Back to Journals » Clinical Ophthalmology » Volume 19
Treatment Adherence in Myopia Progression Management: A Monocentric Retrospective Study on Rates and Determinants
Authors Lembo A, Curci A, Villani E, Schiavetti I, Nucci P
Received 24 June 2025
Accepted for publication 29 October 2025
Published 7 November 2025 Volume 2025:19 Pages 4107—4115
DOI https://doi.org/10.2147/OPTH.S549320
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Andrea Lembo,1 Alessandra Curci,1 Edoardo Villani,1,2 Irene Schiavetti,3,4 Paolo Nucci1,5
1Eye Clinic, San Giuseppe Hospital - IRCCS MultiMedica, Milan, Italy; 2Department of Clinical Sciences and Community Health, Department of Excellence 2023– 2027, University of Milan, Milan, Italy; 3Section of Biostatistics, Department of Health Sciences, University of Genoa, Genoa, Italy; 4IRCCS Ospedale Policlinico San Martino, Genoa, Italy; 5Department of Biomedical, Surgical and Dental Sciences, University of Milan, Milan, Italy
Correspondence: Andrea Lembo, Eye Clinic, San Giuseppe Hospital - IRCCS MultiMedica, Via San Vittore 12, Milano, 20123, Italy, Email [email protected]
Purpose: To identify factors influencing good adherence when using different myopia management solutions, including low-dose atropine, defocus spectacle lenses (DIMS), defocus contact lenses, photobiomodulation with low-intensity red light, and combined approaches.
Design: Retrospective, observational, single-center chart review.
Patients and Methods: This single center retrospective study analyzed clinical and demographic data of myopic patients younger than 17 years. Exclusion criteria were presence of systemic and ocular pathologies, significant refractive (other than myopia) or binocular vision disorders, and follow-up less than 6 months. Data on age, sex, cycloplegic refraction, myopic progression, type of myopia control treatment, and patient-reported adherence to treatment (categorized as good, fair, poor) was obtained from the medical charts.
Results: We analyzed 177 Caucasian pediatric patients (49.2% female; mean age 11.1 ± 2.78 years); 84.2% reported good adherence to treatment, 6.8% reported moderate adherence, and 9.0% reported poor adherence. In multivariate logistic regression analysis, DIMS spectacle lenses showed the strongest association with adherence (OR = 21.17, p = 0.003), followed by the combined use of DIMS spectacle lenses and atropine (OR = 4.02, p = 0.038). Higher myopia progression in spherical equivalent (SE) (OR = 0.31, p = 0.002), and older age (OR 0.78, p = 0.05) were significantly associated with lower adherence.
Conclusion: These findings suggest that younger age and lower myopia progression are associated with better adherence to treatment. Among treatment options, DIMS spectacle lenses alone or combined with atropine, were the strongest predictors of adherence, while other approaches showed no significant associations. This favors optical-based strategies when adherence is a concern and calls for enhanced counseling strategies in adolescents.
Plain Language Summary: Several treatments aim to control myopia progression in children, but they only work if adherence is correctly followed over time. We wanted to learn which options are easier to stick with and which factors influence day-to-day use.This study reviewed records from one Milan hospital for myopic children who used at least one option for myopia control for ≥ 6 months: low-dose atropine, defocus spectacle lenses, myopia-control soft contact lenses, low-level red-light therapy, or combinations. During last visit, children and families reported how consistently they used the treatment.Overall, 84% reported good adherence (≥ 75%). The highest adherence was seen with defocus spectacles (95.7%) and defocus soft contact lenses (95.0%), followed by defocus glasses + atropine (90.5%) and defocus glasses + contact lenses (81.0%); in contrast, atropine alone (66.7%) and red-light therapy (40.0%) showed lower adherence.
Older adolescents struggled more, whereas lower myopia progression was linked to better adherence.In everyday practice, optical options – especially defocus glasses, alone or with atropine – may be the most practical choices when sticking with treatment is a concern. Simple routines and tailored counselling are particularly important for adolescents to support long-term, everyday use. Our findings come from one center and rely on self-reports, so results may not apply to all settings.
Keywords: myopia control, adherence, compliance, atropine, defocus lenses
Introduction
Myopia is the most common refractive error, with prevalence ranging from ~25% in children and adolescents in Western Countries1 to over 90% in Taiwan university students.2 Its incidence, progressively increasing worldwide, is reaching epidemic proportions.3 A systematic review and meta-analysis with projection modeling estimated that by 2050, half of the world’s population (4.8 billion people) will be myopic, and of these, approximately 1 billion people will have high myopia.4 Myopia and high myopia are associated, with increased ocular morbidity,5 higher rate of visual impairment,4 relevant individual and societal economic burden,6,7 and decreased quality of life.8
Pharmacological, optical, and environmental strategies for management of myopic progression are increasingly supported by a growing body of literature.9,10 These include low-dose atropine,11,12 defocus spectacle lenses (eg Defocus Incorporated Multiple Segments),13,14 orthokeratology,15,16 defocus contact lenses,17,18 photo biomodulation with low-intensity red light.19,20 To understand the clinical benefit of these myopia management solutions, myopia control treatments need to be adopted for several years until myopia is stable Consequently, long-term adherence emerges as the key determinant of effectiveness in routine practice. However, treatment nonadherence is a significant public health concern in patients with chronic conditions, especially in pediatric populations, with nonadherence rates reported to be around 50% of children21 and 65–90% of adolescents.22
At present, little is known about treatment adherence in myopia control, with limited and heterogeneous data on spectacles, contact lens, and pharmacological interventions. Adherence is frequently cited but seldom predefined as an outcome, and is typically assessed indirectly (eg, discontinuation, hours worn). A recent Cochrane living systematic review and meta-analysis23 found quantitative data on adherence to myopia control treatment in 25 randomized clinical trials and reported percentages of always or mostly- compliant ranging from 72% to 97% for spectacles, from 31% to 100% for contact lens, and from 79% to 99% for pharmacological interventions.
Existing adherence studies are largely trial-based, heterogeneous, and short-term, with limited real-world pediatric evidence and scarce objective measurement. We designed a retrospective study in a pediatric myopic population with a primary aim of comparing adherence of different myopia control strategies and investigating factors affecting patients’ adherence in a real-life setting, providing complementary estimates and practice-level barriers not captured in trials, where adherence is often inflated by protocolized follow-up, eligibility restrictions, and close monitoring.
Materials and Methods
Study Design
A retrospective chart review was conducted to analyze adherence to myopia control treatments among pediatric patients. This study was conducted in accordance with the ethical standards in the 1964 Declaration of Helsinki and its subsequent amendments. At the time of their visits, patients (or their legal guardians) provided consent for the use of their anonymized clinical data for research purposes. Given the retrospective nature of the study and the use of anonymized data, additional informed consent was not required. The study protocol was approved by the Human Subjects Ethics Committee of the University of Milan. Electronic records from University Eye Clinic, San Giuseppe Hospital of Milan were reviewed, after approval, for Caucasian children aged between 4 and 17 years, with myopia in at least one eye (defined as cycloplegic spherical equivalent (SE) ≤-0.5 diopters (D),24 who had completed at least 6 months of follow-up, with their most recent visit occurring between 01/01/2024 and 01/06/2024. No maximum treatment duration was prespecified.
Exclusion criteria included presence of ocular diseases, astigmatism >3.00 D, anisometropia >3.00D, amblyopia, strabismus and binocular vision abnormalities, systemic or genetic diseases, cognitive disabilities (meaning difficulty in understanding or cooperating) and allergy to cycloplegic drugs.
Prior to commencing myopia control, all patients attending the University Eye Clinic undergo a full baseline ophthalmological assessment including symptoms and history, visual acuity with their current spectacles (if any are worn), orthoptic testing, refraction (including cycloplegic autorefraction) and dilated fundoscopy.
Population
Parents and/or carers of suitable patients were provided with verbal information on myopia control options including low dose atropine, myopia control spectacles, defocus contact lenses, red light treatment and combination treatment (myopia control spectacles and atropine or myopia control spectacles and contact lenses). Counseling covered indications and expected benefits, risks/side effects, wear or dosing targets, handling/safety, and the follow-up schedule. Education was delivered as usual care and was not protocolized or recorded verbatim for this study. Options are discussed with patients, parents/carers and clinicians based on the patient’s age, history of myopia progression and previous history of myopia management. Patients and their parents/carers made an informed choice for their preferred myopia control method or opt for their children to continue wearing single vision lenses. Their choice of myopia control treatment determined which group they were assigned to. At initiation, families received pragmatic, modality-specific schedules covering dosing/wear targets and follow-up. Recommendations were: 1 drop in each eye nightly (7/7 nights) for low dose atropine; full-time wear during waking hours for myopia-control defocus spectacles and/or soft contact lenses; two 3-minute sessions/day on 5 days/week for red-light therapy. For children prescribed both defocus spectacles and soft contact lenses, daily adherence was defined using a single combined item: the day counted as adherent if either modality was worn for the recommended waking hours (no summation/double counting). Routine recommended follow-up was annual for all modalities. Red-light therapy followed a different schedule with visits at 1 week, 1 month, 3 months, and 6 months, then every 6 months thereafter, as suggested by the manufacturer. For comparability with other modalities, adherence for red-light therapy was analyzed at the 6-month visit; interim reviews were arranged as clinically indicated (eg, accelerated progression, side-effects, fitting/handling issues).
Data Collection
Data collected included baseline age, sex, family history of myopia, baseline cycloplegic SE, type of optical correction and/or myopia control treatment, time from treatment initiation, previous treatment with low-dose atropine, follow-up duration, final cycloplegic SE, and adherence classification. In daily clinical practice, the issue of “proper adherence to prescribed therapy” is not always specified, and this has become an increasingly frequent subject of study in recent years. As per our usual care, cycloplegia was achieved by instilling two drops of Cyclopentolate 10 mg/mL 5 minutes apart. After a 30-minute wait from the second instillation and the verification of pupillary dilation, the measurement of objective refraction was performed using a portable autorefractometer (0.25D steps, average of 3 readings).
As part of routine care, treatment adherence was assessed at follow-up visits during history taking via a structured interview supported by a dedicated questionnaire (Figure 1), with the patient and parents participating together. The questionnaire was previously developed in alignment with our clinic’s workflow constraints and it explores simultaneously implementation and persistence, using a 30-day recall with harmonized response formats to reduce burden and improve comparability.
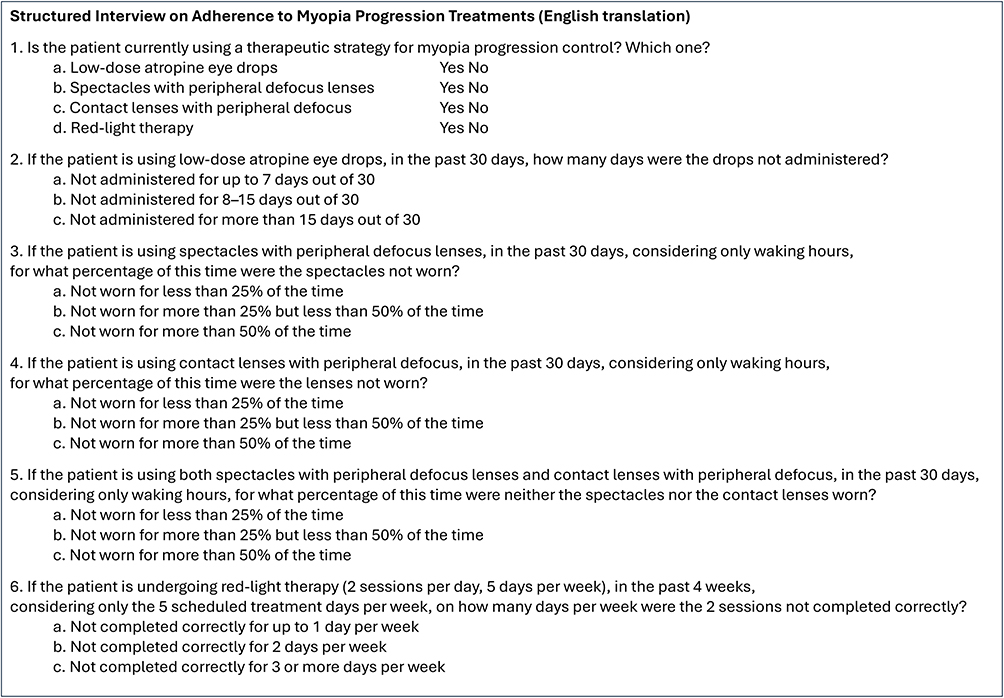 |
Figure 1 English translation of the structured interview used, in our daily clinical practice, to assess reported adherence to myopia control treatments, jointly interviewing patients and parents. |
Because no universally accepted thresholds exist for categorizing adherence, we pre-specified pragmatic bands for interpretability in routine care as poor (less than 50% of days for medications and treatment sessions, or less than 50% of total waking hours for optical corrections), moderate (50% to 75% for all parameters), or good (greater than 75%) – consistent with literature that similarly stratifies adherence into ordinal categories.25 For inferential analyses we modeled “good” (≥75%) vs other, which also addresses a binary compliant/non-compliant framing.
Statistical Analysis
Statistical analysis was performed using R version 4.1.3 (2022-03-10). Since this was a retrospective study, the sample size was determined by the number of eligible patients available in the database over the study period. No formal power calculation was performed. Participants missing any core variable were excluded. Imputation was not performed; tables display the final sample sizes.
Adherence was assessed at the patient level (rather than per eye), consistent with binocular optical wear and patient-level administration of other myopia-control therapies.
Data distribution was assessed by Shapiro–Wilk and continuous variables were expressed as mean ± standard deviation. Categorical variables were expressed as frequency with percentages.
Spearman correlation coefficient, along with Bland-Altman analysis, was used to analyze the correlation grade of baseline cycloplegic SE between right and left eye to confirm interchangeability, as myopia progression was considered a contextual factor potentially associated with adherence and analyzed as a determinant/covariate.
Both univariate and multivariate logistic regression analyses were conducted to explore the associations between age, sex, family history of myopia, type of optical correction and/or myopia control treatment, previous treatment with low-dose atropine, treatment duration, baseline cycloplegic SE, myopic progression (D/year, annualized), and good adherence to treatment. Univariate screening used a liberal threshold (p < 0.10) to retain candidate predictors; those meeting this criterion entered the multivariable model, where statistical significance was set at p < 0.05.
Results
This retrospective analysis included 177 pediatric patients, 49.2% females, with a mean age of 11.1±2.78 years (Table 1).
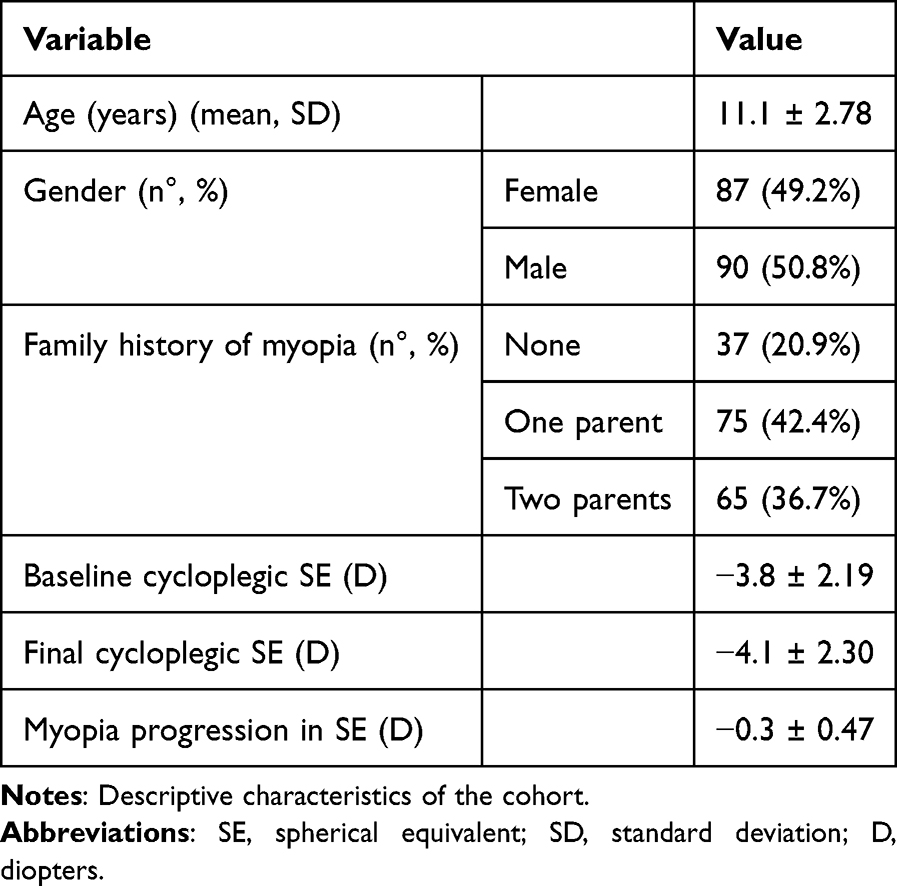 |
Table 1 Demographic and Cycloplegic Data |
The correlation analysis between the right and left eye measurements demonstrated a strong relationship (rho: 0.83; p<0.001), suggesting that one eye could potentially serve as a proxy for the other. These data are confirmed by the Bland-Altman analysis, which showed a mean difference of 0.08D and limits of agreement ranging from −1.86D to 2.02D, indicating that the differences between the two eyes are generally small and within an acceptable range of variability. Cycloplegic outcomes were summarized using the right eye as the patient-level value.
Different myopia control strategies were adopted with a mean treatment duration of 1.1±0.41 years, with an interquartile range of 0.9–1.1 years. Atropine eye drops were used by 42 patients, with 28 of them (66.7%) demonstrating good adherence. Defocus spectacle lenses were the most frequently used strategy, adopted by 47 patients, of whom 45 (95.7%) had good adherence to treatment. A combined approach of defocus spectacle lenses and atropine was followed by 42 patients, with good adherence observed in 38 (90.5%) of them. Defocus contact lenses were used by 20 patients, with 19 (95.0%) adhering well to the treatment. Additionally, a combination of defocus spectacle lenses and defocus contact lenses was chosen by 21 patients, with good adherence recorded in 17 (81.0%). Finally, red light therapy was the least commonly used approach, adopted by 5 patients, of whom only 2 (40.0%) showed good adherence (Table 2).
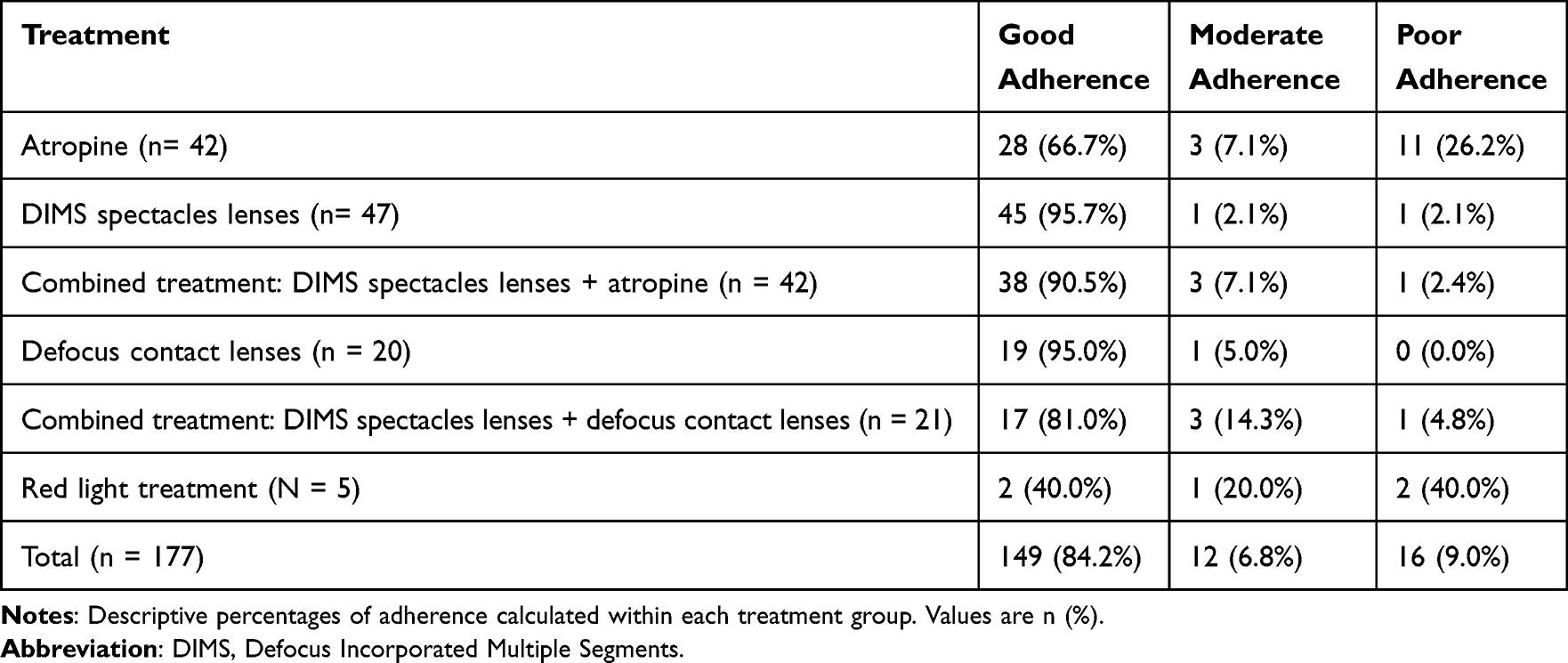 |
Table 2 Adherence Among Different Treatments |
Age was found to be marginally associated with adherence to treatment, suggesting that younger individuals may have better adherence (OR = 0.78, 95% CI: 0.61–1.00, p = 0.05); no significant associations were observed for sex, family history of myopia, previous treatment, or baseline cycloplegic SE.
Among treatment modalities, DIMS spectacle lenses were strongly associated with increased adherence compared to atropine (OR = 21.17, 95% CI: 2.84–157.66, p = 0.003), as was the combined treatment with DIMS spectacle lenses and atropine (OR = 4.02, 95% CI: 1.08–15.02, p = 0.038). Defocus contact lenses also showed a positive association, though with borderline significance (OR = 9.59, 95% CI: 1.00–92.02, p = 0.05). Other treatment modalities, including the combination of DIMS spectacle lenses with defocus contact lenses and red-light treatment, were not significantly associated with good adherence, with wide CIs reflecting small sample sizes. Treatment duration showed a negative correlation with “good” adherence to treatment in univariate analysis (OR 0.66; 95% CI 0.51–0.86; p<0.01), but this lost significance in multivariate model (OR 0.74; 95% CI 0.51–1.06; p=0.10). Finally, higher myopia progression in SE was significantly linked to lower adherence (OR = 0.31, 95% CI: 0.05–0.51, p = 0.002). (Table 3)
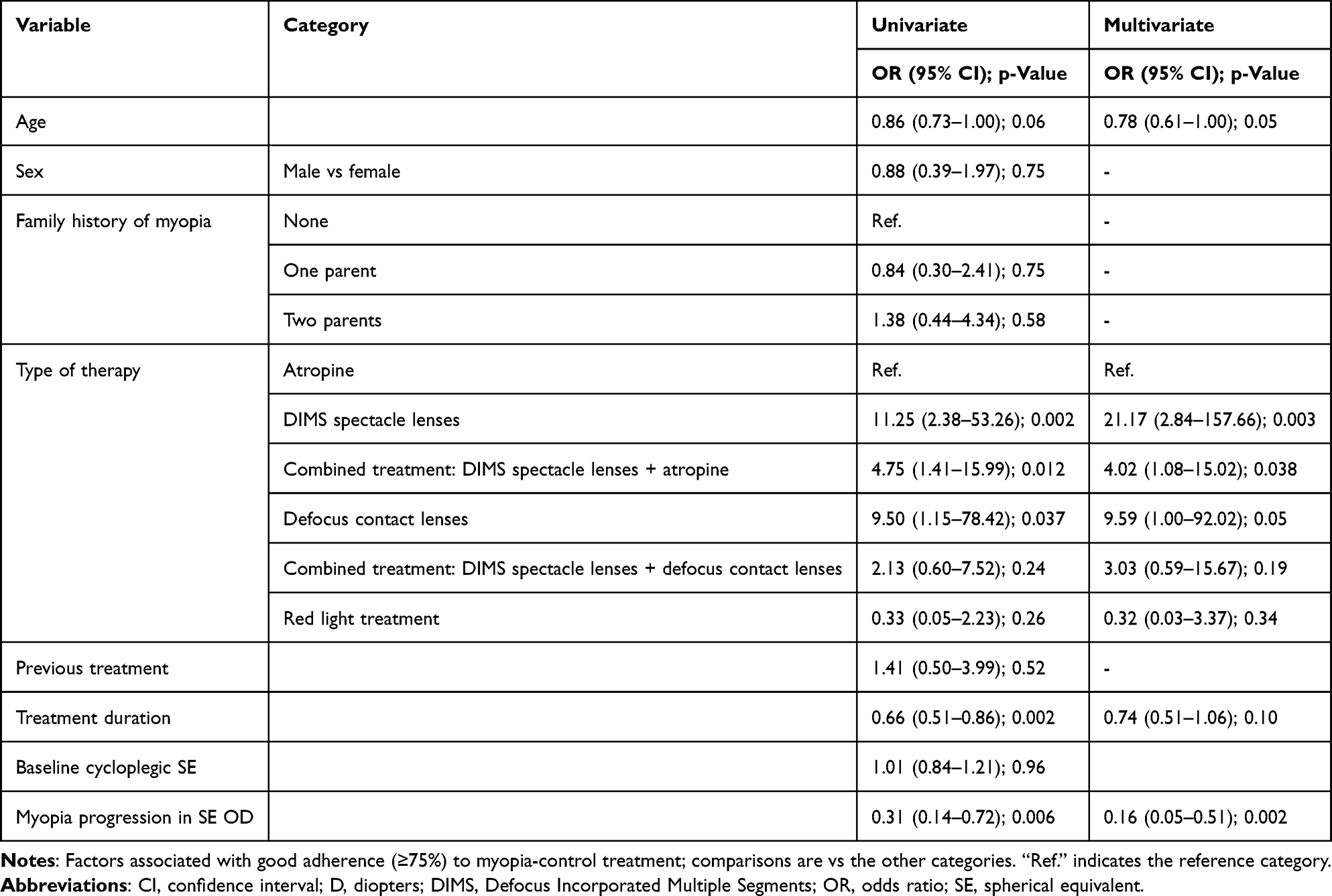 |
Table 3 Logistic Regression Analysis of Factor Associated with “Good” Adherence to Treatment |
Discussion
This retrospective study explored factors influencing adherence to various myopia control solutions in a pediatric population. Our findings reveal that while overall adherence rates were high (87.4%), several variables significantly impacted adherence, including patient age, type of therapy, and degree of myopia progression. These real-world adherence patterns broadly align with, but also refine, RCT-based estimates. In the Cochrane living review, “always/mostly adherent” ranged 72–97% for spectacles, 31–100% for contact lenses, and 79–99% for pharmacologic treatments.23
In our cohort, DIMS spectacles (95.7%) and defocus contact lenses (95.0%) fall near the upper RCT spectrum, whereas atropine (66.7%) is lower than many trial reports. Combined regimens (DIMS+atropine 90.5%; DIMS+CL 81.0%) remain high but more variable, while red-light (40.0%) is comparatively low. Differences likely reflect routine-care conditions – less intensive monitoring and broader eligibility – versus the closer follow-up typical of trials. Notably, DIMS spectacles – alone (OR 21.17; 95.7%) or combined with atropine (OR 4.02; 90.5%) – and defocus contact lenses (OR 9.59; 95.0%) showed the strongest associations with higher adherence, underscoring their pragmatic advantages in real-world use.
One of the key findings was the negative association between age and adherence, with older children showing lower adherence rates. This aligns with previous studies suggesting that increased autonomy and reduced parental oversight in older pediatric patients lead to poorer adherence to chronic treatments.22,26 These results highlight the need for age-specific strategies, such as targeted education and motivational interventions for adolescents.
Adherence to chronic treatments remains a complex challenge across various medical disciplines, often impacting the effectiveness of therapeutic interventions.27 Once a patient accepts the treatment recommendation, adherence involves several key steps: obtaining the prescribed therapy, correctly applying or following the treatment protocol, adhering to the recommended schedule, and maintaining persistent use over time.28
In ophthalmology, adherence difficulties are well-documented, particularly in conditions requiring long-term management such as glaucoma28,29 and dry eye disease,30 where patients frequently struggle with complex treatment regimens, the peculiar nature of early disease stages, and poor perception of the treatment effect.
Pediatric populations present unique challenges regarding adherence, influenced by developmental, cognitive, and psychosocial factors.21,22 In children, treatment adherence often depends heavily on parental involvement and supervision,31 but as children grow older and seek greater autonomy, maintaining consistent treatment routines can become increasingly difficult, also because of the challenges in shared decision-making.26 Additionally, the child’s understanding of the condition, motivation, and the perceived impact of the treatment on their daily life play crucial roles in treatment adherence.31
In this specific context, it is important to note that while myopia is primarily considered a simple refractive error it is increasingly recognized as a chronic disease with sight-threatening sequelae, and recent consensus reports recommend classifying it as a disease,32 underscoring the need for sustained control therapy. Treatments mainly focus on slowing myopia progression to reduce the risk of potential future complications.33
The type of myopia control treatment also influenced adherence. Patients using DIMS spectacle lenses and contact lenses had higher odds of good adherence compared to those on low-dose atropine, likely due to the ease of integrating optical corrections into daily routines, serving both refractive and myopia control purposes. Combination therapies, especially DIMS spectacle lenses with low-dose atropine, further improved adherence, suggesting that multimodal approaches may enhance patient engagement.
Our findings have relevant clinical implications. Improving treatment adherence requires simplifying treatment regimens, integrating therapies, and providing targeted education both to patients and caregivers. During a pediatric clinical evaluation, it is useful to discuss with the caregivers the reason for choosing a certain therapy, and especially to discuss with the relatives regarding the cost/benefit ratio of a medical or optical treatment. This is particularly important for older children who perceived myopia management solutions as burdensome.
This study has several limitations, including its retrospective design, reliance on self-reported adherence (subject to recall and social desirability biases; recall bias may have been partially mitigated through cross-informant corroboration during joint parent–child interviews), cross-sectional assessment of adherence (precluding causal inference), single-center setting, an exclusively Caucasian sample, and imbalance across treatment groups – particularly the red-light subgroup (n=5) – limiting generalizability of the results. Treatment allocation was preference-based and non-randomized, which may introduce selection bias and confounding by indication. The study’s limited follow-up may lead to underestimation of long-term determinants of adherence, including treatment effects on the physical, psychological, and environmental dimensions of patients’ and parents’ quality of life.34 In addition, differences in treatment duration were not controlled for and may have introduced residual confounding. Nevertheless, our structured 30-day recall interview captured early signals related to both implementation and persistence.35
Additionally, because of the study design, factors like socio-economic status, affordability and availability, health literacy, and quality of life impacts, all of which could influence adherence, were not assessed.
Despite these limitations, this is the first study to offer valuable insights into real-world adherence patterns in pediatric myopia control, helping to address the current evidence gap. Future prospective studies with diverse populations and objective adherence measures are needed to confirm these findings and develop optimized intervention strategies.
Conclusion
Adherence to myopia control treatments is multifactorial, influenced by patient age, treatment type, and disease progression. Tailored strategies focusing on simplifying regimens, enhancing education, and implementing age-appropriate interventions are essential to improve long-term adherence and optimize myopia control outcomes. Actionable steps include teach-back counseling, a short routine-based plan, shared reminders, simplification of dosing/wear targets, early cost/access checks, and structured follow-up with recall – measures aligned with age-specific needs to sustain long-term adherence.
Data Sharing Statement
Unpublished data are available upon reasonable request.
Ethics Approval
The study adhered to the tenets of the Declaration of Helsinki.
The study was approved by the Human Subjects Ethics Committee of the University of Milan (opinion n° 52/24, 16 April 2024).
Patient Consent to Participate
Not applicable due to retrospective design.
Consent for Publication
All authors gave final approval of the version to be published.
Author Contributions
Andrea Lembo: Conceptualization, Methodology, Investigation, Writing - Original Draft; Alessandra Curci: Conceptualization, Methodology, Investigation, Writing - Original Draft; Edoardo Villani: Analysis and interpretation, Writing - Review & Editing, Supervision; Irene Schiavetti: Formal analysis, Writing - Original Draft, Visualization; Paolo Nucci: Conceptualization, Writing - Review & Editing, Supervision. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
Dr Andrea Lembo reports personal fees from Essilor Luxottica and Hoya. Prof. Edoardo Villani reports grants/personal fees and/or non-financial supports from Abbvie, Alcon, FB Vision, SIFI, Thea, TRB, Unifarco, SUN Pharma, Santen, Essilor Luxottica, and Alfa Intes, outside the submitted work. Dr Irene Schiavetti reports personal compensation for speaking and consulting from Roche, Biogen, Hoya, Hippocrates Research, D.M.G Italia, Eyepharma, and DreamsLab. Professor Paolo Nucci reports personal fees from Essilor Luxottica, Hoya, Zeiss, Santen, during the conduct of the study. The authors declare that they have no other competing interests in this work.
References
1. Liang J, Pu Y, Chen J, et al. Global prevalence, trend and projection of myopia in children and adolescents from 1990 to 2050: a comprehensive systematic review and meta-analysis. Br J Ophthalmol. 2025;109(3):362–367. doi:10.1136/bjo-2024-325427
2. Sankaridurg P, Tahhan N, Kandel H, et al. IMI Impact of Myopia. Invest Ophthalmol Vis Sci. 2021;62(5):2. doi:10.1167/iovs.62.5.2
3. Dolgin E. The myopia boom. Nature. 2015;519(7543):276–278. doi:10.1038/519276a
4. Holden BA, Fricke TR, Wilson DA, et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
5. Haarman AEG, Enthoven CA, Tideman JWL, et al. The Complications of Myopia: a Review and Meta-Analysis. Invest Ophthalmol Vis Sci. 2020;61(4):49. doi:10.1167/iovs.61.4.49
6. Ma Y, Wen Y, Zhong H, et al. Healthcare utilization and economic burden of myopia in urban China: a nationwide cost-of-illness study. J Glob Health. 2022;12:11003. doi:10.7189/jogh.12.11003
7. Naidoo KS, Fricke TR, Frick KD, et al. Potential Lost Productivity Resulting from the Global Burden of Myopia: systematic Review, Meta-analysis, and Modeling. Ophthalmology. 2019;126(3):338–346. doi:10.1016/j.ophtha.2018.10.029
8. Rose K, Harper R, Tromans C, et al. Quality of life in myopia. Br J Ophthalmol. 2000;84(9):1031–1034. doi:10.1136/bjo.84.9.1031
9. Wolffsohn JS, Flitcroft DI, Gifford KL, et al. IMI - Myopia Control Reports Overview and Introduction. Invest Ophthalmol Vis Sci. 2019;60(3):M1–M19. doi:10.1167/iovs.18-25980
10. Bullimore MA, Saunders KJ, Baraas RC, et al. IMI-Interventions for Controlling Myopia Onset and Progression 2025. Invest Ophthalmol Vis Sci. 2025;66(12):39. doi:10.1167/iovs.66.12.39
11. Chia A, Chua WH, Cheung YB, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012;119(2):347–354. doi:10.1016/j.ophtha.2011.07.031
12. Sacchi M, Serafino M, Villani E, et al. Efficacy of atropine 0.01% for the treatment of childhood myopia in European patients. Acta Ophthalmol. 2019;97(8):e1136–e1140. doi:10.1111/aos.14166
13. Carlà MM, Boselli F, Giannuzzi F, et al. Overview on Defocus Incorporated Multiple Segments Lenses: a Novel Perspective in Myopia Progression Management. Vision. 2022;6(2):20. doi:10.3390/vision6020020
14. Erdinest N, London N, Lavy I, et al. Peripheral Defocus and Myopia Management: a Mini-Review. Korean J Ophthalmol. 2023;37(1):70–81. doi:10.3341/kjo.2022.0125
15. Lipson MJ, Brooks MM, Koffler BH. The Role of Orthokeratology in Myopia Control: a Review. Eye Contact Lens. 2018;44(4):224–230. doi:10.1097/ICL.0000000000000520
16. Cho P, Cheung SW. Retardation of myopia in Orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest Ophthalmol Vis Sci. 2012;53(11):7077–7085. doi:10.1167/iovs.12-10565
17. Chamberlain P, Peixoto-de-matos SC, Logan NS, et al. A 3-year Randomized Clinical Trial of MiSight Lenses for Myopia Control. Optom Vis Sci. 2019;96(8):556–567. doi:10.1097/OPX.0000000000001410
18. Lumb E, Sulley A, Logan NS, et al. Six years of wearer experience in children participating in a myopia control study of MiSight® 1 day. Cont Lens Anterior Eye. 2023;46(4):101849. doi:10.1016/j.clae.2023.101849
19. Jiang Y, Zhu Z, Tan X, et al. Effect of Repeated Low-Level Red-Light therapy for myopia control in children. Ophthalmology. 2022;129(5):509–519. doi:10.1016/j.ophtha.2021.11.023
20. Dong J, Zhu Z, Xu H, et al. Myopia Control Effect of Repeated Low-Level Red-Light Therapy in Chinese Children: a Randomized, Double-Blind, Controlled Clinical Trial. Ophthalmology. 2023;130(2):198–204. doi:10.1016/j.ophtha.2022.08.024
21. McGrady ME, Hommel KA. Medication adherence and health care utilization in pediatric chronic illness: a systematic review. Pediatrics. 2013;132(4):730–740. doi:10.1542/peds.2013-1451
22. Logan D, Zelikovsky N, Labay L, et al. The Illness Management Survey: identifying Adolescent’s Perceptions of Barriers to Adherence. J Pediatric Psychol. 2003;28(6):383–392. doi:10.1093/jpepsy/jsg028
23. Lawrenson JG, Huntjens B, Virgili G, et al. Interventions for myopia control in children: a living systematic review and network meta-analysis. Cochrane Database Syst Rev. 2025;2(2):CD014758. doi:10.1002/14651858.CD014758.pub3
24. Flitcroft DI, He M, Jonas JB, et al. IMI - Defining and Classifying Myopia: a Proposed Set of Standards for Clinical and Epidemiologic Studies. Invest Ophthalmol Vis Sci. 2019;60(3):M20–M30. doi:10.1167/iovs.18-25957
25. Zhang X, Wu Y, Shi H, et al. Impact of Co-Management Mode on Diagnosis and Treatment Compliance in Community-Level Diabetic Patients with Retinopathy. Br J Hosp Med. 2024;85(10):1–13.
26. Sobode OR, Jegan R, Toelen J, et al. Shared decision-making in adolescent healthcare: a literature review of ethical considerations. Eur J Pediatr. 2024;183(10):4195–4203. doi:10.1007/s00431-024-05687-0
27. Haynes RB, McKibbon KA, Kanani R. Systematic review of randomised trials of interventions to assist patients to follow prescriptions for medications. Lancet. 1996;348(9024):383–386. doi:10.1016/S0140-6736(96)01073-2
28. Muir KW, Lee PP. Glaucoma medication adherence: room for improvement in both performance and measurement. Arch Ophthalmol. 2011;129(2):243–245. doi:10.1001/archophthalmol.2010.351
29. Oltramari L, Mansberger SL, Souza JMP, et al. The association between glaucoma treatment adherence with disease progression and loss to follow-up. Sci Rep. 2024;14(1):2195. doi:10.1038/s41598-024-52800-2
30. Uchino M, Yokoi N, Shimazaki J, et al. On Behalf Of The Japan Dry Eye Society. Adherence to Eye Drops Usage in Dry Eye Patients and Reasons for Non-Compliance: a Web-Based Survey. J Clin Med. 2022;11(2):367. doi:10.3390/jcm11020367
31. Santer M, Ring N, Yardley L, et al. Treatment non-adherence in pediatric long-term medical conditions: systematic review and synthesis of qualitative studies of caregivers’ views. BMC Pediatr. 2014;14(1):63. doi:10.1186/1471-2431-14-63
32. National Academies of Sciences. Engineering, and Medicine; Division of Behavioral and Social Sciences and Education; Board on Behavioral, Cognitive, and Sensory Sciences; Committee on Focus on Myopia: pathogenesis and Rising Incidence. In: Myopia: Causes, Prevention, and Treatment of an Increasingly Common Disease. Washington (DC): National Academies Press (US); 2024.
33. Khanal S. Is myopia a disease or just a dis-ease? Ophthalmic Physiol Opt. 2023;43(4):595–597. doi:10.1111/opo.13145
34. Fatimah M, Agarkar S, Narayanan A. Impact of defocus incorporated multiple segments (DIMS) spectacle lenses for myopia control on quality of life of the children: a qualitative study. BMJ Open Ophthalmology. 2024;9(1):e001562. doi:10.1136/bmjophth-2023-001562
35. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br. J Clin Pharmacol. 2012;73(5):691–705.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Low-Dose Atropine (0.01% to 0.05%) in Reducing Myopia Progression: A Systematic Review and Meta-Analysis
Alqahtani AS, Almarwani SH, Alweal BS, Albadri M, Alghamdi LN, Bin Saddiq BW, Morad AS
Clinical Ophthalmology 2026, 20:564944
Published Date: 7 May 2026