Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Trajectories of functional exercise capacity in patients undergoing pulmonary rehabilitation
Authors Lee CT, Hsieh PL, Chien MY, Chien JY ![]() , Wu HD, Lin JS, Lin HC, Yang PY, Wang LY
, Wu HD, Lin JS, Lin HC, Yang PY, Wang LY ![]()
Received 3 January 2019
Accepted for publication 4 March 2019
Published 17 April 2019 Volume 2019:14 Pages 863—870
DOI https://doi.org/10.2147/COPD.S200247
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chunxue Bai
Video abstract presented by Chien-Tzu Lee.
Views: 570
Chien-Tzu Lee,1 Ping-Lun Hsieh,1,2 Meng-Yueh Chien,1 Jung-Yien Chien,3 Huey-Dong Wu,4 Jia-Shin Lin,1 Hsiao-Chen Lin,1 Pei-Yu Yang,2 Li-Ying Wang1,2
1School and Graduate Institute of Physical Therapy, College of Medicine, National Taiwan University, Taipei, Taiwan; 2Physical Therapy Center, National Taiwan University Hospital, Taipei, Taiwan; 3Department of Internal Medicine, National Taiwan University Hospital, National Taiwan University College of Medicine, Taipei, Taiwan; 4Department of Integrated Diagnostics and Therapeutics, National Taiwan University Hospital, Taipei, Taiwan
Background: Pulmonary rehabilitation (PR) is now considered fundamental when managing patients with chronic respiratory disease. The individual variation in functional exercise capacity (FEC) response to PR within the cohort is unknown. The purpose of this study was to identify FEC patterns in response to PR in patients with chronic respiratory disease using the trajectory modeling method.
Methods: The data of 67 patients with the chronic respiratory disease were retrospectively reviewed and analyzed in this study. All patients received once-weekly supervised training for 8 weeks. Six-minute walk distance (6MWD) was used to measure FEC. Muscle strength and 6MWD were assessed at baseline, Week 4, Week 8 and monthly for two months after PR completion. Group-based trajectory modeling (GBTM) was used to identify patterns in 6MWD in response to PR. The generalized estimating equation method was then used to detect the differences within and between the trajectories of identified groups across time.
Results: Patients were grouped into low- (n=13), moderate- (n=34) and high- (n=20) FEC group based on GBTM analysis. All groups demonstrated significant improvements in 6MWD and leg muscle strength after 8-week PR. Compared to the high-FEC group, a greater proportion of the patients in the low-FEC group required oxygen supplementation during training and had worse baseline leg muscle strength.
Conclusions: Patients showed distinct patterns of 6MWD changes in response to 8-week PR. Distinct characteristics for the low-FEC group included poor lower extremity strength and a greater proportion of required oxygen use at home and during training.
Keywords: chronic respiratory disease, exercise training, functional exercise capacity, trajectory
Introduction
Chronic obstructive pulmonary disease (COPD) is the leading cause of morbidity and mortality worldwide, and its prevalence is expected to rise over the next 30 years.1 COPD is a chronic inflammatory lung disease that causes obstructed airflow from the lung and is characterized by a chronic cough with sputum, dyspnoea and exercise intolerance.1 Exercise intolerance leads to limited physical participation and reduces the quality of life in patients with COPD.2 Pulmonary rehabilitation (PR) aims to reduce the symptom burden, maximize exercise capacity, improve participation in activities of daily living (ADLs) and enhance the quality of life.2
Although the benefits of PR may follow a dose–response relationship, there is no consensus on the optimal duration or frequency of PR for patients with COPD.2 Typically, a PR programme duration of at least eight weeks and 2 or 3 days per week of hospital-based outpatient PR is recommended to achieve a substantial effect.3 A small pilot study (n=30) and randomized controlled trial of once- vs twice-weekly supervised PR for eight and six weeks, respectively, reported equivalent improvements on incremental (ISWT) and endurance (ESWT) shuttle walk test performance.4,5 However, the effect of once-weekly supervised PR on six-minute walk test (6MWT) performance has not yet been determined.
Exercise training is considered a fundamental component of PR programmes, and exercise performance-related outcomes are therefore consistently used to assess individual patients’ responses to PR objectively and evaluate intervention efficacy. Field walking tests are commonly employed to evaluate functional exercise capacity (FEC), assess prognosis and evaluate responses to treatment across a wide range of respiratory diseases. 6MWT is low-cost, requires little equipment and is considered more reflective of daily life than laboratory-based treadmill or cycle ergometer exercise tests.6 The meta-analyses showed that improvements in six-minute walk distance (6MWD) in response to PR ranged from 34 to 78 m.7 In patients with chronic respiratory disease, the minimal clinical important difference (MCID) for the 6MWD was 30 m.7,8 Whether once-weekly supervised PR could achieve this 30-m MCID threshold is unknown.
Comparisons of within- and between-group differences in FEC in response to various PR designs (eg, different programme durations or number of sessions per week) were usually analyzed using traditional analytic methods (eg, generalized linear model) at individual time points. Although the mean performance of FEC for a specific type of PR can be estimated for a cohort of patients at different time points, information concerning the within-cohort individual response variation is unknown. Group-based trajectory modeling (GBTM) is a person-centered method that was developed to predict the trajectory curve for each individual with the purpose of classifying individuals into subgroups based on starting points and changes over time.9 Therefore, the purpose of this study was to identify FEC patterns in response to once-weekly supervised PR among patients with chronic respiratory disease using the trajectory modeling method and explore the potential influential factors among different trajectory groups.
Methods
Participants
This is a retrospective study based on the analysis of patient data between May 2017 and March 2018 from a PR clinic at a tertiary teaching hospital. In total, of 84 patients with chronic respiratory disease who were referred to the 8-week outpatient PR programme, 67 of them who completed the PR programme were included in the final analysis (Figure 1). The dropout rate was 20% and reasons for dropout included unwillingness to continue the training due to lack of motivation or personal reasons (n=10), musculoskeletal injury unrelated to training (n=2), hospitalization due to acute exacerbation (AE) (n=4) and metabolic arthritis attack (n=1).
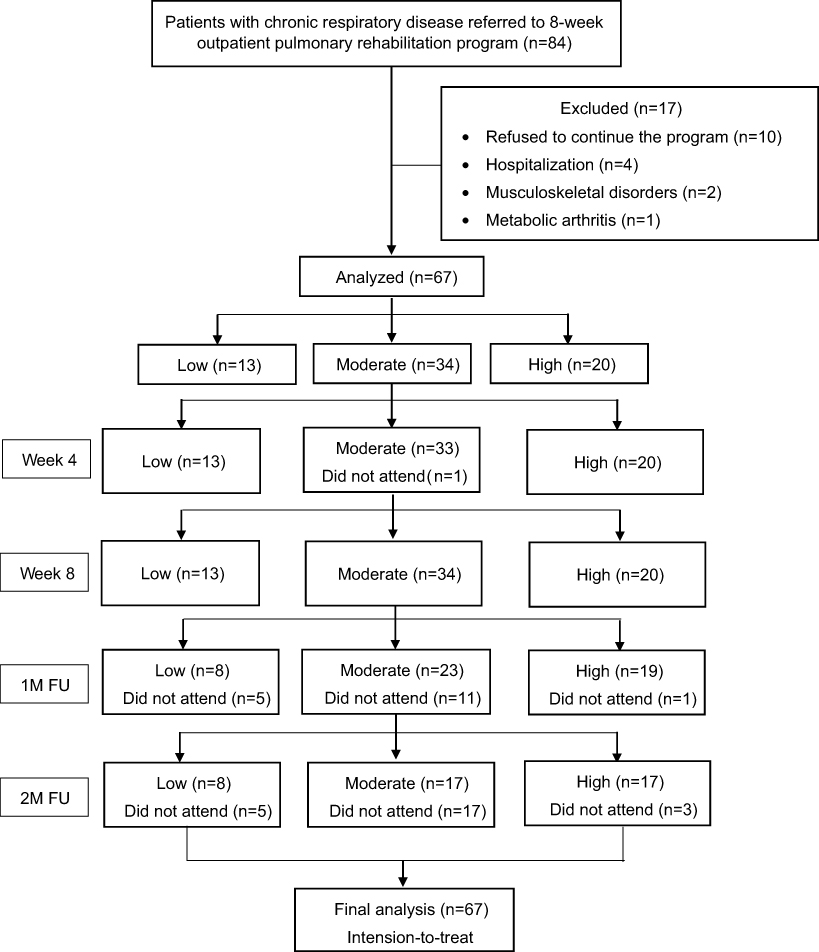 | Figure 1 The flowchart of the patients included in this study.Abbreviations: 1M FU, one month follow-up; 2M FU, two month follow-up. |
Pulmonary rehabilitation
Patients attended the once-weekly hospital-based supervised program for eight weeks. Patients were provided with a home exercise plan in addition to supervised training. The hospital-based program included 30 mins of aerobic exercise using a cycle ergometer with an intensity of 60–80% maximal heart rate (HR, 220 – age)10 and strengthening exercise for both the upper and lower extremities. The hospital-based program also included patient education sessions that covered airway clearance techniques, breathing re-training, medications, energy-conservation techniques and the benefits of being physically active. All patients with COPD were educated on how to use short-acting bronchodilators as rescuer during exacerbation, and the pharmacological treatment plan for the patients is shown in Table 1. Home exercise training consisted of brisk walking at an individually tailored speed for 20–30 mins per day, and patients were instructed to exercise at least 3 days per week and record their exercise volume in an exercise diary.
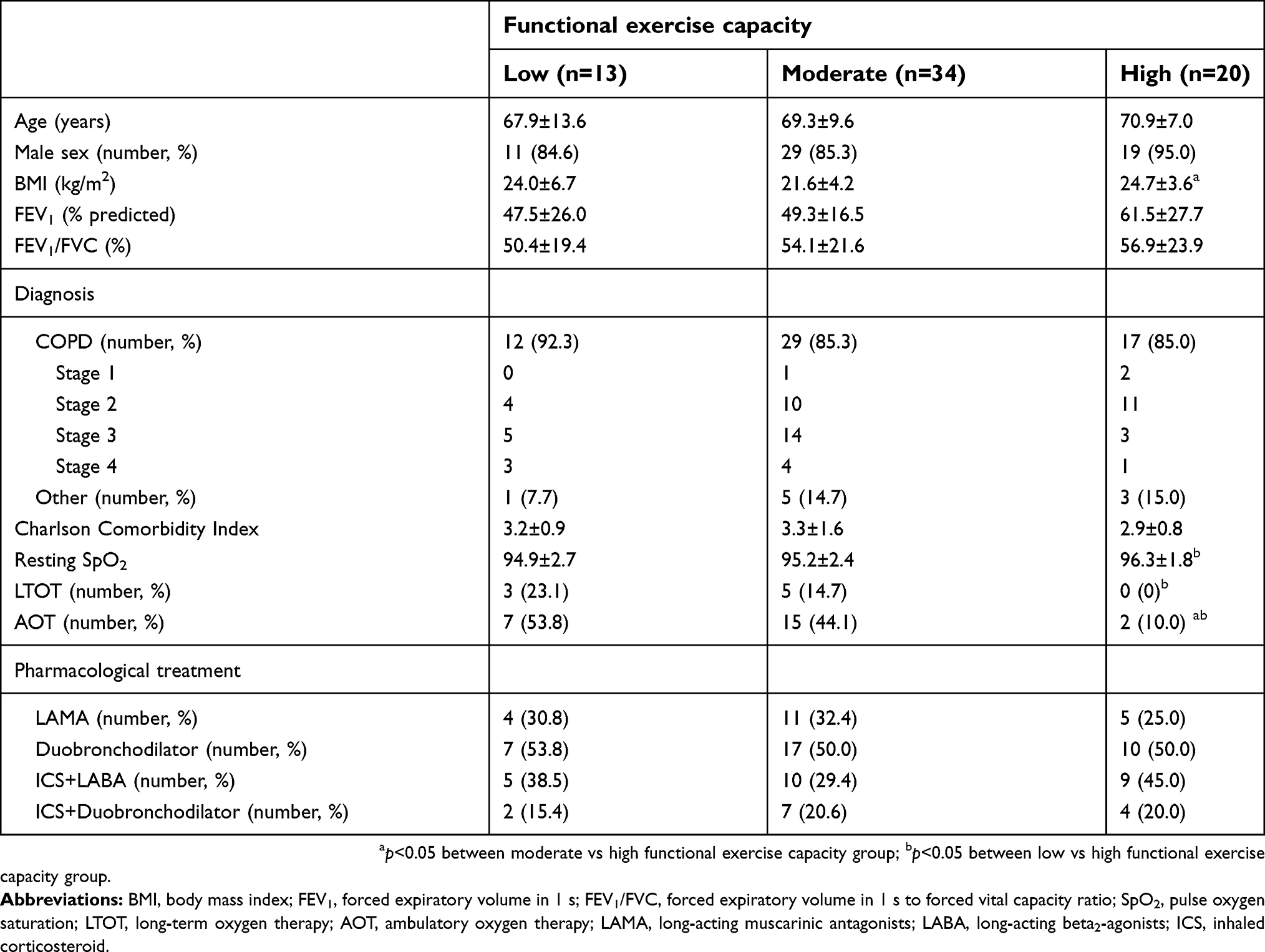 | Table 1 The characteristics of all the patients with chronic respiratory disease, and three trajectory subgroups |
Outcome measures
FEC was assessed by 6MWT at baseline, Week 4 (during PR), Week 8 (PR completion) and first month (1M FU) and second month (2M FU) after the completing PR. The 6MWT was performed according to the American Thoracic Society (ATS) guidelines.11 Blood pressure (BP) and perceived dyspnoea were measured before and after the 6MWT. HR and pulse oxygen saturation (SpO2) were continuously monitored by pulse oximetry throughout the test. The 6MWD was measured for 6MWT. Lower extremity strength was measured using the one-repetition maximum leg press, and handgrip was measured using a handgrip dynamometer. The 6MWD was expressed in absolute (meters) and percentage predicted values, while normal predicted values were derived from the equations of Enright et al, for 6MWD.12 The leg press and handgrip were expressed in absolute (kg) values.
Data collection
Data collection from National Taiwan University Hospital’s medical chart system was approved by the Research Ethics Committee of National Taiwan University Hospital (201805017RINB). Informed consent was waived by the ethics committee due to the retrospective nature of the study and no subjects could be identified, directly or through identifiers linked to the subjects. This study was conducted in accordance with the Declaration of Helsinki. The collected data included baseline patient characteristics; evaluations at baseline, Week 4 (during PR), Week 8 (completion of PR) and monthly for two months after the completion of PR (1M FU and 2M FU); and the patients’ self-recorded home exercise diaries. The AE frequency was also recorded, which defined as a sustained worsening of the condition with increased inflammation which may warrant additional treatment in patients with COPD.1
Statistical analysis
GBTM was used to group patients based on within-individual 6MWD changes (% predicted) over the five time points (baseline, Week 4, Week 8, 1M FU and 2M FU).9,13,14 Akaike’s Information criterion (AIC), the Bayesian information criterion (BIC), the Lo-Mendel-Rubin Likelihood Ratio Test and entropy were used to help determine the optimal number of subgroups. Lower absolute values of AIC and BIC indicate better-fitting models.15 The number of subjects in each subgroup is suggested to be more than 5% of the total sample size.16 Patients in the study were identified and grouped into different 6MWD (% predicted) trajectory groups based on the GBTM analysis. All data were analyzed by intention-to-treat analysis. Then, the generalized estimating equation (GEE) method was used to detect the differences in parameters within and between trajectory groups across time. The significance level was set to α=0.05. The GBTM analysis was performed using Mplus (version 8.1 Demo, Muthén and Muthén, Los Angeles, CA, USA), and GEE was performed using the Statistical Package for the Social Sciences (SPSS), version 18.0 (IBM Corporation, Armonk, NY, USA). The trial was registered as NCT03591263.
Results
The GBTM analysis of 6MWD (% predicted) over time found that the optimal fit was a model with three trajectory subgroups in which patients in the study were grouped into low- (n=13), moderate- (n=34) and high- (n=20) FEC groups (Figure 1). Table 1 presents the characteristics of the patients in the three trajectory subgroups. COPD (87%) was the main diagnosis for our cohort of patients, and the proportion with severe (GOLD 3) or very severe (GOLD 4) COPD was significantly higher in the low- (67%) and moderate- (62%) FEC groups than in the high- (24%) FEC group. The mean age was not different between the groups, but patients in the high-FEC group had a significantly higher body mass index than those in the moderate-FEC group (p<0.05). Although the mean percentage predicted FEV1 tended to be higher in the high-FEC group than in the low- and moderate-FEC groups, the differences did not reach statistical significance. The study cohort had a mean (±SD) Charlson Comorbidity Index of 3.2 (±1.3), and no differences were found among the three different FEC groups. Compared to the high-FEC group, a significantly greater proportion of patients in the low-FEC group were under long-term oxygen therapy (LTOT) (0% vs 23.1%, p=0.02) and required oxygen supplementation during exercise training (10% vs 53.8%, p=0.02). In the moderate-FEC group, the proportion of patients receiving LTOT and requiring oxygen supplementation during exercise was 14.7% and 44.1%, respectively. Resting SpO2 was significantly higher among the high-FEC group than the low-FEC group (p=0.04).
The high-FEC group had significantly higher baseline leg press strength compared to the other two groups (p<0.001). The mean (% predicted) baseline 6MWD was 213.5 (44.2%), 332.1 (67.3%) and 393.7 m (86.4%) for the low-, moderate- and high-FEC groups, respectively. The nadir of SpO2 during 6MWT showed a trend that was higher in the high-FEC group than the other two groups (p=0.07), and the Borg score of baseline 6MWT was similar among the three FEC groups.
Compared to baseline, 6MWD improved significantly after four weeks of training for all groups (all p<0.05), but only the high-FEC group demonstrated further increases at 8 week of training (Table 2). The improvement of 6MWD after 8-week training was maintained in the moderate- and high-FEC groups at 1M and 2M FU. In contrast, the low-FEC group showed a declining trend of 6MWD at 1M and 2M FU. The nadir of SpO2 and Borg score during 6MWT remained similar throughout the five outcome measurement time points for all FEC groups (Table 2). The maximal leg press strength increased significantly after training for all groups at Weeks 4 and 8 of training, and it was maintained for the subsequent two months (Table 2). The average weekly home exercise volume over the 8-week training period was 2.7 (±1.0), 3.7 (±1.1) and 3.7 (±1.5) MET-hr for the low-, moderate- and high-FEC groups, respectively. Home exercise volume was significantly less in the low-FEC group compared to the moderate- and high-FEC groups (both p<0.05). During follow-ups, the home exercise volume remained similar to that during the 8-week PR in the moderate- and high-FEC groups, and it increased by 30.9% and 23.4% at 1M FU and 2M FU, respectively, for the low-FEC group. The mean value of home exercise compliance in low-, moderate-, high-FEC group was 43.5 (±17.5)%, 57.7 (±16.7)% and 61.3 (±20.2)%, respectively, and the compliance in the low-FEC group was significantly lower than those of the other two groups (both p<0.01). The mean (±SD) AE frequency was 0.3 (±0.7), 0.2 (±0.4) and 0.2 (±0.4) times for low-, moderate- and high-FEC group, respectively, and there were no differences among the group (p=0.47). The proportions of patients who had AE more than or equal to one during follow-ups were 23.1%, 17.6% and 15% in low-, moderate- and high-FEC group, respectively (p=0.77), and no hospitalization was required for any AE event.
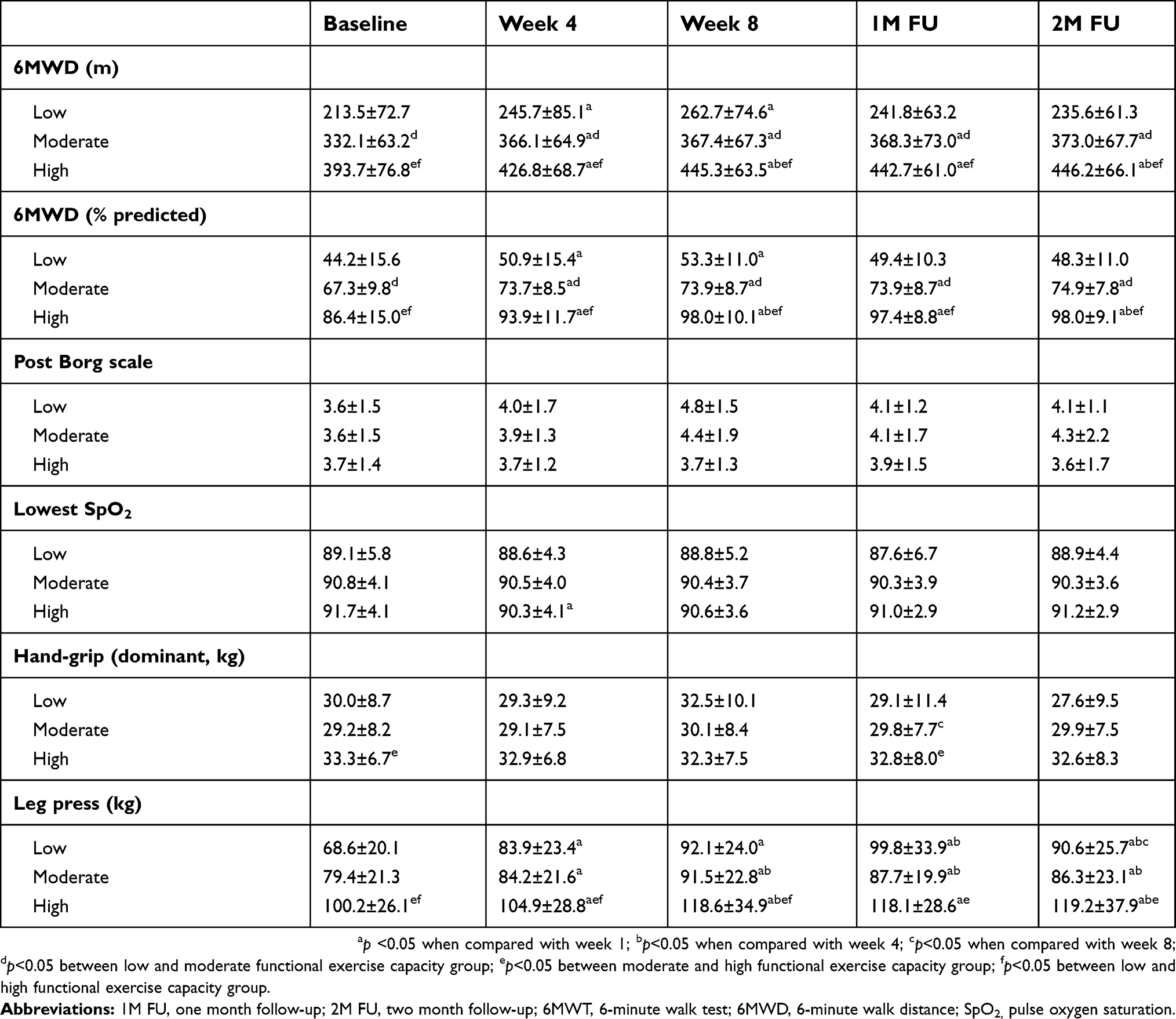 | Table 2 Physiological responses of 6MWT during 8-week pulmonary rehabilitation and follow-ups |
Discussion
This is the first study to use GBTM to explore and compare the differences in FEC trajectory in response to once-weekly supervised PR in patients with chronic respiratory disease. Lung function tended to be worse (but did not reach statistical significance) in the low- and moderate-FEC groups compared to the high-FEC group. Compared to the high-FEC group, a greater proportion of patients identified in the low-FEC group were receiving LTOT, required oxygen supplementation during exercise training, had poor baseline leg press strength, and had lower home exercise volume. All three FEC groups demonstrated significant improvements in 6MWD and leg press strength after 8-week PR. Patients in the moderate- and high-FEC groups showed maintenance of training effects, while patients in the low-FEC group showed a declining trend over the two-month follow-up after PR.
Holland et al, recommended an MCID of 30 m for the 6MWD for patients with chronic respiratory disease.8 Results of a recent meta-analysis showed that the mean improvement of 6MWD for PR was 43.93 m.2 In this study, the mean improvements of 6MWD were 49.2, 35.3 and 51.6 m for the low-, moderate- and high-FEC groups, respectively, indicating both statistical and clinical significance for the effects of PR. However, compared to baseline, the improvement in 6MWD was 28.3 and 22.1 m at 1M FU and 2M FU in the low-FEC group, indicating that the benefits of PR could not be maintained above the clinical significance threshold. In our study, the proportions of patients who had reached MCID of 30 m8 for 6MWD after PR were 61.5%, 50.0% and 65.0%, respectively, and were 46.2%, 38.2% and 60.0%, respectively, if using MCID of 54 m17 for patients in low-, moderate- and high-FEC group. This finding implied that selecting the MCID threshold for defining 6MWD improvements after PR is not a simple task when great differences of FEC exited in patients with chronic respiratory disease (as shown by trajectories). The ancillary analysis revealed that factors associated with low-FEC included poor baseline leg-press strength, lower % predicted FEV1, higher baseline perceived dyspnoea, poor handgrip strength and oxygen supplementation required during exercise. Leg-press strength at baseline alone was accounted for 12% of variance in 6MWT performance. The declining trend of lower extremity strength was greater in the low-FEC group compared to the other two groups at follow-ups, thus, decreased lower extremity strength might partially explain why PR benefits were not able to maintain in this group. Other unidentified factors which could also have a negative impact on PR benefit maintenance in low-FEC group warrant further investigation. A three-year prospective study (ECLIPSE) showed that patients with COPD with a 6MWD ≤334 m had an estimated three-year mortality and hospitalization hazard ratio of 2.3.18 In this study, only the low-FEC group had an average 6MWD ≤334 m, and since benefits were not maintained after PR, this subgroup of patients might be at risk for mortality and hospitalization. Further work is required to investigate how to refine PR to optimize and maintain the training benefits for this patient subgroup.
The average home exercise volume in this study was significantly higher in the moderate- and high-FEC groups than the low-FEC group. Furthermore, more patients in the low-FEC group were receiving LTOT, and not all patients were equipped with a portable oxygen supply device. This might present a barrier to home exercise, and it could partially explain the lower home exercise volume among this group of patients. Both behavioral and physical components could affect patients’ compliance with home exercise programs. Regarding the physical component, Pitta et al, found that patients with COPD who had higher exercise tolerance tended to have higher directly measured everyday activities, which included walking time.19 It is possible that low home exercise volume among low-FEC patients was just due to their poor exercise tolerance. In addition, all patients in the study were encouraged to continue exercising at home as maintenance training. It was interesting to note that only low-FEC patients showed a trend of increased home exercise volume during follow-ups after PR had finished, while the other two groups maintained similar amounts. This phenomenon implied that a training load of once-weekly supervised training together with home exercise might be too much for low-FEC patients, and thus, determining how to modify training accordingly warrants further investigation.
Ambulatory oxygen therapy (AOT) is defined as the use of supplemental oxygen during exercise and ADLs.20 AOT is also often supplied to LTOT recipients during exercise. However, we found that 31%, 29% and 10% of the patients in the low-, moderate- and high-FEC groups in this study, respectively, were not hypoxemic at rest but desaturated (SpO2<88%) during 6MWT. This finding supports the American Thoracic Society and British Thoracic Society (ATS/BTS) guidelines that exercise assessment is required before starting an exercise training program to evaluate the potential need for supplemental oxygen. Patients in the low- and moderate-FEC groups had lower average FEV1 (% predicted) than those in the high-FEC group (although not to a statistically significant degree), indicating a more severe expiratory flow limitation and thus higher potential to develop dynamic hyperinflation during exercise in these patient groups. A previous study found that the use of AOT could be beneficial during PR through a reduction in dynamic hyperinflation.21 Furthermore, Waatevik et al, reported that patients with COPD who experienced oxygen desaturation during the 6MWT had a significantly worse prognosis than non-desaturating patients for multiple important disease outcomes.22 Therefore, it is of clinical importance to follow up on patients’ desaturation status during 6MWT.
Leg press strength increased significantly in all three FEC groups after eight weeks of PR with a mean of 34.3%, 15.2% and 18.4%, for the low-, moderate- and high-FEC groups, respectively. It is unsurprising that people with lower muscle strength at baseline obtained a larger improvement after PR training. Although the benefit of PR on lower extremity strength could still be seen at 2M FU for all three groups, the low-FEC group showed a declining trend compared to immediately after PR, while the improvements in the other two groups were preserved. In this study, the improved lower extremity strength could be the result of combined aerobic and strength training, which agrees with previous findings.23,24 Note that although the home exercise volume increased after PR was finished in the low-FEC group, the declining trend of leg press strength after this time point implied that walking exercise alone was insufficient to maintain lower extremity strength in this group of patients. Although walking is the most commonly reported form for home exercise, the recent evidence showed that the threshold value to define moderate-intensity ambulatory activity in apparently healthy adults estimates of >100 steps/min.25 Only very few of patients in our cohort were able to walk with the cadence of >100 steps/min as their home exercise training speed, thus, it was possible the training volume was not sufficient to maintain aerobic capacity gained during PR. On the other hand, whether the walking speed threshold which defined moderate-intensity for healthy adults (ie, cadence of >100 steps/min) is suitable for patients with chronic respiratory disease requires further investigation. Moreover, the importance of including lower extremity resistance exercise in the home-based maintenance exercise programs should be emphasized.
The limitations of this study included its retrospective nature, the lack of a control group and the fact that the home exercise volume was obtained from subjective records (ie, self-recorded training logs). All patients in this study received PR delivered in the same setting, with the same structure, from the same personnel and of the same duration, which minimized the potential bias from program deviation. Grouping patients based on GBTM analysis from a larger sample size study will help us understand the distinct pattern of PR benefit trajectories and help us design more precise personalized training programs for patients with chronic respiratory disease.
Conclusions
Patients with chronic respiratory disease showed distinct patterns of 6MWD changes in response to exercise training. Factors for low FEC in patients with chronic respiratory disease included poor lower extremity strength and supplemental oxygen requirement at rest and during exercises. For patients with chronic respiratory disease undergoing PR, GBTM could be used to identify FEC improvement trajectories and provide groupings that may be of clinical utility.
Data availability
The data that support the findings of this study are available from the corresponding author [LW] upon reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
References
1.
2. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;(2):Cd003793.
3. Beauchamp MK, Janaudis-Ferreira T, Goldstein RS, Brooks D. Optimal duration of pulmonary rehabilitation for individuals with chronic obstructive pulmonary disease – a systematic review. Chron Respir Dis. 2011;8(2):129–140. doi:10.1177/1479972311404256
4. O’Neill B, McKevitt A, Rafferty S, et al. A comparison of twice- versus once-weekly supervision during pulmonary rehabilitation in chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2007;88(2):167–172. doi:10.1016/j.apmr.2006.11.007
5. Liddell F, Webber J. Pulmonary rehabilitation for chronic obstructive pulmonary disease: a pilot study evaluating a once-weekly versus twice-weekly supervised programme. Physiotherapy. 2010;96(1):68–74. doi:10.1016/j.physio.2009.04.007
6. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
7. Singh SJ, Puhan MA, Andrianopoulos V, et al. An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1447–1478. doi:10.1183/09031936.00150414
8. Holland AE, Spruit MA, Troosters T, et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1428–1446. doi:10.1183/09031936.00150314
9. Nagin DS, Nagin D. Group-Based Modeling of Development. Cambridge, MA: Harvard University Press; 2005.
10.
11. American Thoracic Society 2002 Committee on proficiency standards for clinical pulmonary function laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
12. Enright PL, Sherrill DL. Reference equations for the six-minute walk in healthy adults. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1384–1387. doi:10.1164/ajrccm.158.5.9710086
13. Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Struct Equ Model. 2007;14(4):535–569. doi:10.1080/10705510701575396
14. Frankfurt S, Frazier P, Syed M, Jung KR. Using group-based trajectory and growth mixture modeling to identify classes of change trajectories. Couns Psychol. 2016;44(5):622–660. doi:10.1177/0011000016658097
15. Greenbaum PE, Del Boca FK, Darkes J, Wang CP, Goldman MS. Variation in the drinking trajectories of freshmen college students. J Consult Clin Psychol. 2005;73(2):229–238. doi:10.1037/0022-006X.73.2.229
16. Delucchi KL, Matzger H, Weisner C. Dependent and problem drinking over 5 years: a latent class growth analysis. Drug Alcohol Depend. 2004;74(3):235–244. doi:10.1016/j.drugalcdep.2003.12.014
17. Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting small differences in functional status: the six minute walk test in chronic lung disease patients. Am J Respir Crit Care Med. 1997;155(4):1278–1282. doi:10.1164/ajrccm.155.4.9105067
18. Andrianopoulos V, Wouters EF, Pinto-Plata VM, et al. Prognostic value of variables derived from the six-minute walk test in patients with COPD: results from the ECLIPSE study. Respir Med. 2015;109(9):1138–1146. doi:10.1016/j.rmed.2015.06.013
19. Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):972–977. doi:10.1164/rccm.200407-855OC
20. Hardinge M, Annandale J, Bourne S, et al. British Thoracic Society guidelines for home oxygen use in adults. Thorax. 2015;70(Suppl 1):i1–i43. doi:10.1136/thoraxjnl-2015-206865
21. O’Donnell DE, D’Arsigny C, Webb KA. Effects of hyperoxia on ventilatory limitation during exercise in advanced chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;163(4):892–898. doi:10.1164/ajrccm.163.4.2007026
22. Waatevik M, Johannessen A, Gomez Real F, et al. Oxygen desaturation in 6-min walk test is a risk factor for adverse outcomes in COPD. Eur Respir J. 2016;48(1):82–91. doi:10.1183/13993003.00975-2015
23. Rinaldo N, Bacchi E, Coratella G, et al. Effects of combined aerobic-strength training vs fitness education program in COPD patients. Int J Sports Med. 2017;38(13):1001–1008. doi:10.1055/s-0043-112339
24. Zambom-Ferraresi F, Cebollero P, Gorostiaga EM, et al. Effects of combined resistance and endurance training versus resistance training alone on strength, exercise capacity, and quality of life in patients with COPD. J Cardiopulm Rehabil Prev. 2015;35(6):446–453. doi:10.1097/HCR.0000000000000132
25. Tudor-Locke C, Han H, Aguiar EJ, et al. How fast is fast enough? Walking cadence (steps/min) as a practical estimate of intensity in adults: a narrative review. Br J Sports Med. 2018;52(12):776–788. doi:10.1136/bjsports-2017-097628
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.