Back to Journals » Journal of Asthma and Allergy » Volume 13
Treatment Adherence in Adolescents with Asthma
Received 2 October 2019
Accepted for publication 9 December 2019
Published 14 January 2020 Volume 2020:13 Pages 39—49
DOI https://doi.org/10.2147/JAA.S233268
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Alan Kaplan, 1– 3 David Price 3, 4
1University of Toronto Department of Family and Community Medicine, Toronto, ON, Canada; 2Family Physician Airways Group of Canada, Edmonton, AB, Canada; 3Observational and Pragmatic Research Institute, Singapore, Singapore; 4Centre of Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Aberdeen, UK
Correspondence: Alan Kaplan
University of Toronto Department of Family and Community Medicine, 7335 Yonge Street, Thornhill, Toronto ON, Canada
Tel +1 905 883 1100
Fax +1 905-884-1195
Email [email protected]
Abstract: The burden of asthma is particularly notable in adolescents, and is associated with higher rates of prevalence and mortality compared with younger children. One factor contributing to inadequate asthma control in adolescents is poor treatment adherence, with many pediatric studies reporting mean adherence rates of 50% or lower. Identifying the reasons for poor disease control and adherence is essential in order to help improve patient quality of life. In this review, we explore the driving factors behind non-adherence in adolescents with asthma, consider their consequences and suggest possible solutions to ensure better disease control. We examine the impact of appropriate inhaler choice and good inhaler technique on adherence, as well as discuss the importance of selecting the right medication, including the possible role of as-needed inhaled corticosteroids/long-acting β 2-agonists vs short-acting β 2-agonists, for improving outcomes in patients with mild asthma and poor adherence. Effective patient/healthcare practitioner communication also has a significant role to engage and motivate adolescents to take their medication regularly.
Keywords: asthma, adherence, adolescents, treatment
Plain Language Summary
Asthma is particularly serious for adolescents. Asthma is more common in this age group, and more adolescents than younger children die due to asthma. One reason for this is that around half of adolescents with asthma do not take their medication properly. It is important to understand why this happens in order to improve their outlook and quality of life. Here, we look at the range of reasons for why adolescents do not take their asthma medications properly and the results of this. These include adolescents becoming more independent and wanting to be responsible for taking their medication, but sometimes forgetting to take it or being embarrassed to take it in front of their friends. We also discuss possible answers. These include why using the right inhaler and learning to use it effectively is important. Choosing the best treatment to suit each person is also critical. We look at how doctors can communicate better with adolescents to engage and motivate them to take their medication regularly.
Introduction
Asthma is recognized as the most common non-communicable disease in children worldwide,1 affecting approximately 8.4% of children and adolescents in the US and 9.1% in the UK,2,3 although data from the International Study of Asthma and Allergies in Childhood indicate that the prevalence of asthma symptoms in young people varies considerably between countries.4 The burden of asthma is particularly high in adolescents, with an increased prevalence and mortality compared with younger children.5–7 For example, in the US between 1980 and 2007, the number of asthma-related deaths was 1.9 per 1 million children aged 0–4 years, rising to 2.8 per 1 million children aged 11–17 years, respectively, with prevalence rising from 6.2% to 10.0% between the two age groups.6
Irrespective of age, the aim of asthma therapy is to achieve good symptom control, and to minimize the risk of future exacerbations, fixed airflow limitation and side effects of treatment.8 Treatment strategies recommended by the Global Initiative for Asthma (GINA) are tailored according to age, with separate recommendations for adults, adolescents and children aged 6–11 years versus those ≤5 years.8 However, despite the availability of effective treatments such as inhaled corticosteroids (ICS), long-acting β2-agonists and long-acting muscarinic antagonists, many children and adolescents with asthma remain uncontrolled.9 Many factors influence the success of treatment and of achieving disease control, such as asthma triggers, comorbidities and asthma phenotype.10 Other influences may be related to the physician (eg, not following guidelines, assessing the patient inappropriately, or inadequate choice of treatment or inhaler device) or the patient (eg, sociodemographic factors, exposure to cigarette smoke, poor treatment adherence, and inadequate inhaler technique or disease education).10,11 Additional contributing factors may relate to the healthcare system, such as medicinal coverage and spirometry testing.12
Although estimates vary, adherence to prescribed therapy is generally low in adolescents and children (~30–70%), as described in more detail below. Non-adherence is particularly concerning in adolescents, who have specific age-related barriers to taking their medication, which can have a disastrous impact on asthma control and subsequent outcomes.5,13–18 The aim of this review is to understand the driving factors behind non-adherence in adolescents with asthma, their consequences and possible solutions to ensure better disease control.
Classification of Adherence/Non-Adherence
Adherence is defined by the World Health Organization as “the extent to which a person’s behavior – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider.”19 Traditionally, adherence has been evaluated from the patient perspective, although more recent models have a more prominent role for healthcare professionals (HCPs).20
There are several stages where adherence to treatment can fail, as illustrated in Figure 1. Non-adherence can be divided into three distinct temporal phases: failure to initiate treatment, failure to implement treatment correctly, and non-persistence with treatment.21 Initiation (ie, when the patient takes their first dose of a prescribed medication) is typically a binary event, with patients either starting to take their medication or not.21 The second step – implementation – can be defined as the extent to which a patient’s actual dosing corresponds with their prescribed dosing regimen over time, from initiation until the last dose is taken.21 This involves taking the medication as directed, which, in asthma, includes inhaler technique. Persistence – the final step – refers to the time that elapses between initiation and eventual treatment discontinuation.21 After this time point, a period of non-persistence may follow until the end of the intended prescribing period.
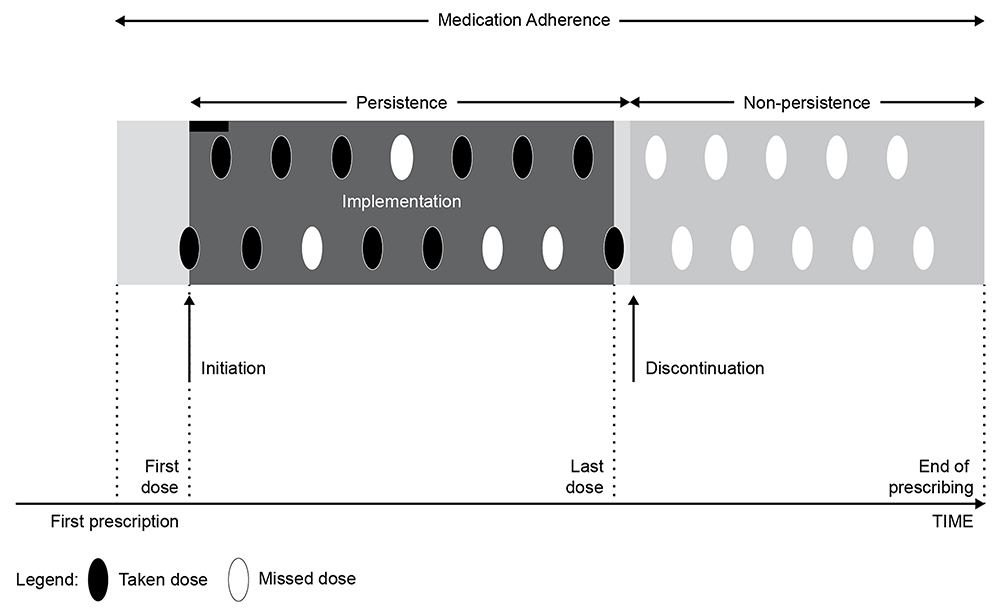 |
Figure 1 Stages of medication adherence: initiation, implementation and persistence. Reprinted from The Journal of Allergy and Clinical Immunology: In Practice, 4/5, Vrijens et al, What We Mean When We Talk About Adherence in Respiratory Medicine, 802–812, 2016, with permission from Elsevier. |
Non-adherence may either be deliberate or accidental.22 Deliberate or intentional non-adherence refers to patients missing or altering doses to suit their own needs, and includes an unwillingness to take medication as prescribed and not attending medical appointments. Accidental or unintentional non-adherence, however, includes unknowingly using the inhalation device incorrectly or forgetting to take medication as prescribed.19,22
It should be noted that non-adherence can be difficult to measure. General problems with evaluating adherence include the fact that there is currently no gold standard available, while some of the available methods are inaccurate, biased or costly.18,21 In addition, a high rate of variability is observed when calculating adherence rates, possibly due to differences between study populations, including race and age.18 Physician assessment of adherence is often inaccurate (eg, using closed- rather than open-ended questioning), and patients or caregivers may be reluctant to admit to non-adherence, contributing further to the difficulties in quantification.18
Although this review focuses specifically on medication adherence, it should be noted that non-adherence to asthma trigger modification is also a recurrent problem in clinical practice that needs to be addressed.23 Findings from a 2-year retrospective cohort study showed that advice for managing asthma triggers was given in only 30% of visits and adherence to trigger advice was evaluated at only 6% of visits.23 These results show that asthma trigger management is suboptimal across multiple healthcare settings and should be a target for improvement in routine asthma outpatient visits.23
Prevalence of Non-Adherence in Adolescents
Although adolescents are less studied than other populations, the few studies carried out in this age group show a substantial reduction in adherence compared with younger children or older patients with asthma.5,13–18,24,25 However, estimates vary from study to study, in part because of the range of methods available to evaluate adherence. These include both subjective and objective methods, as well as electronic monitoring devices, which represent the current gold standard for monitoring adherence.26
Several studies have been carried out using electronic monitoring devices. In a 6-month prospective study evaluating 27 children aged 7–12 years with mild-to-moderate asthma, adherence (evaluated using a metered-dose inhaler equipped with an electronic doser attached to their ICS) was found to decrease significantly with increasing age.13 Similar results were seen in a 1-month study of 106 children with asthma, which used electronic monitoring to measure medication adherence and also found a negative relationship between adherence and age.24 However, despite reduced adherence, adolescents in this study reported significantly increased knowledge and reasoning about asthma, and claimed to take greater responsibility for asthma management, compared with their younger counterparts.24 According to a review of pediatric asthma studies using electronic adherence monitoring, mean adherence rates are largely below 75%, while as many as half report rates of 50% or lower.15 For example, findings from an observational cohort study of 40 15–18-year-olds with asthma who were prescribed fluticasone/salmeterol, which was electronically monitored between visits, indicated a median treatment adherence of 43%, with significantly better adherence reported in the younger versus older participants.14
Although electronic adherence monitoring is widely considered to be more accurate than many other methods, several studies have looked at alternative ways of monitoring adherence. For example, a population-based cohort study of Dutch children aged 5–18 years evaluated adherence in terms of medication possession ratio and ratio of controller to total asthma drug, deriving data from a large primary care database (N>14,000).17 Using this approach, only 33% of ICS users were found to regularly use their inhaler more than 80% of the time.17 Studies using telephone interviews and retrospective analysis of prescription fills indicate that adherence to oral corticosteroids after emergency department visits is also lower in adolescents compared with younger patients.27,28
Some studies where adherence rates were self-reported by adolescents or parents gave higher estimates, although it should be noted that this method tends to give inflated figures compared with other measures.13 One study indicated a 77% rate of adherence to asthma treatment in adolescents, versus 92% in children.25 In another study, adherence recorded from interviews/surveys with adolescents and caregivers was 60% and 69%, respectively.16 Assuming that an adherence level of >75–80% is clinically relevant in terms of reducing asthma exacerbations,5,29 even these self-reported estimates of adherence in adolescents are insufficient for effective treatment.
Driving Factors Behind Non-Adherence in Adolescents
As described above, there are a number of stages during which treatment adherence can be affected. When considering adherence in asthma specifically, additional complexity is provided by the variable nature and seasonality of the condition, which further complicates medication adherence due to flexible dosage recommendations provided in self-management plans.21
Treatment initiation in asthma can be affected by a range of psychologic and practical barriers, including denial of asthma diagnosis, lack of disease awareness, lack of trust in HCPs, medication fears, stigma around using inhalers, cognitive ability, affordability and access to therapy.30 In terms of treatment implementation and persistence, challenges regarding the mode of delivery of maintenance treatment represent a major barrier to adherence.30
Below, we review in more detail the different factors that can affect medication adherence in asthma, both in general and specifically in adolescents. This information is also summarized in Table 1.
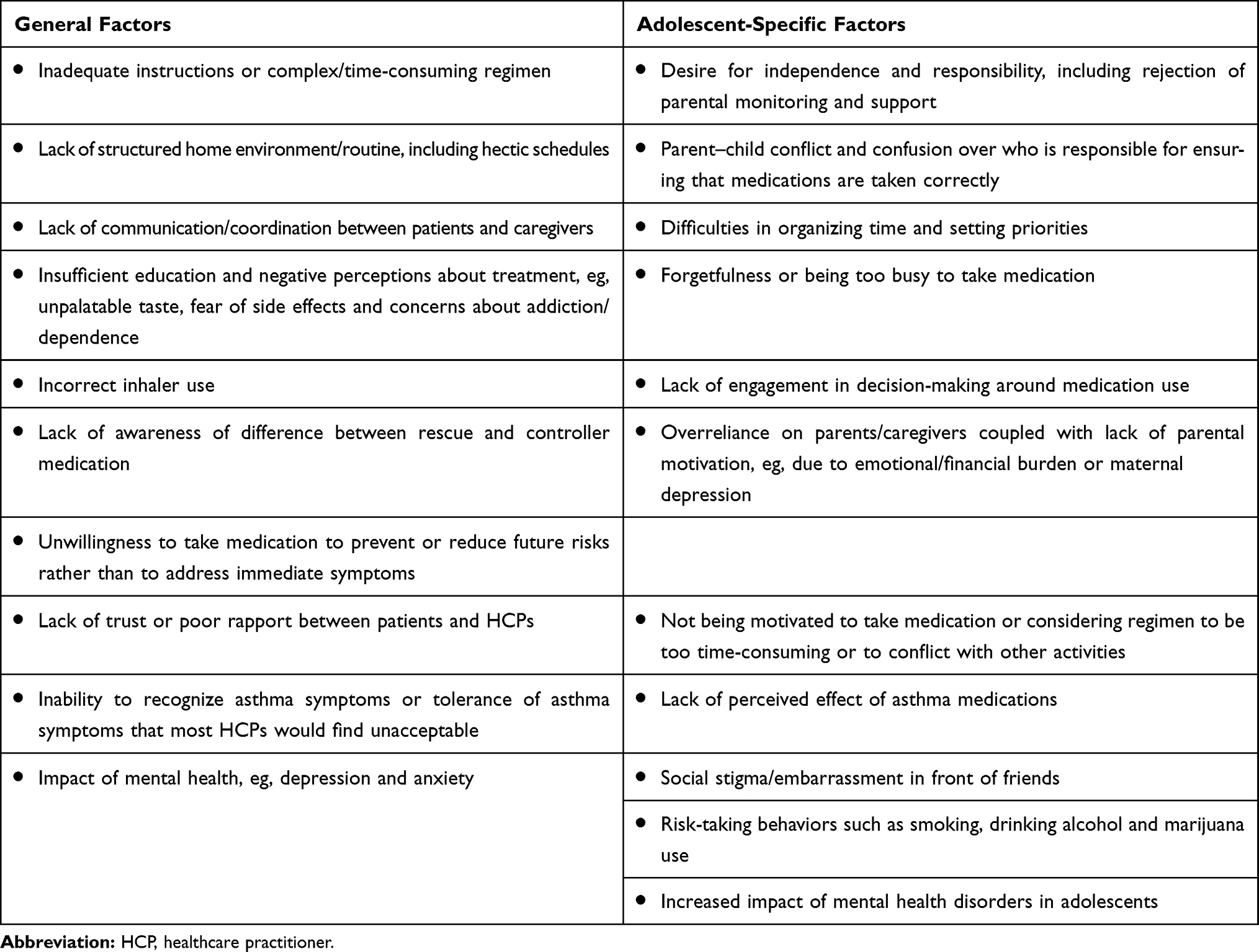 |
Table 1 Factors Affecting Asthma Medication Non-Adherence |
General Factors Affecting Non-Adherence
Asthma regimens often require planning and forethought, including filling prescriptions and taking treatment appropriately and at the correct time. Inadequate instructions, or a regimen that is too complex or time-consuming (eg, multiple components or dosing several times a day), are important considerations that can affect adherence. In addition, lack of a structured home environment with clearly structured routines is a challenge for successful daily treatment regimens.18 The hectic schedules of patients and caregivers, or parents living in separate households with insufficient communication and coordination between them, can all affect adherence.14,18
Lack of education and negative perceptions about treatment and providers also frequently influence adherence. Concerns for patients with asthma include the unpalatable taste of ICS, fear of side effects and worries about addiction/dependence.14 Education is also required to learn how to administer the treatment correctly. Incorrect inhaler use, in particular, caused by poor coordination, is common and is associated with decreased lung deposition of ICS, leading to poor asthma control.31 Patients may also be confused by the difference between rescue and controller medication, leading to unintentional poor adherence.18 Moreover, patients may also be less inclined to take medication to prevent or reduce risks rather than taking medication for immediate symptoms.14 These problems are compounded by physician-related issues, such as poor rapport with patients.18 In particular, studies suggest that between 39% and 85% of HCPs are unable to demonstrate and educate patients in the proper use of their inhaler devices.30
Asthma has also been found to affect the mental health of affected individuals,32 and studies have shown that depression and anxiety disorders are associated with increased functional impairment, which can have an adverse impact on adherence.33 In terms of symptom perception, 15–60% of patients are not able to recognize asthma symptoms,34 whereas others may tolerate asthma symptoms that most HCPs would find unacceptable.35 This may include accepting mild asthma exacerbations as normal, or attributing their asthma symptoms to other causes,35 and is associated with a heavy burden in terms of hospitalizations and emergency department visits.36 Alexithymia, a condition characterized by an inability to identify and express emotions, has also been associated with inadequate treatment adherence.32
Factors Specific to Adolescents
It is apparent that different challenges to adherence exist at successive developmental stages.37 As children with asthma become adolescents, the barriers impeding good adherence start to change. While younger children rely on caregivers and parents for the administration of asthma medication,18 adolescence is the age during which children begin to claim more independence and responsibility, which may in turn affect adherence.13,37 They begin to form individual opinions and beliefs about their health, and develop organizational skills and self-regulatory behavior that can significantly contribute to adherence. However, since adolescents often reject parental monitoring and support at this stage, parent–child conflict and confusion over who is responsible for ensuring that medications are taken correctly may follow, with adherence commonly suffering.37 Involvement in decision-making around medication use is key to ensure effective initiation, implementation and persistence with asthma medications, but lack of engagement by adolescents in this process can put adherence at risk.37
In contrast, some adolescents still rely on their parents/caregivers and struggle to take responsibility for their asthma management,38,39 and so parental motivation may still remain important for adherence.18 This can be challenging since chronic diseases such as asthma can place an emotional and financial burden on the family.18 Maternal depression has been linked with a number of factors that can affect their children’s adherence to asthma medication, including negative beliefs about asthma therapy, and lack of understanding about the function of asthma medications or how to use them effectively.40
The ease of use and acceptance of the inhaler device plays an important role in adherence in adolescents. In the UK, there is evidence that most adolescents, even those with uncontrolled severe asthma, have poor adherence to taking their medication as prescribed.39 This intentional non-adherence is associated with other factors, such as not being bothered, being too time-consuming or conflicting with other activities, as well as a lack of perceived effect of asthma medications.39,41 This is significant given that patients’ belief in their medication and the importance of inhaler use is associated with adherence.42 Other factors linked with non-adherence in adolescents include forgetfulness and being too busy to take medication.14,41,43 Adolescents surveyed about their asthma medication use cited “feeling well” and “having no symptoms” as reasons for forgetting to take medications, whereas others attributed it to difficulties in organizing time and setting priorities.14
The perceived social stigma of having an illness may also have a contributing effect on why adolescents choose not to use their inhalers, especially in public or in front of their peers.5 Insights from adolescents suggest a sense of denial over their asthma and an unwillingness to be treated differently or to be labeled as “an ill person” or “an asthmatic”.5 Stigma around using inhalers can affect adherence at the levels of initiation, implementation or persistence.30 For adolescents with asthma, embarrassment in front of friends is a predominant reason for non-adherence, including a desire to hide their condition and treatment from their peers.5,13 A study in the US found that, among adolescents, approximately 50% of non-adherence occurred in the presence of friends.44
Risk-taking behaviors such as smoking, drinking alcohol and marijuana use can also have a significant negative impact on adherence. In a survey of adolescents by the Centers for Disease Control and Prevention in the US, students reporting current asthma had a greater frequency of depressive symptoms, cigarette smoking and cocaine use than their asthma-free peers.45 Behaviors such as smoking and drinking can be interpreted as a sign of general disregard for one’s health, and this often extends to adherence.46 A study examining the circumstances surrounding 21 asthma-related deaths of children and adolescents found the risk profile included depressive symptoms in adolescents, family dysfunction, parental psychopathology, alcoholism, and lack of self-care and adherence.47
Children and adolescents with symptomatic asthma are also reported to be more likely to suffer from mental health disorders compared with their healthy peers, which in turn has an impact on adherence.32 The evidence to date implies that the development of asthma may predispose patients to depression, anxiety and other mood disorders, and that these may in turn influence disease severity and control.32 Reports from caregivers suggest that over 40% of children and adolescents with asthma aged 6–16 years have major or minor psychosocial problems, representing a doubling compared with the general population, which will, in turn, have a knock-on effect upon adherence.48
Consequences of Non-Adherence
The main consequence of non-adherence to asthma medications is a decrease in asthma control, leading to poor symptom control, higher rates of exacerbations and reduced quality of life.18,30,49 The relationship between good adherence and decreased frequency of exacerbations is well established, with the primary treatment benefit seen in patients with >75–80% adherence.29 However, given that adherence is considerably lower than this according to most studies carried out in adolescents, the impact on asthma control may be substantial.
Uncontrolled asthma resulting from inadequate adherence and other factors is a major cause of mortality and disability, particularly in children and adolescents.18 Non-adherence can also lead to a significant increase in healthcare utilization and costs, including hospitalizations and emergency department visits, due to lack of asthma control.49,50 This may include increased use of oral corticosteroids, which can have both short- and long-term adverse consequences.51 If non-adherence remains undetected, the dose of medication may be increased or extra treatment may be prescribed unnecessarily in order to try to achieve disease control, thus further increasing the cost and complexity of the regimen.22 Other consequences may include sleep disruption and a limited ability to do sports or recreational activities.50 Poorly controlled asthma is also one of the leading causes of school absenteeism in the US annually, with a total of 13.8 million missed school days reported in 2013.52
Possible Solutions to Non-Adherence
Improving Inhaler Technique
Poor inhaler instruction and technique represent a fundamental cause of asthma medication non-adherence, resulting in ineffective drug delivery to the lungs and a reduction in medication efficacy.30 Improving understanding of the need for inhaled therapy and advice on optimal technique for using the inhaler device should increase patient adherence.30
HCPs can help to improve adherence by ensuring that they have good knowledge across a range of inhaler devices and device types, so that they can advise their patients optimally.30 Assessments of inhaler technique, using checklists of critical inhaler errors as a guide, should be carried out regularly, and retraining and/or alternative treatment options considered where appropriate.30,53 The CRITical Inhaler mistaKes and Asthma controL (CRITIKAL) study identified certain inhaler errors that were considered to be the most important, based on their impact on asthma outcomes.54 For example, insufficient inspiratory effort (reported in 32–38% of dry-powder inhaler users) was associated with uncontrolled asthma and increased exacerbation rate, and actuation before inhalation (reported in 24.9% of metered-dose inhaler users) was associated with uncontrolled asthma.55 It is therefore important that primary and secondary care management of asthma should implement inhaler training to specifically target these critical errors.55
Choosing the Most Appropriate Inhaler
Patient preference for and satisfaction with specific inhaler devices also correlates with improved adherence and clinical outcomes.11,56 Some studies suggest that specific inhaler types may be associated with better adherence, although further investigation is needed to confirm this.56
Many factors, including age, dexterity, inspiratory capacity, cognitive ability, health literacy and ethnicity, affect the ability and motivation of patients to use their inhaler devices, and it is therefore imperative that the most appropriate inhaler device to suit each individual patient is chosen in order to improve adherence.54 This includes taking into account patients’ demographic characteristics, lifestyle and comorbidities, as well as patient preferences.30,42,54 Features to consider include ease of use (eg, learning to use, holding, operating and cleaning), convenience (eg, size, color, shape, durability and weight) and oral sensation (eg, taste and irritation).42 All adolescents should be encouraged to use their metered-dose inhaler with a spacer or else to use a dry-powder inhaler.42,57 For this age group, in particular, regular review by an HCP who has received inhalation technique training is essential.42
Choosing the Most Appropriate Medication
Choice of medication may also affect adherence; for example, when comparing as-needed treatment with maintenance therapy. Results from the SYmbicort Given as needed in Mild Asthma (SYGMA) program showed that as-needed budesonide/formoterol combination therapy had a comparable effect on exacerbations compared with maintenance budesonide (although with substantially lower glucocorticoid exposure), and a superior effect on both symptoms and exacerbations versus terbutaline therapy in patients with mild asthma.58,59 This approach represents an alternative treatment option for patients with mild asthma who may rely too heavily on short-acting β2-agonist (SABA) reliever medication – which does not address underlying inflammation – and who may be less adherent with maintenance therapy.60 In support of this, the 2019 GINA recommendations include as-needed ICS/formoterol for adolescents and adults with mild asthma.8
Enhancing Collaboration with HCPs
Adherence also improves when physicians and patients collaborate to ensure comprehensive understanding of asthma and the necessary treatment.61,62 A model of how clinicians and patients with asthma can collaborate effectively is shown in Figure 2.
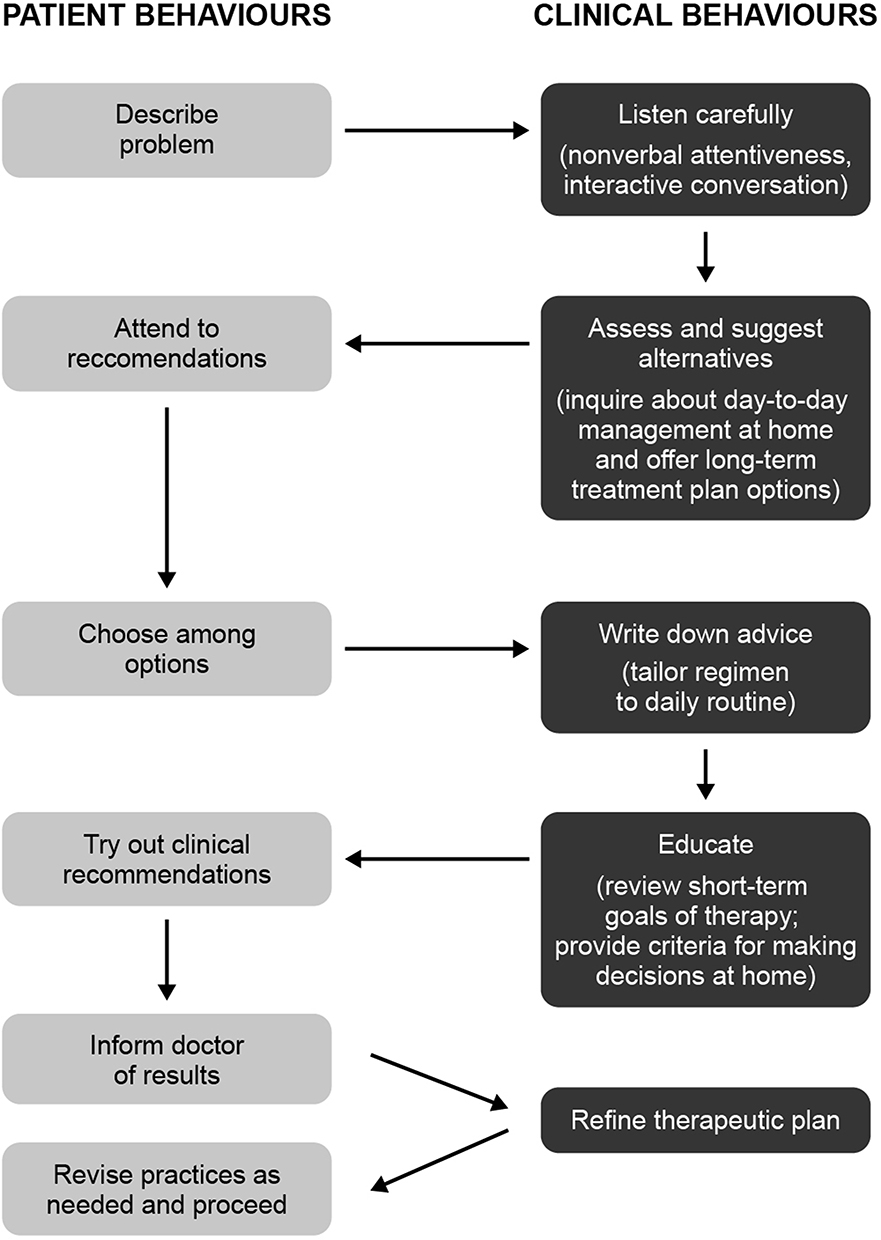 |
Figure 2 Model of clinician–patient partnership in asthma. Reprinted from Clinical Pediatrics, 47 (1), Clark et al, The Clinician-Patient Partnership Paradigm: Outcomes Associated With Physician Communication Behavior, 49–57, 2017, with permission from SAGE Publications. |
Clear and open patient–physician communication that builds empathy and incorporates motivational interviewing techniques and shared decision-making/treatment goals is vital, particularly for adolescents.62 This approach can address patient-specific concerns, evaluate their beliefs, engage patients in the management of their disease, and ensure family members are educated and able to support the patient. Understanding is key in order to recognize any symptom changes and to adjust treatment, or switch to available treatment alternatives according to guidelines. It is also important to ensure that regular follow-up appointments are arranged with the treating physician, with reminders and other organizational factors to help improve adherence.62
Other Strategies
Given the poor adherence of adolescents to their asthma regimens, one approach that may help to support behavior modification is the routine identification of non-adherent patients.26 Several methods of adherence monitoring are available, each with a unique set of advantages and disadvantages. These include subjective monitoring tools (for example, physician assessment of adherence, parental/child assessment of adherence, or self-report questionnaires such as the Morisky scale, Medicines Adherence Report Scale – Asthma, Test of the Adherence to Inhalers and Beliefs About Medication Questionnaire).26,63,64 In addition, a questionnaire has recently been developed that is specific to adolescents with asthma, called the Adolescent Asthma Self-Efficacy Questionnaire.65 Objective monitoring approaches are also available, including analysis of prescription data, weighing inhaler canisters, dose counters, directly observed therapy and nurse home visits.26 Meanwhile, other approaches are being evaluated, including reminder-based systems (eg, electronic medical record reminders), the integration of digital technologies (eg, sensors from Adherium, Propeller Health and Timestamp66), controller apps and biomarkers of adherence.26, 62,67,68
The current gold standard method of measuring adherence – electronic monitoring – assesses when and how often patients activate their inhaler, with the potential to download data using smartphone applications.26 Although electronic monitoring devices are widely regarded as the most accurate and objective measure of recording medication use, many of them have drawbacks, including cost and a lack of information on inhaler technique or why patients are non-adherent.26 However, findings from a survey show that this is a popular approach with adolescents, enabling them to achieve a greater degree of responsibility and independence,69 and some models (such as the INCA device) have been adapted to include sensors that can monitor inhalation.26 Electronic monitoring also has an important role in determining future management, both in terms of tailoring adherence interventions and in supporting decision-making regarding treatment changes.70 Management needs to focus on and address the reasons for poor adherence rather than simply escalating the prescribed treatment.70 Importantly, electronic monitoring can help to identify those people with poor asthma control despite good adherence who may be eligible for more expensive therapies, such as biologics.70
Other approaches that adolescents suggest may help to influence adherence include peer support, medication reminders (preferably via smartphone applications) and user-friendly online support systems with messaging functionality.41,71 In addition, routine screening for depression and other mood/mental disorders may also result in better asthma control71 and thus increase adherence.
Conclusion
Medication adherence in adolescents with asthma faces many challenges. Identifying the reasons for poor disease control and adherence is essential in order to help improve patient quality of life.
Patient/HCP communication is a key component for effective and comprehensive patient assessment and for tailoring treatment to individual requirements.
Abbreviations
CRITIKAL, CRITical Inhaler mistaKes and Asthma controL; GINA, Global Initiative for Asthma; HCP, healthcare professional; ICS, inhaled corticosteroids; SABA, short-acting β2-agonist; SYGMA, SYmbicort Given as needed in Mild Asthma.
Acknowledgments
Cindy Macpherson from MediTech Media has provided medical writing assistance, funded by Boehringer Ingelheim.
Disclosure
Dr. Kaplan reports personal fees from Boehringer Ingelheim, Covis, GlaxoSmithKline, Teva, Novartis, Pfizer, AstraZeneca, Purdue, Sanofi, Paladdin and Trudell outside the submitted work. Professor David Price has board membership with Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Circassia, Mylan, Mundipharma, Napp, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme and Teva Pharmaceuticals; consultancy agreements with Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Mylan, Mundipharma, Napp, Novartis, Pfizer, Teva Pharmaceuticals and Theravance; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from AKL Research and Development Ltd, AstraZeneca, Boehringer Ingelheim, British Lung Foundation, Chiesi, Circassia, Mylan, Mundipharma, Napp, Novartis, Pfizer, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi Genzyme, Teva Pharmaceuticals, Theravance, UK National Health Service and Zentiva (Sanofi Generics); payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mylan, Merck, Mundipharma, Novartis, Pfizer, Regeneron Pharmaceuticals, Sanofi Genzyme and Teva Pharmaceuticals; payment for manuscript preparation from Mundipharma and Teva Pharmaceuticals; payment for the development of educational materials from Mundipharma and Novartis; payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Circassia, Mundipharma, Napp, Novartis and Teva Pharmaceuticals; funding for patient enrollment or completion of research from Chiesi, Novartis, Teva Pharmaceuticals and Zentiva (Sanofi Generics); stock/stock options from AKL Research and Development Ltd; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia and UK) and 74% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); and is peer reviewer for grant committees of the Efficacy and Mechanism Evaluation Programme and Health Technology Assessment. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Asthma fact sheet 307. 2017.
2. Centers for Disease Control and Prevention. National Health Interview Survey (NHIS) Data. 2015.
3. Asthma UK. Asthma facts and statistics, 2017.
4. Lai CK, Beasley R, Crane J, et al. Global variation in the prevalence and severity of asthma symptoms: phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax. 2009;64:476–483. doi:10.1136/thx.2008.106609
5. De Simoni A, Horne R, Fleming L, et al. What do adolescents with asthma really think about adherence to inhalers? Insights from a qualitative analysis of a UK online forum. BMJ Open. 2017;7:e015245. doi:10.1136/bmjopen-2016-015245
6. Akinbami LJ, Moorman JE, Garbe PL, et al. Status of childhood asthma in the United States, 1980–2007. Pediatrics. 2009;123:S131–S145. doi:10.1542/peds.2008-2233C
7. Akinbami LJ, Schoendorf KC. Trends in childhood asthma: prevalence, health care utilization, and mortality. Pediatrics. 2002;110:315–322. doi:10.1542/peds.110.2.315
8. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention (2019 Update). 2019.
9. Hamelmann E, Szefler SJ, Lau S. Severe asthma in children and adolescents. Allergy. 2019;74:2280–2282. doi:10.1111/all.13862
10. Braido F. Failure in asthma control: reasons and consequences. Scientifica (Cairo). 2013;2013:549252.
11. Price D, Harrow B, Small M, et al. Establishing the relationship of inhaler satisfaction, treatment adherence, and patient outcomes: a prospective, real-world, cross-sectional survey of US adult asthma patients and physicians. World Allergy Organ J. 2015;8:26. doi:10.1186/s40413-015-0075-y
12. Rabe KF, Adachi M, Lai CK, et al. Worldwide severity and control of asthma in children and adults: the global asthma insights and reality surveys. J Allergy Clin Immunol. 2004;114:40–47. doi:10.1016/j.jaci.2004.04.042
13. Bender B, Wamboldt FS, O’Connor SL, et al. Measurement of children’s asthma medication adherence by self report, mother report, canister weight, and doser CT. Ann Allergy Asthma Immunol. 2000;85:416–421. doi:10.1016/S1081-1206(10)62557-4
14. Naimi DR, Freedman TG, Ginsburg KR, et al. Adolescents and asthma: why bother with our meds? J Allergy Clin Immunol. 2009;123:1335–1341. doi:10.1016/j.jaci.2009.02.022
15. Morton RW, Everard ML, Elphick HE. Adherence in childhood asthma: the elephant in the room. Arch Dis Child. 2014;99:949–953. doi:10.1136/archdischild-2014-306243
16. Sleath B, Gratie D, Carpenter D, et al. Reported problems and adherence in using asthma medications among adolescents and their caregivers. Ann Pharmacother. 2018;52:855–861. doi:10.1177/1060028018766603
17. Engelkes M, Janssens HM, de Jongste JC, et al. Prescription patterns, adherence and characteristics of non-adherence in children with asthma in primary care. Pediatr Allergy Immunol. 2016;27:201–208. doi:10.1111/pai.12507
18. Desai M, Oppenheimer JJ. Medication adherence in the asthmatic child and adolescent. Curr Allergy Asthma Rep. 2011;11:454–464. doi:10.1007/s11882-011-0227-2
19. World Health Organization. Adherence to Long-Term Therapies – Evidence for Action. Geneva: World Health Organization; 2003.
20. Amir M, Feroz Z, Beg AE. A new health care professional-based model for medication adherence. Patient Prefer Adherence. 2018;12:2085–2091. doi:10.2147/PPA.S171989
21. Vrijens B, Dima AL, Van Ganse E, et al. What we mean when we talk about adherence in respiratory medicine. J Allergy Clin Immunol. 2016;4:802–812. doi:10.1016/j.jaip.2016.05.019
22. Burgess S, Sly P, Devadason S. Adherence with preventive medication in childhood asthma. Pulm Med. 2011;2011:973849. doi:10.1155/2011/973849
23. Rank MA, Wollan P, Li JT, et al. Trigger recognition and management in poorly controlled asthmatics. Allergy Asthma Proc. 2010;31:99–105. doi:10.2500/aap.2010.31.3405
24. McQuaid EL, Kopel SJ, Klein RB, et al. Medication adherence in pediatric asthma: reasoning, responsibility, and behavior. J Pediatr Psychol. 2003;28:323–333. doi:10.1093/jpepsy/jsg022
25. Raherison C, Tunon-de-Lara JM, Vernejoux JM, et al. Practical evaluation of asthma exacerbation self-management in children and adolescents. Respir Med. 2000;94:1047–1052. doi:10.1053/rmed.2000.0888
26. Pearce CJ, Fleming L. Adherence to medication in children and adolescents with asthma: methods for monitoring and intervention. Expert Rev Clin Immunol. 2018;14:1–9. doi:10.1080/1744666X.2018.1532290
27. Butler K, Cooper WO. Adherence of pediatric asthma patients with oral corticosteroid prescriptions following pediatric emergency department visit or hospitalization. Pediatr Emerg Care. 2004;20:730–735. doi:10.1097/01.pec.0000144914.78124.6f
28. Cooper WO, Hickson GB. Corticosteroid prescription filling for children covered by Medicaid following an emergency department visit or a hospitalization for asthma. Arch Pediatr Adolescent Med. 2001;155:1111–1115. doi:10.1001/archpedi.155.10.1111
29. Williams LK, Peterson EL, Wells K, et al. Quantifying the proportion of severe asthma exacerbations attributable to inhaled corticosteroid nonadherence. J Allergy Clin Immunol. 2011;128:1185–1191.e1182. doi:10.1016/j.jaci.2011.09.011
30. Braido F, Chrystyn H, Baiardini I, et al. “Trying, but failing” – the role of inhaler technique and mode of delivery in respiratory medication adherence. J Allergy Clin Immunol. 2016;4:823–832. doi:10.1016/j.jaip.2016.03.002
31. Giraud V, Roche N. Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur Respir J. 2002;19:246–251. doi:10.1183/09031936.02.00218402
32. Baiardini I, Sicuro F, Balbi F, et al. Psychological aspects in asthma: do psychological factors affect asthma management? Asthma Res Pract. 2015;1:7. doi:10.1186/s40733-015-0007-1
33. McCauley E, Katon W, Russo J, et al. Impact of anxiety and depression on functional impairment in adolescents with asthma. Gen Hosp Psychiatry. 2007;29:214–222. doi:10.1016/j.genhosppsych.2007.02.003
34. Janssens T, Verleden G, De Peuter S, et al. Inaccurate perception of asthma symptoms: a cognitive-affective framework and implications for asthma treatment. Clin Psychol Rev. 2009;29:317–327. doi:10.1016/j.cpr.2009.02.006
35. Yawn BP. The role of the primary care physician in helping adolescent and adult patients improve asthma control. Mayo Clin Proc. 2011;86:894–902. doi:10.4065/mcp.2011.0035
36. Rhee H, Belyea MJ, Halterman JS. Adolescents’ perception of asthma symptoms and health care utilization. J Pediatr Health Care. 2011;25:105–113. doi:10.1016/j.pedhc.2009.10.003
37. Costello RW, Foster JM, Grigg J, et al. The seven stages of man: the role of developmental stage on medication adherence in respiratory diseases. J Allergy Clin Immunol. 2016;4:813–820. doi:10.1016/j.jaip.2016.04.002
38. Blaakman SW, Cohen A, Fagnano M, et al. Asthma medication adherence among urban teens: a qualitative analysis of barriers, facilitators and experiences with school-based care. J Asthma. 2014;51:522–529. doi:10.3109/02770903.2014.885041
39. Edgecombe K, Latter S, Peters S, et al. Health experiences of adolescents with uncontrolled severe asthma. Arch Dis Child. 2010;95:985–991. doi:10.1136/adc.2009.171579
40. Bartlett SJ, Krishnan JA, Riekert KA, et al. Maternal depressive symptoms and adherence to therapy in inner-city children with asthma. Pediatrics. 2004;113:229–237. doi:10.1542/peds.113.2.229
41. Koster ES, Philbert D, de Vries TW, et al. “I just forget to take it”: asthma self-management needs and preferences in adolescents. J Asthma. 2015;52:831–837. doi:10.3109/02770903.2015.1020388
42. Price D, Bosnic-Anticevich S, Inhaler Error Steering C, et al. Inhaler competence in asthma: common errors, barriers to use and recommended solutions. Respir Med. 2013;107:37–46. doi:10.1016/j.rmed.2012.09.017
43. Koster ES, Philbert D, Winters NA, et al. Adolescents’ inhaled corticosteroid adherence: the importance of treatment perceptions and medication knowledge. J Asthma. 2015;52:431–436. doi:10.3109/02770903.2014.979366
44. Mulvaney SA, Ho YX, Cala CM, et al. Assessing adolescent asthma symptoms and adherence using mobile phones. J Med Internet Res. 2013;15:e141. doi:10.2196/jmir.2413
45. Bender BG. Depression symptoms and substance abuse in adolescents with asthma. Ann Allergy Asthma Immunol. 2007;99:319–324. doi:10.1016/S1081-1206(10)60547-9
46. Bender BG. Risk taking, depression, adherence, and symptom control in adolescents and young adults with asthma. Am J Respir Crit Care Med. 2006;173:953–957. doi:10.1164/rccm.200511-1706PP
47. Strunk RC, Mrazek DA, Fuhrmann GS, et al. Physiologic and psychological characteristics associated with deaths due to asthma in childhood. A Case-Controlled Study. JAMA. 1985;254:1193–1198.
48. Tibosch M, Reidsma C, Landstra A, et al. An asthma-related quality of life instrument is unable to identify asthmatic children with major psychosocial problems. Eur J Pediatr. 2010;169:1495–1501. doi:10.1007/s00431-010-1250-3
49. Makela MJ, Backer V, Hedegaard M, et al. Adherence to inhaled therapies, health outcomes and costs in patients with asthma and COPD. Respir Med. 2013;107:1481–1490. doi:10.1016/j.rmed.2013.04.005
50. Ahmad A, Sorensen K. Enabling and hindering factors influencing adherence to asthma treatment among adolescents: a systematic literature review. J Asthma. 2016;53:862–878. doi:10.3109/02770903.2016.1155217
51. Price DB, Trudo F, Voorham J, et al. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J Asthma Allergy. 2018;11:193–204. doi:10.2147/JAA.S176026
52. Centers for Disease Control and Prevention. Asthma-related missed school days among children aged 5–17 years. 2015.
53. Kaplan A, Price D. Matching inhaler devices with patients: the role of the primary care physician. Can Respir J. 2018;2018:9473051. doi:10.1155/2018/9473051
54. Price DB, Roman-Rodriguez M, McQueen RB, et al. Inhaler errors in the CRITIKAL study: type, frequency, and association with asthma outcomes. J Allergy Clin Immunol. 2017;5:1071–1081. doi:10.1016/j.jaip.2017.01.004
55. Lenney J, Innes JA, Crompton GK,. Inappropriate inhaler use: assessment of use and patient preference of seven inhalation devices EDICI. Respir Med. 2000;94:496–500. doi:10.1053/rmed.1999.0767
56. Laube BL, Janssens HM, de Jongh FH, et al. What the pulmonary specialist should know about the new inhalation therapies. Eur Respir J. 2011;37:1308–1331. doi:10.1183/09031936.00166410
57. Bateman ED, Reddel HK, O’Byrne PM, et al. As-needed budesonide-formoterol versus maintenance budesonide in mild asthma. N Engl J Med. 2018;378:1877–1887. doi:10.1056/NEJMoa1715275
58. O’Byrne PM, FitzGerald JM, Bateman ED, et al. Inhaled combined budesonide-formoterol as needed in mild asthma. N Engl J Med. 2018;378:1865–1876. doi:10.1056/NEJMoa1715274
59. O’Byrne PM, FitzGerald JM, Zhong N, et al. The SYGMA programme of Phase 3 trials to evaluate the efficacy and safety of budesonide/formoterol given ‘as needed’ in mild asthma: study protocols for two randomised controlled trials. Trials. 2017;18:12. doi:10.1186/s13063-016-1731-4
60. Bender B, Milgrom H, Apter A. Adherence intervention research: what have we learned and what do we do next? J Allergy Clin Immunol. 2003;112:489–494. doi:10.1016/S0091-6749(03)01718-4
61. van Boven JF, Ryan D, Eakin MN, et al. Enhancing respiratory medication adherence: the role of health care professionals and cost-effectiveness considerations. J Allergy Clin Immunol. 2016;4:835–846. doi:10.1016/j.jaip.2016.03.007
62. Plaza V, Fernández-Rodríguez C, Melero C, et al. Validation of the ‘Test of the Adherence to Inhalers’ (TAI) for asthma and COPD patients. J Aerosol Med Pulm Drug Deliv. 2016;29:142–152. doi:10.1089/jamp.2015.1212
63. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14:1–24. doi:10.1080/08870449908407311
64. Holley S, Knibb R, Latter S, et al. Development and validation of the Adolescent Asthma Self-Efficacy Questionnaire (AASEQ). Eur Respir J. 2019;54:1801375. doi:10.1183/13993003.01375-2018
65. TimeStamp. Home page. 2018.
66. Kagen S, Garland A. Asthma and allergy mobile apps in 2018. Curr Allergy Asthma Rep. 2019;19:6. doi:10.1007/s11882-019-0840-z
67. Lei D, Sokol K. Improving the use of spirometry in the diagnosis and management of asthma with an EMR alert. J Allergy Clin Immunol. 2017;139:AB89. doi:10.1016/j.jaci.2016.12.243
68. Howard S, Lang A, Sharples S, et al. See I told you I was taking it! - Attitudes of adolescents with asthma towards a device monitoring their inhaler use: implications for future design. Appl Ergon. 2017;58:224–237. doi:10.1016/j.apergo.2016.06.018
69. Jochmann A, Artusio L, Jamalzadeh A, et al. Electronic monitoring of adherence to inhaled corticosteroids: an essential tool in identifying severe asthma in children. Eur Respir J. 2017;50:1700910. doi:10.1183/13993003.00910-2017
70. Panzera AD, Schneider TK, Martinasek MP, et al. Adolescent asthma self-management: patient and parent-caregiver perspectives on using social media to improve care. J School Health. 2013;83:921–930. doi:10.1111/josh.12111
71. Goodwin RD, Robinson M, Sly PD, et al. Severity and persistence of asthma and mental health: a birth cohort study. Psychol Med. 2013;43:1313–1322. doi:10.1017/S0033291712001754
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.