments, a decision was made to initiate therapy with methotrexate, starting with an oral dose of 10 mg per week. The patient’s condition showed improvement following the introduction of methotrexate; however, during a follow-up visit on July, the patient reported inadequate control of her symptoms, noting the recurrence of urticaria despite adherence to the methotrexate regimen. In light of the persistent symptoms, patient was started on omalizumab at a dose of 300 mg administered subcutaneously every four weeks, in conjunction with methotrexate. Two weeks later during the follow-up, the patient’s symptoms remained persistent. In light of the persistent symptoms, methotrexate was discontinued, and the patient was started on omalizumab, in conjunction with cyclosporine at a dose of 50 mg twice daily. This combination therapy was intended to enhance the management of her condition. The Dosage of cyclosporine was reduced by one tablet every two weeks. The patient attended follow-up visits on August, and significant improvement in her condition was noted as shown in Figure 2a–d; no recurrence of urticaria was observed during the September visit. The patient’s symptoms were well-controlled, and she continues to be monitored in follow-up.
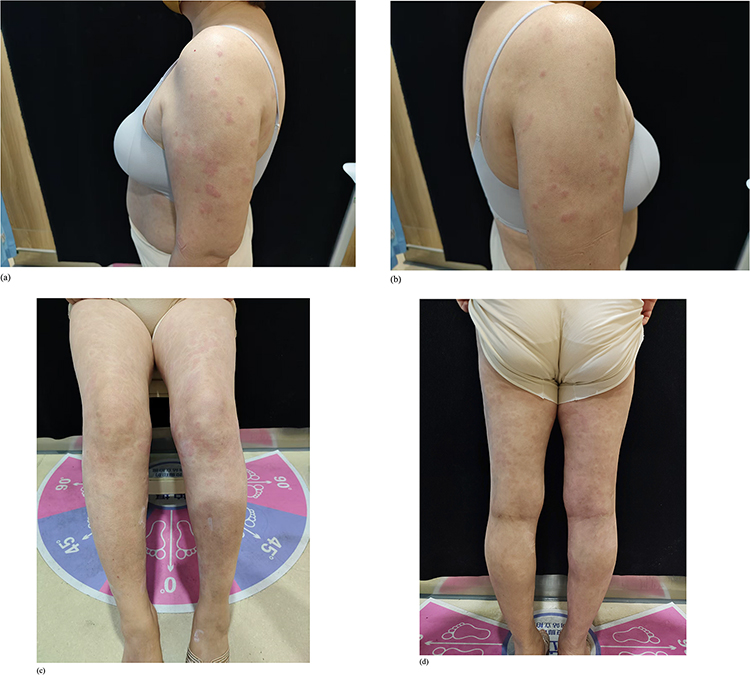 |
Figure 1 (a–d) Generalized erythematous wheals all over the body, June, 2025. |
 |
Figure 2 (a–d) A small amount of scattered erythematous wheals all over the body, August, 2025. |
Discussion
UV is a distinct syndrome that differs fundamentally from chronic spontaneous urticaria, making its management notoriously difficult due to a broad spectrum of clinical presentations and unpredictable therapeutic responses. UV is subdivided into normocomplementemic (NUV) and hypocomplementemic (HUV) types, with the hypocomplementemic form being linked to systemic diseases like systemic lupus erythematosus (SLE). It occurs at a rate of 0.5 per 100,000 person-years.8 UV not only presents with skin manifestations, but also causes systemic lesions.9 Certolizumab, a drug that blocks tumor necrosis factor-α (TNF-α), may cause UV.10 Although we do not have direct evidence to prove that Ixekizumab causes UV, we cannot completely rule out the possibility that it does. Autoimmune thyroiditis and systemic lupus erythematosus are relatively common comorbidities of UV and antihistamines provide limited efficacy, with systemic corticosteroids showing rapid control during acute phases but often failing as a long-term solution.11 Although Omalizumab has shown significant efficacy in treating some patients with UV,12 its response varies significantly among patients, necessitating individualized treatment strategies among the population with refractory UV Moreover, the combination of Omalizumab with immunosuppressants like cyclosporine has been explored, revealing variable effectiveness across different patient profiles, with some achieving substantial symptom relief.1 Meanwhile, cyclosporine has shown good clinical efficacy in the treatment of urticarial vasculitis and psoriasis. A Study have shown that for patients with refractory UV, the combination therapy of upadacitinib with omalizumab and dapsone can significantly improve clinical symptoms.1
The research on omalizumab and immunosuppressants mainly focuses on chronic urticaria.13 The research on the combined treatment of UV with omalizumab and immunosuppressants is limited. The first-line treatment for UV remains glucocorticoids. Patients who experienced exacerbation after steroid treatment might benefit from switching to other immunosuppressants such as methotrexate or mycophenolate mofetil, which have shown comparable efficacy in managing refractory cases.3,4 However, in this case, the patient’s condition worsened after using glucocorticoids, which indicates that we need to seek out individualized treatment plans. As such, the integration of Omalizumab in combination with other agents represents a potential avenue for enhancing treatment efficacy, particularly in refractory cases. The significance of monitoring long-term outcomes and adjusting treatment plans based on patient response is critical in managing this complex condition.
Conclusion
This case further demonstrates the crucial importance of personalized treatment plans. Especially when conventional therapies such as antihistamines and glucocorticoids are ineffective or exacerbate symptoms, the combination of omalizumab and cyclosporine represents a breakthrough in UV treatment.
Ethics Approval
Ethical approval was not required for the publication of this case report.
Consent for Publication
The authors confirm that informed consent was secured for publication and that this case report adheres to the relevant CARE guidelines.
Informed Consent for Publication
The patient provided informed consent for the publication of the anonymized case details and associated images.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Almaghrabi MM, Kalantan N, Alshareef A, et al. Case Report: upadacitinib in the management of refractory urticarial vasculitis. Front Med. 2025;12:1669513. doi:10.3389/fmed.2025.1669513
2. Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7(3):290–5. doi:10.1016/j.ijwd.2021.01.021
3. Rattananukrom T, Svetvilas P, Chanprapaph K. Successful treatment of normocomplementemic urticarial vasculitis with omalizumab: a report of three cases and literature review. Asian Pac J Allergy Immunol. 2020;38(4):286–289. doi:10.12932/AP-050918-0402
4. Loricera J, Calvo-Río V, Mata C, et al. Urticarial vasculitis in northern Spain: clinical study of 21 cases. Medicine. 2014;93(1):53–60. doi:10.1097/MD.0000000000000013
5. Abuzakouk M, Ghorab O, Namas R, et al. Long-term efficacy and safety of omalizumab monotherapy in a patient with normocomplementemic urticarial vasculitis. J Drugs Dermatol. 2022;21(10):1124–1126. doi:10.36849/JDD.6739
6. Bonnekoh H, Jelden-Thurm J, Allenova A, et al. Urticarial vasculitis differs from chronic spontaneous urticaria in time to diagnosis, clinical presentation, and need for anti-inflammatory treatment: an International prospective UCARE Study. J Allergy Clin Immunol Pract. 2023;11(9):2900–2910.e21. doi:10.1016/j.jaip.2023.06.030
7. Kutlubay Z, Erdogan BÇ, Engin B, et al. Cyclosporine in dermatology. Skinmed. 2016;14(2):105–109.
8. Mut Quej JE, Ramirez Molina PI, Saad Manzanera MI, et al. Vasculitis urticarial hipocomplementémica en LES: entre urticaria y autoinmunidad [Hypocomplementemic urticarial vasculitis in SLE: between urticaria and autoimmunity]. Rev Alerg Mex. 2025;72(3):88. doi:10.29262/ram.v72i3.1526
9. Dorian L, Peché R, Guiot J, et al. Respiratory involvement during the course of hypocomplementemic urticarial vasculitis: a case report. Cureus. 2025;17(8):e89813. doi:10.7759/cureus.89813
10. Ouni B, Chahed F, Slim R, et al. Certolizumab-induced urticarial vasculitis: a case report. Curr Drug Saf. 2025. doi:10.2174/0115748863356947250302165303
11. Artosi F, Cosio T, Diluvio L, et al. Challenging clinical therapeutic approach to urticarial vasculitis: a case series. J Clin Med. 2025;14(13):4580. doi:10.3390/jcm14134580
12. Edek YC, Ertürk E, Adışen E. Omalizumab in the treatment of refractory urticarial vasculitis triggered by SARS-Cov-2 infection: a pediatric case report. Dermatol Pract Concept. 2024;14(4):e2024252. doi:10.5826/dpc.1404a252
13. Sánchez J, Alvarez L, Cardona R. Cyclosporine and omalizumab together: a new option for chronic refractory urticaria. J Allergy Clin Immunol Pract. 2020;8(6):2101–2103. doi:10.1016/j.jaip.2020.02.012
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.