Back to Journals » Substance Abuse and Rehabilitation » Volume 17
Trauma History Among Patients Receiving Methadone Maintenance Treatment: Sex Differences, Characteristics, and Outcomes
Authors Peles E ![]() , Sason A, Adelson M
, Sason A, Adelson M
Received 30 March 2026
Accepted for publication 27 May 2026
Published 15 June 2026 Volume 2026:17 608409
DOI https://doi.org/10.2147/SAR.S608409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rajendra Badgaiyan
Einat Peles,1– 3 Anat Sason,1 Miriam Adelson1
1Dr. Miriam & Sheldon G. Adelson Clinic for Drug Abuse, Treatment & Research, Psychiatry Department, Tel-Aviv Sourasky University Medical Center, Tel Aviv, Israel; 2Gray Faculty of Medical and Health Sciences, Tel-Aviv University, Tel Aviv, Israel; 3Sagol School of Neuroscience, Tel-Aviv University, Tel Aviv, Israel
Correspondence: Einat Peles, Dr. Miriam & Sheldon G. Adelson Clinic for Drug Abuse, Treatment & Research, Tel-Aviv Sourasky University Medical Center, 10 Dafna Street, Tel-Aviv, 6492805, Israel, Tel +972-3-6973226, Fax +972-3-6973822, Email [email protected]
Background: Most patients with opioid use disorder have experienced traumatic events; however, sex differences in trauma exposure, its timing, and its association with treatment outcomes remain unclear.
Methods: Of the 1194 patients admitted to a methadone maintenance treatment (1993– 2025), 923 completed an intake questionnaire assessing traumatic events and their timing relative to substance use (before, during, “always”, or “never”). Predictors of long-term retention were examined using Kaplan–Meier analyses and a Cox multivariate model.
Results: Of 923 participants, 23.5% were female, and 74.4% reported trauma. Males (35.7%) more often reported trauma during substance use than females (27.6%), whereas females more frequently reported trauma occurring “always” (31.3%) than males (22.2%; p=0.024). Interpersonal trauma category was more prevalent in females (59% vs. 40.2%, p< 0.001) with no differences in physical trauma (50.8%) and self-directed harm (38.8%). The age of opioid initiation was comparable between sexes but females were admitted to MMT younger. Substance use at admission was comparable between sexes, as were one-year and long-term retention (mean=9.8 years, 95% CI 9.1– 10.6). Long-term retention between trauma timing groups and trauma categories were comparable, also when stratified by sex. Sex-specific differences emerged only when trauma type and timing were considered. Specifically rape history was associated with shorter retention among males but not females.
Conclusion: Traumatic experiences differed between sexes but were not associated with long-term retention and did not change the comparable outcomes between sexes. A bigger sample is needed to confirm the findings of shorter retention in male who experienced rape.
Keywords: trauma history, long-term retention, sex differences, retention, methadone maintenance treatment
Introduction
Exposure to traumatic experiences, particularly during childhood, has been consistently associated with the development of substance use disorders (SUDs). Traumas during childhood of all types (emotional, physical, sexual abuse and emotional and physical neglect) are well-established risk factors for later substance abuse, with trauma exposure also linked to increased psychiatric symptom burden among affected individuals.1,2 Sex differences have been repeatedly observed in both the prevalence and impact of trauma. Females report higher rates of childhood abuse and intimate partner violence than males, and the association between childhood physical or sexual abuse and SUDs appears to be stronger among females.3,4 Moreover, females are more likely than males to have experienced traumatic events prior to substance use initiation.5
Within the context of opioid use disorder (OUD), childhood trauma is a recognized risk factor.6,7 The prevalence of childhood trauma among individuals with OUD is substantial, ranging from 16% to 43% across different trauma types.7 In a large US study across multiple addiction treatment facilities, including methadone maintenance treatment (MMT), nearly half of the participants (49.3%) reported lifetime physical and/or sexual trauma, with females reporting rates up to five times higher than males.2
Sex differences extend beyond trauma exposure to clinical presentation and treatment outcomes. Systematic reviews and cohort studies have demonstrated that females receiving MMT exhibit greater impairment across multiple domains, including employment, social functioning, and physical and psychiatric health, whereas males show higher rates of criminal involvement and alcohol use.5,8,9 Retention, which reflects treatment success in MMT, has generally been comparable between sexes;10–12 however, higher retention has been reported among methadone-treated females compared with males, while lower retention has been observed among buprenorphine-treated females,13 with inconsistent findings reported in a meta-analysis of buprenorphine studies.14
Despite the high prevalence of trauma among patients receiving MMT, important gaps remain regarding the role of trauma timing and sex-specific patterns in shaping treatment outcomes. Traumatic experiences may precede substance use initiation and contribute to its onset, while additional traumas may occur later as a consequence of substance use-related lifestyles. The type and timing of trauma may therefore differ by sex and may have distinct implications for treatment outcomes (including retention and substance use discontinuation). In the current study, we examined patient characteristics and treatment outcomes in relation to the timing of traumatic experiences, with a particular focus on sex differences. We hypothesized that trauma prevalence, timing, and associated outcomes would differ between males and females, reflecting distinct clinical profiles within MMT populations.
Materials and Methods
All participants provided written informed consent at admission to MMT before data collection. The study was approved by the Tel-Aviv Sourasky Medical Center (TASMC) Institutional Review Board (IRB) (“Helsinki Committee” Protocol no. 07–111).
Study Population
The MMT clinic is accredited by the Commission on Accreditation of Rehabilitation Facilities (CARF) and is affiliated with a large, tertiary, university medical center. The clinic treats approximately 300 patients who meet criteria similar to those specified in US federal regulations for entry into methadone treatment (ie, DSM-5 criteria for opioid dependence with multiple daily self-administrations of heroin for at least one year, and according to the Israeli Ministry of Health, at least two failed institutional detoxification attempts). The clinic opened on June 25, 1993, and through December 2025, a total of 1194 patients had been admitted to MMT.
In July 2002, a structured questionnaire regarding trauma history was incorporated into the patients’ intake assessment and was completed by all current patients (around 300) at that time. Thereafter the questionnaire was completed by all newly admitted patients as part of the intake process, resulting in trauma history data for 923 patients (77.3%) of the 1194 patients ever admitted MMT. Patients with missing trauma history data were primarily those who left treatment before 2002. This was reflected in the significantly shorter treatment duration among the 271 patients without trauma history data (cumulative retention: 1.9 years, 95% CI 1.5–2.2), compared with the 923 patients with available trauma data (9.8 years, 95% CI 9.1–10.6; p < 0.001).
As part of the intake process, patients were interviewed by their therapist using a structured questionnaire that specifically asked about the following traumatic experiences: motor vehicle accidents (as a driver or non-driver), falls, rape, suicide attempts, physical violence, self-harm, and fire-related injuries. For each trauma type, timing (occurring prior to and/or since substance use onset) was self-reported as part of the intake assessment. We defined “any prior trauma” as at least one traumatic event occurring before substance use onset, and “any trauma during” as at least one traumatic event occurring since substance use onset. Trauma timing was also classified into four categories: patients with no trauma (“never”), trauma prior to substance use only, trauma since substance use onset only, and trauma occurring both prior to and since substance use onset (“always”).
Trauma types were also grouped into three categories; physical trauma (driver or non-driver car accident, falls), interpersonal trauma (violence, rape), and any self-directed harm (suicide attempt, self-damage, self-fire).
To examine potential changes in traumas prevalence over time, we stratified the patient group into three periods based on year of admission: 1993–2002 (n=314), 2003–2014 (n=331), 2015–2025 (n=278).
Treatment outcome included one year retention, drug discontinuation after one year, and cumulative retention since first admission and until left or end of follow-up (December 31, 2025).
Patients sociodemographic and addiction history were taken from patient’s chart. Specifically, age of admission, age of opioid onset, age of cannabis onset, age of benzodiazepine onset, years of education, ever drug injected, living status (alone or with a partner), having children, and place of birth. Laboratory results for hepatitis C and HIV antibody, and hepatitis B antigen were taken, as well as DSM-IV-TR psychiatric diagnosis made by senior psychiatrist at admission to MMT.
Urine Toxicology
Patients undergo repeated observed random urine tests (around 2 per month) throughout the entire length of their treatment. Opiates, cocaine metabolite (benzoylecgonine), benzodiazepine, cannabinoids (THC), and methadone metabolite are detected by enzyme immunoassay systems (DRI® and CEDIA®).15 Positive results for each substance were defined as having at least one positive screening test during the admission month, and after a year in MMT (month 13).
Statistical Analyses
Statistical analyses were performed using the IBM SPSS Statistics version 30 package. Comparisons between groups were performed using the chi-square test or Fisher’s exact test for categorical variables and one-way analysis of variance (ANOVA) for continuous variables. ANCOVA was performed to control for sex and for variables that differed significantly in univariate analyses (p ≤ 0.05). For significant comparisons, F values (for ANOVA or ANCOVA) and likelihood ratio or linear-by-linear association statistics (for chi-square tests) are reported. Kaplan-Meier analysis was used to compare cumulative retention between groups, with the Log rank test used to assess statistical significance. Mean and 95% confidence intervals (CI) are reported and for significant difference log rank chi square is reported. To specifically examine sex different in trauma-related retention, Kaplan Meier analyses were stratified by sex for each trauma group. A multivariate Cox proportional hazards model was performed to control for variables found to be significant in univariate analyses.
Results
Characteristics Differences Between Sex Groups (Table 1)
Age at opioid use onset did not differ between sexes (p = 0.2), but females were admitted to MMT at a younger age (p < 0.001), following a shorter duration of opioid use (p < 0.001). More males had ever used cannabis (p < 0.001), and they initiated use at a younger age than females (p < 0.001). Similarly, more males had ever used benzodiazepines (p = 0.006), but their age of onset was older than that of females (p = 0.005). More males ever drug injected (p=0.05). Females were more educated (p < 0.001), a higher proportion had children (p = 0.01), and a higher proportion had Axis I and II psychiatric diagnoses (p = 0.012). The proportion of patients who tested positive for any substance (cocaine, cannabis, or benzodiazepines) in urine at admission did not differ between sexes.
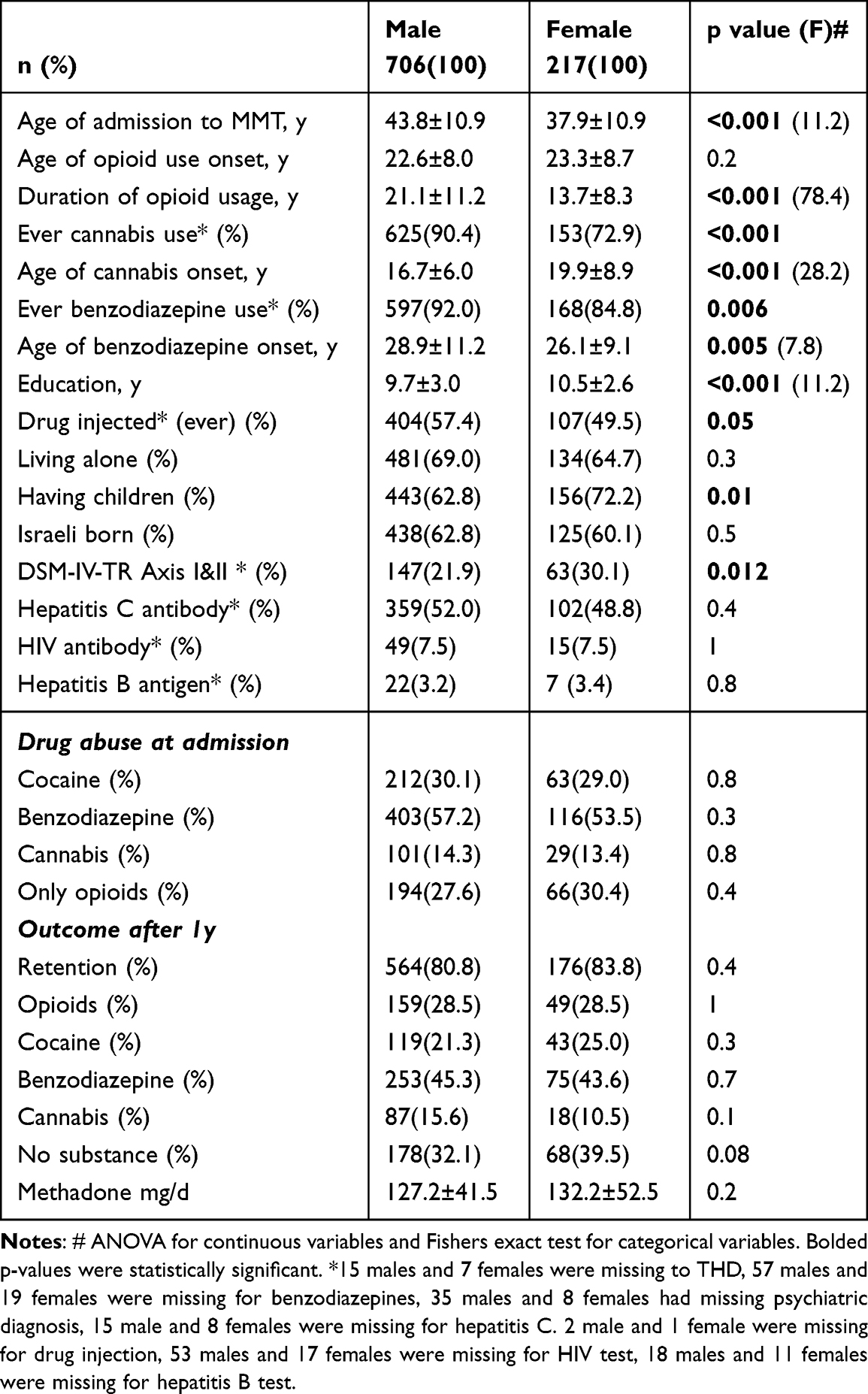 |
Table 1 Comparison Between Sexes |
Trauma Groups Distribution and Sex Differences (Table 2)
Traumas were reported by 687 patients (74.4%) of the cohort. Specifically, traumas occurred prior to substance use in 375 (40.6%) patients and after substance use onset in 537 (58.2%) of the 923-patient cohort. Comparing by 217 females (23.5%) and 706 males (76.5%), the proportion of traumas prior to substance use was higher in females (48.8%) than in male (38.1%, p=0.006) but was comparable between female and male respectively after substance use onset (59% vs. 57.9%, p=0.8).
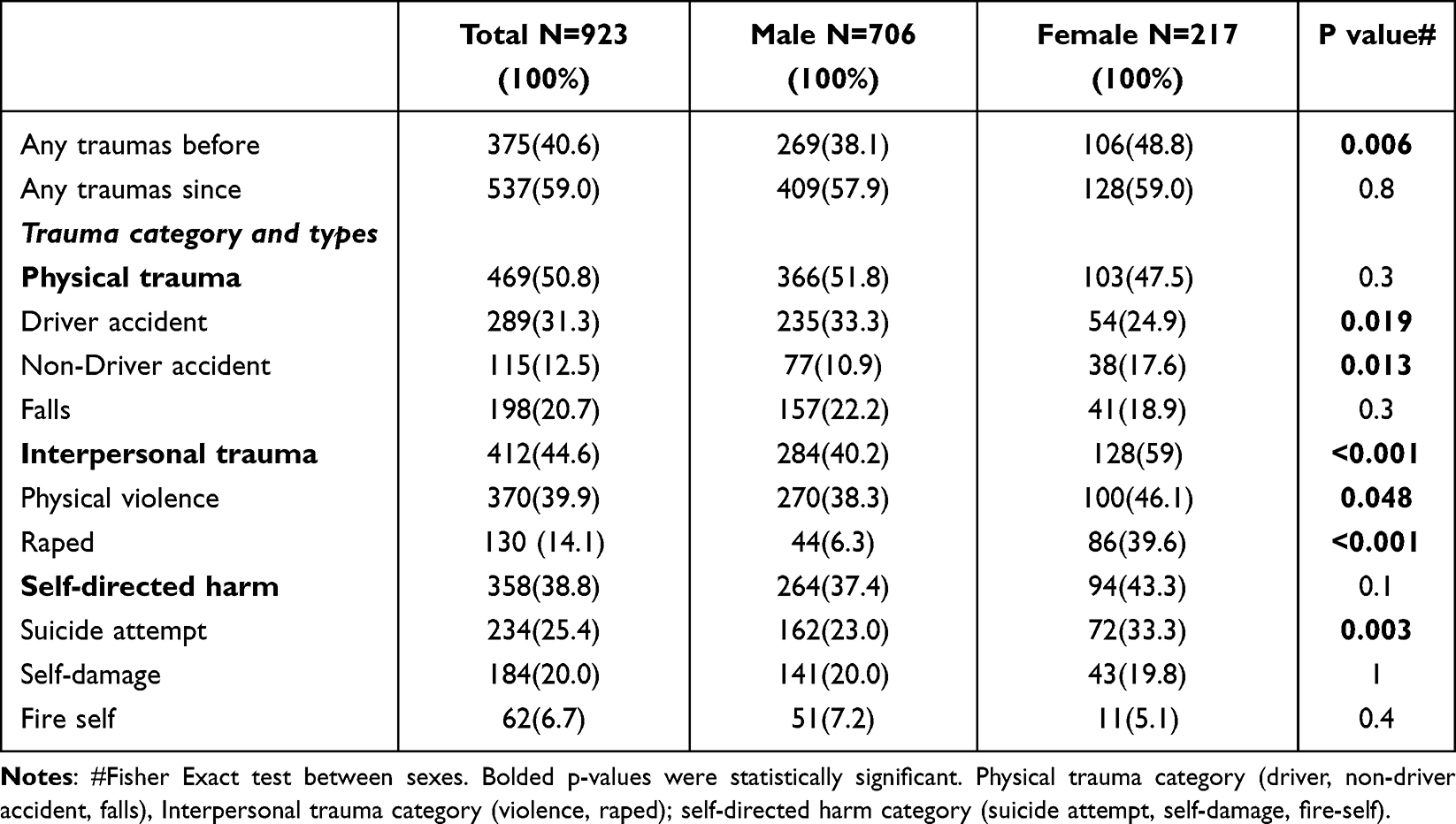 |
Table 2 Trauma Category and Type History Distribution by Sex |
Of the three trauma categories (Table 2), physical trauma (50.8%), interpersonal trauma (44.6%) and self-directed harm (38.8%), only interpersonal trauma was more prevalent among females (59%) than males (40.2%, p<0.001). No significant sex differences were found for self-directed harm (p=0.1) or physical traumas (p=0.3). Overall, types of traumas were primarily physical violence (39.9%) followed by driver accident (31.3%), suicide attempt (25.4%), falls (20.7), self-damage (20.0%), being raped (14.1%), non-driver accident (12.5%) and self-fire (6.7%). Except driver accident that was more prevalent among males (p=0.019), non-driver accident (p=0.013), physical violence (p=0.048), raped (p<0.001), and suicide attempt (p=0.003) were more prevalent among females. The proportion of falls, self-damage, and self-fire did not differ between sexes.
When patients were stratified into three time periods (1993–2002, 2003–2014, 2015–2025), the proportions of physical trauma and interpersonal trauma did not differ significantly across periods or between sexes (data not shown). However, the proportion of self-directed harm differed across time periods. Among females, a decreasing trend was observed (47.7%, 48.1%, and 28.8% respectively; linear by linear association chi square= 3.9, p=0.047). In males, the distribution differed significantly across periods, without linear trend (34.1%, 43.7%, 33.6% respectively, Chi square=6.7, p=0.035).
Characteristics Differences Between 4 Trauma Subgroups (Table 3)
Patients were divided into four groups: patients with no trauma history (25.6%, n=236), patients exposed to trauma only before drug use (16.3%, n=150), patients exposed only during drug use (33.8%, n=312), and patients exposed to traumas both prior to and during substance use (24.4%, n=225). The 4 groups differed by sex distribution, with the highest proportion of males experienced traumas during substance use and the highest proportion of females experienced traumas both before and during substance use (p=0.024). Age of opioid onset (p<0.001), age of cannabis onset (p<0.001) and benzodiazepine onset (p=0.019), were all showed similar pattern of older age of onset by the no traumas or traumas prior to substance use groups, compared with the two other groups of traumas during substance use, either with or without traumas prior to substance use. Shorter duration of opioid usage (p=0.03), older age of admission (p<0.001), shorter proportion of ever drug injection (p<0.001), of fewer psychiatric comorbidity (p=0.008), and shorter proportion of benzodiazepine (p=0.01) and cocaine (p=0.014) were again characterized no traumas and close to prior to substance use traumas as compared to the other two groups whom trauma were exposed during substance use groups.
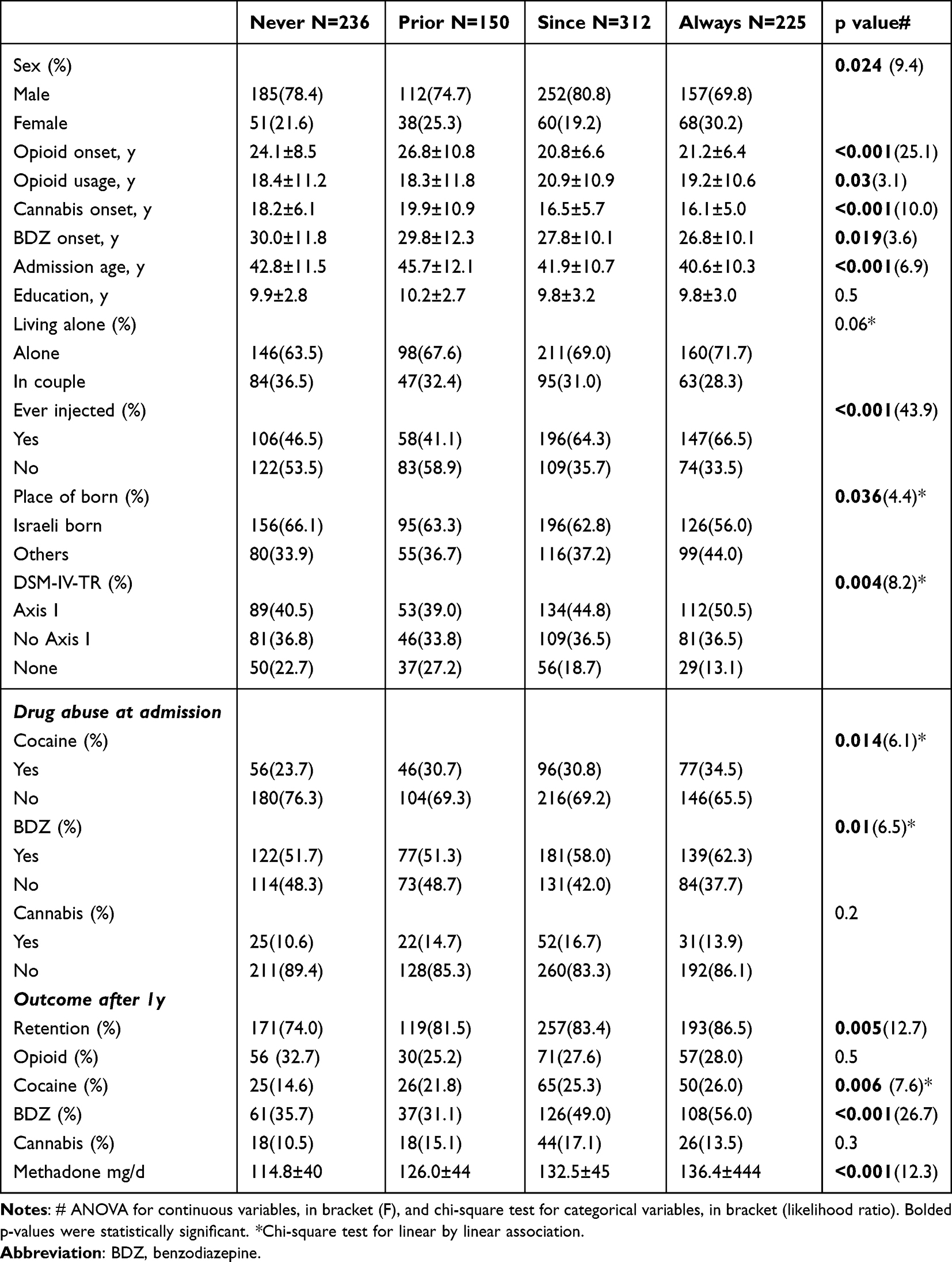 |
Table 3 Comparison of Characteristics by Trauma Group |
Characteristics Differences Between 4 Trauma Subgroups by Sexes (Table 4)
Stratified trauma groups by sex, age of cannabis onset was still significant by trauma and sex, but with interaction effect, reflecting older age of females but not males and no traumas or trauma prior to substance use (Corrected model p(F=11.2)<0.001, Trauma groups p(F=12.8) <0.001; Sex p(F=42.2)<0.001, Interaction p(F3.0)=0.02). Age at opioid onset by timing of trauma and sex showed that trauma groups and sex were related (Corrected model p(F=12.6)<0.001, Trauma groups p(F=21)<0.001; Sex p(F=6.6)=0.01, Interaction p=0.1. Age of admission to MMT by trauma and sex showed that both trauma group and sex were related, with no interaction effect (Corrected model p(F=10)<0.001, Trauma groups p(F=5.2)=0.001; Sex p(F=46)<0.001, Interaction p=0.99). Stratified by sexes, drug injections were significantly related for both male (Chi square 34.7, p<0.001) and female (Chi square 13.3, p=0.004). Benzodiazepine was related to trauma groups by male (Chi square Linear by linear association 4.3, p=0.04) and cocaine by females (Chi square 13.1, p=0.004).
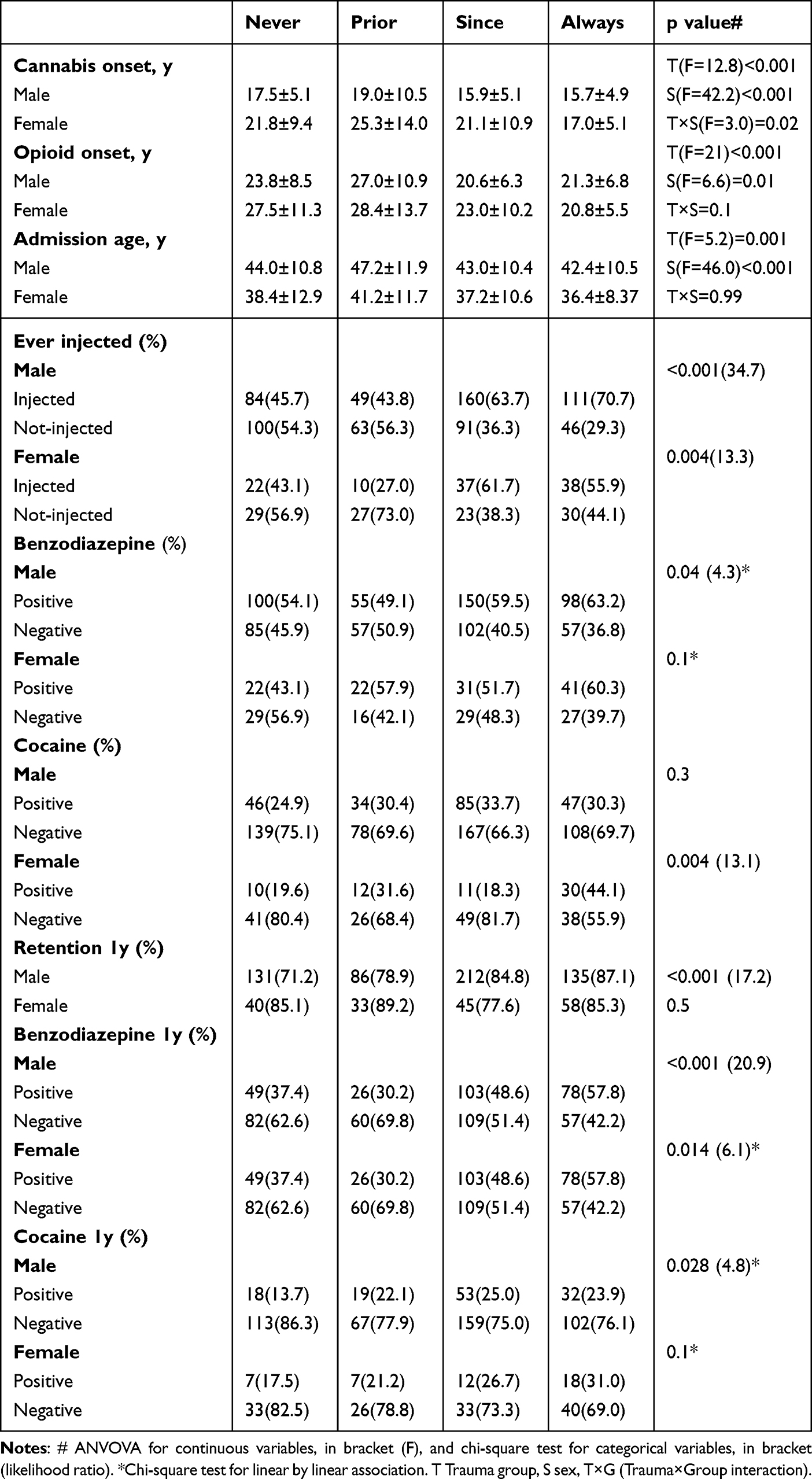 |
Table 4 Comparison of Characteristics by Trauma Group and Sex-Selected Significant Variables |
Outcome - Sex Differences
Outcomes were comparable between females and males. Specifically, one-year retention rates were 83.1% in females and 80.5% in males (p=0.5), and opioid discontinuation after one year was 71.5% in both sexes. After one year, the proportions of cocaine, cannabis, benzodiazepine, and opioid in urine did not differ between the sexes (Table 1). Methadone dose at one year also did not differ between males and females (p=0.2). Cumulative retention was comparable between females and males (10.5 years, 95% CI 9.0–12.0 vs. 9.6 years, 95% CI 8.8–10.5, p=0.3).
Outcome - Trauma Group Differences
Comparing the four trauma groups by one-year retention showed the lowest retention rate (74%) among those with no trauma history and the highest retention rate (86.5%) among those whose traumas occurred before and during substance use (Chi square 12.7, p=0.005) (Table 3). After one year, proportion of patients tested positive to cocaine was lowest (14.6%) among those with no trauma history and highest among those exposed to trauma during substance use, with (26%) or without (25.3%) prior trauma exposure (Chi square linear by linear association 7.6, p=0.006). Benzodiazepine use was also higher in the two groups exposed to trauma during substance use, with (56%) or without (49%) prior trauma exposure (Chi square 26.7, p<0.001). Opioid and cannabis use did not significantly differ between the trauma groups. Cumulative retention of the entire cohort was 9.8 years (95% CI 9.1–10.6), with no difference between the four trauma groups (p=0.3).
Outcome - Trauma Group and Sex Differences
When comparing by sex, one-year retention between trauma time groups showed a similar pattern to that observed in the entire cohort for males (Chi square 17.2, p<0.001), but without a significant difference among females (p=0.5) (Table 4). Similarly, proportions of urine tested positive to benzodiazepine as well as for cocaine after one year were lower in the “never” and higher in the “always” trauma timing groups among males. Among females, only as a trend for significance was observed for cocaine-positive urine tests (Table 4). Cumulative retention showed no significant differences by trauma group or sex, except for a trend toward longer retention among females with prior trauma compared with males (Table 5). When stratified by trauma category and type by sex (Table 6), the cumulative retention was comparable by each of the 3 trauma categories. Lower cumulative retention was found only among males exposed to rape compared with females who were raped (p=0.043, log rank chi square 4.1) and compared with other males (p=0.046, log rank chi square 4.0). Males with a history of self-harm had shorter cumulative retention than males with no history of self-harm (p=0.045, log rank chi square 4.0), and females with a history of self-fire had shorter cumulative retention compared with other females (p=0.005, log rank chi square 7.8) and with males with a history of self-fire (p=0.003, log rank chi square 8.9). Females with any trauma before substance use had longer cumulative retention than those with no traumas before substance use (p=0.035, log rank chi square 4.5).
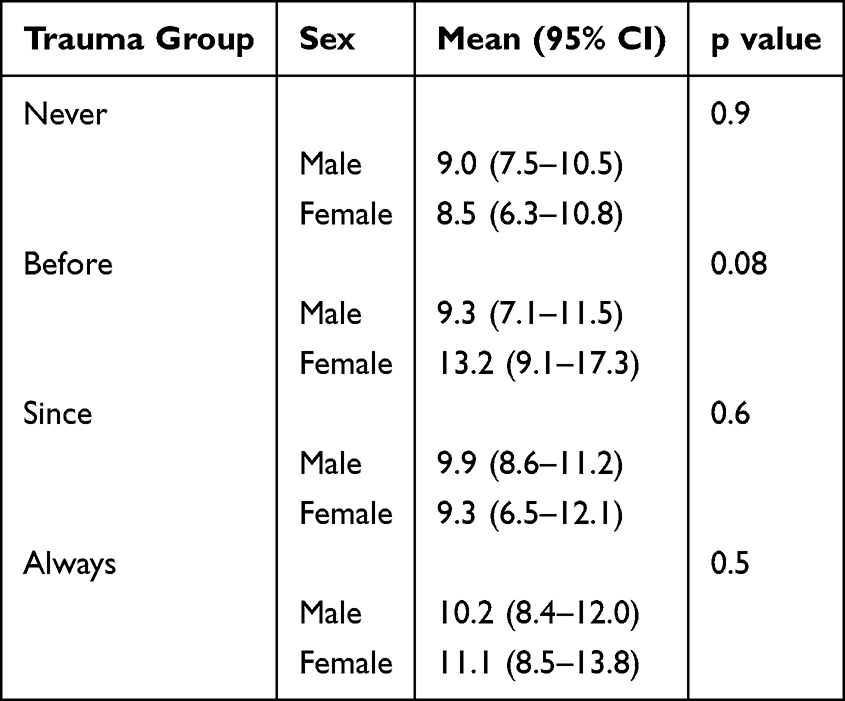 |
Table 5 Means Cumulative Retention Time (Years) by Trauma Timing Groups and Sex |
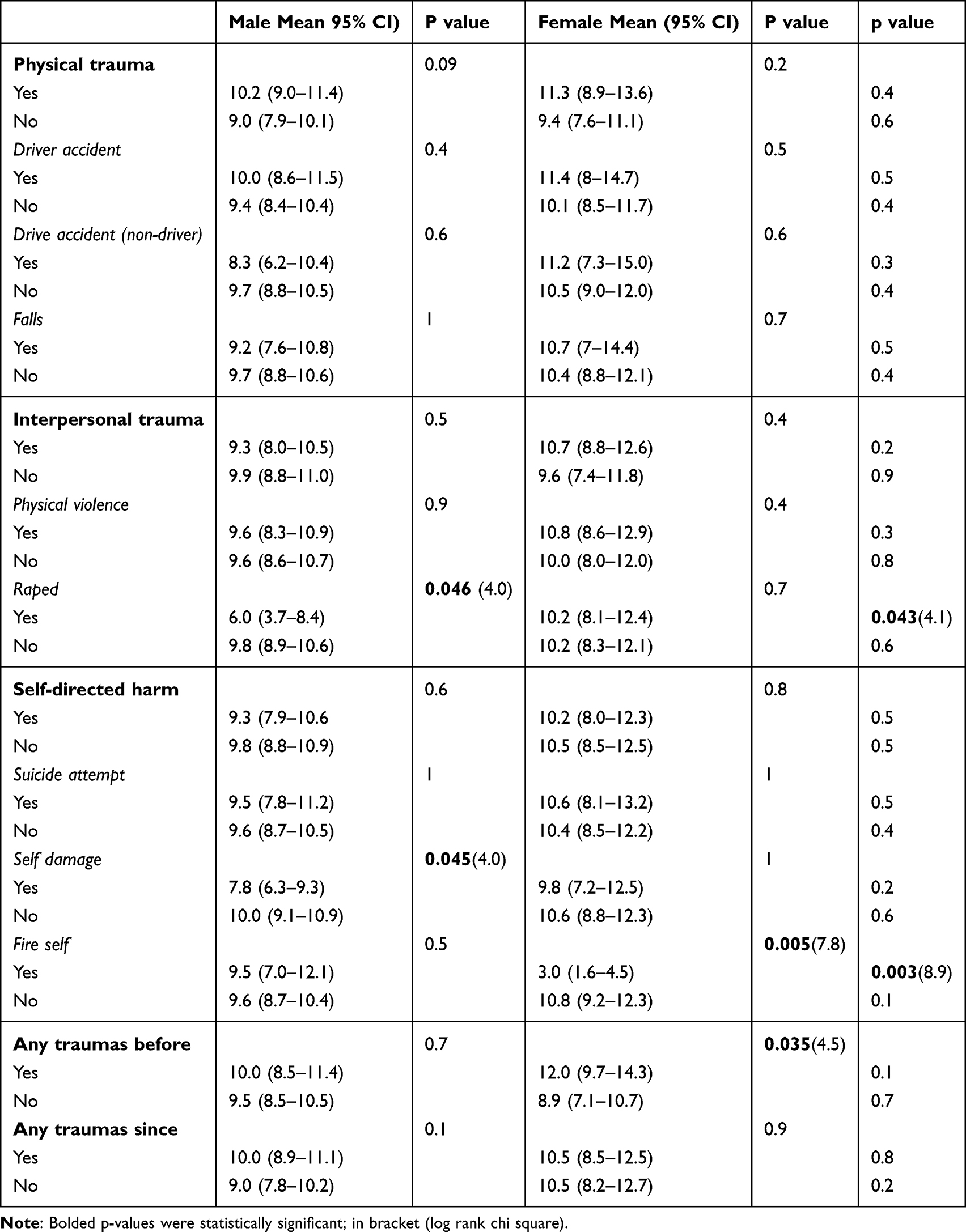 |
Table 6 Cumulative Retention by Trauma Category and Type and Sex |
In a multivariate Cox model among females, a history of self-fire trauma was associated with a higher likelihood of shorter retention (HR=2.7, 95% CI 1.4–5.2, p=0.003), whereas trauma prior to substance use onset was associated with a lower likelihood of shorter retention in MMT (HR=0.7, 95% CI 0.5–0.9, p=0.021).
In a Cox model among males, both self damage (HR=1.2, 95% CI 1.0–1.5, p=0.055), and history of rape (HR=1.4, 95% CI 0.98–2.0, P=0.057) showed a trend toward significance for an association with shorter cumulative retention.
Discussion
The current study aimed to evaluate whether retention in MMT is related to patients’ traumatic experiences, their timing, and whether these associations differ between sexes. We found that approximately two-third of the study cohort experienced trauma, 40% had been exposed to trauma prior to substance use (more commonly females), whereas 60% experienced trauma during substance use. Comparing sexes, most males experienced traumas during substance use, while most females both before and during substance use (“always”). Interpersonal traumas were more prevalent among females, with no difference in self-directed harm and physical trauma.
The “always” trauma group of both sexes started cannabis at a younger age, started opioid use earlier, and entered MMT following a shorter duration of opioid use. They had also a higher proportion of injection drug use, benzodiazepine use at admission, and of cocaine use particularly among females.
With respect to outcome, sexes showed comparable one-year and long-term retention. The traumatic experiences that differed between sexes were not associated with long-term retention and did not alter the comparable treatment outcomes observed between sexes. Male, compared with females, who experienced specific trauma types (rape and self harm) had shorter long-term retention.
Our finding that females were more likely than males experienced trauma prior to substance use, has already been reported by others.5 This may support, although not directly studied, previous literature suggesting that males are more likely to engage in sensation-seeking behaviors, whereas females may use substances for self-medication and pain relief resulting from trauma.16 Interestingly, in a study conducted in mental health facility in Israel, pathological gambling trait was significantly associated with exposure to trauma in men, but not in women.17
Thus, during substance use there were no sex differences in the proportion of patients exposed to trauma. The trauma type that was more prevalent among females than males was interpersonal trauma, which was also most common in females than physical trauma and self-directed harm.
When comparing the four trauma-timing groups (before, “always”, during and “never”), a clear distinction was observed between those exposed to trauma during substance use (regardless of whether exposure also occurred prior to substance use) and those exposed only prior to substance use, whose characteristics were more similar to individuals with no trauma exposure.
Based on the characteristics of those exposed to trauma during substance use, namely, higher rates of cocaine and benzodiazepine use at admission and a greater proportion with a history of injection drugs use - these individuals may have been more likely to experience risky lifestyle involving unsafe environments, violence, and abuse, and therefore greater exposure to traumatic events.
In contrast, individuals exposed to trauma prior to substance use may have initiated opioid use possibly as a form of self-medication, most likely at an older age, but may also have maintained a more stable lifestyle without experiencing a high-risk violent environment, as their characteristics were similar to those of individuals with no trauma exposure. However, our study assessed only retention and substance use outcome. Importantly, a history of physical violence has previously been shown to characterize patients in MMT with anxiety following the October 7th, 2023 Hamas attack on civilians and military personnel in southern Israel.18
Another study related to war exposure in Israel examined whether a large household sample of Israelis was at increased risk for alcohol use disorders following exposure to the 2006 Lebanon War. The study found increased odds of alcohol use disorders in the first year after the war, but only among individuals with a childhood history of maltreatment.19 Moreover, findings following the October 7, 2023 attack examined the relationships between adverse childhood experiences, post-traumatic stress symptoms, and substance use disorder following a large-scale collective trauma in Israel. The authors found that adverse childhood experiences directly predicted increased substance use disorder severity, even after controlling for post-traumatic stress symptoms.20
As our study covered 30 years, changes over time should also be explored. Some changes in patients’ characteristics were recently reported by our group.21 Specifically, over these years, the proportion of females decreased from 27% to 20%, the age of admission rosed from 37 to 43 years, and cocaine misuse increased. One year retention (72.2%) and opioids discontinuation rate after one year (72.3%) showed no significant trend change.21
With respect to traumas proportion and trauma types, no change was observed over time by sex or across trauma categories, except for self-harm, which changed over time and was particularly reduced among females in the most recent latest period. This may reflect a higher proportion of females who developed opioid use disorder following exposure to prescription opioids, whose clinical characteristics differ substantially from those of more typical patients with OUD.22
Looking at outcomes, as consistently shown in our MMT studies,11,12 males and females showed comparable one-year retention as well as long-term retention. When comparing trauma-timing groups, one-year retention was interestingly highest among those exposed to trauma both prior to and during substance use and lowest among those with no trauma history. Although this finding was somewhat unexpected, among those who remained in treatment, a higher proportion of benzodiazepine and cocaine use was again observed in the two groups exposed to trauma during substance use, and lower proportions were observed among those exposed only prior to substance use or with no trauma exposure.
With respect to long-term outcomes, similar cumulative retention was observed across all four trauma groups, with a trend toward longer retention among females with trauma prior to substance use.
Outcome differences by sex were related to a specific trauma type, namely rape, which was also more prevalent among females. While females who reported rape trauma had outcomes comparable to those of non-raped females, males who reported rape had poorer outcomes, with shorter cumulative retention compared with non-raped males and with raped females. Due to small numbers, it was not possible to statistically compare the timing of rape exposure, although most cases of rape in both sexes occurred before and during substance use.
It should also noted that trauma exposure prior to substance use most likely occurred years before initiation of MMT, even though it is hard to explain the similarity of this group to those with no trauma history. One possible explanation is that patients in MMT receive both pharmacological treatment (methadone) and psychosocial therapy, which together may contribute to clinical stabilization. Methadone treatment has been suggested to stabilize physiological functioning, including stress responsivity associated with the hypothalamic–pituitary–adrenal (HPA) axis.23 Therefore, despite complex lifetime trauma histories, many patients may achieve stable rehabilitation.
Moreover, patients with a trauma history may receive additional support from the treatment facility, potentially contributing to the lack of observed outcome differences. It is also possible that the “never” group included individuals who did not self-report traumatic experiences, either because such experiences were not recalled or were not recognized as traumatic. Nevertheless, all participants initiated substance use and developed OUD. In contrast, continued trauma exposure during the years of substance use may better reflect patients’ current circumstances, independent of earlier trauma that may have contributed to substance use initiation.
Of interest, studies comparing patients in MMT exposed to sexual traumas with non-OUD individuals found lower dissociation among MMT patients,24 and other studies also found lower than opioid detoxified patients25,26 and suggest that MMT serve as “protective shield against the painful memories” according to the “chemical dissociation” hypothesis.25,27 Moreover, maintenance treatment with methadone or buprenorphine was reported to be associated with a reduced risk of suicide among individuals with OUD.28,29
Limitation
Trauma exposure and its timing were based on self-reported information, which may be influenced by the patient’s condition, substance use, and recall bias related to the time elapsed since the events occurred. Another limitation is the small number of cases for several trauma types when comparing sexes, resulting in limited statistical power. In addition, patients may have experienced multiple-trauma types, and therefore trauma categories were not mutually exclusive and may have overlapped. The outcome measure, namely retention, included mortality and treatment discontinuation, which may differ across subgroups. Finally, although the findings were derived from a single clinic, one of 13 in Israel, and the only one with CARF accreditation, located within a large (1500-bed) university medical center in Tel Aviv that serves a catchment area of over one million people, the data may limit generalizability.
Conclusions
The traumatic experiences that differed between sexes were not associated with long-term retention and did not alter the comparable outcomes observed between males and females. A larger sample is needed to confirm the findings of shorter cumulative retention among males with a history of rape and to better understand the similarity in characteristics between patients with no trauma history and those exposed to trauma prior to substance use.
Data Sharing Statement
Data availability will be given upon personal request from the corresponding author.
Ethics Statement
The study complies with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Dr. Miriam and Sheldon G. Adelson Foundation for the Biology of Addictive Diseases.
Disclosure
All authors have no conflicts of interest in this work.
References
1. Zhang S, Lin X, Liu J, et al. Prevalence of childhood trauma measured by the short form of the childhood trauma questionnaire in people with substance use disorder: a meta-analysis. Psychiatry Res. 2020;294:113524. doi:10.1016/j.psychres.2020.113524
2. Keyser-Marcus L, Alvanzo A, Rieckmann T, et al. Trauma, gender, and mental health symptoms in individuals with substance use disorders. J Interpers Viol. 2015;30(1):3–13. doi:10.1177/0886260514532523
3. Hughes T, McCabe SE, Wilsnack SC, West BT, Boyd CJ. Victimization and substance use disorders in a national sample of heterosexual and sexual minority women and men. Addiction. 2010;105:2130–2140. doi:10.1111/j.1360-0443.2010.03088.x
4. Rivera EA, Phillips H, Warshaw C, Lyon E, Bland PJ, Kaewken O. An applied research paper on the relationship between intimate partner violence and substance use. National Center on Domestic Violence, Trauma & Mental Health. 2015.
5. McHugh RK, Votaw VR, Sugarman DE, Greenfield SF. Sex and gender differences in substance use disorders. Clin Psychol Rev. 2018;66:12–23. doi:10.1016/j.cpr.2017.10.012
6. Conroy E, Degenhardt L, Mattick RP, Nelson EC. Child maltreatment as a risk factor for opioid dependence: comparison of family characteristics and type and severity of child maltreatment with a matched control group. Child Abuse Negl. 2009;33:343–352. doi:10.1016/j.chiabu.2008.09.009
7. Santo T, Gisev N, Campbell G, Nelson E, Degenhardt L. Drug Alcohol Depend. The effects of childhood trauma and mental disorders on treatment engagement, contact with the criminal justice system, and mortality among people with opioid dependence. Drug Alcohol Depend. 2023;243:109734. doi:10.1016/j.drugalcdep.2022.109734
8. Bawor M, Dennis BB, Bhalerao A, et al. Sex differences in outcomes of methadone maintenance treatment for opioid use disorder: a systematic review and meta-analysis. CMAJ Open. 2015;3:E344–351. doi:10.9778/cmajo.20140089
9. Back SE, Payne RL, Wahlquist AH, et al. Comparative profiles of men and women with opioid dependence: results from a national multisite effectiveness trial. Am J Drug Alcohol Abuse. 2011;37:313–323. doi:10.3109/00952990.2011.596982
10. Soyka M, Zingg C, Koller G, Kuefner H. Retention rate and substance use in methadone and buprenorphine maintenance therapy and predictors of outcome: results from a randomized study. Int J Neuropsychopharmcol. 2008;11:641–653. doi:10.1017/S146114570700836X
11. Adelson M, Linzy S, Peles E. Characteristics and outcome of male and female methadone maintenance patients: MMT in Tel Aviv and Las Vegas. Subst Use Misuse. 2018;53(2):230–238. doi:10.1080/10826084.2017.1298619
12. Peles E, Adelson M. Gender differences and pregnant women in a methadone maintenance treatment (MMT) clinic. J Addict Dis. 2006;25:39–45. doi:10.1300/J069v25n02_06
13. Hser YI, Saxon AJ, Huang D, et al. Treatment retention among patients randomized to buprenorphine/naloxone compared to methadone in a multi-site trial. Addiction. 2014;109:79–87. doi:10.1111/add.12333
14. Ling S, Mangaoil R, Cleverley K, Sproule B, Puts M. A systematic review of sex differences in treatment outcomes among people with opioid use disorder receiving buprenorphine maintenance versus other treatment conditions. Drug Alcohol Depend. 2019;197:168–182. doi:10.1016/j.drugalcdep.2019.02.007
15. Hawks RL. Analytical methodology. NIDA Res Monogr. 1986;73:30–42.
16. Becker JB, Perry AN, Westenbroek C. Sex differences in the neural mechanisms mediating addiction: a new synthesis and hypothesis. Biol Sex Differ. 2012;3(1):14. doi:10.1186/2042-6410-3-14
17. Cohen M, Nakash O, Apter-Levy Y. Gender differences in the relationship between lifetime exposure to trauma and the development of pathological personality traits. J Trauma Dissociation. 2024;25(3):394–407. doi:10.1080/15299732.2024.2320436
18. Sason A, Adelson M, Potik D, Schreiber S, Peles E. Patients’ anxiety levels and their reactions towards the needed adaptation of policies in methadone maintenance treatment following the october 7th, 2023, Hamas Attack. Subst Abuse Rehabil. 2025;16:95–104. doi:10.2147/SAR.S509821
19. Keyes KM, Shmulewitz D, Greenstein E, et al. Exposure to the Lebanon War of 2006 and effects on alcohol use disorders: the moderating role of childhood maltreatment. Drug Alcohol Depend. 2014;134:296–303. doi:10.1016/j.drugalcdep.2013.10.014
20. Levitin MD, Shmulewitz D, Levine E, et al. The unique contributions of adverse childhood experiences to increases in post-traumatic stress symptoms and problematic substance use after trauma exposure. Sci Rep. 2026;16(1):6870. doi:10.1038/s41598-026-37883-3
21. Peles E, Adelson M, Schreiber S. Trends in substance use over 31 years in a large methadone maintenance treatment (MMT) clinic in Israel. J Psychiatr Res. 2025;191:265–270. doi:10.1016/j.jpsychires.2025.09.049
22. Mendelson Z, Sason A, Schreiber S, Adelson M, Peles E. Treatment outcomes in a specialized opioid maintenance program for prescription opioid use disorder in Israel. Subst Abuse Rehabil. 2026;17:584953. doi:10.2147/SAR.S584953
23. Schluger JH, Borg L, Ho A, Kreek MJ. Altered HPA axis responsivity to metyrapone testing in methadone maintained former heroin addicts with ongoing cocaine addiction. Neuropsychopharmacology. 2001;24(5):568–575. doi:10.1016/S0893-133X(00)00222-0
24. Peles E, Adelson M, Seligman Z, Bloch M, Potik D, Schreiber S. Psychiatric comorbidity differences between women with history of childhood sexual abuse who are methadone-maintained former opiate addicts and non-addicts. Psychiatry Res. 2014;219:191–197. doi:10.1016/j.psychres.2014.05.003
25. Somer E, Altus L, Ginzburg K. Dissociative psychopathology among opioid use disorder patients: exploring the “chemical dissociation” hypothesis. Compr Psychiatry. 2010;51:419–425. doi:10.1016/j.comppsych.2009.09.007
26. Peles E, Hacohen S, Sason A, Lamberg S, Schrieber S, Adelson M. Is a history of sexual abuse related to poor sleep among former opioid-addicted women with and without methadone maintenance treatment? Subst Use Misuse. 2017;52:1478–1485. doi:10.1080/10826084.2017.1289224
27. Langeland W, Draijer N, van den Brink W. Trauma and dissociation in treatment-seeking alcoholics: towards a resolution of inconsistent findings. Compr Psychiatry. 2002;43:195–203. doi:10.1053/comp.2002.32350
28. Nielsen S, Larance B, Degenhardt L, Gowing L, Kehler C, Lintzeris N. Opioid agonist treatment for pharmaceutical opioid dependent people. Cochrane Database Syst Rev. 2016;CD011117. doi:10.1002/14651858.CD011117.pub2
29. Santo T Jr, Clark B, Hickman M, et al. Association of opioid agonist treatment with all-cause mortality and specific causes of death among people with opioid dependence: a systematic review and meta-analysis. JAMA Psychiatry. 2021;78:1–15. doi:10.1001/jamapsychiatry.2021.0976
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.