Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Translation, Cultural Adaptation, and Validation of the Arabic Version of the “Readiness to Alter Sun-Protective Behaviour” Questionnaire
Authors Alrodiman YA, AbuDujain NM ![]() , Alajlan A
, Alajlan A ![]() , Alekrish KA
, Alekrish KA ![]() , Borschmann R, Aleisa A, Alghamdi KM
, Borschmann R, Aleisa A, Alghamdi KM
Received 19 April 2026
Accepted for publication 18 June 2026
Published 30 June 2026 Volume 2026:19 618202
DOI https://doi.org/10.2147/CCID.S618202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Monica K. Li
Yazeed A Alrodiman1,*, Nasser M AbuDujain2,*, Alhanoof Alajlan3, Khalid A Alekrish3, Rohan Borschmann4–7, Abdullah Aleisa3, Khalid M Alghamdi3,8
1College of Medicine, Alfaisal University, Riyadh, Saudi Arabia; 2University Family Medicine Center, King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia; 3Department of Dermatology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 4Health Service and Population Research Department, Institute of Psychiatry, Psychology and Neuroscience, King’s College London, London, UK; 5Better Health & Care Hub, King’s College London, London, UK; 6Department of Psychiatry, University of Oxford, Oxford, UK; 7Melbourne School of Psychological Sciences, Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, Melbourne, Australia; 8Vitiligo Research Chair, College of Medicine, King Saud University, Riyadh, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Khalid M Alghamdi, Department of Dermatology, College of Medicine, King Saud University, P.O. Box 240997, Riyadh, 11322, Saudi Arabia, Email [email protected]
Purpose: Ultraviolet radiation exposure is a major risk factor for skin cancer development, and sun protection remains the primary prevention strategy. The Readiness to Alter Sun-Protective Behaviour (RASP-B) questionnaire was developed to assess individuals’ readiness to engage in sun-protective behaviours. This study aimed to translate, culturally adapt, and validate an Arabic version of the RASP-B for use in Arabic-speaking populations.
Patients and Methods: Three independent translators conducted forward translation of the questionnaire into Arabic, followed by back translation by three additional translators. A consensus version was developed after review by the study team, pilot-tested for clarity and acceptability, and shared with the original instrument developer. Participants completed demographic items, the Arabic RASP-B, and the Sun Exposure and Behaviour Inventory (SEBI). Psychometric evaluation included internal consistency, test-retest reliability, construct validity, and convergent validity.
Results: A total of 152 Arabic-speaking participants were enrolled from dermatology clinics at King Saud University Medical City, Riyadh, Saudi Arabia. Most participants were Saudi nationals (97.4%), and 54.6% were female. The Arabic RASP-B showed good internal consistency (Cronbach’s α = 0.81) and test-retest reliability (overall ICC = 0.84; item-level ICC = 0.72– 0.86). The data were suitable for factor analysis (KMO = 0.78; Bartlett’s test: χ 2 = 620, p < 0.001). Exploratory factor analysis identified a three-factor structure corresponding to precontemplation, contemplation, and action stages. RASP-B scores correlated significantly with SEBI behaviours, including shade-seeking (ρ = 0.32), wearing long sleeves (ρ = 0.35), sunscreen use frequency (ρ = 0.26), and intentional tanning (ρ = − 0.31; p < 0.05).
Conclusion: The Arabic RASP-B demonstrated promising preliminary reliability and validity in a single-center dermatology clinic sample. Further multicenter validation, including confirmatory factor analysis, is needed before broader clinical implementation.
Keywords: sun-protection, RASP-B, psychometrics, adaptation, readiness, Arabic
Introduction
Skin cancer is among the most common malignancies worldwide, and excessive ultraviolet (UV) radiation exposure is the primary environmental risk factor driving its development.1–3 UV exposure contributes to melanomas, non-melanoma skin cancers, actinic damage, and photoaging, making sun protection a central component of global cancer-prevention strategies.1–4
Saudi Arabia experiences intense, year-round UV radiation due to its geographic latitude, arid climate, and high annual sunshine levels.5 Although the skin cancer incidence in Saudi Arabia remains lower compared with Western countries, it represents a meaningful proportion of national cancer diagnoses, and registry reports indicate a gradual upward trend.6,7 Contributing factors include outdoor occupational activities, recreational sun exposure, and increasingly Westernized leisure behaviours.5–7 Additionally, recent public awareness studies conducted in Saudi Arabia highlight persisting gaps in sun-protective knowledge and practice, especially among adolescents and young adults.8,9 These findings underscore the need for effective behavioural interventions tailored to local cultural and environmental contexts.
Sun-protective behaviours, including shade-seeking, use of protective clothing, avoidance of midday sun, and sunscreen application, are widely recommended by global health authorities as primary prevention strategies.1,10 However, consistent adoption of these behaviours depends not only on awareness but also on an individual’s readiness to change, emphasizing the importance of behavioural psychology frameworks in prevention programs. The Transtheoretical Model (TTM), proposed by Prochaska and DiClemente, conceptualizes behavioural change as a progression through distinct stages, including precontemplation, contemplation, preparation, action, and maintenance.11 This model has been successfully applied to a range of health-related behaviours, including smoking cessation, alcohol consumption reduction, and sun-protective practices.12–14
Building on the TTM, Borschmann and Cottrell (2009) developed the Readiness to Alter Sun-Protective Behaviour questionnaire (RASP-B), a 12-item instrument designed to categorize individuals into precontemplation, contemplation, or action stages with respect to sun-protective behaviours.15 In its original development, the RASP-B demonstrated a clear three-factor structure, acceptable internal consistency (Cronbach’s α = 0.67–0.76), and strong construct validity based on observed correlations with actual sun-avoidance behaviours.15 Because the tool is brief, theoretically grounded, and psychometrically robust, it is well-suited for clinical, community, and public-health settings.
Despite its utility, the RASP-B has not been translated, culturally adapted, or validated in Arabic, including in Saudi Arabia. This represents a significant gap, as sun-exposure habits, linguistic nuances, sociocultural norms, and environmental conditions differ substantially from the Western settings in which the instrument was originally developed. Without rigorous cross-cultural adaptation, psychometric tools risk losing conceptual equivalence and may fail to accurately measure behavioural constructs. International guidelines recommend that the gold-standard translation of behavioural instruments should include forward translation, back translation, cognitive testing, and full psychometric validation to ensure reliability and construct validity.16
To address this gap, the present study aimed to translate, culturally adapt, and validate an Arabic version of the RASP-B for use in Arabic-speaking populations. Establishing a culturally appropriate Arabic version will support future behavioural research, enable the development of stage-matched interventions, and strengthen national public health strategies aimed at reducing preventable UV-related skin damage across Arabic-speaking populations.
Materials and Methods
Study Design, Participants, and Setting
This quantitative, analytical, cross-sectional study was conducted at the Dermatology Clinics of King Saud University Medical City in Riyadh, Saudi Arabia, between November and December 2025. The study included Arabic-speaking patients aged ≥18 years who were presenting for dermatological care, regardless of diagnosis. Patients who were unable to read or understand Arabic or who declined to participate were excluded from the study. The final sample of 152 participants exceeded the commonly used 10:1 participant-to-item ratio for exploratory factor analysis of the 12-item RASP-B, supporting its adequacy for psychometric validation.
Questionnaire
Participants completed an electronic survey that included basic demographic information (age, sex, and monthly income), the translated Arabic version of the RASP-B to assess their readiness to adopt sun-protective behaviours, and the Arabic Sun Exposure and behaviour Inventory (SEBI) to document patterns of sun exposure and protective practices. Integrating both instruments into a single survey enabled the simultaneous assessment of behavioural readiness and current sun-related behaviours. The original English RASP-B items and the final Arabic translated items are provided in Supplementary Appendix 1.
Instrument Translation Process
The translation and cultural adaptation of the RASP-B were conducted following internationally recognized guidelines for instrument translation.17 First, the questionnaire was forward-translated into Arabic by three professional native Arabic translators fluent in English. The translators had professional linguistic expertise and were not involved in the clinical care of the study participants. Three forward translations (T1, T2, and T3) were reviewed in detail by an independent reviewer and the study authors to compare the translations with each other and with the original RASP-B. Only minor linguistic variations were noted, and a reconciled draft was produced and designated as the initial Arabic version. This version was then back-translated into English by three additional independent translators (BT1, BT2, and BT3), all fluent in both Arabic and English. The back-translated versions were examined side by side and compared with the original RASP-B to evaluate conceptual equivalence. No major discrepancies were identified between the original and the back-translated versions. Following consensus from the reviewers and study team, the pre-final Arabic RASP-B was established.
Psychometric Analysis for Validity and Reliability
The pre-final Arabic version was pilot-tested among six native Arabic-speaking adults to assess clarity, readability, comprehension, and acceptability. Detailed demographic data were not collected during the pilot-testing phase. Participants were asked to identify any items that were unclear, confusing, culturally inappropriate, or potentially ambiguous. Feedback indicated that the items were generally clear, and only minor wording refinements were made to improve comprehension while preserving the original conceptual meaning of the items.
Ethical Considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the Institutional Review Board of the College of Medicine at King Saud University in August 2025 (No. E-25-10038, Ref. No. 25/0585/IRB). All participants reviewed an electronic information sheet outlining the study purpose, procedures, and voluntary nature of participation, and provided informed consent before completing the electronic survey.
Statistical Analyses
Data were analyzed using SPSS v28. No missing item-level data were identified in the final analytic dataset; therefore, no imputation was required. Descriptive statistics (means ± standard deviations [SDs], frequencies, and percentages) summarized participant characteristics and questionnaire responses, following data screening for completeness and suitability for psychometric analysis. The internal consistency of the Arabic RASP-B was assessed using Cronbach’s alpha and corrected item–total correlations using item-deletion analysis to evaluate reliability. Test-retest reliability was examined in a subset of 64 participants who completed the Arabic RASP-B again after a two-week interval. Intraclass correlation coefficients (ICCs) were calculated using a two-way mixed-effects model with absolute agreement. Construct validity was evaluated through exploratory factor analysis after confirming adequacy through the Kaiser–Meyer–Olkin (KMO) and Bartlett’s tests using principal axis factoring and multiple criteria for factor retention. Convergent validity was assessed using Spearman correlation between RASP-B scores and sun protective behaviours. Floor and ceiling effects were considered significant if >15% of the participants scored at extremes. Statistical significance was set at p < 0.05.
Results
Sample Characteristics and Practices
In total, 152 participants were included in the analysis. The mean age of the respondents was 38.6 (SD: 15.1) years. More than half were female (54.6%), and the vast majority were Saudi nationals (97.4%). Most participants reported a monthly personal income between 5,000 and 15,000 SAR (38.2%), corresponding to a lower-to-middle income group. This was followed by those earning < 5,000 SAR (30.9%) (low income group), 15,001–30,000 SAR (23.7%) (upper-to-middle income group), and > 30,000 SAR (7.2%) (high income group) (Table 1).
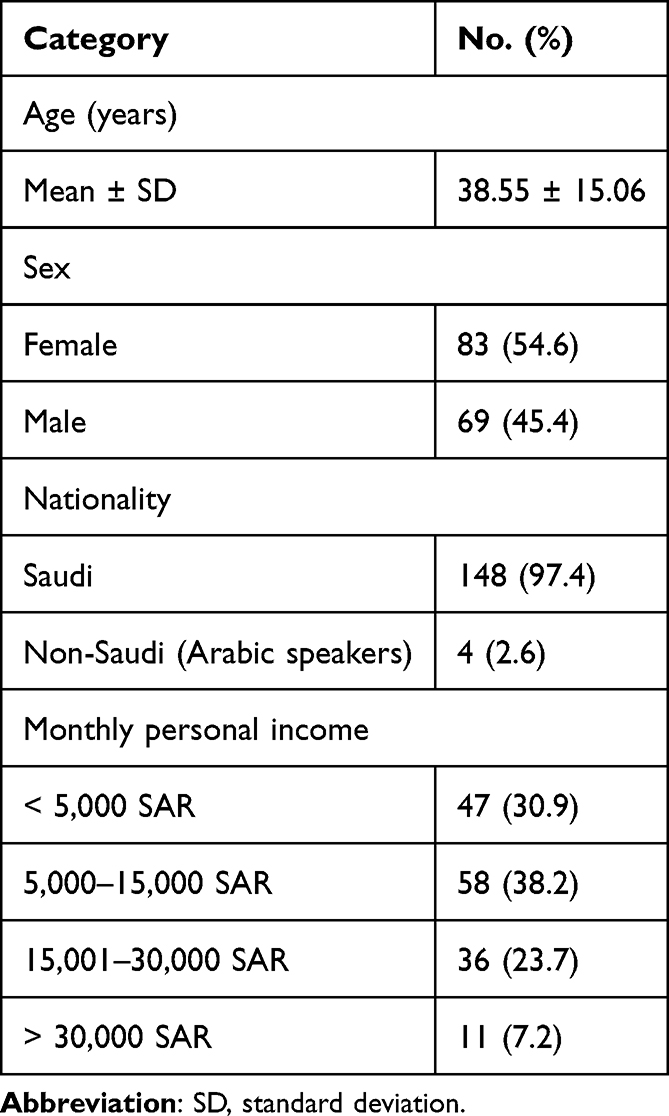 |
Table 1 Sociodemographic Characteristics of Participants (N = 152) |
Sample Adequacy and Preliminary Analysis
A total of 152 participants completed the Arabic version of the RASP-B, meeting and exceeding the recommended sample size criteria for scale validation (≥10 participants per item). The item response distributions showed adequate variability, and no missing item-level data were identified in the final analytic dataset. This dataset was suitable for factor analysis. The KMO measure of sampling adequacy was 0.78, indicating good adequacy. Bartlett’s test of sphericity was statistically significant (χ2 = 620, p < 0.001), confirming sufficient inter-item correlations.
Internal Consistency Reliability
The internal consistency reliability was assessed using Cronbach’s alpha. The Arabic RASP-B showed good overall internal consistency with an alpha coefficient of 0.81. Corrected item-total correlations ranged from 0.42 to 0.67, exceeding the acceptable thresholds. The removal of any individual item did not result in a meaningful improvement in Cronbach’s alpha, supporting the retention of all 12 items (Table 2).
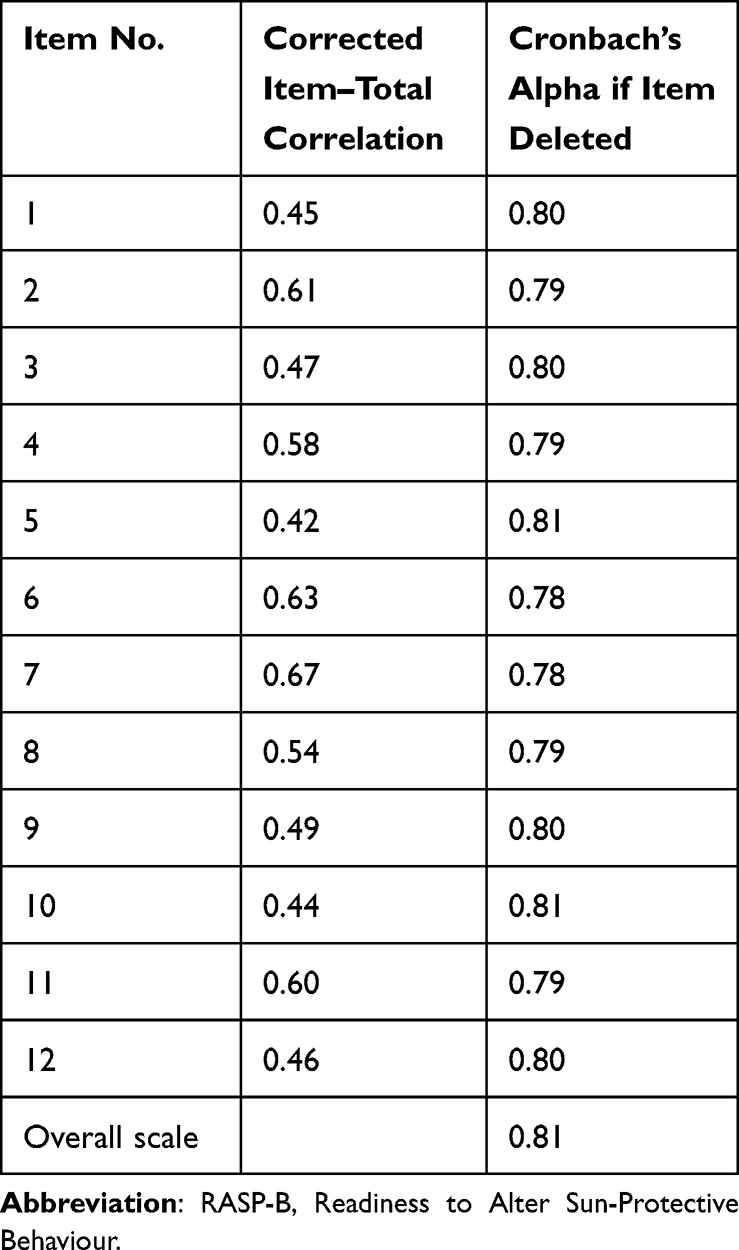 |
Table 2 Internal Consistency Reliability of the Arabic RASP-B |
Test-Retest Reliability
Test-retest reliability was evaluated among 64 participants who completed the Arabic RASP-B twice over a two-week interval. Participants in the test-retest subset were selected from the same dermatology clinic sampling frame and were invited to complete the questionnaire again after two weeks. No study-related sun-protection counseling, educational intervention, or behavioural intervention was provided between the first and second assessments. The Arabic RASP-B demonstrated good temporal stability, with an overall ICC of 0.84 (95% CI: 0.78–0.89). Item-level ICCs ranged from 0.72 to 0.86, indicating stable responses over time (Table 3).
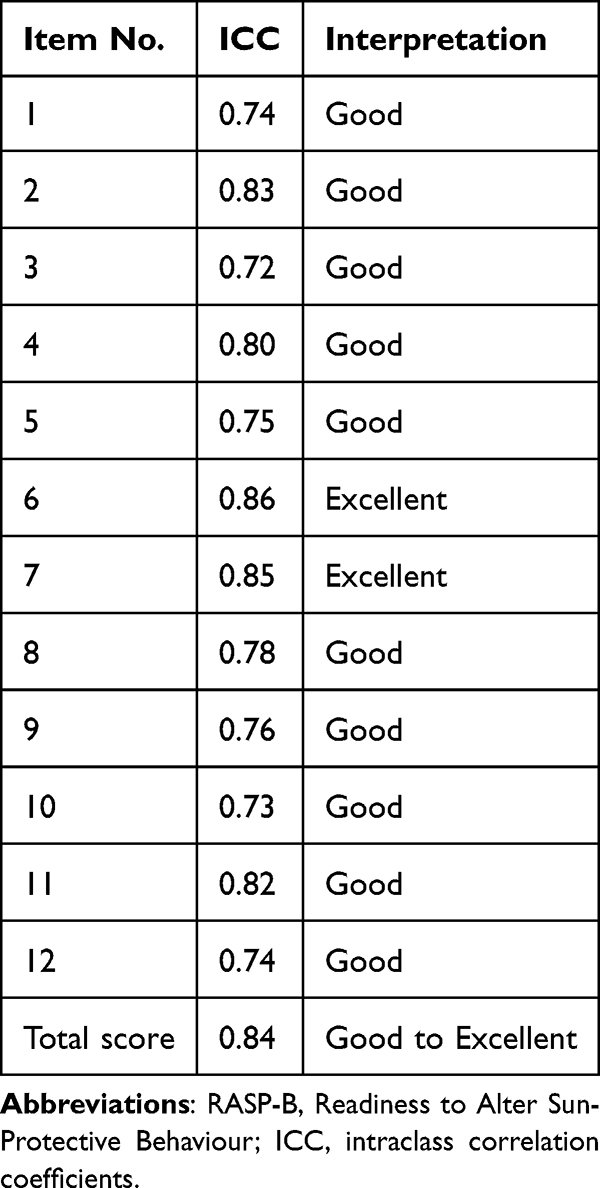 |
Table 3 Test-Retest Reliability of the Arabic RASP-B (2-Week Interval) |
Construct Validity
Exploratory Factor Analysis
Exploratory factor analysis using principal axis factoring with varimax rotation identified a three-factor structure consistent with the theoretical framework of the original RASP-B and the TTM. Eigenvalues >1, along with scree plot inspection, supported this solution. Together, these three factors explained 60% of the total variance, with the precontemplation, contemplation, and action factors explaining 22%, 19%, and 19% of the variance, respectively. Factor loadings were strong, ranging from 0.59 to 0.78, with minimal cross-loadings (Table 4).
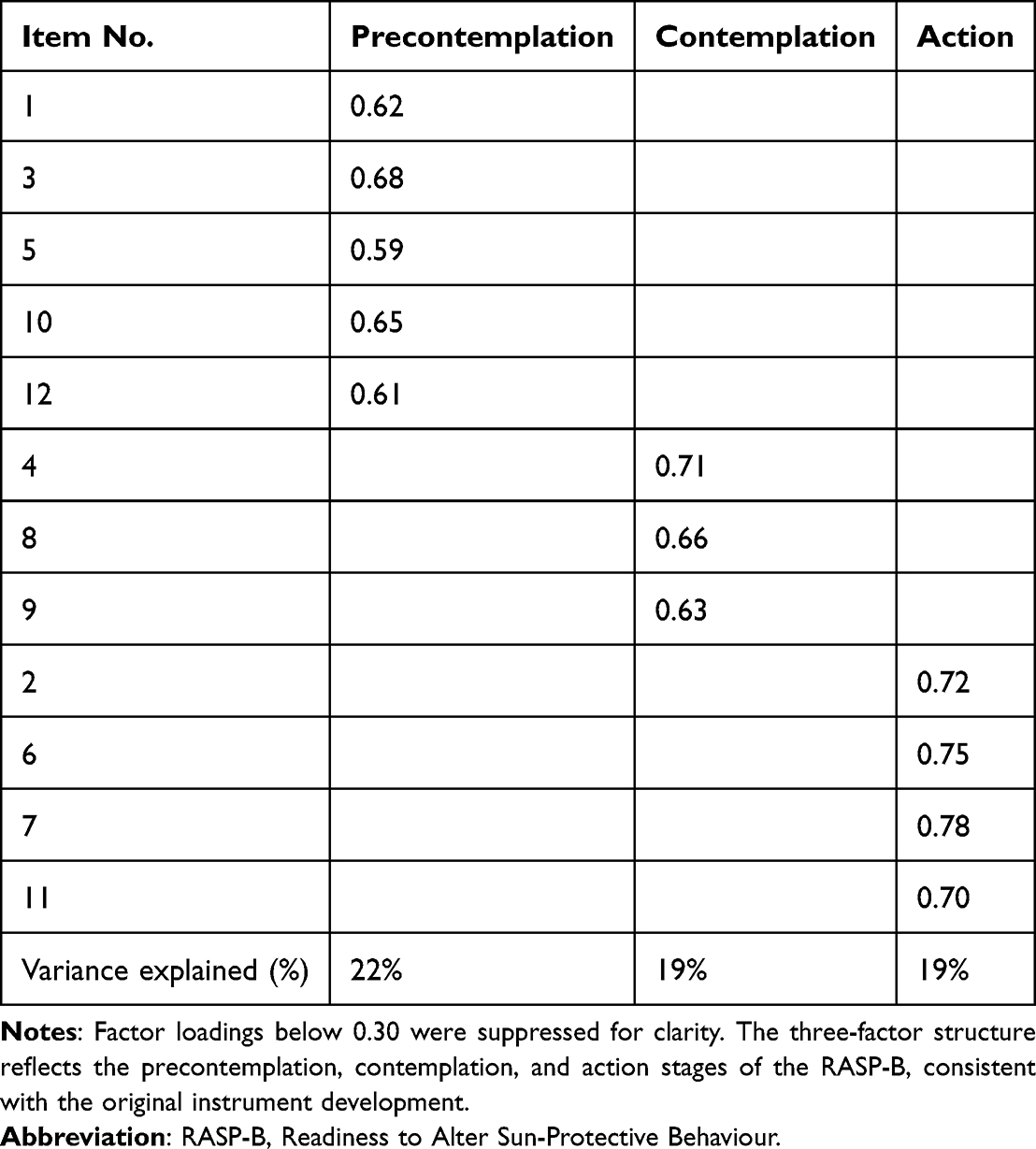 |
Table 4 Exploratory Factor Analysis of the Arabic RASP-B |
Convergent Validity
Convergent validity was supported by correlations between RASP-B scores and self-reported sun protective behaviours. Higher readiness scores were significantly correlated with greater shade-seeking (Spearman’s ρ = 0.32), wearing long sleeves (ρ = 0.35), and sunscreen frequency (ρ = 0.26), and were inversely correlated with intentional tanning (ρ = −0.31), all p < 0.05 (Table 5). These findings support convergent validity.
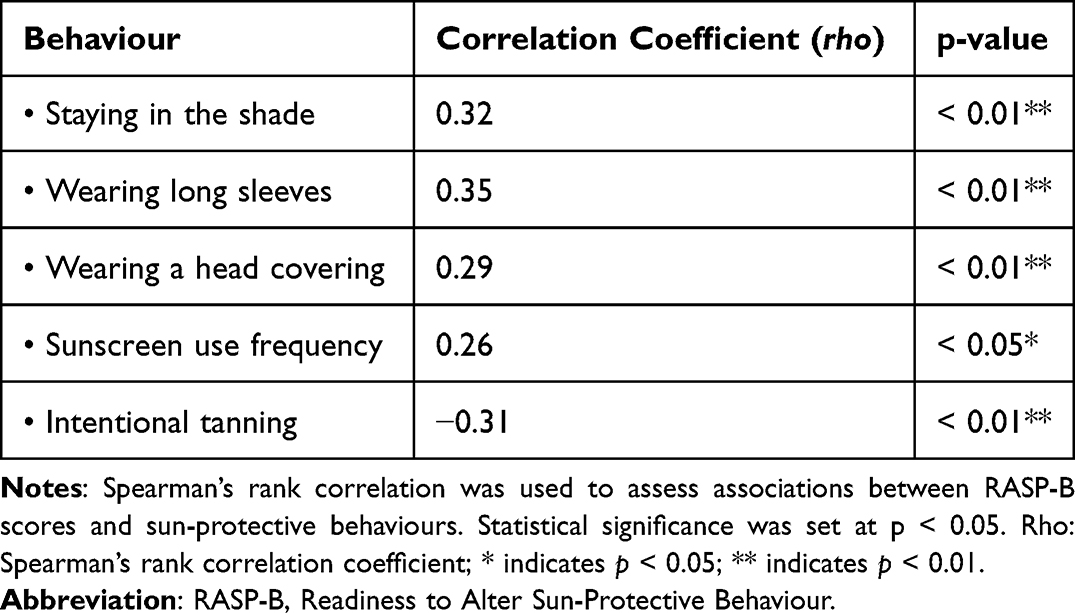 |
Table 5 Correlations Between Arabic RASP-B Scores and Sun-Protective Behaviours |
Floor and Ceiling Effects
No substantial floor or ceiling effects were observed. Less than 15% of the participants achieved the minimum or maximum possible total scores, indicating adequate score dispersion and sensitivity across the readiness stages.
Discussion
In this study, we translated and validated an Arabic version of the RASP-B. The Arabic RASP-B demonstrated good internal consistency (Cronbach’s α = 0.81), good test-retest reliability (ICC = 0.84), significant positive correlations with sun-protective behaviours (Spearman’s ρ = 0.26–0.35), and an inverse association with intentional tanning (ρ = −0.31).
Our exploratory factor analysis results are similar to those of the original RASP-B study, which found a clear three-factor structure that matched the pre-contemplation, contemplation, and action stages of the TTM. The study also concluded that the action stage correlated with better sun protection behaviours. This finding supports the utility of the staging provided by the RASP-B, as each stage corresponds to a specific level of readiness.15
The item loadings were conceptually consistent with the three-stage structure of the original RASP-B. Items loading onto the precontemplation factor reflected limited intention or motivation to adopt sun-protective behaviours, whereas items loading onto the contemplation factor reflected consideration of behavioural change without consistent implementation. Items loading onto the action factor reflected active engagement in sun-protective practices. No items demonstrated loadings that clearly contradicted their intended theoretical stage, supporting the conceptual interpretability of the three-factor solution.
In a cross-sectional Filipino study conducted in 2023, in which 278 adult participants were involved, the findings demonstrated feasibility and internal consistency after a single-translator translation and pretesting, whereas our study included a more rigorous translation methodology with multiple forward and backward translators, as well as broad psychometric evaluation, including test-retest reliability, exploratory factor analysis, and convergent validity.18 Compared to the original English survey in which a subscale Cronbach’s alpha coefficient ranging from 0.67 to 0.76 was reported, the Arabic adaptation reported a 0.81 Cronbach’s alpha coefficient, and an acceptable 0.63 for the Filipino version. However, this comparison should be interpreted cautiously because the original study reported subscale-level reliability, whereas the Filipino and Arabic studies reported full-scale reliability.15,18
The SEBI, a tool which measures current patterns of sun exposure and sun-protective behaviours, has been validated with a Cronbach’s alpha of 0.71–0.84 and acceptable test-retest agreement. This supports the tool being a useful benchmark for sun-behaviour questionnaires.19 Translation of a sun-behaviour assessment tool into Arabic is possible; a Saudi SEBI validation study reported Cronbach’s alpha of 0.61–0.71, correlation coefficients of 0.67–0.72, and a three-factor solution explaining 51.2% of variance.20 Given the prior availability and validation of the Arabic version of the SEBI, we incorporated it as a behavioural comparator, and significant correlations were observed between higher RASP-B scores and greater engagement in SEBI-measured sun-protective behaviours (Table 5).
Although all corrected item-total correlations exceeded the minimum acceptable threshold, items 5 and 10 showed the lowest correlations. This may reflect cultural or contextual differences in how specific sun-protective readiness items are interpreted in Arabic-speaking populations. However, deletion of these items did not improve the overall Cronbach’s alpha, supporting retention of all 12 items in the Arabic version.
Cultural context may also influence responses to sun-protective behaviour items. In Saudi Arabia and other Arabic-speaking settings, traditional clothing and head covering may reduce sun exposure for reasons unrelated to deliberate sun-protection readiness. Therefore, behaviours such as wearing protective clothing may reflect cultural norms, modesty, occupational context, or environmental adaptation rather than a deliberate preventive behaviour. This may partly explain variation in item performance and the observed associations between readiness scores and SEBI-measured behaviours. The observed association between wearing a head covering and RASP-B scores should be interpreted cautiously, as head coverings may be worn primarily for cultural or religious reasons rather than as an intentional sun-protective behaviour. This may increase baseline physical protection independently of an individual’s readiness to change and may affect the interpretation of clothing-related sun-protection measures.
The Sun Exposure and Protection Index (SEPI) is another tool that can be used to assess sun-protection behaviours and provides useful guidance for sun-protection counseling by assessing sun-related behaviours and readiness to increase protection. However, unlike the RASP-B, which is a stage-based readiness instrument, the SEPI measures both the current behaviours and readiness to increase protection.21 A study aimed at validation of the tool demonstrated modest internal consistency with Cronbach’s alpha ranging from 0.57 to 0.69 across two parts and multiple country samples.21
Instead of providing uniform education to all patients, a survey-guided approach may help doctors provide individualized, stage-matched counseling to individuals based on their position on the spectrum of readiness to adopt sun-protection behaviours, as stage-matched interventions have been found to be effective at increasing self-reported sun-protective behaviours.22–24 For instance, a healthcare provider may offer motivational interviewing to a lower-readiness individual, while assisting with maintenance and relapse prevention in cases of high-readiness individuals.24 Such a tailored approach is needed, as a large nationwide study that included more than 11,000 participants found large discrepancies in sun-protection practices between individuals.25
Rigorous translation and recruitment in a dermatology clinic, where sun-protection counseling is directly relevant, are among the strengths of this study. Nonetheless, this study has notable limitations. The cross-sectional design limits the assessment of predictive validity, longitudinal responsiveness, and changes in sun-protective behaviour over time. Additionally, recruitment was conducted at a single dermatology clinic, which may limit the generalizability of the findings to broader Arabic-speaking populations. Patients attending dermatology clinics may have higher skin-health awareness than the general population, which could influence readiness scores and sun-protective behaviour reporting. The predominance of Saudi participants may also limit the generalizability of the findings to Arabic-speaking populations in other countries with different cultural, environmental, and behavioural contexts. Furthermore, convergent validity analysis relied on self-reported sun-protective behaviours, which may be affected by recall bias and social desirability bias. Another limitation is that confirmatory factor analysis was not performed. Therefore, although exploratory factor analysis supported a three-factor structure, future studies should confirm this structure in independent, larger, and multicenter samples.
Conclusion
To the best of our knowledge, this study provides the first Arabic translation and psychometric evaluation of the RASP-B. The Arabic RASP-B demonstrated good internal consistency, temporal stability, and preliminary evidence of construct and convergent validity in a single-center dermatology clinic sample. The tool may help clinicians assess patients’ readiness to adopt sun-protective behaviours and support more individualized counseling. However, further multicenter studies, including confirmatory factor analysis and longitudinal responsiveness testing, are needed before broader clinical implementation.
Data Sharing Statement
Data used in this study are available upon reasonable request from the corresponding author.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of the College of Medicine at King Saud University in August 2025 (No. E-25-10038, Ref. No. 25/0585/IRB). Electronic informed consent was obtained from all participants before participation.
Consent for Publication
All participants gave written informed consent for publication.
Acknowledgments
The authors extend their appreciation to the Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia, for funding through the Ongoing Research Funding Program: Research Chairs (ORF-RC-2025-3906).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Ongoing Research Funding: Research Chairs (ORF-RC-2025-3906), King Saud University, Riyadh, Saudi Arabia.
Disclosure
The authors declare that they have no competing financial interests or personal relationships that may have influenced the work reported in this study. Rohan Borschmann receives salary support from the Better Health & Care Hub at King’s College London, UK.
References
1. Arthey S, Clarke VA. Suntanning and sun protection: a review of the psychological literature. Soc Sci Med. 1995;40(2):265–10. PubMed PMID: 7899938. doi:10.1016/0277-9536(94)e0063-x
2. Kripke ML, Ananthaswamy HN. Carcinogenesis: ultraviolet radiation. In: Freedberg IM, Eisen AZ, Wolff K, editors. Fitzpatrick’s Dermatology in General Medicine.
3. Elwood JM, Jopson J. Melanoma and sun exposure: an overview of published studies. Int J Cancer. 1997;73(2):198–203. PubMed PMID: 9335442. doi:10.1002/(sici)1097-0215(19971009)73:2<198::aid-ijc6>3.0.co;2-r
4. Diffey BL. What is light? Photodermatol Photoimmunol Photomed. 2002;18(2):68–74. PubMed PMID: 12147039. doi:10.1034/j.1600-0781.2002.180203.x
5. Dobbinson S, Wakefield M, Hill D, et al. Children’s sun exposure and sun protection: prevalence in Australia and related parental factors. J Am Acad Dermatol. 2012;66(6):938–947. PubMed PMID: 21890234. doi:10.1016/j.jaad.2011.06.015
6. Saudi Cancer Registry. Cancer Incidence Report Saudi Arabia. Riyadh; 2021; 2018. (Cancer registry report).
7. Linos E, Keiser E, Fu T, Colditz G, Chen S, Tang JY. Hat, shade, long sleeves, or sunscreen? Rethinking US sun protection messages based on their relative effectiveness. Cancer Causes Control. 2011;22(7):1067–1071. PubMed PMID: 21637987, PubMed Central PMCID: PMC3873510. doi:10.1007/s10552-011-9780-1
8. Holman DM, Berkowitz Z, Guy GP, Hawkins NA, Saraiya M, Watson M. Patterns of sunscreen use on the face and other exposed skin among US adults. J Am Acad Dermatol. 2015;73(1):83–92.e1. PubMed PMID: 26002066, PubMed Central PMCID: PMC4475428. doi:10.1016/j.jaad.2015.02.1112
9. Diepgen TL, Mahler V. The epidemiology of skin cancer. Br J Dermatol. 2002;146(suppl 61):1–6. PubMed PMID: 11966724. doi:10.1046/j.1365-2133.146.s61.2.x
10. World Health Organization. Global solar UV index: a practical guide. Geneva; 2002.
11. Prochaska JO, DiClemente CC. Transtheoretical therapy: toward a more integrative model of change. Psychother Theory Res Pract. 1982;19(3):276–288. doi:10.1037/h0088437
12. Kristjánsson S, Helgason AR, Rosdahl I, Holm LE, Ullén H. Readiness to change sun-protective behaviour. Eur J Cancer Prev. 2001;10(3):289–296. PubMed PMID: 11432718. doi:10.1097/00008469-200106000-00014
13. Weinstock MA, Rossi JS, Redding CA, Maddock JE, Cottrill SD. Sun protection behaviors and stages of change for the primary prevention of skin cancers among beachgoers in southeastern New England. Ann Behav Med. 2000;22(4):286–293. PubMed PMID: 11253439. doi:10.1007/BF02895664
14. Rossi JS, Blais LM, Redding CA, Weinstock MA. Preventing skin cancer through behavior change: implications for interventions. Dermatol Clin. 1995;13(3):613–622. PubMed PMID: 7554509. doi:10.1016/S0733-8635(18)30067-6
15. Borschmann RD, Cottrell D. Developing the readiness to alter sun-protective behaviour questionnaire (RASP-B). Cancer Epidemiol. 2009;33(6):451–462. doi:10.1016/j.canep.2009.09.003
16. Gjersing L, Caplehorn JRM, Clausen T. Cross-cultural adaptation of research instruments: language, setting, time and statistical considerations. BMC Med Res Methodol. 2010;10:13. PubMed PMID: 20144247, PubMed Central PMCID: PMC2831007. doi:10.1186/1471-2288-10-13
17. Sousa VD, Rojjanasrirat W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J Eval Clin Pract. 2011;17(2):268–274. PubMed PMID: 20874835. doi:10.1111/j.1365-2753.2010.01434.x
18. Budiman V. A validation study of behaviors towards sun protection among Filipino using Filipino-translated version of Readiness to Alter Sun-Protective Behaviour Questionnaire (RASP-B). J Asian Med Stud Assoc. 2023;10(1). doi:10.52629/jamsa.v10i1.248
19. Jennings L, Karia PS, Jambusaria-Pahlajani A, Whalen FM, Schmults CD. The Sun Exposure and Behaviour Inventory (SEBI): validation of an instrument to assess sun exposure and sun protective practices. J Eur Acad Dermatol Venereol. 2013;27(6):706–715. PubMed PMID: 22487012. doi:10.1111/j.1468-3083.2012.4541.x
20. Aleisa A, Alajlan A, Alrodiman YA, Almuhaideb QA, AbuDujain NM. Development and validation of the sun exposure and behavior inventory in the Arabic language. Dermatol Surg. 2025;51(7):e32–e38. PubMed PMID: 40036269. doi:10.1097/DSS.0000000000004603
21. Detert H, Hedlund S, Anderson CD, et al. Validation of sun exposure and protection index (SEPI) for estimation of sun habits. Cancer Epidemiol. 2015;39(6):986–993. doi:10.1016/j.canep.2015.10.022
22. Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot. 1997;12(1):38–48. PubMed PMID: 10170434. doi:10.4278/0890-1171-12.1.38
23. Weinstock MA, Rossi JS, Redding CA, Maddock JE. Randomized controlled community trial of the efficacy of a multicomponent stage-matched intervention to increase sun protection among beachgoers. Prev Med. 2002;35(6):584–592. PubMed PMID: 12460526. doi:10.1006/pmed.2002.1114
24. A “stages of change” approach to helping patients change behavior. AAFP [Internet]. Available from: https://www.aafp.org/pubs/afp/issues/2000/0301/p1409.html.
25. Aleisa A, AbuDujain NM, Almuhaideb QA, et al. Sun exposure and behaviours in Saudi Arabia: a national study of over eleven thousand participants utilising the Arabic sun exposure and behaviour inventory. Healthcare (Basel). 2025;13(23):3078. doi:10.3390/healthcare13233078
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The 11-Item Weight-Related Behaviours Questionnaire-Short Form (WRB-Q-SF): New Psychometric Evidence for the Arabic Version in Pregnant Women
Al Hage N, Obeid S, Sakr F, Dabbous M, Zaarour P, Hallit S, Fekih-Romdhane F
International Journal of Women's Health 2025, 17:4047-4055
Published Date: 4 November 2025