Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Trans-Cricothyroid Membrane Injection of Local Anesthesia Attenuates Cough Response and Postoperative Sore Throat to the Nasotracheal Tube
Authors Huang L ![]() , Wang L, Peng W, Zhang T
, Wang L, Peng W, Zhang T
Received 19 December 2019
Accepted for publication 4 February 2020
Published 20 February 2020 Volume 2020:16 Pages 103—108
DOI https://doi.org/10.2147/TCRM.S242952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Lili Huang, Li Wang, Wei Peng, Tiejun Zhang
Department of Anesthesiology, The State Key Laboratory Breeding Base of Basic Science of Stomatology (Hubei-MOST) and Key Laboratory of Oral Biomedicine Ministry of Education, School and Hospital of Stomatology, Wuhan University, Wuhan, Hubei 430079, People’s Republic of China
Correspondence: Tiejun Zhang
The State Key Laboratory Breeding Base of Basic Science of Stomatology (Hubei-MOST) and Key Laboratory of Oral Biomedicine Ministry of Education, School and Hospital of Stomatology, Wuhan University, Wuhan, Hubei 430079, People’s Republic of China
Tel/Fax +86 27 87686055
Email [email protected]
Objective: This study aims to investigate the effects of trans-cricothyroid membrane injection of local anesthesia on cough response and postoperative sore throat to the nasotracheal tube.
Methods: Patients who require general anesthesia with nasotracheal tube for oral and maxillofacial surgery were randomised divided into groups L and C. The patients in group L received trans-cricothyroid membrane injection of 2% lidocaine (3 mL) before anesthesia. Meanwhile, the same volume of 0.9% saline was administered to group C. The incidences of cough response, mean arterial pressure (MAP) and heart rate (HR) were recorded during emergency from general anesthesia. Postoperative sore throat (POST) was assessed at 1, 6, 12 and 24 h after surgery.
Results: The data of 60 patients in group L and 61 in group C were included in this study. The incidence of cough was lower in group L than in group C, ie, 41.7% vs 67.2% upon extubation (P=0.006) and 20.0% vs 41.0% at five minutes after extubation (P=0.018). MAP and HR in group L were significantly lower than in group C during emergency from general anesthesia (P< 0.05). POST incidence was significantly reduced in group L at 1 and 6 h after surgery, ie, 35.0% vs 55.7% at 1 h after surgery (P=0.029) and 20.0% vs 37.7% at 6 h after surgery (P=0.044).
Conclusion: Trans-cricothyroid membrane injection of local anesthesia is a simple and effective method to attenuate the incidence of cough response during emergency from general anesthesia. This technique can reduce the incidence of POST after surgery.
Keywords: cricothyroid membrane, cough response, postoperative sore throat
Introduction
The incidence of cough response during emergency from general anesthesia is reported to be 67% to 80%1 and is related to the activation of the sympathetic nervous system that manifests with cardiovascular response. Acute hemodynamic changes may lead to life-threatening complications, such as hypertension, tachycardia, myocardial ischemia and cardiac arrhythmia.2 In addition, postoperative sore throat (POST) is the most common postoperative problem that leads to patient dissatisfaction. Tanaka et al reported that its incidence varies from 30% to 70% after tracheal intubation.3 Various methods and drugs have been applied to moderate cough response and POST,4–6 however, these interventions may lead to other complications, such as respiratory depression or delays in postoperative awakening.
Cricothyroid membrane is in a neutral position of the head and anterior neck. The position is superficial with less vascular and easy to palpate.7 This membrane serves as a route for application of local anaesthetics before awake intubation and awake surgical cricothyrotomy.8,9 In clinical work, we have observed many advantages of this technique for patients in terms of their response to nasotracheal tube from general anesthesia. However, only a few articles have reported the merits of this technology.
The primary objective of our present study was to observe the effect of trans-cricothyroid membrane injection of local anesthesia on cough response during emergency from general anesthesia. The secondary objective was to assess the incidence and severity of POST after surgery.
Patients and Methods
The present study was approved by the Ethics Committee of School and Hospital of Stomatology, Wuhan University (IRB-2018B15) and registered in the Chinese Clinical Trial Registry (ChiCTR-1800017576).This study was conducted at School and Hospital of Stomatology of Wuhan University in accordance with the declaration of Helsinki. All patients provided written informed consent. Patients classified as American Society of Anesthesiologist (ASA) physical status 1 and 2 and aged 20 to 60 years old who were scheduled to undergo oral and maxillofacial surgery. Exclusion criteria include smoking, pre-existing cough, hoarseness or sore throat, Mallampati grade>Ⅱand major systemic illness.
The patients were randomly divided into group L with 60 patients and group C with 61 patients using a computer-generated sequence of numbers. An anesthesiologist (experience>5 years) performed the cricothyroid membrane injection and nasotracheal intubation for all patients using Glidescope. Another anesthesiologist was involved in recording the observations.
All patients were premedicated with a muscle injection of 0.01 mg/kg atropine at 30 min before anesthesia. In the operating room, the radial artery was cannulated for real-time blood pressure monitoring. The electrocardiography, blood oxygen saturation (SaO2), end-tidal carbon dioxide (PetCO2) and cerebral state index were also continuously monitored during the operation.
The patients in group L received cricothyroid membrane injection of 2% lidocaine 3 mL before anesthesia, whereas those in group C received cricothyroid membrane injection of 0.9% normal saline 3 mL. Anesthesia induction was performed through intravenous injection of propofol (1.5–2 mg/kg) and sufentanil (0.4 μg/kg), followed by cis-rocuronium (0.2 mg/kg) to facilitate nasotracheal intubation. Polyvinylchloride ETTs with a 7 mm ID for male and 6.5 mm ID for female were used for intubation. All patients were successfully intubated at one time. The cuff pressure was maintained at 25 cmH2O. Anesthesia was maintained with 10 μg/kg/h remifentanil and 2–3% sevoflurane. Mechanical ventilation was to maintain the PetCO2 at 35 mmHg to 40 mmHg and SaO2 above 98%. At 30 min before the end of surgery, 0.1 μg/kg sufentanil was administered as an intravenous bolus to every patient, and residual neuromuscular block was antagonised with IV-administered 0.02 mg/kg neostigmine and 0.01 mg/kg atropine. All patients received the same patient-controlled intravenous analgesia for postoperative pain therapy.
Our primary outcome was the incidence and severity of cough response and the value of MAP and HR, which were recorded at baseline (T0), before intubation (T1), upon intubation (T2), upon extubation (T3) and 5min after extubation (T4). Secondary outcome was the incidence and severity of POST after surgery. The patients rated their incidence and severity of cough and sore throat using the scoring system as described previously: cough: 0=no cough, 1=minimal cough, 2=moderate cough and 3=severe cough; sore throat: 0=no sore throat, 1=minimal sore throat, 2=moderate sore throat and 3=severe sore throat.10
We recorded the respiratory recovery, extubation and observation times in the post-anesthesia care unit (PACU). Adverse events, which include respiratory depression, hypoxemia, laryngeal oedema and nausea–vomiting, were recorded.
Statistical Analysis
According to the incidence of cough at extubation between two groups from our preliminary experiment and by using Chinese High Intellectualized Statistical Software with a type-I error of 5% and a power of 80%, 57 patients were assigned to each group. Anticipating a 10% dropout rate, we recruited a sample size of 65 per group. All statistical analyses were performed using SPSS 18.0 (SPSS Inc., Chicago, IL, USA). Data are expressed as mean±standard deviation or number. Student’s-t test was used in the comparisons of MAP, HR, age, body mass index (BMI), duration of surgery, respiratory recovery time, extubation time and observation time in PACU. The gender, ASA, incidence and severity of cough, POST and postoperative complications in two groups were compared using chi-square tests and Fisher’s exact test. P<0.05 indicated statistically significant difference.
Results
General Information
Among 130 patients who were assessed for eligibility, six patients refused to consents and three patients violated the protocol. Finally, we analysed a total of 121 patients, ie,60 patients in group L and 61 patients in group C (Figure 1). There were no significant differences between the two groups in terms of age, gender, BMI, ASA and surgery duration (Table 1).
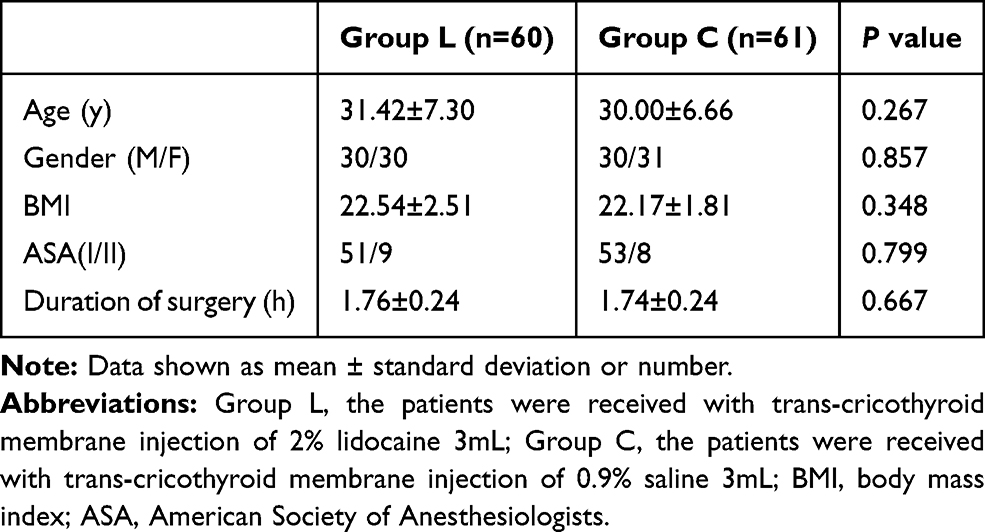 |
Table 1 Demograhic and Surgical Profiles of the Patients |
 |
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) flow diagram of the patients included in the study. |
The Incidence of Cough and Hemodynamic Response During Emergency
The proportion of patients with cough during emergency was 41.7% in group L vs 67.2% in group C at T3 (P=0.006) and 20.0% vs 41.0%, respectively, at T4 (P=0.018, Figure 2). Hemodynamic values at different time-points are shown in Table 2. We found that MAP and HR were significantly lower in group L than in group C at T2 to T4 (P<0.05).
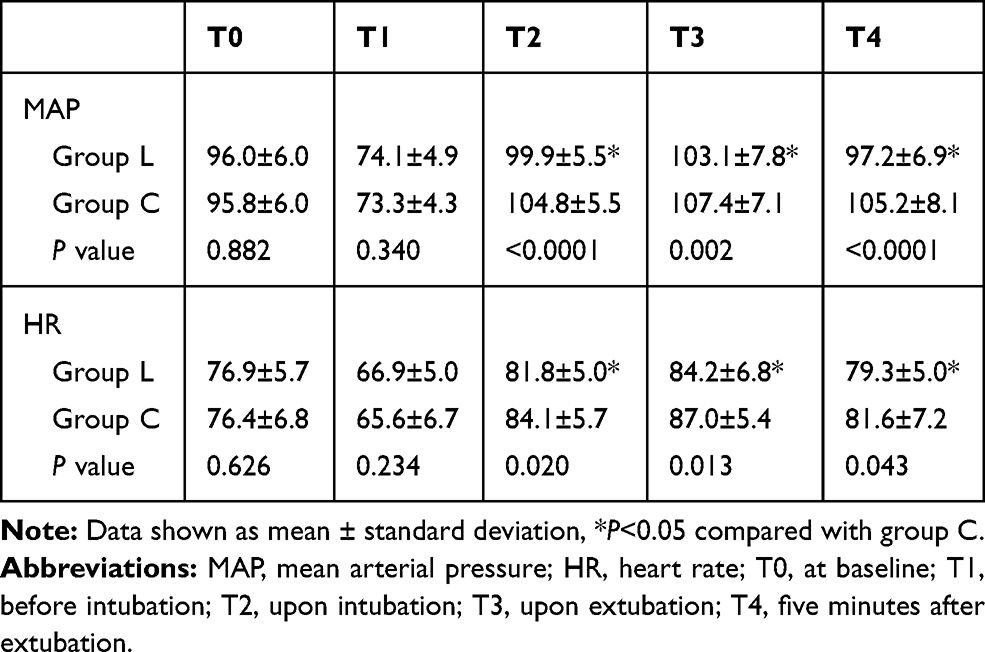 |
Table 2 Comparison of Hemodynamic Responses at Different Time-Points |
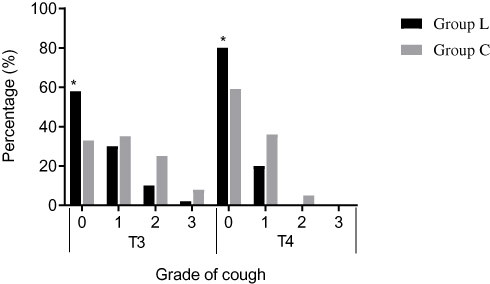 |
Figure 2 Comparion of incidence and severity of cough during emergency. Data are presented as %; Group L: the patients were received with trans-cricothyroid membrane injection of 2% lidocaine 3mL; Group C: the patients were received with trans-cricothyroid membrane injection of 0.9% saline 3mL;T3=upon extubation; T4=five minutes after extubation; 0= no cough during extubation; 1= minimal cough; 2= moderate cough; 3= severe cough. *P<0.05 compared with group C. |
The Incidence of POST After Surgery
The percentages of patients with POST were 35.0% and 55.7% in group L and group C at 1 h after surgery (P=0.029) and 20.0% and 37.7%, respectively, at 6 h after surgery (P=0.044, Figure 3).However, no significant differences were noted in the incidence of POST between the two groups at 12 and 24 h after surgery (P>0.05).
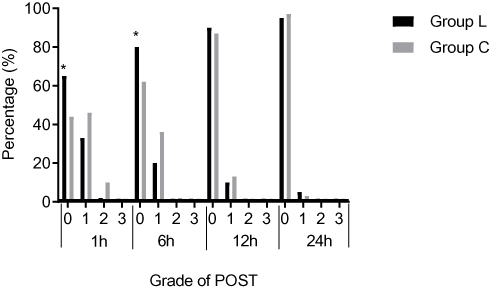 |
Figure 3 Comparion of incidence and severity of POST at 1 h, 6h, 12h and 24h after surgery. Data are presented as %; Group L: the patients were received with trans-cricothyroid membrane injection of 2% lidocaine 3mL; Group C: the patients were received with trans-cricothyroid membrane injection of 0.9% saline 3mL; 1h=1h after surgery; 6h=6h after surgery; 12h=12h after surgery; 24h=24h after surgery; 0= no sore throat after surgery, 1= minimal sore throat ,2=moderate sore throat, and 3= severe sore throat. *P<0.05 compared with group C. |
Complications
The respiratory recovery, extubatd and observation times in PACU were similar between the two groups. Meanwhile, no significant difference was noted between the groups in terms of complications observed during the first 24 h postsurgery (P>0.05, Table 3).
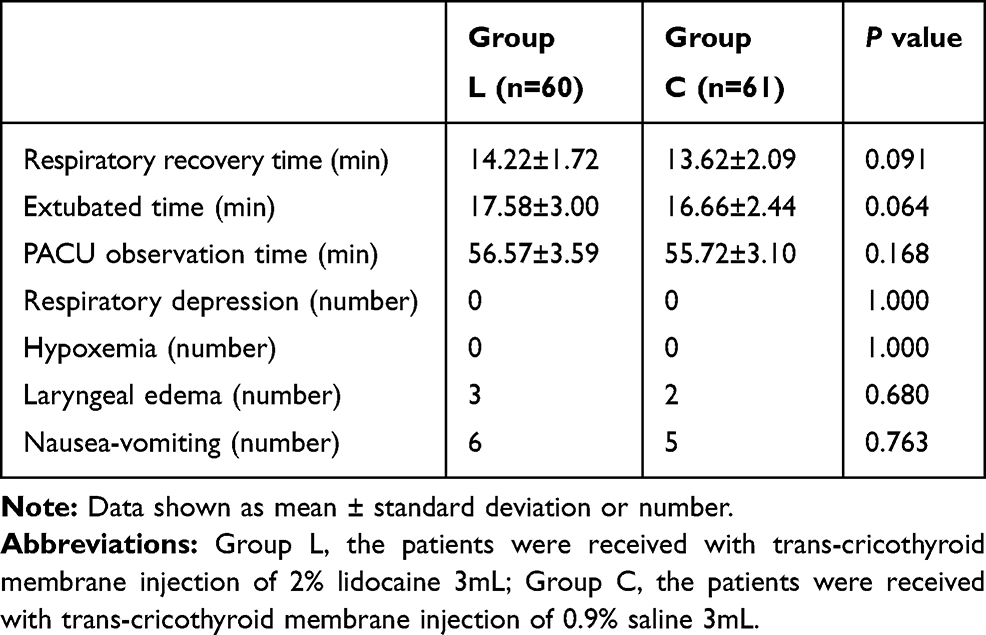 |
Table 3 Recovery Parameters and Complications in Two Groups |
Discussion
Our study revealed that trans-cricothyroid membrane injection of local anesthesia can significantly attenuate the cough response and hemodynamic fluctuations to the nasotracheal tube during emergency from general anesthesia. In addition, this technique is a simple and effective method to reduce the incidence of POST after surgery.
Cough response from general anesthesia is a common and critical clinical problem. The incidence of cough was reportedly 67–80% during emergency, which is related to activation of the sympathetic nervous system that manifests with serious cardiovascular responses.1 Acute hemodynamic changes may lead to severe complications, such as hypertension, tachycardia, myocardial ischaemia and cardiac arrhythmia.2,11 Recently, many methods and drugs, such as deep extubation and intravenous administration of remifentanil, lidocaine or dexmedetomidine,4–6 have been applied to attenuate cough response. However, these methods and drugs can cause respiratory depression, awakening delay and other side effects.
Cricothyroid membrane is in a neutral position of the head and anterior neck. The position is superficial with less vascular and easy to palpate.7 In the present research, the injection of cricothyroid membrane is a fast and simple method that was successfully completed in each patient. No complications, such as subcutaneous emphysema, oesophageal injury, respiratory depression or aspiration occurred. However, Kristensen et al reported that ultrasonographic identification of the cricothyroid membrane may be better for patients with obesity or difficult airway.12 The topical anesthetic used in this trail is lidocaine, which is a common local anesthetic with less side effects.3 Some reports indicated that lidocaine can reduce emergency cough, maintain hemodynamic stability and relieve POST through several routes that include intravenous injection, nasotracheal tube cuff or laryngotracheal instillation.13–15 In our present study, lidocaine is directly injected through cricothyroid membrane, and the incidence of cough was significantly lower in group L than in group C during emergency (41.7% vs 67.2%, P=0.006 at T3 and 20.0% vs 41.0%, P=0.018 at T4) without respiratory depression and delayed awakening (P<0.01) (Figure 2, Table 3). In addition, the MAP and HR of patients were significantly stable during extubation (P<0.05) (Table 2). However, the mechanism is unclear, trans-cricothyroid membrane injection of lidocaine may block the receptors involved in the reflexes in airway mucosa or anaesthetise some part of the trachea.
In addition, the incidence of POST after surgery was reduced by local anaesthetic in our research. POST is the most common postoperative problem that causes patient dissatisfaction. Its incidence varies from 30% to 70% after tracheal intubation.3 Several independent risk factors for POST include larger ETT size, age, female sex, tracheal cuff pressure, prolonged duration of anesthesia and trauma during airway manipulation.16,17 Several interventions have been attempted to reduce the incidence of POST,16 however, none of these interventions were able to eliminate this complication completely. In the present research, the incidences of POST were 35.0% and 20.0% in group L compared with 55.7% and 37.7% in group C at 1 and 6 h after surgery (P=0.029 at 1 h after surgery and P=0.044 at 6 h after surgery, Figure 3), respectively. Trans-cricothyroid membrane injection of local anaesthetic can significantly reduce POST. Our results are consistent with a systemic review that suggested that lidocaine can be used for POST prevention.3 However, no significant differences at 12 and 24 h were noted (P>0.05), the reason for which may be the short half-time of lidocaine. Panpan et al showed that ropivacaine, which was sprayed on the tracheal mucosa, epiglottis, tongue base and glottis, can reduce the visual acuity score of sore throat at 12 h after surgery because of its long action time.5
Some limitations were encountered in our present study. First, lidocaine is a short-half-life local anaesthetic, which cannot inhibit the incidence of POST at 12 and 24 h after surgery. Thus, long-acting topical anaesthetics may be used better for future research. Second, application of airway ultrasonographic identification of the cricothyroid membrane would be better, although we all successfully completed cricothyroid membrane injection at first administration to each patient without complications.
In conclusion, trans-cricothyroid membrane injection of local anesthesia is a simple and effective method to attenuate cough response during emergency from general anesthesia. This technique can also reduce the incidence of POST after surgery.
Data Sharing Statement
We are pleased to share individual deidentified participant data; the trial-related data and figures and tables will be available by contacting Lili Huang through, the email is: [email protected]. The data can be used permanently after the article is published.
Acknowledgments
The authors thank all the colleagues of Department of Anesthesiology, School and Hospital of Stomatology, Wuhan University.
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. Aouad MT, Al-Alami A, Nasr VG, et al. The effect of low-dose remifentanil on responses to the endotracheal tube during emergency from general anesthesia. Anesth Analg. 2009;108(4):1157–1160. doi:10.1213/ane.0b013e31819b03d8
2. Hartley M, Vaughan RS. Problems associated with tracheal extubation. Br J Anaesth. 1993;71(4):561–568. doi:10.1093/bja/71.4.561
3. Tanaka Y, Nakayama T, Nishimori M, et al. Lidocaine for preventing postoperative sore throat. Cochrane Database Syst Rev. 2015;7:CD004081.
4. Fan Q, Hu C, Ye M, et al. Dexmedetomidine for tracheal extubation in deeply anesthetized adult patients after otologic surgery: a comparison with remifentanil. BMC Anesthesiol. 2015;15(1):106–112. doi:10.1186/s12871-015-0088-7
5. Fang PP, Zong ZJ, Yao L, et al. Effect of topical ropivacaine on the response to endotracheal tube during emergence from general anesthesia: a prospective randomized double-blind controlled study. BMC Anesthesiol. 2018;18:134. doi:10.1186/s12871-018-0601-x
6. Ghodratv MR, Hasani V, Bagheri-Aghdam A, et al. Remifentanil infusion during emergence moderates hemodynamic and cough responses to the tracheal tube: a randomized controlled trial. J Clin Anesth. 2016;33:514–520. doi:10.1016/j.jclinane.2015.09.001
7. Hiller KN, Karni RJ, Cai C, et al. Comparing success rates of anesthesia providers versus trauma surgeons in their use of palpation to identify the cricothyroid membrane in female subjects: a prospective observational study. Can J Anesth. 2016;63:807–817. doi:10.1007/s12630-016-0647-5
8. Xue FS, Yang GZ, Sun C. Topical anaesthesia for awake fibreoptic intubation. Anaesthesia. 2016;71(10):1240–1241. doi:10.1111/anae.2016.71.issue-10
9. Asai T. Emergency cricothyrotomy: toward a safer and more reliable rescue method in “cannot intubate, cannot oxygenate” situation. Anesthesiology. 2015;123:995–996. doi:10.1097/ALN.0000000000000849
10. Harding CJ, McVey FK. Interview method affects incidence of postoperative sore throat. Anaesthesia. 1987;42:1104–1107. doi:10.1111/ana.1987.42.issue-10
11. Lee B, Lee JR, Na S. Targeting smooth emergency: the effect site concentration of remifentanil for preventing cough during emergency during propofol-remifentanil anaesthesia for thyroid surgery. Br J Anaesth. 2009;102:775–778. doi:10.1093/bja/aep090
12. Kristensen MS, Teoh WH, Rudolph SS. Ultrasonographic identification of the cricothyroid membrane: best evidence, techniques, and clinical impact. Br J Anaesth. 2016;117(S1):i39–i48. doi:10.1093/bja/aew176
13. Nath P, Williams S, Herrera LM, et al. Alkalinized Lidocaine preloaded endotracheal tube cuffs reduce emergence cough after brief surgery: a prospective randomized trial. Anesth Analg. 2018;126(2):615–620. doi:10.1213/ANE.0000000000002647
14. D’Aragon F, Beaudet N, Gagnon V, et al. The effects of lidocaine spray and intra-cuff alkalinized lidocaine on the occurrence of cough at extubation: a double-blind randomized controlled trial. Can J Anesth. 2013;60:370–376. doi:10.1007/s12630-013-9896-8
15. Lee J, Lee YC, Son JD, et al. The effect of lidocaine jelly on a taper-shaped cuff of an endotracheal tube on the postoperative sore throat: a prospective randomized study: aCONSORT compliant article. Medicine. 2017;96:e8094. doi:10.1097/MD.0000000000008094
16. El-Boghdadly K, Bailey CR, Wiles MD. Postoperative sore throat: a systematic review. Anaesthesia. 2016;71:706–717. doi:10.1111/anae.2016.71.issue-6
17. Subedi A, Tripathi M, Pokharel K, et al. Effect of intravenous lidocaine, dexamethasone, and their combination on postoperative sore throat: a randomized controlled trial. Anesth Analg. 2019;129(1):220–225. doi:10.1213/ANE.0000000000003842
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.