Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Transcranial Magnetic Stimulation (TMS) Safety with Respect to Seizures: A Literature Review
Authors Stultz DJ ![]() , Osburn S
, Osburn S ![]() , Burns T, Pawlowska-Wajswol S, Walton R
, Burns T, Pawlowska-Wajswol S, Walton R
Received 15 August 2020
Accepted for publication 17 November 2020
Published 7 December 2020 Volume 2020:16 Pages 2989—3000
DOI https://doi.org/10.2147/NDT.S276635
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Roger Pinder
Debra J Stultz, Savanna Osburn, Tyler Burns, Sylvia Pawlowska-Wajswol, Robin Walton
Stultz Sleep & Behavioral Health, Barboursville, WV 25504, USA
Correspondence: Debra J Stultz
Stultz Sleep & Behavioral Health, 6171 Childers Road, Barboursville, WV 25504, USA
Tel +1 304-733-5380
Fax +1 304-733-5796
Email [email protected]
Abstract: Transcranial magnetic stimulation is an increasingly popular FDA-approved treatment for resistant depression, migraines, and OCD. Research is also underway for its use in various other psychiatric and medical disorders. Although rare, seizures are a potential adverse event of TMS treatment. In this article, we discuss TMS-related seizures with the various coils used to deliver TMS, the risk factors associated with seizures, the differential diagnosis of its presentations, the effects of sleep deprivation and alcohol use on seizures, as well as seizure risks with protocols for traditional TMS, theta-burst stimulation, and accelerated TMS. A discussion is presented comparing the potential risk of seizures with various psychotropic medications versus TMS. Included are case reports of TMS seizures in the child/adolescent patient, bipolar disorder patients, patients with a history of a traumatic brain injury, and those with epilepsy. Reports are also shared on TMS use without seizures in patients with a history of head injuries and TMS’s continued use if patients have a seizure during their TMS treatment. Findings generated in this review suggest the following. Seizures, if present, are usually self-limiting. Most treatment recommendations for TMS-related seizures are supportive in nature. The risk of TMS-related seizures is < 1% overall. TMS has successfully been used in patients with epilepsy, traumatic brain injuries, and those with a prior TMS-related seizure. The rate of TMS-related seizures is comparable to that of most psychotropic medications. While having a seizure is a rare but serious adverse effect of TMS, the benefits of treating refractory depression with TMS may outweigh the risk of suicidal ideation and other significant complications of depression.
Keywords: transcranial magnetic stimulation, transcranial magnetic stimulation-related seizures, transcranial magnetic stimulation safety, transcranial magnetic stimulation in epilepsy patients, head injuries and transcranial magnetic stimulation, transcranial magnetic stimulation in children and adolescents
Introduction
Transcranial Magnetic Stimulation (TMS) is FDA approved for depression, migraines, and OCD, with other symptoms and disorders being aggressively studied for benefit. Lefaucheur et al 20201 have an extensive review of the evidence-based use of rTMS in other disorders such as stroke, multiple sclerosis, tinnitus, anxiety, schizophrenia, substance abuse, Alzheimer’s, ALS, epilepsy, panic, PTSD, and others. TMS uses an electromagnetic coil placed on varying areas of the scalp. This coil generates magnetic pulses and stimulates different brain areas to create the desired pathophysiologic and clinical outcome. TMS was first approved for depression in 2008;2 since that time, various coils have been created, altering the area and depth stimulated. It has been suggested that the different coils may have variations in side effects and the possible frequency of the adverse event of a seizure. There are also different protocols of stimulation used with TMS, with the most recent advances called theta-burst stimulation and accelerated treatment. Theta-burst stimulation uses three magnetic pulses 20 ms apart and repeated every 200 ms of 50 Hz stimulation.3 Accelerated TMS uses multiple TMS stimulation treatments per day.4
Methodology
This paper will focus on the adverse event of a seizure during TMS, which is an abnormal electrical activity and may be due to systemic or local causes. We will also review TMS use in patients with known epilepsy, which is usually due to a structural abnormality of the brain and is that of repeated seizures.
After having a patient who had a seizure during her TMS treatment in 2018, we began looking for all suggestions and references we could find on TMS-related seizures. We had difficulty finding specific information on whether to continue the TMS and what steps to take immediately after the patient had been stabilized from the seizure. From that time forward, we have reviewed articles/books found on PubMed, MEDLINE, Medscape, Cochrane Libray, Scopus, and Google Scholar while collecting information with Mendeley. In this article, we have presented data from 1998 to 2020 (See Table 1). We will discuss the general risk factors associated with seizures, the risks associated with the different TMS coils, reports of seizures with differing TMS protocols, the risk of psychotropic medication alteration on having a seizure, TMS seizures in the child/adolescent population, TMS seizures in bipolar disorder, as well as the possible effects of alcohol use and sleep deprivation on seizures. We will review TMS use with epilepsy and traumatic head injury patients. We will report on continued TMS after a seizure. We will also describe specific steps to take should the patient have a seizure.
 |
 |
 |
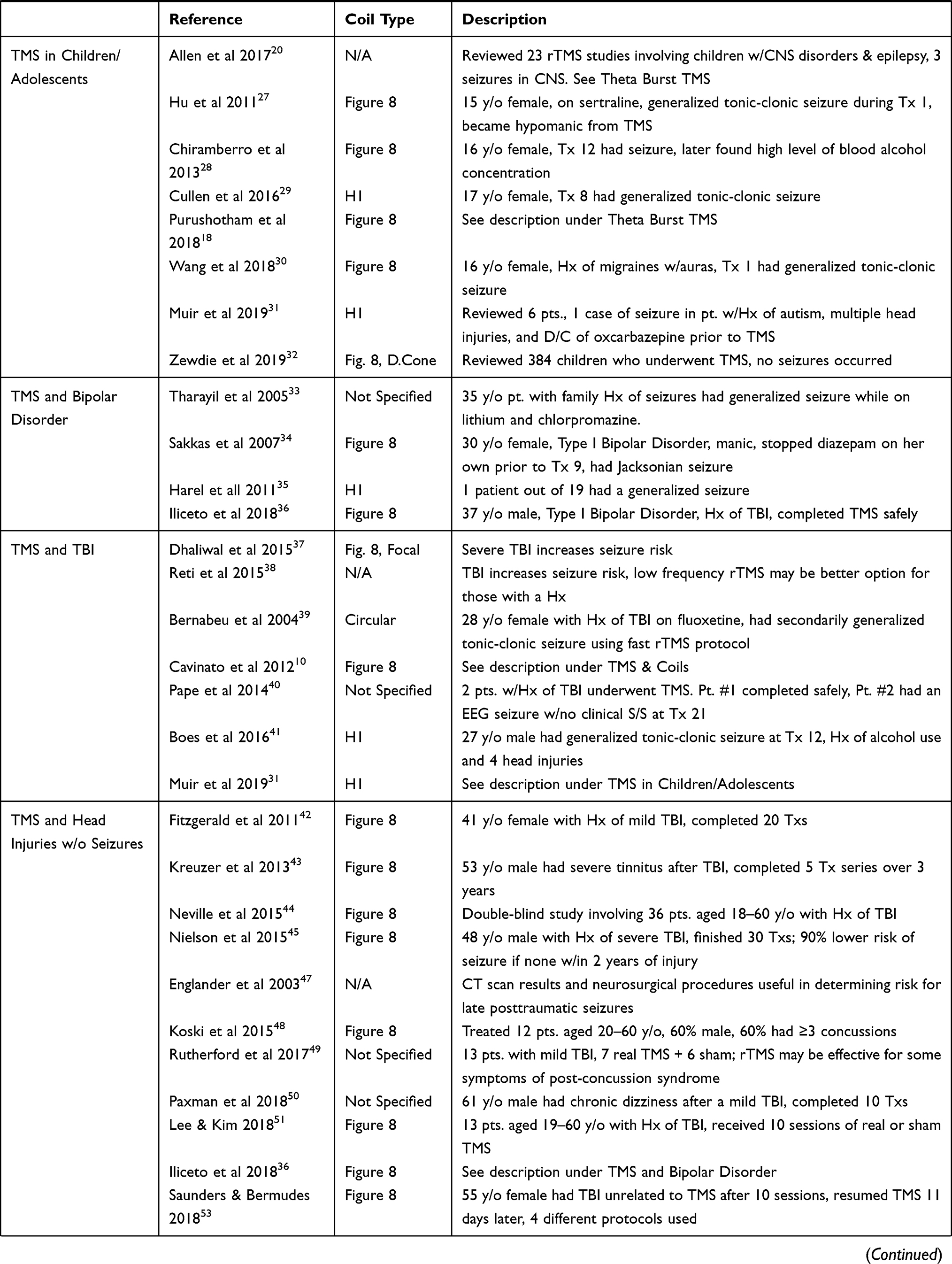
Table 1 Stultz et al TMS Seizure Review Articles |
TMS and Coils
The general risks of a seizure with TMS have been reported to be <1/30,000 (<0.003%) by Rossi et al 2009.5 The risk of seizure with theta burst is estimated at 0.02% by Oberman et al 2011.6 With the Figure-8 coil, the risk of seizure has been estimated by Carpenter et al 20127 to be 3/1000 or <1% overall. Janicak et al 20208 reported postmarketing seizure rates with the Neurostar coil are even lower than previously reported. Tendler et al 20189 reviewed available data for the Brainsway H1-Coil and reported a seizure rate of 0.087%. They reviewed 31 reported cases of seizures with the H1-Coil and felt most were due to the motor threshold (MT) not being rechecked weekly, as recommended by the company. Six seizures were due to stimulation with intensity >120% of the Motor Threshold. No seizures were reported with the first TMS treatment. Nine seizures were associated with medication issues, increased alcohol intake was reported with six patients, and three seizures were associated with sleep issues. While most seizures occur during or around the time of treatment, Cavinato et al 201210 reported on a patient with a traumatic brain injury who had a seizure 3 hours after his TMS treatment. Also, Koudijs et al 201011 reported an increased frequency of seizures for up to 3 days in four children with known epilepsy who had TMS treatment.
Lerner et al 201912 reviewed surveys from 174 providers from 2012 to 2016, revealing 24 seizures out of 318,560 TMS sessions. They reported the risk of seizures with TMS was 0.08/1000 and that “TMS delivered within published guidelines to individuals without risk factors appears to cause fewer than one seizure per 60,000 sessions.” In their review, 62% of seizures occurred on the first exposure to TMS and 75% within the first three treatments. Of the 24 seizures, seven occurred in patients with congenital epilepsy, all of whom were on anti-epileptic medication at the time. Two patients were described as having refractory epilepsy. Lerner et al described the seizure risk for the different coil types as follows: 0.08/1000 for conventional figure-8 coils, double cone coils of 0.12/1000 and 0.43/1000 for H-coils. Only three seizures were reported with the H-coil, but only 7577 (2%) of the 318,560 TMS sessions were completed using the H-coil. The smaller sample size may have made the H-coil numbers appear higher.
TMS Seizure Risk Factors
Rossi et al 20095 conveyed
Seizures are caused by hyper synchronized discharges of groups of neurons in the gray matter, mainly due to an imbalance between inhibitory and excitatory synaptic activity in favor of the latter. Seizures can be induced by rTMS when pulses are applied with relatively high-frequencies and short interval periods between trains of stimulation.
Wasserman 199813 stated that “Intervals between series less than 20 seconds were associated with increased seizures”. (This may have been the cause of the increased seizures reported earlier in the literature using TMS.) McClintock et al 20182 stated
the risk of tonic-clonic seizure, a rare event during rTMS, is related to the direct stimulation of motor cortex or stimulation of the adjacent brain areas with spread of neuronal excitation to the motor cortex. Inspection of the contralateral hand for signs of twitching or movement during stimulation may ensure that stimulation does not spread from prefrontal to primary motor cortex, which can lead to generalized seizure induction with tonic-clonic movement pattern.
McClintock also stated, “seizures can occur within safety guidelines, even in patients who present with no known risk factors.”
The risk factors associated with TMS-related seizures were discussed in the book entitled “Transcranial Magnetic Stimulation in Neuropsychiatry” (George and Belmaker 200714). They reported on the increased risk of seizures with focal or generalized encephalopathy, severe head trauma, non-treated epilepsy, family history of epilepsy in first-degree relatives, heavy alcohol use, severe cardiac disease, increased intracranial pressure, medications that lower seizure threshold, cocaine usage, and other epileptogenic drugs. Other risk factors associated with seizures described throughout the years include a personal history of seizure, stroke, epilepsy, concussions, family history of brain tumors, eating disorders, neurologic disease with altered seizure threshold, sleep deprivation, excessive caffeine/stimulant/cocaine use, MDMA (Ecstasy) use, theophylline use, alcohol withdrawal, benzodiazepine withdrawal, electrolyte disturbance (decreased sodium, change in glucose), other medications that lower seizure threshold, depression, demyelinating disorders (such as Multiple Sclerosis), and fever.
Differential Diagnosis of TMS Seizures
Concerning the differential diagnosis, a distinction must be made between vasovagal syncope and seizure during an episode. Vasovagal syncope symptoms include a transient rapid onset, self-limited loss of consciousness associated with lightheadedness, pale skin, yawning, blurred vision, and a feeling of being warm, cold, clammy, or sweaty (Sheldon et al 200215). Jerky myoclonic movements have also been reported with both vasovagal syncope and seizures.
TMS seizures can be generalized or partial. Kinback in 201816 described a partial tonic seizure in a 42-year-old white female using the H1 coil during treatment 21, where she developed tense jaw and arm muscles, fixed gaze, unresponsiveness, and bilateral upper extremity flexion with clinched wrists. She had slight spine arching but no lower extremity involvement. She stayed fully aware without incontinence or LOC.
Theta-Burst TMS and Seizures
As previously stated, theta-burst TMS has been associated with an estimated seizure risk of 0.02%.6 Oberman and Pascual-Leone 200917 recounted a seizure in a 33-year-old man with no risk factors (except possible sleep deprivation) using theta burst. Purushotham et al 201818 reported on a 15-year-old female with schizophrenia who developed a seizure with theta burst within the first 30 seconds of the first session. Lenoir et al 201819 described two cases of seizures with theta burst. One had a generalized seizure, and one a partial complex seizure. Allen et al 201720 identified no seizures after reviewing three theta-burst studies in 90 healthy children and 40 pediatric patients with CNS disorders.
Accelerated TMS and Seizures
Kallel and Brunelin 202021 described an 18-year-old female with major depression receiving a protocol of 5 sessions per day during four consecutive working days over the left dorsolateral prefrontal cortex using the MagPro X30 figure-eight coil. The patient developed a seizure on the third session of the second day. The seizure underwent secondary generalization and was associated with urinary incontinence and postictal confusion. Twelve days later, the patient agreed to additional TMS given at 1-Hz right DLPFC treatment with one session per day for 30 additional sessions. She also had maintenance TMS scheduled every 2 weeks afterwards and had no seizure activity during her continued or maintenance treatments.
TMS, Psychotropic Medications, and Seizures
Over the years, various medications have been used during which a TMS-related seizure has occurred, but we have found no absolute contraindication with any specific medication to date. Rossi et al5 in their safety article of 2009 listed several medications described as having either a strong potential for hazard or a relative hazard for interactions with TMS. They also included medications that if withdrawn could create a strong relative hazard. (Please see their article for a complete list of medications listed.) Since their 2009 article, many of these substances have been used during TMS without incident.
There has been discussion about changing medications during the TMS treatment, and Loo et al 200822 stated,
If medications are altered during the TMS course, the motor threshold should be re-measured and the stimulus intensity adjusted accordingly. This is based on the premise that medications which alter seizure threshold could also alter motor cortical threshold.
Dobek et al 201523 while studying bupropion treatment with TMS and after an extensive literature review reported the following seizure incidence rates in percent for psychotropic medications independent of TMS use: Bupropion SR 0.1%, Bupropion IR 0.4%, Citalopram 0.25%, Duloxetine 0.2%, Fluoxetine 0.2%, Fluvoxamine 0.2%, Mirtazapine 0.04%, Paroxetine 0.1%, Sertraline up to 0.2%, Venlafaxine 0.3%, Tricyclics 0.1–0.4%, Olanzapine 0.9%, Quetiapine 0.8%, Aripiprazole 0.4%, Ziprasidone 0.4%, and Risperidone 0.3%. Lertxurdi et al 201324 reported that second-generation antipsychotics might have a higher risk of seizures, especially clozapine and possibly olanzapine and quetiapine. Khoury and Ghossoub 201925 revealed studies with antipsychotics are associated with 0.5% to 1.2% risk of seizures, and also reported clozapine appears to increase the risk the most. The above information reveals that the rates of seizures for psychotropic medications are similar or higher than the general TMS rates of <0.003% to 0.087% mentioned previously. Dobek et al23 also stated that TMS-induced seizure data are not associated with any particular antidepressant, and bupropion is not a contraindication to TMS. Thanki et al 202026 even reported on using rTMS in a 60-year-old male with a history of hyponatremic seizures with antidepressants on two different occasions while on sertraline 50 mg and then later on venlafaxine 75 mg, who was later successfully treated with 1 Hz TMS to the right dorsolateral prefrontal cortex at 90% of the resting motor threshold without having a seizure.
TMS Seizures in Child/Adolescent Patients
The overall risk of TMS-related seizures in the child/adolescent population appears to be similar to that of the adult. Allen et al 201720 reported on a review in the pediatric population of 23 repetitive TMS (rTMS) studies (including 230 CNS and 24 epileptic children) identifying three seizures in the CNS patients, with a risk of 0.14% per session. They reviewed three theta-burst studies in 90 healthy children and 40 pediatric patients with CNS disorders and identified no seizures.
Case reports of seizures in the child/adolescent patient have been reported. Hu et al 201127 described an adolescent female on Zoloft who had a seizure and became hypomanic with TMS. She subsequently stopped TMS. Chiramberro et al 201328 reported on a 16-year-old girl who had a seizure during the 12th treatment session with TMS. Of interest, the patient was on sertraline, olanzapine, and hydroxyzine, and she was also found to have used alcohol around the time of treatment. Cullen et al 201629 recounted a 17-year-old female in a sham-controlled study who developed a generalized tonic-clonic seizure during the 8th treatment session of TMS (which was the first day at 120% MT). Purushotham et al 201818 reported a 15-year-old girl with schizophrenia who had a seizure while using theta-burst TMS. Wang et al 201830 told of a 16-year-old girl previously diagnosed as having migraine with aura who had a seizure 10 seconds after the onset of the third rTMS train.
In the transition years to adulthood ages (18–20), Muir et al 201931 reviewed six patients and presented a case of one seizure using the H 1 coil at 120% MT with the risk factors of autism, multiple head injuries, and the discontinuation of oxcarbazepine during the week before TMS initiation. They felt the spontaneous discontinuation of oxcarbazepine was the most likely cause. Most recently, Zewdie et al 201932 reviewed the results of 384 children over ten years that underwent TMS or direct current stimulation (tDCS). Neuromodulation TMS occurred in 119 of the patients with a median age of 14. “Despite 221 (58%) of the patients having some sort of brain injury/or epilepsy, no seizures occurred with single, paired, or rTMS or with tCDS.”
TMS Seizures in Bipolar Patients
TMS seizures have been described in diagnoses other than depression and in the bipolar patient have been reported in 2005 by Tharayil et al, by Sakkas et al, and described again by Harel et al in 2011. Tharayil et al 200533 reported a generalized seizure in a bipolar patient while on chlorpromazine and lithium who also had a positive family history of seizures. Sakkas et al 200734 described a Jacksonian seizure in a manic patient treated with rTMS. Harel et al 201135 studied TMS in 19 Bipolar patients and had only one generalized seizure patient. In 2018, Iliceto et al36 treated a patient with bipolar disorder, generalized anxiety, a TBI, and a history of a suicide gesture without the patient having a seizure. The specific seizure rate with TMS in bipolar disorder is not clear at this time.
TMS in Traumatic Brain Injury Patients
Head injuries are another situation associated with an increased risk of seizures. Dhaliwal et al 201537 stated, “patients with severe TBI do show an increased risk of unprovoked seizures,” and
there is a strong connection between the severity of a brain injury and the subsequent risk of seizures; individuals with mild to moderate TBI have a substantially lower seizure risk than those with severe TBI.
Reti et al 201538 indicated,
TBI is associated with an increased risk of both early and late spontaneous seizures, a significant consideration in evaluating rTMS as a potential treatment for TBI depression. Whilst the risk from rTMS is low; underlying neuropathology may somewhat increase that risk.
They suggested that low-frequency rTMS might be less likely to trigger a seizure.
Various reports of patients with a history of a head injury having a TMS-related seizure have been described. Bernabeu et al 200439 reported a seizure in a TBI patient on fluoxetine but was using a brief interstimulus interval. Cavinato et al 201210 described a 31-year-old male with a history of a severe TBI 8 months before TMS initiation. He had a secondary generalized seizure on the 4th of 10 daily sessions. TMS was delivered at 90% MT, 20 Hz, 1s train duration, and 1-minute inter-train interval to the dorsolateral prefrontal cortex (DLPFC). The seizure developed 3 hours after treatment. Pape et al 201440 reported on a 32-year-old male who had a TBI 9 years before TMS initiation who had an EEG identified seizure during the treatment with no clinical expression. Boes et al 201641 reported on a 27-year-old male with MDE, GAD, alcohol use, and a history of 4 prior head injuries. He was also sleep deprived. He developed a seizure during the 12th treatment session. As described previously, Muir et al 201929 presented a patient with a history of oxcarbazepine withdrawal the week before, autism, and multiple head injuries who had a seizure.
TMS Treatment Without Seizures in Patients with Head Injuries
Transcranial Magnetic Stimulation has also been used successfully without seizures in patients with a history of brain injury. Fitzgerald et al 201142 presented one of the original studies about using TMS without adverse events in a depressed patient with a history of a mild TBI 14 years before the TMS. Kreuzer et al 201343 treated a TBI patient with TMS for severe tinnitus after a head injury with five treatment series of 1 Hz to the left primary auditory cortex at 110% MT and no reported seizure. Neville et al 201544 completed a randomized controlled trial of 36 patients with TBI divided into two groups and administered ten sessions of 10 Hz TMS over the left DLPFC, which demonstrated improvement in depression and cognitive functioning. Nielson et al 201545 reported on a 48-year-old man with a severe TBI history 5 years before TMS was administered with low-frequency right dorsolateral prefrontal cortex stimulation daily for 6 weeks. The patient demonstrated a 49% improvement in his Hamilton Depression Rating Scale46 with treatment. In their article, they set forth that those who have not had a seizure within 2 years of injury have a 90% lower risk of seizure based on work by Englander et al 2003.47
Koski et al 201548 treated 12 patients with post-concussive symptoms (headaches, depression, and cognitive deficits) following mild TBI using rTMS to the left DLPFC at 5-sec trains, 10 Hz, and 110% Motor Threshold. Their patients demonstrated a decrease of 14.6 points (p= 0.009) of post-concussive symptoms. Rutherford et al 201749 studied 13 patients with mild TBI delivering 13 treatment sessions of rTMS to the left DLPFC at 20 Hz in 1.5-second trains of 30 pulses and an inter-stimulation separation of 28.5 seconds. Paxman et al 201850 safely used TMS in a mild TBI patient when treating for chronic dizziness with ten sessions of rTMS to the left DLPFC at 70% motor threshold and a frequency of 10 HZ. Lee and Kim 201851 studied 13 patients divided into an experimental group and sham group. The patients were given rTMS to the right DLPFC for ten sessions and demonstrated improvements in mood based on the Montgomery-Asberg Depression Rating Scale.52 Iliceto et al 201836 treated a 37-year-old man with a severe TBI secondary to a suicide attempt who had a history of anxiety and bipolar disorder. The patient received 30 treatments of 6 Hz TMS to the left DLPFC at 120% MT and a 26-second inter-stimulation interval. Using the PHQ-9 he had a 70.8% improvement in mood.
Saunders and Bermudes 201853 described a 55-year female with a TBI with loss of consciousness during her series of TMS treatments. The event was unrelated to the TMS, and the patient was hospitalized for 4 days. TMS was restarted 11 days after the injury without incident. In 2018 Siddiqi et al54 used 20 sessions of bilateral TMS in a retired NFL defensive lineman. The patient reported at least 12 previous concussions. Using the Montgomery – Asberg Depression Rating Scale, the patient documented improved scores from 32 to 9. Stultz et al 201955 presented a case of a 23-year-old male with a history of four concussions (two of which required hospitalization) having significant depression, generalized anxiety, panic, and OCD symptoms who received 34 TMS treatments and nine booster sessions without a seizure and with improvement in mood and anxiety. He was treated with the H1 coil at 120% MT to the left DLPFC.
TMS Seizures and Alcohol
Excessive alcohol use and withdrawal can precipitate seizures and has been found to possibly increase the risk of TMS-related seizures. Tendler et al 20189 indicated 6 of the 31 patients reviewed with TMS-related seizures using the H1 coil had a history of increased alcohol intake. Alcohol use was also reported in TMS seizure patients’ history by Boes et al 201641 and Chiramberro et al 2013.28 These cases are described elsewhere in this report.
TMS Seizures and Sleep Deprivation
Sleep deprivation has long been identified as a precipitant to having a seizure in epilepsy patients and may increase the risk of a TMS-related seizure. Nakken et al 200556 reported on 1677 patients with epilepsy revealing 53% reported at least one seizure precipitant, with 30% reporting two or more factors had contributed at times to having a seizure. The three most common seizure-precipitating factors were emotional stress, sleep deprivation, and tiredness. Patients having generalized seizures were reported to be more sensitive to sleep deprivation. Ferlisi and Shorvon 201457 studied 104 patients at a tertiary-care adult epilepsy clinic to identify triggering factors to their epilepsy. Ninety-seven percent cited at least one precipitant, with stress, sleep deprivation, and fatigue being the most commonly reported. Those with idiopathic generalized epilepsy were more sensitive to seizures during wake periods and sleep deprivation, with those having extratemporal epilepsy reporting more seizures during sleep.
There are reports of patients having a seizure during TMS in which sleep deprivation may have played a role. Prikryl and Kucerova 200558 described a seizure in a sleep-deprived depressed patient at 110% MT, 15 Hz, and train duration of 10 seconds. Tendler et al 20189 reported that of the 31 patients they reviewed having had a seizure with the H1 coil; three had sleep issues. Oberman and Pascual-Leon 200917 reported on a 33-year-old male who had flown from London to Boston and may have been sleep-deprived before the TMS in which he had a seizure.
TMS in Patients with Epilepsy
TMS has been used in patients with known epilepsy. Bae et al 200759 reported the seizure risk with TMS in patients with epilepsy is less than 2% (4 of 280 patients). Pereira et al 201660 recounted 12/410 patients who had a history of epilepsy developed a seizure during TMS, suggesting a crude rate of seizures per subject of 2.9% in epilepsy patients treated with TMS. Vernet et al 201261 usually indicated TMS-associated seizures in epilepsy patients have been clinically similar to the patients’ typical spontaneous seizures, and the risk of a seizure in temporal association with TMS is less than 2% in epilepsy patients. Allen et al 2017,20 in their previously mentioned review of 23 rTMS studies using TMS in children, included 24 pediatric patients with epilepsy. Koudijs et al 201011 reported an increased frequency of seizures for up to 3 days after TMS in 4 children with known epilepsy based upon follow-up phone conversations. Stultz et al 201962 reported on a 69-year-old white female with a history of complex partial seizures, resistant depression, generalized anxiety disorder, and panic disorder who had three generalized seizures in her lifetime. She received 31 TMS treatments with the H1 coil at 120% MT over the left DLPFC without having a seizure. She has returned for booster TMS sessions without having a seizure. Fitzgerald 201463 described a 57-year-old man diagnosed with epilepsy when he was 26 years old who had been stabilized on sodium valproate and lamotrigine. He was later treated with rTMS of 1 Hz stimulation to the right dorsolateral prefrontal cortex for 20 consecutive weekdays with documented improvement in both mood and anxiety without a seizure.
Continued TMS After a Seizure
If the patient does have a seizure, then the question is that of whether to continue treatment. Bagati et al 201264 described a patient who developed a seizure during treatment session #4, and while using valproate to cover for seizures, he finished TMS. Stultz 201965 reported previously on a patient who had a seizure during treatment session #11 but was then able to continue TMS without additional seizures or additional medications. The patient received 39 treatment sessions in total. In the accelerated TMS article referenced previously by Kalle and Brunelin21, the patient continued treatment and later maintenance treatment after having a seizure.
The Treatment Plan Should a Patient Have a Seizure
Fitzgerald and Daskalakis66 report,
Seizures are likely to terminate fairly rapidly and not require medication treatment: emergency response medical units should potentially be summoned if the seizure does not terminate in several minutes.
Most treatment recommendations for TMS seizures are supportive, with ensuring patient safety, avoiding aspiration, and monitoring blood pressure if possible. Currently, there are no specific recommendations for oxygen or suctioning during the seizure.
As seizures are usually a rare occurrence in the outpatient psychiatric office, one must also debrief the staff and may use the episode as a teachable moment to review seizure protocols with the staff and emphasize the need to be discussing sleep hygiene continually, alcohol use, medication change, etc., with patients daily before their TMS treatment. Concerning documentation, always include the date of occurrence, TMS treatment number, train, placement, motor threshold, and device used. A detailed description of the seizure, how it first presented and then progressed should be described. Documentation should include any identifiable risk factors and the absence of others. List all medications the patient was taking at the time of the seizure, including non-psychotropic meds. Review with the patient any changes they may have had before the seizure concerning sleep, medications, or alcohol/caffeine use. The risk of not treating severe depression versus the risk of another seizure must be discussed with the patient and the family if TMS is to be continued. While not always necessary, some practitioners have added anti-epileptic medications to the treatment regimen before continuing TMS treatment. The seizure should be reported to the FDA and the manufacturer of the TMS unit. Also, one should consider a letter to the editor of a journal to help keep others informed of potential risks and outcomes.
Conclusion
In summary, while TMS has a risk of seizure that is generally <1% overall, some situations may increase that risk, such as alcohol use, brain injury, sleep deprivation, family history, etc. Various case studies have been described in this article in which these situations may have been contributing factors. Traditional TMS, theta burst, accelerated TMS, and child/adolescent TMS use have been reviewed with similar risks for seizures. Comparable seizure rates are reported with both TMS and various psychotropic medications we prescribe daily. (TMS has a lower risk than some of the medications.) We have described successful continued TMS use in patients having had a seizure during TMS and in those with a history of head injury/concussion. TMS use in patients with known epilepsy has also been reviewed. While seizure is a potentially serious adverse event of TMS and must be discussed with the patient, the benefit of treating refractory depression and possibly suicidal ideation may outweigh the risk.
Disclosure
The authors have no conflict of interests to report.
References
1. Lefaucheur JP, Aleman A, Baeken C, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014–2018). Clin Neurophysiol. 2020;131(2):474–528. doi:10.1016/j.clinph.2019.11.002
2. McClintock SM, Reti IM, Carpenter LL, et al. Consensus recommendations for the clinical application of repetitive transcranial magnetic stimulation (rTMS) in the treatment of depression. J Clin Psychiatry. 2018;79(1):35–48. doi:10.4088/JCP.16cs10905
3. Chung SW, Hoy KE, Fitzgerald PB. Theta-burst stimulation: a new form of TMS treatment for depression? Depress Anxiety. 2015;32(3):182–192. doi:10.1002/da.22335
4. Sonmez AI, Camsari DD, Nandakumar AL, et al. Accelerated TMS for depression: a systematic review and meta-analysis. Psychiatry Res. 2019;273:770–781. doi:10.1016/j.psychres.2018.12.041
5. Rossi S, Hallett M, Rossini PM, et al. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin Neurophysiol. 2009;120(12):2008–2039. doi:10.1016/j.clinph.2009.08.016
6. Oberman L, Edwards D, Eldaief M, Pascual-Leone A. Safety of theta burst transcranial magnetic stimulation: a systematic review of the literature. J Clin Neurophysiol. 2011;28(1):67–74. doi:10.1097/WNP.0b013e318205135f
7. Carpenter LL, Janicak PG, Aaronson ST, et al. Transcranial magnetic stimulation (TMS) for major depression: a multisite, naturalistic, observational study of acute treatment outcomes in clinical practice. Depress Anxiety. 2012;29(7):587–596. doi:10.1002/da.21969
8. Janicak P, Heart K, McGugan B. 166 Post market rate of seizures during TMS treatment with NeuroStar® system appears to be lower than previously estimated. CNS Spectr. 2020;25(2):306. doi:10.1017/S1092852920000826
9. Tendler A, Roth Y, Zangen A. Rate of inadvertently induced seizures with deep repetitive transcranial magnetic stimulation. Brain Stimul. 2018;11(6):1410–1414. doi:10.1016/j.brs.2018.09.001
10. Cavinato M, Iaia V, Piccione F. Repeated sessions of sub-threshold 20-Hz rTMS. Potential cumulative effects in a brain-injured patient. Clin Neurophysiol. 2012;123(9):1893–1895. doi:10.1016/j.clinph.2012.02.066
11. Koudijs SM, Leijten FSS, Ramsey NF, van Nieuwenhuizen O, Braun KPJ. Lateralization of motor innervation in children with intractable focal epilepsy—a TMS and fMRI study. Epilepsy Res. 2010;90(1–2):140–150. doi:10.1016/j.eplepsyres.2010.04.004
12. Lerner AJ, Wassermann EM, Tamir DI. Seizures from transcranial magnetic stimulation 2012–2016: results of a survey of active laboratories and clinics. Clin Neurophysiol. 2019;130(8):1409–1416. doi:10.1016/j.clinph.2019.03.016
13. Wassermann EM. Risk and safety of repetitive transcranial magnetic stimulation: report and suggested guidelines from the international workshop on the safety of repetitive transcranial magnetic stimulation, June 5–7, 1996. Electroencephalogr Clin Neurophysiol. 1998;108(1):1–16. doi:10.1016/S0168-5597(97)00096-8
14. George MS, Belmaker RH, eds. Transcranial Magnetic Stimulation in Clinical Psychiatry. Washington, D.C: American Psychiatric Publishing; 2007.
15. Sheldon R, Rose S, Ritchie D, et al. Historical criteria that distinguish syncope from seizures. J Am Coll Cardiol. 2002;40(1):142–148. doi:10.1016/S0735-1097(02)01940-X
16. Kinback KM. Unusual or possibly dangerous TMS side effects, a case series. Brain Stimul. 2018;11(3):e4. doi:10.1016/j.brs.2018.01.017
17. Oberman LM, Pascual-Leone A. Report of seizure induced by continuous theta burst stimulation. Brain Stimul. 2009;2(4):246–247. doi:10.1016/j.brs.2009.03.003
18. Purushotham A, Sinha VK, Goyal N, Tikka SK. Intermittent theta burst stimulation induced seizure in a child with schizophrenia: a case report. Brain Stimul. 2018;11(6):1415–1416. doi:10.1016/j.brs.2018.09.008
19. Lenoir C, Algoet M, Vanderclausen C, Peeters A, Santos SF, Mouraux A. Report of one confirmed generalized seizure and one suspected partial seizure induced by deep continuous theta burst stimulation of the right operculo-insular cortex. Brain Stimul. 2018;11(5):1187–1188. doi:10.1016/j.brs.2018.05.004
20. Allen CH, Kluger BM, Buard I. Safety of transcranial magnetic stimulation in children: a systematic review of the literature. Pediatr Neurol. 2017;68:3–17. doi:10.1016/j.pediatrneurol.2016.12.009
21. Kallel L, Brunelin J. A case report of transcranial magnetic stimulation–related seizure in a young patient with major depressive disorder receiving accelerated transcranial magnetic stimulation. J ECT. 2020;36(3):e31–e32. doi:10.1097/YCT.0000000000000666
22. Loo CK, McFarquhar TF, Mitchell PB. A review of the safety of repetitive transcranial magnetic stimulation as a clinical treatment for depression. Int J Neuropsychopharmacol. 2008;11(1):131–147. doi:10.1017/S1461145707007717
23. Dobek CE, Blumberger DM, Downar J, Daskalakis ZJ, Vila-Rodriguez F. Risk of seizures in transcranial magnetic stimulation: a clinical review to inform consent process focused on bupropion. Neuropsychiatr Dis Treat. 2015;11:2975. doi:10.2147/NDT.S91126
24. Lertxundi U, Hernandez R, Medrano J, Domingo-Echaburu S, García M, Aguirre C. Antipsychotics and seizures: higher risk with atypicals? Seizure. 2013;22(2):141–143. doi:10.1016/j.seizure.2012.10.009
25. Khoury R, Ghossoub E. Antipsychotics and seizures: what are the risks? Curr Psychiatr. 2019;18(3):21–22.:.
26. Thanki MV, Baliga SP, Parameshwaran S, Rao NP, Mehta UM, Thirthalli J. Safe administration of low frequency rTMS in a patient with depression with recurrent antidepressant-associated hyponatremic seizures. Brain Stimul. 2020;13(5):1168–1169. doi:10.1016/j.brs.2020.06.001
27. Hu S-H, Wang -S-S, Zhang -M-M, et al. Repetitive transcranial magnetic stimulation-induced seizure of a patient with adolescent-onset depression: a case report and literature review. J Int Med Res. 2011;39(5):2039–2044. doi:10.1177/147323001103900552
28. Chiramberro M, Lindberg N, Isometsä E, Kähkönen S, Appelberg B. Repetitive transcranial magnetic stimulation induced seizures in an adolescent patient with major depression: a case report. Brain Stimul. 2013;6(5):830–831. doi:10.1016/j.brs.2013.02.003
29. Cullen KR, Jasberg S, Nelson B, Klimes-Dougan B, Lim KO, Croarkin PE. Seizure induced by deep transcranial magnetic stimulation in an adolescent with depression. J Child Adolesc Psychopharmacol. 2016;26(7):637–641. doi:10.1089/cap.2016.0070
30. Wang T, Huang L, Xu H, et al. Seizure induced by repetitive transcranial magnetic stimulation in an adolescent with migraine with aura. Brain Stimul. 2018;11(6):1380–1381. doi:10.1016/j.brs.2018.07.052
31. Muir O, MacMillan C, Khan M, Sang L, Aron T. Safety and tolerability of dTMS treatment in 18–20 year old patients: case series. Brain Stimul. 2019;12(4):e137–e138. doi:10.1016/j.brs.2019.03.049
32. Zewdie E, Ciechanski P, Kuo HC, et al. Safety and tolerability of transcranial magnetic and direct current stimulation in children: prospective single center evidence from 3.5 million stimulations. Brain Stimul. 2020;13(3):565–575. doi:10.1016/j.brs.2019.12.025
33. Tharayil BS, Gangadhar BN, Thirthalli J, Anand L. Seizure with single-pulse transcranial magnetic stimulation in a 35-year-old otherwise-healthy patient with bipolar disorder. J ECT. 2005;21(3):188–189. doi:10.1097/01.yct.0000177516.38421.9c
34. Sakkas P, Theleritis CG, Psarros C, Papadimitriou GN, Soldatos CR. Jacksonian seizure in a manic patient treated with rTMS. World J Biol Psychiatry. 2008;9(2):159–160. doi:10.1080/15622970701624595
35. Harel EV, Zangen A, Roth Y, Reti I, Braw Y, Levkovitz Y. H-coil repetitive transcranial magnetic stimulation for the treatment of bipolar depression: an add-on, safety and feasibility study. World J Biol Psychiatry. 2011;12(2):119–126. doi:10.3109/15622975.2010.510893
36. Iliceto A, Seiler RL, Sarkar K. Repetitive transcranial magnetic stimulation for treatment of depression in a patient with severe traumatic brain injury. Ochsner J. 2018;18(3):264–267. doi:10.31486/toj.17.0075
37. Dhaliwal SK, Meek BP, Modirrousta MM. Non-invasive brain stimulation for the treatment of symptoms following traumatic brain injury. Front Psychiatry. 2015;6. doi:10.3389/fpsyt.2015.00119.
38. Reti IM, Schwarz N, Bower A, Tibbs M, Rao V. Transcranial magnetic stimulation: a potential new treatment for depression associated with traumatic brain injury. Brain Inj. 2015;29(7–8):789–797. doi:10.3109/02699052.2015.1009168
39. Bernabeu M, Orient F, Tormos JM, Pascual-Leone A. Seizure induced by fast repetitive transcranial magnetic stimulation. Clin Neurophysiol. 2004;115(7):1714–1715. doi:10.1016/j.clinph.2004.02.021
40. Pape TL-B, Rosenow JM, Patil V, et al. rTMS safety for two subjects with disordered consciousness after traumatic brain injury. Brain Stimul. 2014;7(4):620–622. doi:10.1016/j.brs.2014.03.007
41. Boes AD, Stern AP, Bernstein M, et al. H-coil repetitive transcranial magnetic stimulation induced seizure in an adult with major depression: a case report. Brain Stimul. 2016;9(4):632–633. doi:10.1016/j.brs.2016.04.013
42. Fitzgerald PB, Hoy KE, Maller JJ, et al. Transcranial magnetic stimulation for depression after a traumatic brain injury. J ECT. 2011;27(1):38–40. doi:10.1097/YCT.0b013e3181eb30c6
43. Kreuzer PM, Landgrebe M, Frank E, Langguth B. Repetitive transcranial magnetic stimulation for the treatment of chronic tinnitus after traumatic brain injury. J Head Trauma Rehabil. 2013;28(5):386–389. doi:10.1097/HTR.0b013e318254736e
44. Neville IS, Hayashi CY, El Hajj SA, et al. Repetitive transcranial magnetic stimulation (rTMS) for the cognitive rehabilitation of traumatic brain injury (TBI) victims: study protocol for a randomized controlled trial. Trials. 2015;16(1):440. doi:10.1186/s13063-015-0944-2
45. Nielson DM, McKnight CA, Patel RN, Kalnin AJ, Mysiw WJ. Preliminary guidelines for safe and effective use of repetitive transcranial magnetic stimulation in moderate to severe traumatic brain injury. Arch Phys Med Rehabil. 2015;96(4):S138–S144. doi:10.1016/j.apmr.2014.09.010
46. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56–62. doi:10.1136/jnnp.23.1.56
47. Englander J, Bushnik T, Duong TT, et al. Analyzing risk factors for late posttraumatic seizures: a prospective, multicenter investigation. Arch Phys Med Rehabil. 2003;84(3):365–373. doi:10.1053/apmr.2003.50022
48. Koski L, Kolivakis T, Yu C, Chen J-K, Delaney S, Ptito A. Noninvasive brain stimulation for persistent postconcussion symptoms in mild traumatic brain injury. J Neurotrauma. 2015;32(1):38–44. doi:10.1089/neu.2014.3449
49. Rutherford G, Mansouri B, Zhang W, et al. rTMS as a treatment for mild traumatic brain injury. Brain Stimul. 2017;10(2):481. doi:10.1016/j.brs.2017.01.409
50. Paxman E, Stilling J, Mercier L, Debert CT. Repetitive transcranial magnetic stimulation (rTMS) as a treatment for chronic dizziness following mild traumatic brain injury. BMJ Case Rep. 2018;
51. Lee SA, Kim M-K. Effect of low frequency repetitive transcranial magnetic stimulation on depression and cognition of patients with traumatic brain injury: a randomized controlled trial. Med Sci Monit. 2018;24:8789–8794. doi:10.12659/MSM.911385
52. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134(4):82–89. doi:10.1192/bjp.134.4.382
53. Saunders R, Bermudes R. TBI during a course of TMS - a case report. Brain Stimul. 2018;11(3):e6. doi:10.1016/j.brs.2018.01.021
54. Siddiqi SH, Trapp NT, Laumann TO, et al. Efficacy and neural network changes with fMRI-targeted rTMS for neuropsychiatric sequelae of repetitive head trauma in a retired NFL player. Brain Stimul. 2018;11(3):e7. doi:10.1016/j.brs.2018.01.023
55. Stultz DJ, Voltin R, Thistlethwaite D, et al. Transcranial magnetic stimulation in the treatment of post-concussion depression. Brain Stimul. 2019;12(4):e140. doi:10.1016/j.brs.2019.03.057
56. Nakken KO, Solaas MH, Kjeldsen MJ, Friis ML, Pellock JM, Corey LA. Which seizure-precipitating factors do patients with epilepsy most frequently report? Epilepsy Behav. 2005;6(1):85–89. doi:10.1016/j.yebeh.2004.11.003
57. Ferlisi M, Shorvon S. Seizure precipitants (triggering factors) in patients with epilepsy. Epilepsy Behav. 2014;33:101–105. doi:10.1016/j.yebeh.2014.02.019
58. Prikryl R, Kucerova H. Occurrence of epileptic paroxysm during repetitive transcranial magnetic stimulation treatment. J Psychopharmacol. 2005;19(3). doi:10.1177/0269881105051545
59. Bae EH, Riviello JJ
60. Pereira LS, Müller VT, da Mota Gomes M, Rotenberg A, Fregni F. Safety of repetitive transcranial magnetic stimulation in patients with epilepsy: a systematic review. Epilepsy Behav. 2016;57:167–176. doi:10.1016/j.yebeh.2016.01.015
61. Vernet M, Walker L, Yoo W-K, Pascual-Leone A, Chang BS. EEG onset of a seizure during TMS from a focus independent of the stimulation site. Clin Neurophysiol. 2012;123(10):2106–2108. doi:10.1016/j.clinph.2012.03.015
62. Stultz DJ, Osburn S, Burns T, Walton R, Wajswol SP. TMS treatment in a patient with seizures and refractory depression. Brain Stimul. 2019;12(3):791. doi:10.1016/j.brs.2019.08.009
63. Fitzgerald PB. Treatment of depression in a patient with epilepsy. Brain Stimul. 2014;7(4):619–620. doi:10.1016/j.brs.2014.03.003
64. Bagati D, Mittal S, Praharaj SK, Sarcar M, Kakra M, Kumar P. Repetitive transcranial magnetic stimulation safely administered after seizure. J ECT. 2012;28(1):60–61. doi:10.1097/YCT.0b013e318221f9b1
65. Stultz DJ. Successful continued TMS treatment after a seizure: a letter to the editor. Brain Stimul. 2019;12(3):791. doi:10.1016/j.brs.2019.01.009
66. Fitzgerald PB, Daskalakis ZJ. A practical guide to the use of repetitive transcranial magnetic stimulation in the treatment of depression. Brain Stimul. 2012;5(3):287–296. doi:10.1016/j.brs.2011.03.006
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.