Back to Journals » Patient Preference and Adherence » Volume 20
Trajectories and Influencing Factors of Depression in Patients with H-Type Hypertension-Related Ischemic Stroke: A Single-Center Longitudinal Study
Authors Guo Y, Wang J, Zhao P, Zhang M, Zhou X ![]() , Guo J, Li Q, Du S, Yuan A, Liu Y, Guo L
, Guo J, Li Q, Du S, Yuan A, Liu Y, Guo L ![]()
Received 20 March 2026
Accepted for publication 21 May 2026
Published 9 June 2026 Volume 2026:20 610786
DOI https://doi.org/10.2147/PPA.S610786
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yuying Guo,1,* Juanjuan Wang,1,* Peng Zhao,2 Mengyu Zhang,1 Xinxin Zhou,2 Jiale Guo,1 Qingyang Li,2 Shuo Du,2 Ao Yuan,2 Yanjin Liu,1 Lina Guo1
1Department of Neurology, National Advanced Stroke Center, the First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 2School of Nursing and Health, Zhengzhou University, Zhengzhou, People’s Republic of China
*Yuying Guo and Juanjuan Wang contributed equally to this work
Correspondence: Lina Guo, Department of Neurology, National Advanced Stroke Center, the first Affiliated Hospital of Zhengzhou University, Zhengzhou; Department of Neurology, Henan Brain Hospital of Tiantan Hospital, National Regional Medical Center, Zhengzhou, People’s Republic of China, Email [email protected]
Background: This study aimed to identify depression trajectory patterns in patients with H-type hypertension-related ischemic stroke and explore predictors using the COM-B framework.
Methods: A prospective longitudinal study enrolled 588 patients from a Chinese tertiary hospital (September 2023–December 2024). Data were collected at six time points (admission and 1, 3, 6, 9, 12 months post-discharge). Growth mixture modeling identified trajectory classes, and multivariate logistic regression determined predictive factors.
Results: Four depression trajectory classes were identified: (1) Rapid Recovery group (n=155, 26.4%): swift symptom resolution; (2) Moderate Improvement group (n=70, 11.9%): moderate symptom improvement; (3) Persistent Low-Symptom group (n=102, 17.3%): optimal reference category; (4) Symptom-Aggravation group (n=261, 44.4%): exacerbation over time. Protective factors included positive health behaviors (strongest across all comparisons), first-time stroke onset, urban residence, and employed status (all p < 0.05). Risk factors included higher health knowledge levels, elevated homocysteine, unemployed/retired status, and higher social support. Notably, elevated homocysteine and higher social support were associated with worsening depression, especially in the Symptom-Aggravation group (p < 0.05).
Conclusion: Four distinct depression trajectories were identified in H-type hypertension-related ischemic stroke patients, with specific predictors. These findings inform targeted interventions to improve depression outcomes.
Keywords: H-type hypertension, post-ischemic stroke depression, COM-B model, longitudinal study
Introduction
Post-stroke depression (PSD) is one of the most common neuropsychiatric complications following stroke, affecting approximately 28 million stroke survivors in China.1 Notably, over 30% of ischemic stroke survivors are diagnosed with PSD,2 which contributes to 17.2% of the total healthcare burden among acute ischemic stroke patients in China, posing a significant public health challenge.3 A recent systematic review and meta-analysis by Liu et al reported that the overall prevalence of PSD is 27%, with early-onset depression (within 3 months after stroke) having a high risk of becoming persistent, and two-thirds of incident depression cases occur within the first 3 months.4 With the growing number of ischemic stroke cases projected in the coming decade, the incidence of PSD is expected to rise accordingly.
Research has shown that both physiological and psychological factors contribute to PSD. Physiological factors include stroke severity, lesion location, inflammatory markers, hypertension, and elevated homocysteine (Hcy) levels.5–7 In China, around 75% of hypertensive patients also present with elevated Hcy levels (≥10μmol/L), a condition termed H-type hypertension.7,8 This combined condition may heighten the risk of PSD by intensifying neuroinflammatory and vascular injury responses after stroke.9 However, research on the relationship between H-type hypertension and PSD remains limited.
Moreover, psychological and behavioral aspects of PSD have often been explored in isolation, overlooking the dynamic interplay among influencing factors. Recent studies suggest that PSD is also linked to cognitive functioning,10 social support,2 and health behaviors11—factors that align closely with the COM-B model (Capability, Opportunity, Motivation–Behavior).12,13 In this study, “capability” refers to disease-related cognitive ability, “opportunity” refers to perceived social support, and “motivation” is represented by depression symptoms, with “behavior” defined as the patient’s health behavior.
Therefore, this study aims to investigate the longitudinal trajectories of depression and identify latent post-stroke depression (PSD) subgroups among patients with H-type hypertension-associated ischemic stroke using the Growth Mixture Model (GMM), while also examining relevant predictive factors. The findings aim to provide a theoretical foundation for the development of targeted, subgroup-specific rehabilitation strategies and improve the quality of life among stroke survivors.
Methods
Participants and Procedure
The present study employed a convenience sampling method to recruit hospitalized stroke patients from a tertiary hospital in Zhengzhou, Henan Province, China. Data collection was conducted between September 2023 and December 2024. The inclusion criteria for this study were as follows: participants had to be diagnosed with ischemic stroke by a neurologist and meet the diagnostic criteria for H-type hypertension, characterized by a serum homocysteine (Hcy) level of ≥ 10 μmol/L.14 Eligible participants were required to be 18 years of age or older, have no communication barriers, and demonstrate no cognitive impairment, diagnosed by a neurologist with no cognitive impairment. Participants were excluded if they were enrolled in other clinical studies or suffering from any serious illness with an expected lifespan of less than one year. According to standard requirements for multivariate analysis, the sample size should be at least equal to a multiple of the number of independent variables included in the model. In this study, with 38 independent variables, the minimum required sample size is ten times that number, amounting to at least 475 participants.15
Ethical Considerations
This study was approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University (Approval Number:2022-KY-1168-001). Written informed consent was obtained from all participants after they were provided with a full explanation of the study’s objectives. The implementation of this study is in line with the principles of the Helsinki Declaration.
Data Collection
At the time of admission, 600 patients met the inclusion criteria and expressed willingness to participate in the study. Ultimately, 588 patients who completed follow-up assessments at six time points were included in the final analysis. During hospitalization, detailed clinical data were collected for each patient. With guidance from the department’s cardio-cerebral health manager, participants established follow-up profiles using a digital management platform.
Eligible patients were enrolled after meeting the inclusion criteria. The researchers provided standardized instructions outlining the requirements for completing the questionnaire to ensure consistency and data integrity. Patients completed self-administered questionnaires; for those who were illiterate or physically unable to do so, trained researchers read the items aloud and recorded the responses. Each session took approximately 20–30 minutes. Completed questionnaires were carefully checked for missing data, and any omissions were immediately addressed with the patient on site.
Following the initial individual assessment during hospitalization (T1), follow-up evaluations were conducted at predetermined time points through telephone interviews, WeChat communication, and face-to-face outpatient visits. These follow-ups occurred at the following intervals: 1 month (T2), 3 months (T3), 6 months (T4), 9 months (T5), and 12 months (T6) after discharge. Telephone interviews were conducted in accordance with the standardized research protocol, with responses recorded in real time. Each interview session lasted no more than 30 minutes.
Measurements
A sociodemographic questionnaire developed by the research team collected information on participants’ gender, age, place of residence, Residential status, education level, employment status, smoking history, and alcohol consumption. In addition, clinical data were extracted from electronic medical records, including the number of stroke episodes, duration since first stroke, homocysteine (Hcy) levels, thrombolysis status, and scores on the Modified Rankin Scale (mRS), National Institutes of Health Stroke Scale (NIHSS) scores, Charlson Comorbidity Index (CCI), and Trial of Org 10172 in Acute Stroke Treatment (TOAST) scores.
Capacity Factor: Disease Cognitive
Disease-related cognitive ability was assessed using the Stroke Prevention Knowledge Questionnaire (SPKQ), developed by Wan et al16 This instrument evaluates eight key dimensions related to stroke prevention: daily routines, diet, exercise, medication adherence, blood pressure monitoring, risk factors, stroke warning signs, and stroke management. The questionnaire consists of 36 items, each scored using a binary system, resulting in a total score ranging from 0 to 36. Higher scores reflect greater knowledge and understanding of stroke prevention. The SPKQ has demonstrated satisfactory internal consistency, with a Cronbach’s alpha of 0.738.
Motivational Factors: Depression (Emotion)
Depressive symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9), which was originally developed and validated by Kroenke et al17 The PHQ-9 consists of nine items, each rated on a 4-point Likert scale, with 0 point for “never” and 3 points for “always”. Total scores range from 0 to 27, calculated by summing the individual item scores. The scale demonstrated excellent internal consistency in this study, with a Cronbach’s alpha of 0.891.
Opportunity Factor: Social Support
Social support was assessed using the Social Support Rating Scale (SSRS) developed by Tang et al18 The scale consists of 10 items designed to evaluate three dimensions: objective support, subjective support, and the utilization of social support. Total scores range from 12 to 66 points, with higher scores indicating greater perceived social support. The SSRS demonstrated acceptable reliability in this study, with a Cronbach’s alpha of 0.731.
Behavior: Health Behavior
Health behaviors were assessed using the Health-Promoting Lifestyle Profile-II (HPLP-II), originally developed by Walker et al19 and culturally adapted by Zhang et al20 The instrument comprises 52 items across six dimensions: interpersonal relationships, stress management, physical activity, nutrition, self-actualization, and health responsibility. Responses were recorded on a 4-point Likert scale, yielding total scores ranging from 52 to 208 points. The scale demonstrated strong internal consistency in this study, with a Cronbach’s alpha of 0.901.
Statistical Analysis
Paper-based questionnaires were carefully reviewed by two independent reviewers and subsequently entered into Microsoft Excel 2021 to create a depression database for ischemic stroke follow-up patients. Latent growth mixture modeling (GMM) of depression trajectories was conducted using Mplus version 8.3. Model fit was evaluated using multiple indices, including the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), adjusted Bayesian Information Criterion (aBIC), entropy, the Lo-Mendell-Rubin Likelihood Ratio Test (LMRT), and the Bootstrapped Likelihood Ratio Test (BLRT). Lower AIC, BIC, and aBIC values indicate better model fit, while entropy values range from 0 to 1, with higher values reflecting greater classification accuracy. The LMRT and BLRT were used to compare models with different numbers of classes; statistically significant p-values for these tests indicate that a model with k classes fits the data better than a model with k-1 classes.
Data analysis was performed using IBM SPSS version 26. Descriptive statistics were based on the null hypothesis. Continuous variables that followed a normal distribution were presented as mean ± standard deviation. Between-group differences for continuous variables were assessed using F-tests. Categorical variables were expressed as frequencies and percentages, and comparisons between groups were conducted using chi-square tests. Analysis of variance (ANOVA) was initially applied to identify factors influencing depression trajectories in ischemic stroke patients. Subsequently, logistic regression analysis was performed with depression trajectory categories as the dependent variable to explore predictive factors across three dimensions: general information, cognitive ability, and behavioral opportunities. A p-value less than 0.05 was considered statistically significant.
Results
Participant Characteristics and Disease Information
The analysis included a total of 588 patients, with a mean age of 64.22 years (SD =11.72), and 68.2% were male. The majority of subjects did not undergo thrombolysis (89.3%). Large-artery atherosclerosis was the most common stroke subtype, accounting for 46.4% of cases. Unemployment status was reported in 51.7% of subjects, and educational attainment was generally low, with 70.7% having completed junior high school or below. Additional participant characteristics are detailed in Table 1.
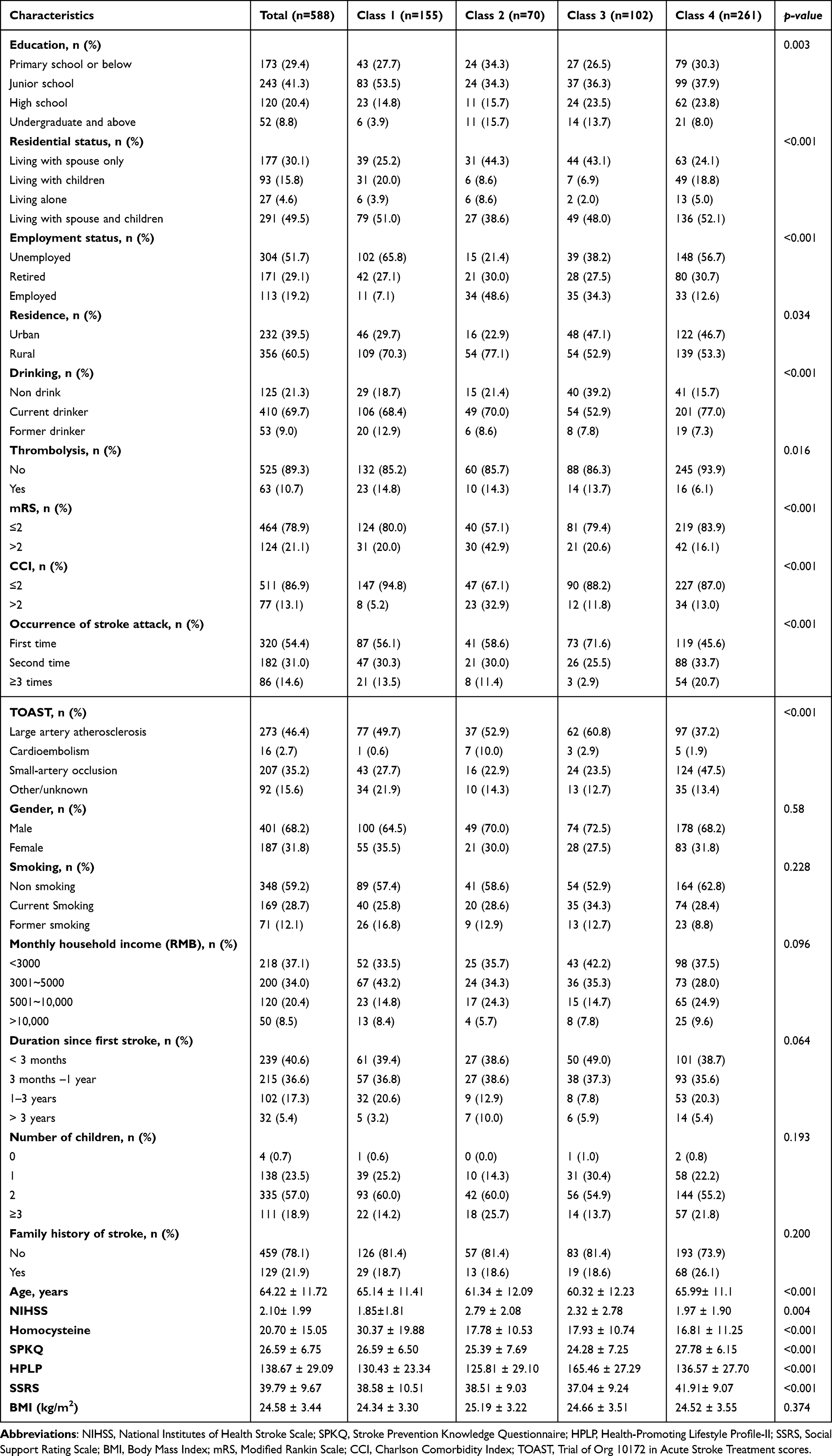 |
Table 1 Characteristics of Patients with Ischemic Stroke Across Depression Trajectory Groups (n=588) |
A COM-B Model-Based Univariate Analysis of Depression Trajectory Classifications
Significant differences were observed among the four depression trajectory groups across all three COM-B components (all p < 0.001). Specifically, the Persistent Low-Symptom Group (Class 3) had the lowest scores in Stroke Knowledge Questionnaire (SPKQ, 24.28 ± 7.25) and Social Support Rating Scale (SSRS, 37.04 ± 9.24), but the highest scores in Health Promotion Lifestyle Practices (HPLP, 165.46 ± 27.29). In contrast, the Symptom-Aggravation Group (Class 4) showed the highest SPKQ (27.78 ± 6.15) and SSRS (41.91 ± 9.07), while the Rapid Recovery Group (Class 1) and the Moderate Improvement Group (Class 2) had intermediate values. Additional participant characteristics are detailed in Table 1.
Depression Trajectories
Latent class growth mixture modeling (GMM) was employed to analyze depression trajectories over six time points in patients with ischemic stroke, with depression scores at each time point designated as variables. The analysis included 588 patients. Starting with a one-class model, the number of classes was incrementally increased, resulting in the fitting of five models. As the number of classes increased, values of the AIC, BIC, and aBIC progressively decreased. The LMRT, BLRT, and entropy values all favored the 4-class model (p < 0.05) (Table 2). Based on these fit indices and patient characteristics, the 4-class model was identified as optimal. Through latent class growth analysis, this study identified four depressive trajectory types among post-stroke patients. Class 1, the “Rapid Recovery Group” (26.4%), had the highest baseline depression levels but showed the greatest improvement. Class 2, the “Moderate Improvement Group” (11.9%), began at moderately elevated levels of depression and maintained a steady trajectory of improvement. Class 3, the “Persistent Low Symptoms Group” (17.3%), showed lower baseline levels and a stable, mild decline. Class 4, the “Symptom-Aggravation group” (44.4%), was the largest subgroup. Despite starting at lower levels, this group exhibited a marked upward trend in depressive symptoms over time, making early identification and intensive intervention critical for this population. The model fitting trajectory is illustrated in Figure 1.
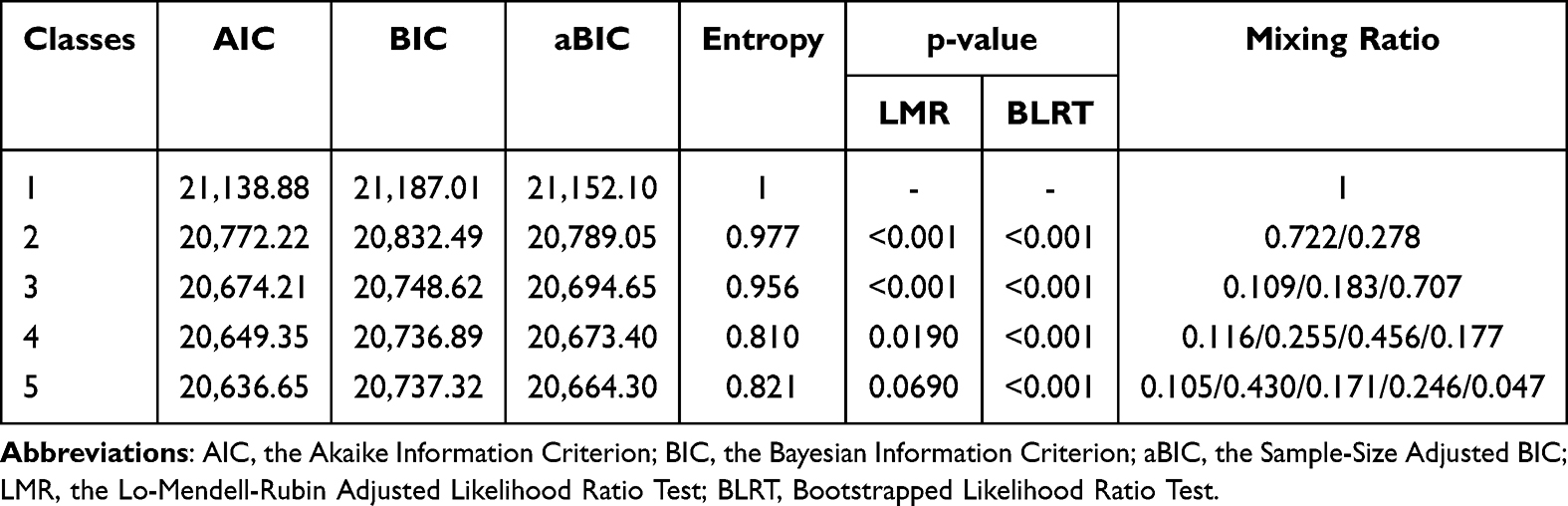 |
Table 2 Growth Mixture Model Fit Indices for One-to-Five-Classes of Depression Trajectories (n=588) |
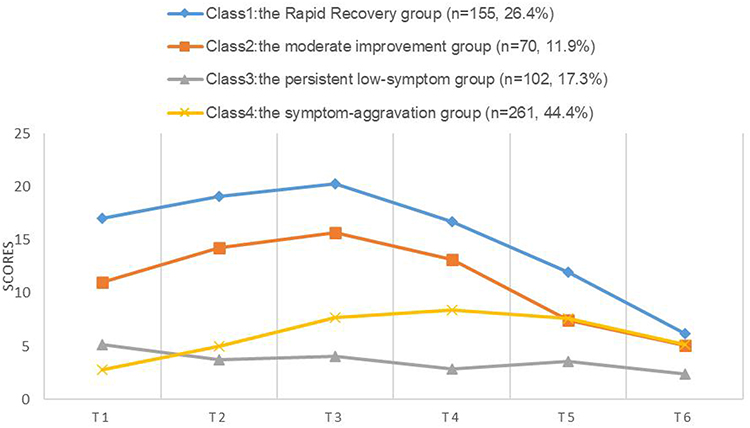 |
Figure 1 Trajectories of depression for the 4-class model. Note: The y-axis represents depression scores, and the x-axis represents time points (months). T1 indicates the baseline assessment during hospitalization; T2 to T6 represent follow-ups at 1, 3, 6, 9, and 12 months after discharge, respectively. |
Predictors of Depression Trajectory Among Patients with Ischemic Stroke
The present analysis treated the four categories of post-stroke depression as the dependent variable. The independent variables encompassed age, education level, residence, residential status, drinking history, employment status, thrombolytic therapy status, TOAST, occurrence of stroke attack, modified Rankin Scale (mRS) score, National Institutes of Health Stroke Scale (NIHSS) score, Charlson Comorbidity Index (CCI), and scores from three scales: The Stroke Prevention Knowledge Questionnaire (SPKQ), the Social Support Rating Scale (SSRS), and the Health-Promoting Lifestyle Profile-II (HPLP-II) are all grounded in the COM-B theoretical framework. Multivariate logistic regression analysis revealed that employment status, residence, residential status, occurrence of stroke attack, homocysteine levels, drinking history, SPKQ, and HPLP-II were significant predictors of post-stroke depression categories. The detailed results are presented in Table 3.
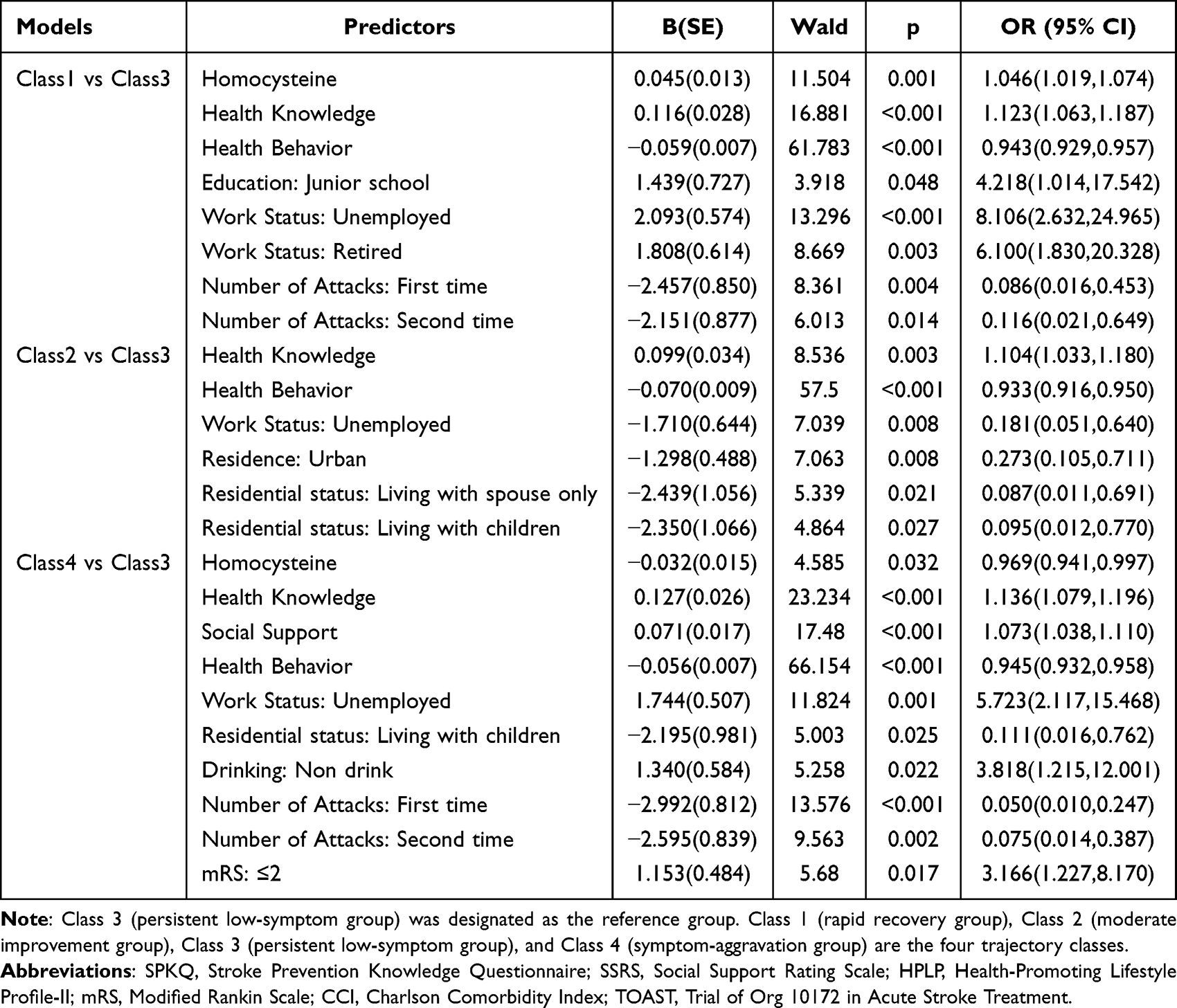 |
Table 3 Multivariate Logistic Regression for Predictors of Depression Trajectory Among Ischemic Stroke Patients (n=588) |
Discussion
The present prospective longitudinal study employed a growth mixture model to analyse depression trajectories among stroke patients over the subsequent 12 months, identifying four distinct depression categories. The results of the study indicated that the Symptom-Aggravation group constituted the largest proportion of the overall sample, with depression levels showing an upward trend over time. This finding is consistent with the research conducted by Huang et al7 Furthermore, this study corroborates the prevailing consensus that stroke survivors frequently exhibit depressive symptomatology, with the majority demonstrating an elevated risk of persistent depression, thereby validating the findings of preceding research.In contrast to the longitudinal study by Ayis et al on a general stroke population,21 the present study focused specifically on patients with H-type hypertension, used a 12-month trajectory, identified a novel “knowledge–behaviour gap”, and tested homocysteine levels as a predictor – none of which were addressed in earlier work.
The present study uncovers a fundamental contradiction that exerts a significant influence on the trajectories of depression following a stroke. The investigation reveals a considerable “knowledge-behaviour gap” between health knowledge and health behaviours. Contrary to common expectations, higher levels of health knowledge did not guide patients towards optimal recovery trajectories. Instead, they became a predictor of suboptimal trajectories. This phenomenon is particularly evident in the Symptom-Aggravation group, comprising patients who possess high health knowledge, abundant social support, and relatively good neurological function, yet paradoxically exhibit a persistent worsening of depressive symptoms. This finding indicates that when individuals encounter the predicament of “knowing but not doing,” the discrepancy between cognition and behaviour may itself become a risk factor, thereby exacerbating their psychological distress.22,23 In contrast, the adoption of positive health behaviours has been shown to offer a protective effect that supersedes the influence of knowledge, emerging as the most stable and potent protective factor across all comparisons of depression trajectories.24–26 This finding necessitates a reevaluation of clinical intervention priorities: For patients with sound physiological foundations yet persistent deterioration, the crux lies not in supplementing health knowledge but in employing behavioural activation strategies to bridge the gap between “knowing” and “doing”. It is imperative that clinical practice evolves from a focus on mere physiological monitoring and knowledge dissemination towards the identification of the “high knowledge-low execution” contradiction. The utilisation of psychological support methodologies, such as cognitive behavioural therapy, is imperative in order to facilitate the management of stress related to the disease and the adjustment of expectations. This approach is pivotal in disrupting the detrimental cycle whereby increased knowledge is purported to engender greater difficulty in action.
The findings of this study suggest that, in comparison to the Persistent Low Symptoms Group, individuals with elevated homocysteine levels, healthy lifestyle habits, and a reduced number of stroke episodes are more likely to be classified as part of the Rapid Recovery Group. The extant research27 suggests a correlation between anxiety in the early post-stroke period and the subsequent development of depression. It is hypothesised that elevated anxiety levels in the acute phase may result in an escalation in depression severity. However, this anxiety may be mitigated as the condition is effectively managed or the patient adapts to their circumstances.28,29 The study’s participants experienced heightened disease anxiety early on due to awareness of their prognosis, leading to temporarily elevated depression scores. However, consistent adherence to healthy behaviours facilitated clinical improvement over time, resulting in rapid depression remission. Notably, both the Rapid Recovery Group and the Symptom-Aggravation group had high unemployment rates (65.8% and 56.7%, respectively), yet their prognoses were opposite. Patients in both groups were generally older (mean age 65.1 years and 66.0 years, respectively), indicating that most unemployed individuals were unable to work due to age (reaching retirement age and exiting the labour force) rather than illness-related job loss. Thus, the direct negative impact of unemployment on prognosis was likely limited. The divergent outcomes can be explained by other factors: the Rapid Recovery Group had a higher proportion of first-ever strokes and better health behaviours, which offset the emotional burden of stroke; whereas the Symptom-Aggravation group had more recurrent strokes, poorer health behaviours, and less social support, leading to a vicious cycle. For such patients, it is recommended that disease information be supplemented with proactive behavioural guidance and psychological support. This approach facilitates the translation of health-related knowledge into consistent behavioural patterns, thereby mitigating the initial stages of disease-related anxiety and promoting the consolidation of expeditious recovery outcomes. Concurrently, the management of homocysteine levels is of equal importance.
By contrast, the prognosis for the moderate improvement group was more closely linked to socioeconomic factors. This group was more likely to be unemployed, live in an urban area, and live with a spouse or children. Employment offers economic security and, furthermore, fosters a sense of purpose and routine, thus playing a vital role in the maintenance of mental health.30 Urban environments are characterised by a greater number of opportunities for social interaction and community support, which can facilitate psychosocial adaptation.31 Concurrently, social support from family members, notably spouses and children, is indispensable in alleviating post-stroke depression, promoting emotional well-being, and providing practical assistance, rendering it crucial for the rehabilitation process.30 It is also worthy of note that the study identified that the absence of a spouse and children was indicative of a certain protective effect. This may be indicative of more independent or supportive family interaction patterns, rather than mere social isolation. It is hypothesised that such arrangements may assist patients in the more autonomous organisation of rehabilitation activities, according to their individual circumstances. This is believed to prevent the impact on self-management abilities caused by excessive dependence or family intervention. Consequently, clinical and community-based interventions should prioritise assisting patients in preserving and optimising their existing socioeconomic advantages and social support networks. With regard to family support, it is imperative to respect individual differences. The emphasis should be shifted from the concept of “cohabitation status” to the “quality” of supportive relationships. It is crucial to advocate for family environments that provide emotional support while respecting the patient’s autonomy in rehabilitation. In summary, the findings of this study emphasise the importance of integrating health knowledge education with behavioural interventions. The development of bespoke, diversified intervention strategies is imperative for cohorts exhibiting disparate risk profiles, with the objective of optimising comprehensive rehabilitation outcomes.
In the present study, although univariate analysis indicated a significant association between age, thrombolysis, CCI and TOAST classification with depression, these associations did not remain statistically significant in the final model. This finding indicates that, once the impact of other variables is taken into account, age, thrombolysis, CCI, and TOAST classification cease to be independent predictors of depression. This phenomenon may be attributed to the masking of the effects of age, thrombolysis, CCI, and TOAST classification by more pronounced effects of other variables within the model. Consequently, it is recommended that subsequent studies undertake a more comprehensive investigation of the association between age, thrombolysis, CCI and TOAST with depression, whilst also contemplating the validation of findings across a more substantial sample size.
Limitation
However, this study has some limitations. First, since all participants were recruited from a single hospital and followed for 12 months, there may be selection bias; moreover, most participants were from rural areas with limited education, which restricts generalizability to urban or more educated populations. Second, we did not collect information on depression-related treatments or supportive care during follow-up; therefore, the observed symptom trajectories reflect the course of depression under routine clinical care rather than untreated natural history. Future research should systematically assess the long-term effects of multidimensional intervention strategies in broader and more diverse populations with longer follow-up periods and better documentation of treatments received. A prospective, multicenter, long-term observational study will improve generalizability and reliability.
Conclusion
This study identified four distinct depressive symptom trajectories in ischemic stroke patients using a growth mixture model: rapid recovery, persistent low symptoms, symptom-aggravation, and moderate improvement. Positive health behaviours emerged as the most stable protective factor across all trajectories, while distinct risk profiles (eg., unemployment, social isolation, urban resources) characterized different subgroups. These findings highlight the need for early identification of high-risk individuals and personalized interventions addressing both health behaviours and psychosocial factors. Notably, the observed trajectories reflect courses under routine clinical care rather than untreated natural history, as information on depression-related treatment during follow-up was not collected.
Funding
This study was funded by the National Natural Science Foundation of China (grant numbers 72204225 and 72274179), the China Postdoctoral Science Foundation (grant number 2023M733234), the Medical Science and Technology Project of Henan Province (LHGJ20220429), and the Nursing Science Foundation of the First Affiliated Hospital of Zhengzhou University (grant number HLKY2023001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xiao W, Liu Y, Huang J, Huang L-A, Bian Y, Zou G. Analysis of factors associated with depressive symptoms in stroke patients based on a national cross-sectional study. Sci Rep. 2024;14(1):9268.
2. Lin F-H, Yih DN, Shih F-M, Chu C-M. Effect of social support and health education on depression scale scores of chronic stroke patients. Medicine. 2019;98(44):e17667.
3. Dou D-M, Huang -L-L, Dou J, Wang -X-X, Wang P-X. Post-stroke depression as a predictor of caregivers burden of acute ischemic stroke patients in China. Psychol Health Med. 2018;23(5):541–10.
4. Liu L, Xu M, Marshall IJ, Wolfe CD, Wang Y, O’Connell MD. Prevalence and natural history of depression after stroke: a systematic review and meta-analysis of observational studies. PLoS Med. 2023;20(3):e1004200.
5. Poddar R. Hyperhomocysteinemia is an emerging comorbidity in ischemic stroke. Exp Neurol. 2021;336:113541.
6. Guo J, Wang J, Sun W, Liu X. The advances of post-stroke depression: 2021 update. J Neurol. 2022;269(3):1236–1249.
7. Huang YJ, You JC, Wang Q, Wen W, Yuan CR. Trajectory and predictors of post-stroke depression among patients with newly diagnosed stroke: a prospective longitudinal study. J Stroke Cerebrovasc Dis. 2024;33(12):108092.
8. Tu W, Yan F, Chao B, Ji X, Wang L. Status of hyperhomocysteinemia in China: results from the China Stroke High-risk Population Screening Program, 2018. Front Med. 2021;15(6):903–912.
9. Gao N, Zhang Y, Li L, et al. Hyperhomocysteinemia-induced oxidative stress aggravates renal damage in hypertensive rats. Am J Hypertens. 2020;33(12):1127–1135.
10. Li G, Jing P, Chen G, et al. Development and validation of 3-month major post-stroke depression prediction nomogram after acute ischemic stroke onset. Clin Interv Aging. 2021;16:1439–1447.
11. Chen M, Wang M, Qiao M, et al. Determinants influencing health-promoting behaviors in individuals at high risks of stroke: a cross-sectional study. Front Public Health. 2024;12:1323277.
12. Michie S, Van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6(1):42.
13. Zhang MY, Guo LN, Namassevayam G, et al. Factors associated with health behaviours among stroke survivors: a mixed-methods study using COM-B model. J Clin Nurs. 2024;33(6):2138–2152.
14. Zhang X, Guo B, Zhu H, et al. H-type hypertension status and influencing factors of the elderly people over 80 years old based on random forest model. Int Heart J. 2024;65(2):263–270.
15. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379.
16. Wan L-H, Zhao J, Zhang X-P, et al. Stroke prevention knowledge and prestroke health behaviors among hypertensive stroke patients in mainland China. J Cardiovasc Nurs. 2014;29(2):E1–9.
17. Kroenke K, Henderson WR, Desrosiers A, et al. Reliability and validity of the Haitian Creole PHQ-9. J Gen Intern Med. 2014;29(12):1691. Capsule commentary on Marc.
18. Tang X, Li L, Yao K, et al. Association between social support and mutual-support needs among the rural adults in China: a cross-sectional study. Front Public Health. 2023;11:1171046.
19. Walker SN, Sechrist KR, Pender NJ. The health-promoting lifestyle profile: development and psychometric characteristics. Nurs Res. 1987;36(2):76–81.
20. Zhang X-P, Pan J-H, Wan L-H, et al. Factors influencing health behaviour, blood pressure control, and disability in hypertensive ischaemic stroke patients after a comprehensive reminder intervention. J Adv Nurs. 2020;76(6):1384–1393.
21. Ayis SA, Ayerbe L, Crichton SL, Rudd AG, Wolfe CDA. The natural history of depression and trajectories of symptoms long term after stroke: the prospective south London stroke register. J Affect Disord. 2016;194:65–71.
22. Platz T, editor. Clinical Pathways in Stroke Rehabilitation: Evidence-Based Clinical Practice Recommendations. Springer International Publishing; 2021.
23. Ito D, Mori N, Shimizu A, et al. Presence and Characteristics of Behavioral and Psychological Symptoms in Subacute Stroke Patients with Cognitive Impairment. Lei P, ed. Behav Neurol. 2023;2023:1–8.
24. Sharmin F, Hossain MF, Bari MU, et al. Impact of lifestyle factors on depression, anxiety, and functional recovery in ischemic stroke survivors in Bangladesh: a cross-sectional study. Discover Public Health. 2025;22(1):616.
25. Paprocka-Borowicz M, Wiatr M, Ciałowicz M, et al. Influence of physical activity and socio-economic status on depression and anxiety symptoms in patients after stroke. Int J Environ Res Public Health. 2021;18(15):8058.
26. Rahman MS, Adams J, Peng W, Sibbritt D. The impacts of a healthy lifestyle on the physical and mental health status of female stroke survivors in Australia. Top Stroke Rehabil. 2025;32(2):161–172.
27. Nelsone L, Rafsten L, Abzhandadze T, Sunnerhagen KS. A cohort study on anxiety and perceived recovery 3 and 12 months after mild to moderate stroke. Front Neurol. 2023;14:1273864.
28. Welten JJE, Cox VCM, Kruithof WJ, et al. Intra- and interpersonal effects of coping style and self-efficacy on anxiety, depression and life satisfaction in patient–partner couples after stroke. Neuropsychol Rehabil. 2023;33(5):849–870.
29. Aljuhani T, Alsubaie S, Al-Mutairi A, et al. Rate of post-stroke depression and associated factors in Saudi single tertiary medical center. J Multidiscip Healthc. 2025;18:5421–5430.
30. Cai Q, Qian M, Chen M. Association between socioeconomic status and post-stroke depression in middle-aged and older adults: results from the China health and retirement longitudinal study. BMC Public Health. 2024;24(1):1007.
31. Gurková E, Bartoníčková D, Šaňák D, Šaňáková Š, Zapletalová J, Štureková L. Relationship between social support, functional outcomes and health-related quality of life in working-aged adults at three months after ischemic stroke: results from the FRAILTY study. Health Qual Life Outcomes. 2025;23(1):8.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.