Back to Journals » Journal of Healthcare Leadership » Volume 17
Transforming Health in Developing Nations: Paving the Way for an Integrated Health System
Authors Pillay P ![]() , Ijoma GN
, Ijoma GN ![]() , Ntwasa M
, Ntwasa M ![]() , Moodley J
, Moodley J ![]()
Received 18 September 2023
Accepted for publication 2 November 2023
Published 14 July 2025 Volume 2025:17 Pages 315—326
DOI https://doi.org/10.2147/JHL.S437070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Preenan Pillay,1,2 Grace Nkechinyere Ijoma,1 Monde Ntwasa,1 Jack Moodley3
1College of Agricultural and Environmental Sciences, University of South Africa, Roodepoort, Gauteng, South Africa; 2Insight, Waterfall City, Gauteng, South Africa; 3Women’s Health and HIV Research Group, Nelson R Mandela School of Medicine, School of Laboratory Medicine and Medical Sciences, University of Kwazulu-Natal, Durban, South Africa
Correspondence: Preenan Pillay, Email [email protected]
Abstract: The World Health Organization (WHO) recognizes the importance of Integrated Health Systems (IHS) in translating health information and its determinants into tangible outcomes. However, effective implementation of an IHS has not been realized due to the lack of a structured Health Information System (HIS) for centralized data analytics and accessibility. This is further exacerbated in developing nations because of the complex interplay between limited resources, inadequate infrastructure, and high disease burden. Therefore, the perspectives presented provide an enhanced engine in the form of a structured HIS to propel the IHS, such that the health system is driven by efficient health data management and analytics. The transformational IHS presented considers resource limitations within the context of the factors influencing political, structural, and economic reforms. This provides an adaptive and progressive approach to address multifaceted health challenges in developing nations. Importantly, the IHS framework presented provides a health system paradigm shift that integrates health practices and their determinants within an artificially intelligent-enabled data-driven architecture to achieve structured and seamless universal health coverage.
Keywords: integrated health system, health information system, digitalization, health artificial intelligence, Enterprise Systems
Introduction
Health systems are defined as activities that primarily promote, restore, and maintain health by considering indirect factors that advocate for improvement.1 These activities are classified as integrated health services that aim to manage the delivery of health services for the continuation of health promotion, disease prevention, diagnosis, treatment, disease management, rehabilitation, and palliative care services across all levels of care.2 However, achieving these goals is challenging because of the fragmentation of modern health systems.3 Therefore, the WHO has formulated a global strategy for the implementation of an integrated people-centered health system to promote Universal Health Coverage (UHC) such that all people have access to quality and affordable health services on demand.4 This strategy provides a high-level perspective that can only be achieved by developing a well-structured integrated health system (IHS) that meets the objectives of UHC.
Global attempts to implement an IHS have been unsuccessful, posing a threat to the global state o health.5,6 This is further exacerbated in developing nations owing to the inherent challenges that reduce health system efficacy. These challenges are caused by a lack of cohesion in digital data derived from health practices, an increase in communicable and non-communicable diseases, a high turnover rate of medical professionals, limitations in health and insurance policies that impede service provision, dispersed health information technology networks, inadequate quality management frameworks, and a limited ability to control population health hazards.7–13 Combined, these challenges inevitably contribute to an increase in health expenditure, which prevents accessibility to quality healthcare14 which is exacerbated in developing nations. Currently, health systems within developing nations are reactionary, as the system of practice is focused on the clinical manifestation of illness, resulting in root cause mismanagement, which stifles the growth and evolution of the health system.15 This polarized system of practice carries inherent hazards and substantial expenses, owing to the absence of accurate medical remedies to avert unfavorable consequences stemming from trial-and-error practices. Therefore, there is a dire need for a paradigm shift in health systems in developing nations that prioritizes meticulous and anticipatory health outcomes in creating a robust system of practice to alleviate stress on the health system and ultimately advance patient health and well-being. To achieve this, a well-structured Health Information System (HIS) architecture is required for the implementation of a coherent IHS that integrates health practices within a socioeconomic context to achieve universal health coverage.
In pursuit of implementing a successful IHS in developing nations, predictive, preventative, personalized, and participatory medicine (PPPPM) emerges as an innovative concept that will prevent the prevalence of communicable and non-communicable diseases.16–18 This concept is the future of medicine and will provide the holy grail to unlocking true health and well-being and achieving UHC; however, it will not be realized within the current state, as it is reliant on the systematic collection, storage, and analysis of accurate health information of individuals throughout their existence. Thus, the success of PPPPM is dependent on an effective IHS that can adapt and evolve to the changing world by systematically providing an advanced matrix, which provides humans with accurate preventative and curative solutions within a multi-layered robust digital architecture built in a setting for human activity. Therefore, building the IHS premised on PPPPM is a holistic approach to achieve total health and well-being in developing nations that would enable the prediction of the disease before onset and the implementation of specific preventative measures and personalized curative methods. To achieve this, there must be a focus on specific outcomes centered on population screening, early prevention, risk identification, stratification for effective treatment, prevention of adverse drug interactions, advanced spatial molecular biology solution markers for enhanced disease modeling, and patient profiling within a socioeconomically viable model. Thus, the perspectives presented in this review critically assess the practical application of PPPPM within a HIS model for the implementation of an IHS designed to address the complex health challenges faced by developing nations.
The Current State
Current progress towards implementing an IHS is slow, and attempts to achieve integrative medicine by combining self-care, traditional complementary medicine with conventional medical practices in Africa and Latin America have not been successful.19,20 This is attributed to the granular approach, as the challenge of implementing an IHS is not merely the theoretical integration of health practices but also the notable disparity between technological applications, health practices, and socioeconomic factors. Therefore, a visible lack of cohesion results in an inefficient method for translating knowledge derived from health-based systems into health outcomes that can be easily managed by healthcare practitioners and patients. It is imperative to realize that, within the context of developing nations, disparities in the implementation of an IHS are exacerbated due to the lack of healthcare funding, shortage of professionals, rapid population growth, insufficient diagnostic capacity, political instability, insecurity, and technological limitations.9,10,21 Thus, in developing nations, there is a critical requirement for a practical IHS that seamlessly translates and integrates valid scientific information into a well-structured HIS. This integration is essential to surmount the barriers prevalent within the contextual influence of the environment and establish widely accepted health practices.
The PPPPM concept has been universally accepted as a promising approach towards generating and applying precise data to improve health outcomes.16 However, the potential of this approach has not been realized due to the large volumes of heterologous data contained within silos, which is further compromised by the limitations of current health systems. To overcome this barrier, PPPPM must be incorporated into a well-structured IHS to improve health equity, patient satisfaction, and overall well-being. This can be achieved by developing a unified IHS with a cohesive HIS strategy towards the classification and management of health data within the PPPPM concept to produce practical predictive models that are intelligible to non-computationally trained clinicians.
Developing an Integrated Health System
Health data remains imperative for evidence-based decision-making and proactive monitoring within all levels of the health system;1 therefore, the WHO recognizes the HIS as a data-centric means to provide valid, translatable, and comparative data for use.2,4 The most commonly used HIS is the open-source District Health Information Management System (DHIS) software program, which is retrofitted into existing structures within many developing nations to collect and transmit information to support clinical decision-making.22 However, the implementation of DHIS and other similar tools does not offer a robust and effective method for disseminating health information for translation into successful health outcomes.23 This is because of its non-systemic architecture, which can accommodate only limited health-related information with insufficient data centralization.24,25 Therefore, a retrofitted approach to HIS implementation cannot determine the analytical potential of the collected health data. This undermines the overall performance of health systems, data producers, and patients in developing countries.
The design and implementation of an IHS within developing nations requires careful consideration, such that the architecture can be built within existing structures to achieve total integration. This strategy must not only focus on the technical elements of the HIS but also on a scale that incorporates all the determinants of the entire system for the efficient translation of data into sustainable health outcomes. To achieve this, a cohesive framework is required to disseminate valid scientific evidence that supports physiological and pathophysiological parameters across a well-structured spatial and temporal model. Moreover, the integration of multifaceted PPPPM-driven analytics of diagnostic, physiological, anthropometric, family history, and lifestyle data within a structured HIS will meet the needs of developing nations and enable the successful implementation of a unified IHS.
The proposed framework (Figure 1) offers a practical and holistic approach for achieving an IHS by amalgamating conventional medicine, complementary therapies, and preventive strategies within a cohesive data structure that considers the physical, mental, emotional, and social dimensions of well-being. This approach does not seek to merely borrow from existing paradigms but rather aims to advance existing health structures in developing countries by providing a unique perspective towards the implementation of a unified IHS. To achieve this, we map out the framework of an advanced HIS that forms the central data bus, which controls and enables the integration and translation of quality health information into health solutions for successful IHS implementation.
 |
Figure 1 Framework for an Integrated Health System: (A) a cohesive structure of all components and determinants of a successful IHS powered by (B) the HIS model aimed at achieving Predictive, Preventative, Personalized, and Participatory medicine (PPPPM). The presented HIS model is stratified within levels of progressive automation which comprise the collection of health data (Primary level), sorting and understanding the data (Secondary level), and translating the data (Tertiary level). |
Paving the Way for an IHS in Developing Nations: Health Information System Integration
Diagnostics is often referred to as the detection and classification of health data for human interpretation to provide definitive information on a patient’s state of health.26 Thus, ensuring the translation of quality data outputs into health outcomes is a critical component of the IHS. Currently, diagnostic and health-related data outputs are not effectively used because of the lack of a structured HIS. This prevents intrinsic discrimination of the accuracy of factors that influence the translation of discrimination across the IHS, thereby providing only an endpoint for diagnosis, which negatively impacts the decisions required to improve overall health and well-being.27 In developing nations, this is further exacerbated to the extent that diagnostic tools are inaccessible to the majority of the population because of the inability to independently measure decision factors for the assessment of the benefits and economics of the diagnostic tool.28–30 This hurdle prevents the effective implementation of diagnostic tools, making them more costly in developing nations, as there is no effective system that allows for efficient transfer, adaptation, automation, and integration into the health system.
Therefore, the HIS framework presented (Figure 1B) provides an advanced diagnostic management solution for developing nations such that there is systematic health management with high accuracy, reduced costs, and minimal human expertise. This framework was progressively modeled towards achieving PPPPM with total cohesion and accuracy for the implementation of an effective IHS. In brief, there are three levels within the HIS presented (Figure 1B): (1) Primary level, centered on the collection of accurate and specific health data. (2) Secondary level: Sorting and understanding data using advanced computational tools and algorithms to create spatial and temporal models. (3) Tertiary level: Making informed health decisions based on modeled data towards enhanced and equitable health. The advanced HIS framework presented will be further expanded in this discourse as systematic models within their stratified levels for the implementation of an IHS in developing nations.
Primary Level
The major hurdle for developing nations is the lack of appropriate data management structures within an already non-cohesive health system.19,23 This is mainly due to the inability to implement appropriate diagnostic tools, considering technological, epidemiological, logistical, and regulatory challenges.19–25 These challenges directly prevent the implementation of an IHS as additional resources are required to overcome these barriers, even before health outcomes within the existing system are realized. This can first be systematically resolved through trans- and inter-governmental policies and agreements that aim to form collaborations to develop diagnostic capacity by removing restraints across borders to effectively reduce costs, gain access to funding mechanisms, and allow intellectual property to be fluid within an agile framework. Within this framework, there must be consideration given to forming a strategy for advancing diagnostic research and development in developing nations, such that there is autonomy in solving specific epidemiological challenges. Practicing scientists and professionals in diagnostics must be supported by accelerated programs in partnership with academia and the industry to develop efficient and cost-effective diagnostic tools for rapid implementation. Within this context, the presented model at the primary level (Figure 2) illustrates the unified data-management framework implemented to ensure that health outcomes are met in developing nations within a cost-conserving structure.
 |
Figure 2 Primary level HIS Model for the unified collection and storage of health data: The model illustrates the systematic flow of data between (A) self-care, conventional and complementary medical practices, and (B) the data model which systematically incorporates the directed diagnostic approach towards Predictive, Preventative, Personalized, and Participatory medicine (PPPPM) such that all the data collected is stored within a regulated unified system for advanced processing. |
Because health practice data within developing nations are disconnected and stored in silos, their quality and translational potential within the existing health system is reduced. Thus, having the most technologically advanced diagnostic tools available in developing nations is irrelevant, as the mismanagement of information from these tools intensifies the demand for resources within an already struggling health system, contributing to its failure and lack of confidence in technology. Therefore, the proposed model provides a data structure for the collection of health practice data for advanced analytics and integration into the health system (Figure 2A) such that PPPPM can be systematically incorporated (Figure 2B). The integration of PPPPM data (Figure 2B) forms an integral component of selecting the most adaptable diagnostic strategy for developing nations within the SMART (Specific, Measurable, Reasonable, and Timely) concept. This will provide a data model for stratification and digitization, with subsequent digitalization of diagnostics for the rapid integration of PPPPM, which has been difficult to realize in many nations.31
Importantly, the primary-level model provides a critical omni-unit system topography for an interconnected database, such that health system information can be processed efficiently. Currently, no universal multiscale data management system exists to achieve the power of scale to potentiate the health diagnostic applications of systems biology in practice for predictive, preventive, personalized, and participatory health applications.31,32 Therefore, the proposed model provides the architectural flow of data for control, storage location, and transmission such that the information can be stored and processed using advanced artificial intelligence (AI) and machine learning (ML) data analytics. Moreover, this model has an integrated component that addresses political, economic, social, technological, legal and environmental (PESTLE) inclusion33 by embedding instructions from universal regulations and policies into a unified data-management architecture.
Secondary Level
Structured data processing is fundamental for the effective implementation of artificial intelligence applications in any system.34 This enables decision process automation by understanding the reason behind a decision to help the system better understand the decision process.35 This data-processing principle within developing nations has not yet been effectively incorporated into the HIS because of the granularity of data collection and storage across an unstructured architecture.
The data processing approach presented (Figure 3), thus, forms the secondary layer of the advanced HIS, which produces diagnostic, predictive, descriptive, and decision models using machine learning, deep learning, and natural language processing. This model provides a system physiological approach to the collection and organization of health data from data collection points at the primary level (Figure 2) within spatial and temporal scales (Figure 3A). This allows the logical ordering of biological data for advanced analytical processing within a pre-programmed data-processing unit (DPU, Figure 3D). The systematic ordering of the biological data will enable the DPU to apply machine learning algorithms to health (Figure 3B) such that the data can be presented within the context of the PPPPM concept using discovery, reporting, optimization, predictive, and statistical analytics (Figure 3C). This will allow the interpretation and agile integration of health data within an IHS in real time, providing healthcare professionals and patients with the information they need to make calculated decisions towards PPPPM.
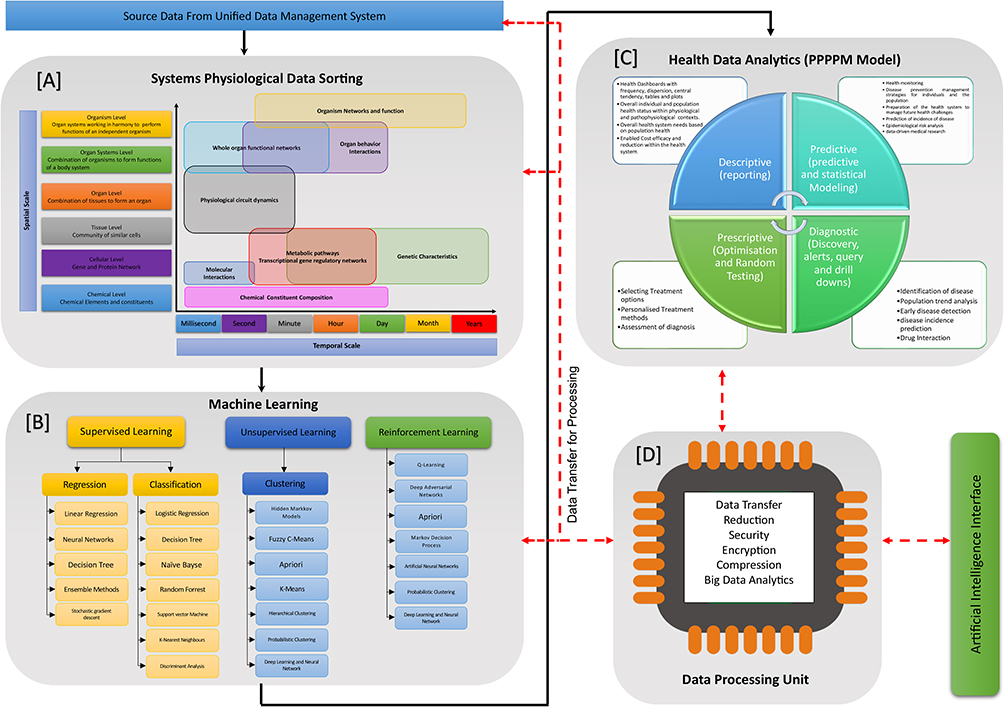 |
Figure 3 Secondary level HIS Model for structured health data analytics: This model illustrates the systematic analytical processing of the stored health data by (A) data sorting across spatial and temporal dimensions, (B) machine learning using statistical algorithms, (C) advanced analytics of the processed information based on the Predictive, Preventative, Personalized, and Participatory medicine (PPPPM) concept within (D) a central data processing unit (DPU) for translation. |
Importantly, the modeled data from the secondary-level HIS directly interfaces with a tertiary-level artificial intelligence architecture to provide advanced health solutions for developing nations. This approach enables the implementation of a robust IHS by reducing resource requirements due to automation, which will in turn lower health expenditure while driving precise health outcomes.
Tertiary Level
Translating health data into clinical utility is a hurdle in healthcare settings because of the poorly structured systems.36 Artificial intelligence in health has emerged as a translation tool; however, its route to implementation is limited because it is currently being applied from a narrow perspective, which creates biases that affect marginalized groups.37 Moreover, this is compounded by dataset shifts caused by changes in technology, population, and behavior.38–40 Thus, the presented IHS approach enables the translation of data into accurate clinical outcomes based on the primary and secondary HIS levels towards a truly PPPPM-propelled IHS. This system overcomes the hurdles in data availability, biased-based models, unbiased preprocessing based on a system’s physiological model, data sharing, and ease of usability by interfacing data analytics with advanced health AI systems.
The structures presented in Levels 1 and 2 form a progressive foundation towards total health systems, which can be efficiently used to create artificial intelligence in healthcare. The tertiary level for propelling the integrated health system is presented in Figure 4, which provides a systematic blueprint for the AI system design within the phases of global technological progression. It must be noted that global nations are currently within the narrow and general artificial intelligence phase, which includes developing nations in which access to hardware, software, and Internet connectivity has revolutionized civilization through cost-efficient integrated mobile devices.41–43 The narrow artificial intelligence model (Figure 4A) integrates AI through machine learning interfaces that apply intelligent thinking algorithms to health data channeled from the DPU and human-interactive data from fuzzy logic models. This will enable the AI processor to create knowledge-based systems that streamline health decision-making, automation of routine and administrative functions, diagnosis, and clinical management strategies across the population spatial scale. This will lead to the creation of user interfaces that form networks for the transfer of knowledge into strategic systems (individuals, healthcare professionals, hospitals, clinics, homes, and self-care) designed to provide advanced integrated health analytics for the human-supervised implementation of PPPPM. In developing nations, this AI model is the most practical, as existing infrastructure and electronic ecosystems can be used with minimal resources. It also allows for progressive growth and expansion towards advancing AI technologies.
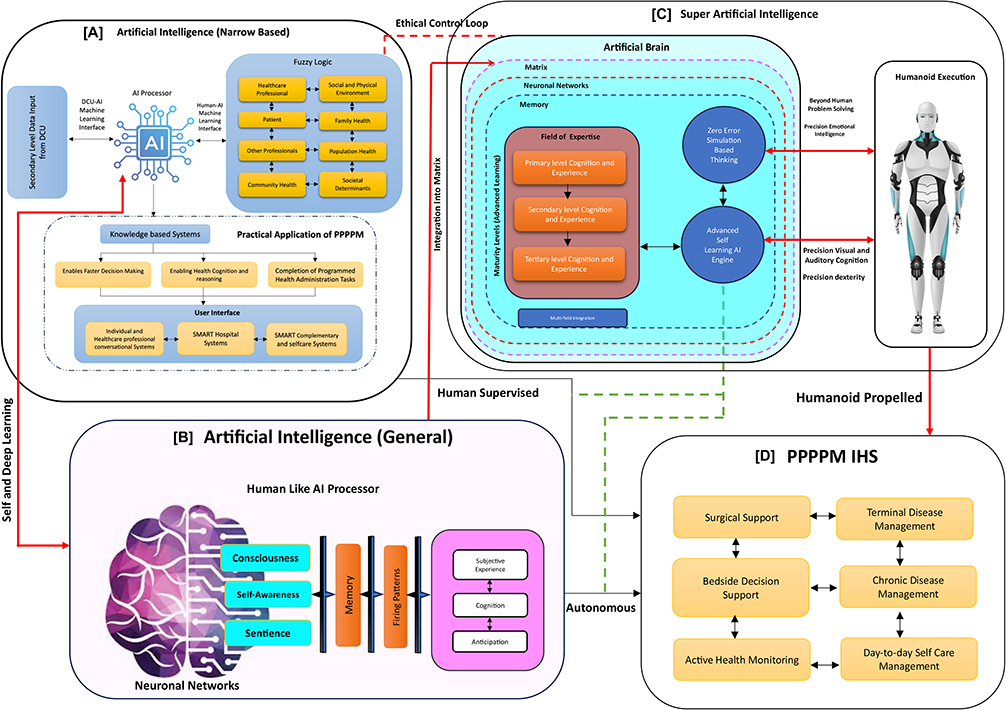 |
Figure 4 Tertiary level HIS Model for structured translation of health data: This model illustrates the use of Artificial Intelligence (AI) and machine learning (ML) to translate the data into practical health outcomes within the (A) narrow AI, (B) general AI and (C) Super AI framework towards achieving (D) an IHS based on the Predictive, Preventative, Personalized, and Participatory medicine (PPPPM) concept. |
General artificial and super-AI are emerging technologies that do not exist at their full potential.44 Importantly, within the health setting, these technologies will not be realized and applied effectively without an integrative health system that is adaptive to technological advancements. The general and advanced AI model presented (Figure 4B and C), therefore, provides a progressive framework for the formation of human-like AI processors that can conduct self- and deep learning within all levels of the system, such that subjective experience, cognition, and anticipation are developed for autonomous interface-led PPPPM applications (Figure 4D). The development of an artificial brain capable of greater human computing power within ethically robust fuzzy-logic mechanisms (Figure 4C) will revolutionize healthcare by enabling a humanoid health workforce built for precision and performance. Within developing nations, this reality may not be realized now; however, the systematic application of the system presented will accelerate civilization towards the final goal of a self-propelled PPPPM towards UHC.
Bringing It Together
The proposed IHS is functionalized through the transversal application of the proposed HIS model, which provides a structural framework for the collection, storage, analysis, and translation of health data within a technologically progressive framework for the developing environment. Moreover, the PPPPM concept is an integral component of the HIS, which forms the primary driver of the transformation towards precision medicine and prevention of illness. The presented IHS aims to offer a holistic approach to achieving total health by accommodating personal and population-driven data that considers mental, emotional, and social dimensions through a universally accepted IHS that unifies outcomes across global PESTLE disparities via a structured HIS.
Importantly, although developing nations do not have a well-established healthcare infrastructure and advanced medical technologies, they have adapted traditional and conventional health practices across a culturally diverse population. These practices aim to cohesively promote early interventions and appropriate self-care practices, which resonate with the PPPPM concept, and thus potentiate the implementation of the proposed IHS towards more resilient, holistic, and sustainable health outcomes.
Implications
Global health expenditure is exponentially increasing annually due to the reactive nature of the current health system. This warrants the need for transformation of the health system to reduce costs and drive operational efficiency whilst assuring quality. This can only be achieved through the systematic integration of information technology within the health ecosystem to streamline processes, provide real-time solutions, efficient communication, and translation of information into health outcomes. The cost-to-benefit value of information technology has been realized across the globe within various industries; however, its impact has not been fully realized within the health sector due to the complexity of the human body and evolving lifestyle needs. This conundrum is exacerbated within developing nations due to the limited resources available, therefore, the presented IHS framework is an all-encompassing strategy, which enables self-propelled health and well-being towards preventing and curing disease within a proactive digital ecosystem. This will, in turn, alleviate the burden on the healthcare system, lower health expenditure, and prevent wastage of resources. Importantly, the agility of the presented IHS framework allows for controlled stratification across diverse nations that will enable scalability within a dynamic network, thereby enabling UHC and translation of data into meaningful health outcomes.
The strategic implementation of the presented IHS will transform global health outcomes towards building nations that are healthy and productive. To achieve this, leaders across the globe will have to prioritize the health and well-being of the people in the absence of commercial or capitalistic bias. This can only be achieved through a revolutionist leadership mindset shift towards the pooling of resources at government level across nations through multi-national agreements and policy reformation strategies. This will accelerate inter-nation knowledge sharing within the structured IHS framework, leading to a stratified value-based health system that is functional within developing nations. The role of government in developing nations is paramount in ensuring that the implementation of an efficient IHS is led by transformative acts, policies, regulations, and procedures that control health priorities of the people and not that of commercial interests within a universal perspective. The legislature of developing nations must protect the people based on the following values and principles within the perspective of the IHS framework presented (Figures 1–4):
- Needs of the nation – Developing nations have dynamic needs within a stratified ecosystem as presented in the framework. Although the challenges encountered across nations differ, they are mainly attributed to high unemployment rates, poverty, and corruption within unseen layers that do not consider the true voice of the nation. Thus, the presented IHS framework allows for the integration of accurate information pertaining to the dynamic individualized needs of the people. This allows for dynamic solutions that not only consider health outcomes but also PESTLE implications, which enable efficient real-time solutions that can be implemented and audited in real-time.
- Economic status of the nation – The disparities in wealth distribution within developing nations are large due to inefficient PESTLE reform. This disadvantages the population at large and prevents access to affordable, quality healthcare. Even though the economic disparity is multifactorial within developing nations, strategies currently in place seek to alleviate poverty but have isolated health. This is a narrow approach as health remains the bedrock of a productive nation and thus cannot be ignored. Therefore, the presented IHS framework allows for the true analytical evaluation of the dynamic economic needs population within the PESLE ecosystem, such that there can be a redistribution and balancing of resources to focused areas of need. Importantly, it allows for balanced pooling of health insurance funds based on the affordability of households within the context of their evolving socio-economic statuses.
- Professional Education – Education is pivotal to ensure the sustainability of health in developing nations. Current curriculum reforms do not consider the need for health transformation and thus are not built for the future, therefore, there is a dire need for the integration of augmented science and technological applications within simulated and actual professional environments as a learning and professional development tool. The presented IHS framework allows for the integration of virtual training by allowing students, interns, and professionals the ability to work with real-time data from the IHS within the classroom and remotely. This will accelerate learning and professional development to deal with current and emerging health challenges. The didactic feedback from educational use will inform the education sector of the gaps for curriculum revisions. Importantly, this process will allow for the emergence of the clinicians of the future who are responsible for precise health and well-being remotely across nations.
- Quality Assurance – Apart from having universally aligned acts and policies within developing nations, they must be systematically applied towards the development of a well-regulated processes for total quality management. Current systems lack rigorous quality assurance measures and thus result in loss of validity and integrity of the information. The presented IHS framework therefore, has been designed in line with the ISO 9001 and 7101 quality management systems guidelines such that universal regulations can be easily adopted by developing nations. This is enabled by the structured multilayered system design, which can process data within a well-regulated AI environment for ease of management and stratification. This will create confidence in the system and enable the effective translation of solutions.
- Active monitoring and control – The role of regulatory bodies in developing nations have the complex task of ensuring conformance to government and international regulations within a fast-evolving local and international environment. Thus, the presented IHS depicts the uni- and bi-directional channels for controlled audit process automation, traceability and accountability such that corrective and preventative actions can be enforced in real-time. This prevents waste of resources and fast-tracks access to affordable, quality health solutions.
- Enhanced Manufacturing capacity – Developing nations comprise dynamic population groups with unique physiological and pathophysiological needs. Thus, retrofitting existing solutions available globally would not offer long-term sustainability for personalized and precise health solutions. The presented IHS allows for the reliable collation of health information across a stratified model, which, when integrated into medical device design, can potentiate its application by providing solutions to specific systems' physiological population dynamics. This will accelerate and empower nationals within developing nations to make informed decisions in the design and scaling of medical devices and services towards increasing local manufacturing capacity.
- Integration of ethics – Developing nations are faced with the complexities of uncontrolled globalization and commercialization, which in many instances result in poor decision-making and corruption due to the lack of governance. The IHS framework presented allows for the systematic integration of ethics into its processes through coherent governance structures that allow for accountability throughout the system. Importantly, universal ethics centralized within the processing engine ensures that the human element remains intact within AI-enabled application of IHS.
- Legal and law enforcement – Developing nations are faced with a growing number of malpractice lawsuits and other related legal challenges, which result in wasteful expenditure. The IHS framework presented allows for total accountability and quality assurance, which will be proactively used to predict possible implications of malpractice, allow for early intervention management, health insurance agencies, professional indemnity agencies. Legal professionals and law enforcement to analyze records for accurate mitigation strategies.
- Community engagement – Current health systems within developing nations have excluded active engagement of the people who are receiving health services. This has resulted in a disconnect between the needs of the people and the progression of the health system towards total health and well-being. Thus, within the digital IHS architecture presented, there are integrations for community feedback, which can be resolved in real-time with full accountability and traceability. Moreover, it allows for continual proactive stratified impact and needs assessment to enable the management of individual and population-specific expectations. Importantly, it allows for the extension of translating system-generated solutions through user-friendly interfaces, which enhance self-propelled participatory medicine.
- Unified Health Insurance – Health insurance remains as means for the population at large to gain access to quality healthcare and is central to achieving health outcomes in developing nations. Therefore, the IHS presented is premised on the PPPPM model as discussed above to ensure access to affordable and efficient health solutions. Inherently, the successful implantation of the presented model will (1) allow for the active management of funds and distribution of premiums within a fair and stratified eco-system based on reliable data analytics and (2) enable inter-nation health insurance modeling to widen access to quality, affordable health for all.
Concluding Remarks
The transformation of health towards total health and well-being in developing nations is dependent on a practical IHS that not only can adapt to global technological advancements but also to the complex political, economic, social, legal, and environmental landscape. Therefore, the presented IHS framework integrates the PPPPM concept for the first time within a stratified and cohesive HIS architecture. The systematic design of the presented system allows for the progressive processing of individualized and stratified health information within a matrix built for agile real-time translation of data into solutions for total health and well-being. Moreover, the presented perspective provides a novel framework to promote transversal research and development collaborations across continents towards the implementation of the presented IHS framework. The framework provides levels within progressive dimensions, which not only allow for efficient data processing but also the integration of core human values, rights, and principles. The integration of AI into the developed IHS framework provides developing nations with advanced health support and analytics within a resource-limited environment, which will transform healthcare, while considering political, structural, and economic reforms, thereby enabling UHC. Importantly, the framework does not promote commercialization of healthcare for capital gain and privatization of health, but rather a solution built for the people based on their specific needs to achieve total health and well-being. It is from this viewpoint that healthcare leaders and professionals shift their mindset towards prioritizing the needs of the people within their specific environments to allow for accessible and equitable health in developing nations. Current work within our research group aims to strategically partner and integrate within the changing ecosystem to potentiate health outcomes and drive affordable and equitable health. This will enable the use of the principles and values above as a compass for navigating the current health landscape in the implementation of the IHS framework presented towards achievingUHC.
Disclosure
Professor Preenan Pillay is the intellectual property owner of this work and is in a partnership agreement with Insight to develop enterprise systems. The authors report no conflicts of interest in this work.
References
1. World Health Organization. Monitoring the building blocks of health systems handbook of indicators and their measurement strategies (2023). Date viewed. Available from: https://apps.who.int/iris/bitstream/handle/10665/258734/9789241564052-eng.pdf.
2. World Health Organization. Integrative Health Services. (2023). Date viewed. Available from: https://www.who.int/teams/integrated-health-services/about.
3. Stange KC. The problem of fragmentation and the need for integrative solutions. Ann Fam Med. 2009;7(2):100–103. doi:10.1370/afm.971
4. World Health Organization. Global strategy on integrated people-centered health services 2016-2026 (2023). Date viewed. Available from: https://www.who.int/teams/integrated-health-services/about.
5. Maruthappu M, Hasan A, Zeltner T. Enablers and barriers in implementing integrated care. Health Syst Reform. 2015;1(4):250–256. doi:10.1080/23288604.2015.1077301
6. Wahls T, Haugen T, Cram P. the continuing problem of missed test results in an integrated health system with an advanced electronic medical record. Joint Comm J Quality Patient Safety. 2007;33(8):485–492. doi:10.1016/S1553-7250(07)33052-3
7. Jackson SF, Perkins F, Khandor E, Cordwell L, Hamann S, Buasai S. & others. Integrated health promotion strategies: a contribution to tackling current and future health challenges. Health Promotion Int. 2006;21(1):75–83. doi:10.1093/heapro/dal054
8. Colombo F, Oderkirk J, Slawomirski L. Health information systems, electronic medical records, and big data in global healthcare. In: Kickbusch I, Ganten D, Moeti M, editors. Handbook of Global Health. Cham: Springer; 2021.
9. Azevedo MJ. The State of Health System(s) in Africa: challenges and Opportunities. Historical Perspectives State of Health Systems Africa. 2017;3:1–73.
10. Koumamba AP, Bisvigou UJ, Ngoungou EB, Diallo G. Health information systems in developing countries: case of African countries. BMC Med Inform Decis Mak. 2021;21:232. doi:10.1186/s12911-021-01597-5
11. Ibeneme S, Karamagi H, Muneene D, Goswami K, Chisaka N, Okeibunor J. Strengthening health systems using innovative digital health technologies in Africa. Front Digit Health. 2022;31:854339. doi:10.3389/fdgth.2022.854339
12. Islam SMS, Purnat TD, Phuong NTA, Mwingira U, Schacht K, Fröschl G. Non‐Communicable Diseases (NCDs) in developing countries: a symposium report. Global Health. 2014;10:81. doi:10.1186/s12992-014-0081-9
13. Boutayeb A. The double burden of communicable and non-communicable diseases in developing countries. Trans R Soc Trop Med Hyg. 2006;100(3):191–199. doi:10.1016/j.trstmh.2005.07.021
14. World Health Organization. Global health expenditure database. global indicators and data. 2023. Available from: https://apps.who.int/nha/database/Select/Indicators/en.
15. Han W. Health care system reforms in developing countries. J Public Health Res. 2012;1(3):199–207. doi:10.4081/jphr.2012.e31
16. Hood L, Flores M. A personal view on systems medicine and the emergence of proactive P4 medicine: predictive, preventive, personalized and participatory. N Biotechnol. 2012;29(6):613–624. doi:10.1016/j.nbt.2012.03.004
17. Khoury MJ, Gwinn ML, Glasgow RE, Kramer BS. A population approach to precision medicine. Am J Prev Med. 2012;42(6):639–645. doi:10.1016/j.amepre.2012.02.012
18. Boffetta P, Collatuzzo G. Application of p4 (predictive, preventive, personalized, participatory) approach to occupational medicine. Med Lav. 2022;113(1):e2022009. doi:10.23749/mdl.v113i1.12622
19. Ampomah IG, Malau-Aduli BS, Malau-Aduli AEO, Emeto TI. Effectiveness of Integrated Health Systems in Africa: a Systematic Review. Medicina. 2020;56(6):271. doi:10.3390/medicina56060271
20. Guido PC, Ribas A, Gaioli M, Quattrone F, Macchi A. The state of the integrative medicine in Latin America: the long road to include complementary, natural, and traditional practices in formal health systems. Eur J Int Med. 2015;7(1):5–12. doi:10.1016/j.eujim.2014.06.010
21. Coovadia H, Jewkes R, Barron P, Sanders D, McIntyre D. The health and health system of South Africa: historical roots of current public health challenges. Lancet. 2009;374:817–834. doi:10.1016/S0140-6736(09)60951-X
22. World Health Organization. Health Information Systems: Toolkit on Monitoring Health Systems Strengthening; 2008. https://www.who.int/publications/m/item/health-information-systems.
23. Sheikh M. Digital Health Information System in Africa’s resource-poor countries: current challenges and Opportunities. J Health Informatics Dev Countries. 2014;8(1).
24. Byrne E, Sæbø JI. Routine use of DHIS2 data: a scoping review. BMC Health Serv Res. 2022;22:1234. doi:10.1186/s12913-022-08598-8
25. World Health Organization. Everybody’s business – strengthening health systems to improve health outcomes: WHO’s framework for action. World Health Organization. 2007.
26. Wurcel V, Cicchetti A, Garrison L. The value of diagnostic information in personalised healthcare: a comprehensive concept to facilitate bringing this technology into healthcare systems. Public Health Genomics. 2019;22(1–2):8–15. doi:10.1159/000501832
27. World Health Organization. Manual for procurement of diagnostics and related laboratory items and equipment. World Health Organization. 2013.
28. Drain PK, Hyle EP, Noubary F. & others. evaluating diagnostic point-of-care tests in resource-limited settings. Lancet Infect Dis. 2015;14:239–249. doi:10.1016/S1473-3099(13)70250-0
29. Pai NP, Vadnais C, Denkinger C, Engel N, Pai M. & others. Point-of-care testing for infectious diseases: diversity, complexity, and barriers in low- and middle-income countries. PLoS Med. 2012;9:e1001306. doi:10.1371/journal.pmed.1001306
30. Peeling RW, Mabey D. Point-of-care tests for diagnosing infections in the developing world. Clin Microbiol Infect. 2010;16:1062–1069. doi:10.1111/j.1469-0691.2010.03279.x
31. Kruk ME, Twum-Danso NAY, Pate M. & others. high-quality health systems in the sustainable development goals era: time for a revolution. Lancet Glob Health. 2018;6(11):e1196–e1252. doi:10.1016/S2214-109X(18)30386-3
32. Cutillo CM. Machine intelligence in healthcare—perspectives on trustworthiness, explainability, usability, and transparency. npj Digit. Med. 2020;3:47.
33. Mantelero A. AI and Big Data: a blueprint for a human rights, social and ethical impact assessment. Comput Law Secur Rev. 2018;34(4):754–772. doi:10.1016/j.clsr.2018.05.017
34. Liang W. Advances, challenges and opportunities in creating data for trustworthy AI. Nat Mach Intell. 2022;4:669–677. doi:10.1038/s42256-022-00516-1
35. Runkler TA. Data Analytics. Wiesbaden, Germany: Springer Vieweg; 2020.
36. Miotto R, Wang F, Wang S, Jiang X, Dudley JT. Deep learning for healthcare: review, opportunities and challenges. Briefings Bioinf. 2018;19(6):1236–1246. doi:10.1093/bib/bbx044
37. Davenport T, Kalakota R. The potential for artificial intelligence in healthcare. Future Healthc J. 2019;6(2):94–98. doi:10.7861/futurehosp.6-2-94
38. Forte P. Data rich, information poor: data, information and decision support in the NHS. Eur J Inf Syst. 1994;3(2):148–154. doi:10.1057/ejis.1994.15
39. Nhampossa JL. The challenge of “translating” health information systems from one developing country context to another: a case study from Mozambique
40. Endriyas M. Factors contributing to poor healthcare data quality: qualitative study from Southern Ethiopia. Health Technol. 2023;13:245–251. doi:10.1007/s12553-023-00741-7
41. Pugliese R, Regondi S, Marini R. Machine learning-based approach: global trends, research directions, and regulatory standpoints. Data Scie Manag. 2021;4:19–29. doi:10.1016/j.dsm.2021.12.002
42. Kopalle PK, Gangwar M, Kaplan A, Ramachandran D, Reinartz W, Rindfleisch A. & Others. Examining artificial intelligence (AI) technologies in marketing via a global lens: current trends and future research opportunities. Int J Res Marketing. 2022;39(2):522–540. doi:10.1016/j.ijresmar.2021.11.002
43. Jiang F. Artificial Intelligence in Healthcare: Past, Present and Future Stroke and Vascular Neurology 2; 2017. doi:10.1136/svn-2017-000101
44. Fjelland R. Why general artificial intelligence will not be realized. Humanit Soc Sci Commun. 2020;7(10). doi:10.1057/s41599-020-0494-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.