Back to Journals » Patient Preference and Adherence » Volume 19
Transcreation and Feasibility of Spanish-Language Pediatric Post-Transplant Adherence App (BMT4me©): Insights from a Community Advisory Board Study
Authors Peek MR ![]() , Olsavsky AL, Franklin BL, Wisne LM, Sezgin E, Beauchemin MP, Skeens MA
, Olsavsky AL, Franklin BL, Wisne LM, Sezgin E, Beauchemin MP, Skeens MA ![]()
Received 19 April 2025
Accepted for publication 19 August 2025
Published 4 October 2025 Volume 2025:19 Pages 3083—3094
DOI https://doi.org/10.2147/PPA.S534983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Madeline R Peek,1 Anna L Olsavsky,1 Bianca L Franklin,1 Lydia M Wisne,1 Emre Sezgin,1,2 Melissa P Beauchemin,3 Micah A Skeens1,2,4
1Center for Biobehavioral Health, Abigail Wexner Research Institute at Nationwide Children’s Hospital, Columbus, OH, USA; 2Department of Pediatrics, Ohio State University, Columbus, OH, USA; 3School of Nursing, Columbia University Medical Center, New York City, NY, USA; 4Division of Pediatric Hematology/Oncology, Nationwide Children’s Hospital, Columbus, OH, USA
Correspondence: Micah A Skeens, Center for Biobehavioral Health, Abigail Wexner Research Institute at Nationwide Children’s Hospital, 700 Children’s Drive, Columbus, OH, 43205, USA, Tel +1 614 722 8550, Email [email protected]
Purpose: Poor medication adherence for children receiving hematopoietic stem cell transplant (HCT) leads to increased risk for infection and fatal complications. Mobile health (mHealth) interventions improve adherence across multiple chronic diseases, yet only 20% of medication apps offer alternative languages. Therefore, it is imperative mHealth interventions are expanded for diverse populations; thus, we aimed to trans-create BMT4me©, an mHealth adherence app, for Spanish-speaking families undergoing HCT.
Patients and Methods: Community Advisory Board focus group members were recruited from Nationwide Children’s Hospital Hispanic employee resource group. Purposive sampling was used to select six interested members (age: M= 38.83 years; SD=9.39) representing diverse backgrounds: Puerto Rican, Peruvian, Venezuelan, Costa Rican, Colombian, and Mexican. Three focus groups were conducted using an iterative app revision process. Upon study completion, members completed the System Usability Scale (SUS) and Reaction Card for app evaluation.
Results: Focus group feedback revealed 4 major qualitative themes: 1) user interface strengths (eg, visuals, legibility); 2) usability improvements (eg, navigation issues, confusing elements); 3) clinical implications (eg, client/provider communication); 4) evaluating content pertinence (eg, socio-cultural appropriateness, comprehension). Notably, members identified mistranslated words and made suggestions to make essential aspects align with Spanish-speaking countries: “There’s not a Spanish word for reset, pero es reiniciar [but it is restart]”.
Conclusion: Overall, the focus groups provided essential feedback regarding visual appeal, usability, clinical relevance, and socio-cultural appropriateness to trans-create the app, leading to an intuitive and useful Spanish version of the mHealth tool. This work underscores the importance of including community partners in transcreation to achieve culturally appropriate digital interventions.
Keywords: hematopoietic stem cell transplant, transcreation, Spanish-speaking, digital interventions
Introduction
Hematopoietic stem cell transplantation (HCT) is a transformative therapy where patients receive healthy stem cells to replace their own diseased or damaged cells.1 This procedure is done for children experiencing a spectrum of malignant (eg, leukemia, sarcoma, and lymphoma) and non-malignant (eg, thalassemia and sickle cell) disorders.1 While transplant holds promise for cure and enhanced quality of life, its success is contingent upon adherence to complex medical regimens, post-transplant care, and consistent follow-up appointments.2 Adherence, in the context of pediatric HCT, extends beyond mere compliance with medication schedules; it encapsulates a comprehensive commitment to multifaceted aspects of care, including infection control measures, dietary restrictions, and rigorous follow-up regimens.2 In pediatric HCT, overall non-adherence rates range from 42% to 75%.2–5 Non-adherence to oral medications has been associated with a higher incidence of infections in children, adversely affecting clinical outcomes.4
Adherence in children is further challenged by language barriers.6–8 Immigrants with limited language proficiency often experience challenges accessing healthcare resources, building effective provider relationships, and learning complex medical terms and protocols.6–8 Additionally, language barriers have been noted to interfere with treatment adherence, subsequently leading to poor health outcomes.6,9 In the US, these challenges are exacerbated among Spanish-speaking families, as Latinos represent the fastest growing minority population. As of 2023, 26% of the United States child population was comprised of Hispanic or Latino children.10 Within the US population, 22.5% of people speak a language other than English at home; more specifically, 13.7% of the US population speak Spanish at home.11 For HCT, limited English proficiency is associated with longer hospitalization and worse clinical outcomes for Spanish-speaking families.12 Moreover, in an integrative review of medication adherence in Latino children, low adherence was widely reported.9 Overall, Spanish-speaking families face significant barriers that affect healthcare access and medication adherence.13 Therefore, enhancing the availability of linguistically and culturally appropriate resources in Spanish is critical to addressing these disparities and improving adherence outcomes.
While more translated resources would increase Spanish-speaking families’ access to healthcare resources, standard translation practices overlook nuanced language, often missing unique vocabulary and idioms used by different Latino subgroups.14 Additionally, translating “word for word” is a common standard practice and often results in a loss of meaning or mistranslation.15 Therefore, a proposed solution to standard translation practices is transcreation: “a translation-related activity that combines processes of linguistic translation and cultural adaptation and re-creation or creative re-interpretation of certain parts of a text”.16 The most endorsed way to facilitate transcreation is through Community Advisory Board (CAB) focus groups: an assembly of community members who advise on a project.17 For specifically Spanish-transcreation, this procedure incorporates the input and recommendations of bilingual native Spanish-speaking research team members and/or community partners into the translation process.14,18 Overall, the structure of CAB focus groups can offer an iterative review of study content and interventions, improve cultural accuracy, assist in maintaining intended meaning, and advise on culturally specific alterations.17,19,20
Taken together, identifying and implementing cross-culturally validated tools that enhance medication adherence are essential for optimizing treatment effectiveness and improving Spanish-speaking patient outcomes. Additionally, the Behavioral Economics Theory posits that low-intensity interventions, such as medication reminders in the context of adherence, can help people make choices that are in their best interest.21 Reminders can be utilized via mobile health (mHealth) interventions, which have shown to be accepted and improve medication adherence in adult,22 pediatric,23,24 and Spanish-speaking chronic illness populations.25 Therefore, the Behavioral Economics Theory was used to create the BMT4me app©, an mHealth tool designed to improve medication adherence in pediatric HCT. The original English BMT4me© app was developed using a user-centered, multiphase iterative process that involved patients, caregivers, and providers.26 The app is fully functional and personalized for managing medications, tracking medications, logging symptoms, and noting side effects (Figure 1). Additionally, the app sends the user pop-up notifications at the scheduled time of the medication dose to ideally improve medication adherence. However, a pilot study evaluating the app27 found one-third of otherwise eligible families were ineligible because they spoke Spanish. Therefore, the aim of this study was to trans-create the mHealth intervention, BMT4me©, into Spanish through an iterative review process involving CAB focus groups to enhance the app’s cultural and linguistic accuracy . Additionally, the study aimed to ensure the app’s content, functionality, and messaging were appropriate, accessible, and relevant for Spanish-speaking families navigating pediatric post-transplant care. Lastly, this work fills the gap in literature that does not address the use of transcreation via CAB focus groups for interventions in the Spanish-speaking pediatric HCT population, and enhances the literature by reiterating the importance of cross-cultural tools in healthcare research.25
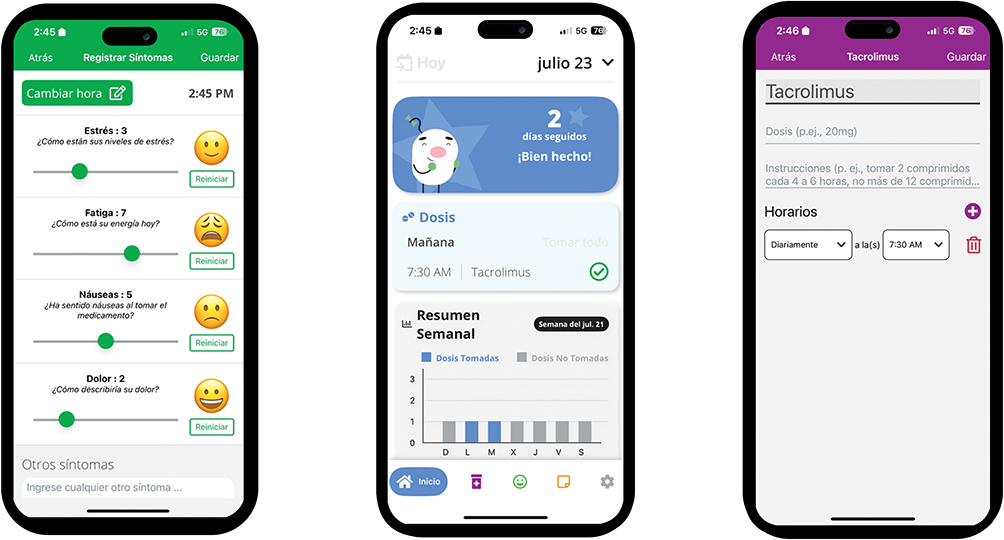 |
Figure 1 The original English BMT4me© app was developed as a personalized tool for managing medications, tracking medications, logging symptoms, and noting side effects in real-time. Medications, doses, and schedules can be put into the app by the user manually or by using the image-to-text feature, which converts the medication label into text. Additionally, the app sends the user pop-up notifications at the scheduled time of the medication dose to remind the user to take or give the medication. The app also records the time the medication was taken and keeps a weekly and monthly log. Symptom ratings are represented by emojis on a slider scale (1 to 10). Additionally, features include a note section to upload pictures and/or record details of care to communicate with the care team. Lastly, the app can be installed on separate devices using the same sign-in code to sync information in real-time for multiple caregivers. |
Materials and Methods
Participant Recruitment
After approval from the Nationwide Children’s Hospital Institutional Review Board (IRB), six Spanish-speaking participants were recruited (see Table 1 for demographic characteristics). Eligible participants (Spanish-speaking community members over the age of 18) were recruited in collaboration with the Hospital’s employee resource group (HOLA ERG), which focuses on supporting Hispanic employees, patients, and community members. A study staff member collaborated with an ERG member to elicit members’ interest in participating. Purposive sampling was used to select members with different backgrounds, including Puerto Rican, Peruvian, Venezuelan, Costa Rican, Columbian, and Mexican. In sum, 11 individuals expressed interest, and there were no declines as the individuals who were selected, agreed to participate (n=6). The same Spanish-speaking participants attended all three meetings.
 |
Table 1 Characteristics of Focus Group Members |
Measures
System Usability Scale
The System Usability Scale (SUS)28 is a 10-item, 5-point Likert scale measure that examined participants’ impression of the app’s functionality and acceptability (eg, “I thought the Spanish BMT4me© app was easy to use; I found the Spanish BMT4me© app unnecessarily complex”). The total scores range from 0 to 100, and scores >68% indicate above average usability.28 Previous literature confirms the validity (r=0.81 with a 7-point, “user-friendliness” scale)29–31 and factor analysis28 verifies acceptable reliability. Additionally, internal consistency (Cronbach α=0.77) was acceptable in this sample.
Reaction Card
The Reaction Card is a part of a toolkit designed by Microsoft to elicit immediate opinions about a specific piece of technology or tool.32 The reaction card listed 55 words, and an endorsement of a word indicated their attitude towards the app (eg, “accessible; complex; easy to use; overwhelming”). Higher frequencies of positive words indicate greater usability and of negative words, lower usability.33 Previous literature and factor analysis33 confirm acceptable reliability and validity.33,34
Procedures
Three community advisory board focus groups were conducted to elicit community perspectives on the content and functionality of the BMT4me© app. The study was conducted at a large, Midwestern, free standing children’s hospital from January 2024 to July 2024. The CAB focus groups were held 3–4 months apart. The focus groups were conducted until the members felt the app was ready for user feedback, which resulted in three focus groups. Consent and demographic information were obtained before the first focus group. After the last focus group, participants completed the SUS and Reaction Card.33,34 Upon study completion, each study participant was compensated with $500 via Clincard. CAB focus groups lasted 60–90 minutes via Microsoft Teams. The focus groups were facilitated by doctorate-level researchers and supported with a bilingual (English and Spanish-speaking) clinical research coordinator (CRC). These focus groups were digitally recorded, transcribed, and double-coded by a bilingual CRC and researchers to ensure accuracy.
Prior to the focus groups, the app was translated by Linguava using a professional linguist to translate the text from English to Spanish. The text was then checked by a second linguist to ensure accuracy, and an English-speaking translator completed a back-translation into English to double-check accuracy. The first CAB focus group reviewed the translated content, and participants were encouraged to comment on the content, tone, and linguistic fidelity of the app’s content. After the first CAB focus group, app recommendations were implemented using Linguava. The second CAB focus group reviewed the changes, and participants were again encouraged to provide feedback. The app prototype was then adapted again using the NCH Research and Information Services Team. Finally, the third CAB focus group assessed the Spanish BMT4me© prototype and participants shared final suggestions and impressions of the app. The complete transcreation process is depicted in Figure 2.
 |
Figure 2 Prior to the focus groups, the app was translated by Linguava using a professional linguist to translate the text from English to Spanish. The text was then checked by a second linguist to ensure accuracy, and an English-speaking translator completed a back-translation into English to double-check accuracy. The first CAB focus group reviewed the translated content, and participants were encouraged to comment on the content, tone, and linguistic fidelity of the app’s content. After the first CAB focus group, app recommendations were implemented using Linguava. The second CAB focus group reviewed the changes, and participants were again encouraged to provide feedback. The app prototype was then adapted again using the NCH Research and Information Services Team. Finally, the third CAB focus group assessed the Spanish BMT4me© prototype and participants shared final suggestions and impressions of the app. |
Data Analysis
Demographic, SUS, and Reaction Card data were analyzed using descriptive statistics. Qualitative data were collected during the focus groups. Initial codes for qualitative analysis of the focus groups were generated from relevant mHealth usability and transcreation literature. Additional codes were added as necessary. The focus group coding was first done separately by two researchers using Excel (Microsoft Corp). A second round of coding was conducted by the researchers together to compare and confirm coding. Once the coding was complete, researchers used an inductive analysis approach to identify recurrent themes across the dataset. Themes were refined through comparison and discussion within the research team to ensure accuracy and depth of interpretation.35–37
Results
Five of the six CAB members had never participated in a CAB before. Four of the six CAB members had used a Spanish app before. On a scale from 1 (extremely uncomfortable) to 10 (extremely comfortable), CAB members highly rated their comfort level using technology (M=9.17; SD=0.98; Median=9.50; IQR 8.00–10.00) and digital health apps (M=8.83; SD=1.17; Median=9.00; IQR 7.75–10.00).
After the CAB focus group meetings were complete, CAB members provided quantitative feedback on the Spanish BMT4me© app. The cumulative SUS score (M=82.5; SD=9.75; Median=83.75; IQR 76.25–90.63) was above average (>68). The most common reaction card endorsements were positive: “Useful” (n=6; 100%), “Accessible” (n=5; 83%), “Valuable” (n=5; 83%), “Collaborative” (n=4; 66%), “Easy” (n=4; 66%), and “Organized” (n=4; 66%). Table 2 presents the full reaction card results.
 |
Table 2 Reaction Card Results From Focus Group Members |
Qualitative Community Advisory Board Feedback
CAB member feedback revealed 4 major themes that were present in all three focus groups: 1) evaluating content pertinence, 2) user interface strengths, 3) usability improvements, and 4) clinical implications. Exemplar quotes highlighting each theme are listed in Table 3.
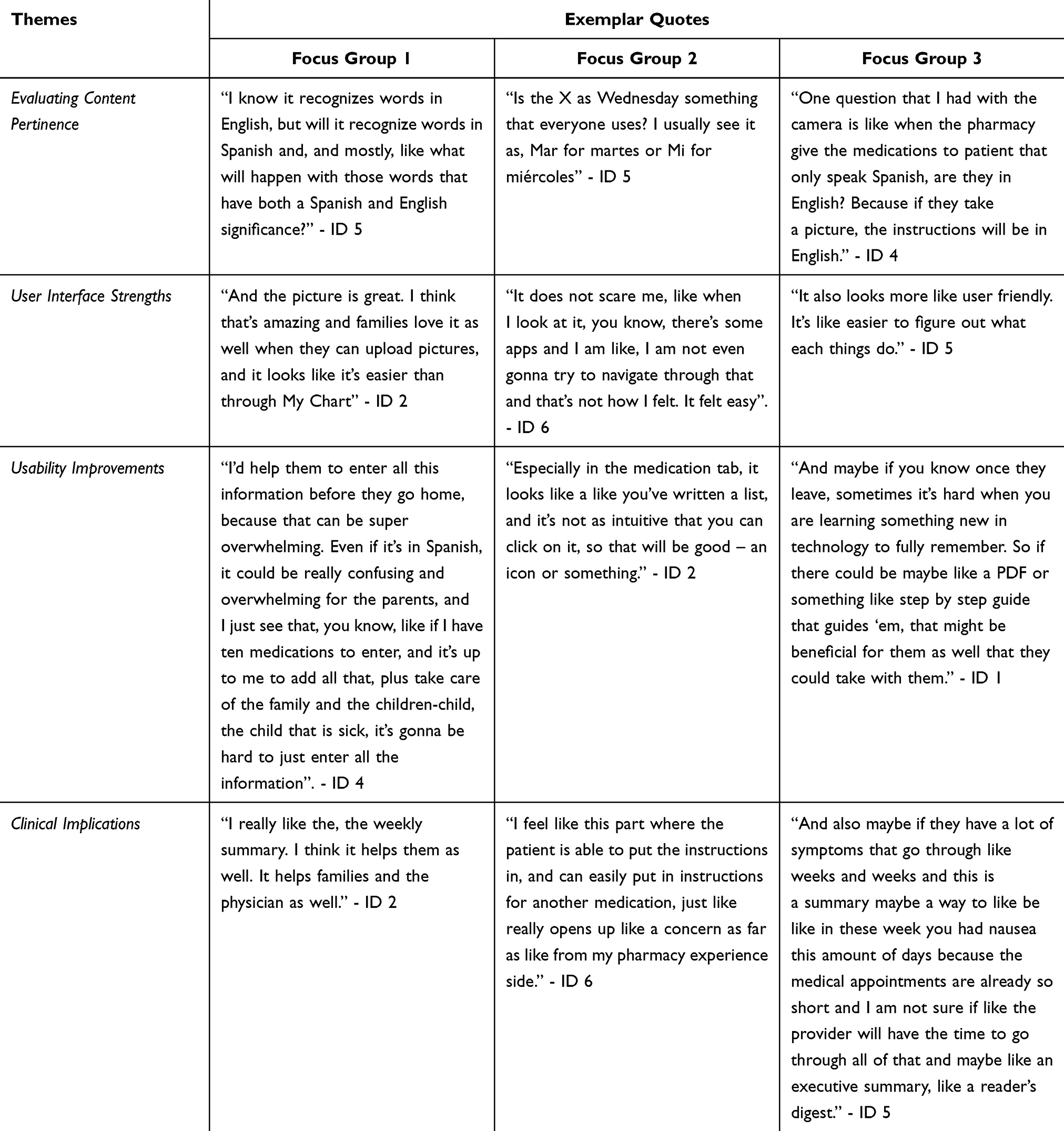 |
Table 3 Primary Qualitative Themes Depicted by Exemplar Quotes From Focus Group Members |
Evaluating Content Pertinence
Across the three focus groups, members addressed the app’s socio-cultural appropriateness, content comprehension, access to information, and non-technical preferences. For instance, members asked about the feasibility of caregivers inputting numerous prescriptions (most of which are in English) into the app, “Does Pharmacy get their things in English and Spanish, or only in English? And if so, could it be possible to get them translated through the app?” (ID 5, CAB 1). Similarly, CAB members expressed concerns related to the app recognizing both English and Spanish, and the outcomes within the app if words have meaning in both English and Spanish (eg, pie means foot in Spanish but is also an English word). They wanted to ensure the app’s software was able to properly make these distinctions and suggested the addition of an embedded translation feature to help with certain translations. Members also identified mistranslated words, for instance, “There’s not a Spanish word for reset, pero es reiniciar [but it is restart]” (ID 2, CAB 2). Moreover, members made suggestions to make essential aspects more aligned with Spanish-speaking countries; for instance, “In Latin America and even in Spain, the dates are the day, the month and then year” (ID 4). Therefore, members suggested changing the format of the dates and times throughout the app to be more easily interpreted by Spanish-speaking individuals. Lastly, members addressed further content-related concerns, such as adding the names of the symptom (nausea or pain) next to the emoticons that are displayed in the symptom section.
User Interface Strengths
Throughout the three focus groups, members brought up the app’s intuitiveness, ease of use, helpfulness, visuals, and legibility. For instance, members felt “the app [was] really user-friendly” (ID 3, CAB 1) and when interacting with the app it seemed “intuitive that you can click and add stuff there” (ID 2, CAB 2). Members also addressed aspects of the app that they found helpful and/or easy to use, such as the weekly summary and ability to upload photos. Additionally, members liked that “there’s the menu bar down there that you can get through the same as clicking. So, there’s a couple options to do the same thing, but it’s very clear and easy to go back to” (ID 2, CAB 2). Furthermore, members gave final approval of the app’s content and visual elements that had been changed based on previous feedback (eg, text boxes and font color: “All of the feedback that we gave before is implemented and even more. I really like it” (ID 4, CAB 3).
Usability Improvements
During all three focus groups, members had suggestions to improve the app’s interface, navigation, technical issues, and confusing elements. For instance, members felt the app would be more visually appealing “if the font was bigger or maybe separate colors all within the white background of everything…like if ‘Medications’ was red, ‘Symptoms’ green and the white font, but the whole button to click would be more colorful” (ID 2, CAB 1). Members also mentioned families might not be tech-savvy because not “everybody has access to the same aspects of technology that you can use with smartphones…we really want to be cognizant of this, the tech knowledge, that, you know, might not be there” (ID 1, CAB 1). Moreover, participants shared how they foresee families having trouble inputting all the medications and suggested a medical team member assists with this task before discharge. Additionally, CAB members mentioned how it could be overwhelming to remember how to use all the app’s features, and they recommended incorporating an FAQ section, a take-home packet, or an in-app PDF guide to alleviate any additional stress. Lastly, members discussed how it was not clear that they could click on a portion of the medication tab and that adding an icon there might make it more intuitive.
Clinical Implications
During the three focus groups, members discussed ways the app could impact provider-patient communication, for instance, “It would be important to add that this is not being seen by the clinical staff because they might be careful with what they add in notes or images” (ID 4, CAB 2). Therefore, members were emphasizing the need for patients to know only the information from the app they want to share with the provider will be shared. Additionally, members brought up the concern that the feature of inputting medication instructions could open the door to patients inputting incorrect directions. They also emphasized that the ease, utility, and relevance of the app should be explicitly emphasized to the patients so when “they use it, they don’t go like, ‘Oh my God, another app’” (ID 2, CAB 2). Lastly, CAB members pointed out that families who do not speak English may not want to call their medical team but rather contact them via Email or messaging. Therefore, providing a way for Spanish-speaking families to virtually communicate with their medical team in a way that is not reliant on speech would be beneficial and help mitigate language barriers.
Discussion
Overall, the CAB focus groups provided essential feedback regarding visual appeal, usability, clinical relevance, and socio-cultural appropriateness to properly trans-create the BMT4me© app into Spanish, leading to an intuitive and useful Spanish mHealth tool. The need for cross-cultural resources, like the BMT4me© app, is supported by the Behavioral Economics Theory, the poor adherence rates and lack of access to healthcare services for the Spanish-speaking population,6,9,13 and acceptance of mHealth interventions in Spanish-speaking chronic illness population.23,25 Additionally, the study aligns with previous literature that outlines the benefit of focus groups for evaluating an mHealth intervention,25,38 as the focus groups with Spanish-speaking CAB members revealed how the app’s content could be socio-culturally and technically improved from a unique and relevant lens. Furthermore, standard translation practices do not consider the nuances of culturally appropriate language,14 yet transcreation does.39 In a scoping review of Spanish language pediatric digital health interventions, 30 interventions were evaluated and only 22 incorporated cultural-tailoring.40 Without the transcreation process, inaccuracies can easily be overlooked and further lead to a family not benefitting from the app; for instance, in our study, CAB members pointed out how dates are formatted differently in most Spanish-speaking countries and that various translations were not universal, accurate, or applicable. Additionally, the iterative process allowed the members to double-check the changes that were made.
Regarding the app’s user interface strengths, the CAB members discussed ways they felt the app was helpful, easy to use, and legible. This positive feedback of the app’s functionality aligns with previous literature as a scoping review examining mHealth apps designed for the Spanish-speaking population explains how multi-modal mHealth interventions that combine reminders with interactive features are most successful.25 Similarly, CAB members provided ways the app could be improved in terms of its navigation, technical issues, and confusing elements. More specifically, as validated by previous literature, focus group members addressed the issue of digital literacy and ensuring members know how to use the application.25 This type of feedback is a necessity as families undergoing HCT face a multitude of stressors that are only exacerbated by limited English proficiency.6 Therefore, it is imperative that BMT4me© and other HCT adherence resources are intuitive and simple, making families’ lives less, not more, burdensome. Transcreation is a proactive means of ensuring the app that families will use is as relevant and usable as possible.
In addition, CAB focus group members discussed the clinical implications of the app and ways it could improve medication adherence and provider-patient communication; these challenges are more pronounced for Spanish-speaking families.6,9,12 However, previous literature has confirmed mHealth reminders improve adherence,25 reiterating the importance of the Spanish BMT4me© app. Furthermore, while CAB focus group members endorsed the app’s strengths, such as its simplicity and embedded photo feature, they also highlighted their concerns about patients inputting many medications into the app during discharge and families forgetting how to use the features of the app. These concerns have been validated by a scoping review that calls upon researchers to provide transparency on how mHealth interventions are introduced and taught to Spanish-speaking families to minimize their burden and increase engagement.25 This socio-culturally relevant feedback on the app’s interface highlights the benefits of transcreation as CAB focus group members confirmed the app’s strengths and suggested improvements. Overall, obtaining recommendations for transcreation of BMT4me©, an app to improve adherence and communicating, was an integral step in addressing the existing health disparities Latino and Hispanic communities in the US face.
In sum, CAB focus group member feedback on the Spanish mHealth app, BMT4me©, further exemplified how transcreation allows for a culturally tailored translation process, as members addressed socio-cultural concerns for various elements of the app. Whether it was a universal translation concern, feedback on the usability and feasibility of the app, or the colors that were used – socio-cultural appropriateness was considered in each focus group. While not all feedback was directly related to the socio-cultural appropriateness of the app, the CAB focus group members’ feedback was given through a culturally relevant lens. Important feedback, such as the changing the formatting of the dates, would have been missed had the transcreation process not been utilized, which underscores the importance of trans-creating an intervention as opposed to using standard translation practices. Thus, findings from this study highlight the significance of transcreation within pediatric HCT. The transcreation of Spanish BMT4me© app contributed to creating more linguistically and culturally appropriate resources for Spanish-speaking families, which is critical in addressing health disparities and improving adherence outcomes. In the last CAB focus group, members positively endorsed the BMT4me© app, which reiterates the strength of the transcreation process and its utilization in future translation research projects. Overall, researchers have been called upon to utilize transcreation in translation studies due to its known positive effects on the community from ensuring researchers are responding directly to the community’s desires and appropriately tailoring the intervention to their needs.18 The results from this study continue to endorse that sentiment.
Limitations
Despite its strengths, this study is not without limitations. Feedback was from community members from 6 different Spanish backgrounds; however, there could have been additional backgrounds represented to provide more diverse feedback. Additionally, all CAB focus group members were educated at a college-level or higher and employees of the same children’s hospital as the study team. While this meant members had above average knowledge of medical and research systems, it is possible it biased our results due to a lack of representation of the breadth of education levels of families using the app. CAB focus group members did not have HCT experience; therefore, content-specific suggestions may have been limited by lack of knowledge of the field. That said, the next phase of the study includes receiving feedback from the population of interest, which will mitigate this limitation as app development continues. The intent was to hold the focus groups one month apart, but technical revisions took longer than a month, which prevented this schedule. Therefore, focus groups occurred between January 2024 and July 2024, which could have resulted in too much time elapsing between focus groups and members misremembering or forgetting topics that were previously discussed. Additionally, the Principal Investigator that created the app led the focus groups, which could have lent itself to CAB focus group members exemplifying greater social desirability bias41 and not sharing their true impressions of the app. Lastly, researchers’ own linguistic/cultural backgrounds could have influenced the app development and content analysis.
Future Directions
As Phase 1 of a broader study, this investigation concentrated on the transcreation of the BMT4me© app and solicited feedback from CAB focus group members to evaluate the usability and acceptability. Phase 2 of the study will continue the transcreation process as it elicits feedback from Spanish-speaking families who have undergone pediatric HCT at two sites. Feedback will continue to inform the development of the app and feasibility of using the app in clinical settings. Additionally, future research can examine the usability and acceptability of BMT4me© in populations beyond pediatric HCT and further examine its ability to enhance patient-provider communication. Lastly, future investigation should consider the clinical outcomes from BMT4me©, specifically medication adherence in Spanish-speaking populations.
Conclusion
This study validates transcreation in place of standard translation processes within the context of pediatric HCT and beyond. The feedback from relevant community members is invaluable and addresses socio-cultural concerns that would not have been addressed otherwise. Additionally, the iterative process ensures the community member voices are adequately illuminated, and feedback is properly integrated for an mHealth application that can improve patient health outcomes. Thus, transcreation should be utilized in research and health care spaces to enhance inclusive clinical care and research methodology.
Abbreviations
SUS, system usability scale; CAB, community advisory board; HCT, hematopoietic stem cell transplant.
Ethics Approval and Informed Consent
All participants consented using the consent process approved by the Nationwide Children’s Hospital Institutional Review Board. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. All participants provided informed consent that included publication of anonymized responses/direct quotes.
Consent for Publication
The authors have seen the details of the manuscript and confirm they can be published.
Acknowledgments
The study team extends heartfelt gratitude to the community members who generously dedicated their time and effort to participate in this study. We also sincerely thank the technology team for their dedication to bringing this product to life. Finally, we acknowledge the National Institutes of Health for their invaluable funding support, which made this work possible.
The protocol for this study was published as a paper in Digital Health in 2025: Transcreating BMT4me: A protocol for adapting an mobile health medication adherence app for Spanish-speaking caregivers in pediatric hematopoietic stem cell transplant – PMC.
Funding
This research was supported by a grant from the National Institute of Minorities and Health Disparities of the National Institutes of Health (R21 MD019075-01). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
The authors have no competing interests to declare for this work.
References
1. Hatzimichael E, Tuthill M. Hematopoietic stem cell transplantation. Stem Cells Cloning. 2010;3:105–117. doi:10.2147/SCCAA.S6815
2. Morrison CF, Martsolf DM, Wehrkamp N, Tehan R, Pai ALH. Medication adherence in hematopoietic stem cell transplantation: a review of the literature. Biol Blood Marrow Transpl. 2017;23(4):562–568. doi:10.1016/j.bbmt.2017.01.008
3. McGrady ME, Williams SN, Davies SM, Pai ALH. Adherence to outpatient oral medication regimens in adolescent hematopoietic stem cell transplant recipients. Eur J Oncol Nurs. 2014;18(2):140–144. doi:10.1016/j.ejon.2013.11.007
4. Pai ALH, Rausch J, Drake S, et al. Poor adherence is associated with more infections after pediatric hematopoietic stem cell transplant. Biol Blood Marrow Transpl. 2018;24(2):381–385. doi:10.1016/j.bbmt.2017.10.033
5. Phipps S, DeCuir-Whalley S. Adherence Issues in Pediatric Bone Marrow Transplantation. J Pediatric Psychol. 1990;15(4):459–475. doi:10.1093/jpepsy/15.4.459
6. Pandey M, Maina RG, Amoyaw J, et al. Impacts of English language proficiency on healthcare access, use, and outcomes among immigrants: a qualitative study. BMC Health Services Res. 2021;21(1):741. doi:10.1186/s12913-021-06750-4
7. Klassen AF, Gulati S, watt L, et al. Immigrant to Canada, newcomer to childhood cancer: a qualitative study of challenges faced by immigrant parents. Psychooncology. 2012;21(5):558–562. doi:10.1002/pon.1963
8. Stewart MJ, Neufeld A, Harrison MJ, Spitzer D, Hughes K, Makwarimba E. Immigrant women family caregivers in Canada: implications for policies and programmes in health and social sectors. Health Soc Care Commun. 2006;14(4):329–340. doi:10.1111/j.1365-2524.2006.00627.x
9. Foronda CL, Muheriwa SR, Fernandez-Burgos M, Prather S, Nersesian P. Hispanic Health Care InternationalVolume 18, Issue 4. Natl Assoc Hispanic Nurs. 2020.
10. Foundation TAEC. Children in Immigrant Families in United States. Available from: https://datacenter.aecf.org/data/tables/115-children-in-immigrant-families?loc=1&loct=1#detailed/1/any/false/1095,2048,1729,37,871,870,573,869,36,868/any/445,446.
11. Bureau USC. Language spoken at home; 2023. Available from: https://data.census.gov/table/ACSST1Y2023.S1601?q=Language%20Spoken%20at%20Home.
12. Robles JM, Troy JD, Schroeder KM, Martin PL, LeBlanc TW. Parental limited English proficiency in pediatric stem cell transplantation: clinical impact and health care utilization. Pediatric Blood Cancer. 2021;68(9):e29174. doi:10.1002/pbc.29174
13. McQuaid EL. Barriers to medication adherence in asthma: the importance of culture and context. Annals of Allergy, Asthma & Immunology. 2018;121(1):37–42. doi:10.1016/j.anai.2018.03.024
14. Sánchez-Johnsen L, Escamilla J, Rodriguez EM, Vega S, Bolaños L. Latino community-based participatory research studies: a model for conducting bilingual translations. Hisp Health Care Int. 2015;13(1):8–18. doi:10.1891/1540-4153.13.1.8
15. Marin G, Marin BV. Research with Hispanic Populations. Sage Publications, Inc; 1991.
16. Díaz-Millón M, Olvera-Lobo MD. Towards a definition of transcreation: a systematic literature review. Perspectives. 2023;31(2):347–364. doi:10.1080/0907676X.2021.2004177
17. Stewart MK, Boateng B, Joosten Y, et al. Community advisory boards: experiences and common practices of clinical and translational science award programs. J Clin Transl Sci. 2019;3(5):218–226. doi:10.1017/cts.2019.389
18. Bowker L. Interdisciplinary research methods: considering the potential of community-based participatory research in translation. J Transl Studies. 2021;1(1):13–26.
19. Mlambo CK, Vernooij E, Geut R, et al. Experiences from a community advisory Board in the Implementation of early access to ART for all in Eswatini: a qualitative study. BMC Medical Ethics. 2019;20(1):50. doi:10.1186/s12910-019-0384-8
20. Vaughn LM, Jacquez F, Lindquist-Grantz R, Parsons A, Melink K. Immigrants as Research Partners: a Review of Immigrants in Community-Based Participatory Research (CBPR). J Immigrant Minority Health. 2017;19(6):1457–1468. doi:10.1007/s10903-016-0474-3
21. Stevens J. Topical review: behavioral economics as a promising framework for promoting treatment adherence to pediatric regimens. J Pediatr Psychol. 2014;39(10):1097–1103.
22. Peng Y, Wang H, Fang Q, et al. Effectiveness of mobile applications on medication adherence in adults with chronic diseases: a systematic review and meta-analysis. J Manage Care Specialty Pharm. 2020;26(4):550–561. doi:10.18553/jmcp.2020.26.4.550
23. Heneghan MB, Hussain T, Barrera L, et al. Access to technology and preferences for an mHealth intervention to promote medication adherence in pediatric acute lymphoblastic leukemia: approach leveraging behavior change techniques. Original Paper. J Med Internet Res. 2021;23(2):e24893. doi:10.2196/24893
24. Israni A, Dean C, Kasel B, Berndt L, Wildebush W, Wang CJ. Why do patients forget to take immunosuppression medications and miss appointments: can a mobile phone app help?. JMIR Public Health Surveill. 2016;2(1):e15. doi:10.2196/publichealth.5285
25. Gonzalez C, Early J, Gordon-Dseagu V, Mata T, Nieto C. Promoting culturally tailored mHealth: a scoping review of mobile health interventions in Latinx communities. J Immigrant Minority Health. 2021;23(5):1065–1077.
26. Kochashvili M, Guttoo P, Sezgin E, et al. Supporting medication adherence in pediatric patients undergoing hematopoietic stem cell transplant using the BMT4me mHealth App: mixed methods usability study. JMIR Cancer. 2025;11:e66847. doi:10.2196/66847
27. Skeens M, Sezgin E, Stevens J, Landier W, Pai A, Gerhardt C. An mHealth app to promote adherence to immunosuppressant medication and track symptoms in children after hematopoietic stem cell transplant: protocol for a mixed methods usability study. JMIR Res Protoc. 2022;11(7):e39098. doi:10.2196/39098
28. Lewis JR, Sauro J. The Factor Structure of the System Usability Scale. Springer; 2009:94–103.
29. Peres SC, Pham T, Phillips R. Validation of the System Usability Scale (SUS) SUS in the Wild. Los Angeles, CA: Sage Publications Sage CA; 2013:192–196.
30. Lewis JR. The System Usability Scale: past, Present, and Future. Int J Human–Comput Interact. 2018;34(7):577–590. doi:10.1080/10447318.2018.1455307
31. Bangor A, Kortum PT, Miller JT. An Empirical Evaluation of the System Usability Scale. Int J Human–Comput Interact. 2008;24(6):574–594. doi:10.1080/10447310802205776
32. Benedek J, Miner T. Measuring desirability: new methods for evaluating desirability in a usability lab setting. Proc Usability Professionals Assoc. 2002;2003(8–12):57.
33. Merčun T. Evaluation of information visualization techniques: analysing user experience with reaction cards. In:
34. Barnum CM. Preparing for usability testing. Usability Testing Essentials. 2021;197–248.
35. Fedele DA, Cushing CC, Fritz A, Amaro CM, Ortega A. Mobile health interventions for improving health outcomes in youth: a meta-analysis. JAMA Pediatrics. 2017;171(5):461–469.
36. Loi CXA, Alfonso ML, Chan I, et al. Application of mixed-methods design in community-engaged research: lessons learned from an evidence-based intervention for Latinos with chronic illness and minor depression. Eval Program Plan. 2017;63:29–38.
37. Squires A, Aiken LH, Van den Heede K, et al. A systematic survey instrument translation process for multi-country, comparative health workforce studies. Int J Nurs Studies. 2013;50(2):264–273.
38. Eborall H, Morton K. Use of Focus Groups in Developing Behavioural mHealth Interventions: a Critical Review. In: Barbour RS, Morgan DL, editors. A New Era in Focus Group Research: Challenges, Innovation and Practice. Palgrave Macmillan UK; 2017:109–127.
39. Ruvalcaba D, Nagao Peck H, Lyles C, Uratsu CS, Escobar PR, Grant RW. Translating/Creating a Culturally Responsive Spanish-Language Mobile App for Visit Preparation: case Study of “Trans-Creation”. JMIR Mhealth Uhealth. 2019;7(4):e12457. doi:10.2196/12457
40. Perez Ramirez A, Osorio AM, Lai S, James R, Ortega A, Canter KS. A scoping review of Spanish language pediatric digital health interventions. J Pediatr Psychol. 2025. doi:10.1093/jpepsy/jsaf013
41. DeMaio TJ. Social desirability and survey. Surveying Subjective Phenomena. 1984;2:257.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.