Back to Journals » Journal of Experimental Pharmacology » Volume 17
Toxicities Associated with Systemic Administration of Interleukin-6 in Wistar Albino Rats
Authors Nabisubi P ![]() , Mugasa CM, Matovu E, Ssekatawa K
, Mugasa CM, Matovu E, Ssekatawa K ![]() , Uwituze V, Ssentamu G, Namayanja M, Kato CD
, Uwituze V, Ssentamu G, Namayanja M, Kato CD ![]()
Received 23 March 2025
Accepted for publication 31 July 2025
Published 8 August 2025 Volume 2025:17 Pages 545—554
DOI https://doi.org/10.2147/JEP.S529995
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Abdelwahab Omri
Patricia Nabisubi,1,2 Claire M Mugasa,3 Enock Matovu,3 Kenneth Ssekatawa,4 Vanessa Uwituze,3 Geofrey Ssentamu,3 Monica Namayanja,3 Charles D Kato3
1African Center of Excellence in Bioinformatics and Data Intensive Science, the Infectious Disease Institute Makerere University, Kampala, Uganda; 2College of Health Science, Makerere University, Kampala, Uganda; 3School of Biosecurity, Biotechnical & Laboratory Sciences, College of Veterinary Medicine, Animal Resources & Biosecurity, Makerere University, Kampala, Uganda; 4Department of Science Technical and Vocational Education, College of Education and External Studies, Makerere University, Kampala, Uganda
Correspondence: Charles D Kato, College of Veterinary Medicine, Animal Resources & Biosecurity, Makerere University, P.O Box 7062, Kampala, Uganda, Tel +256-703320705, Email [email protected]
Background: Interleukin-6 is a pleiotropic cytokine being explored in therapy for cancer, trauma, and inflammatory infections, albeit with limited data about its safety. The main aim of this study was to investigate the toxicities associated with systemic administration of interleukin-6 in Wistar albino rats.
Methods: Four groups of rats, each containing six (6) animals received a daily intramuscular dose of 0.3mls of normal saline, 500ng/kg of recombinant interleukin-6, 1000ng/kg of Interleukin-6, and 2000ng/kg of Interleukin-6 for 21 days. On day 22 post-treatment, rats were euthanized, and blood and body organs were collected for analysis. Blood was used to determine liver and renal function, and hematology parameters, while liver and kidney tissue sections were used for histopathological analysis.
Results: The results revealed that systemic administration of interleukin-6 for 21 days significantly decreased levels of serum creatinine (p< 0.00) and serum urea (p< 0.01). IL-6 administration had no demonstrable effects on liver function across treatment groups We observed a significant decrease in lymphocytes numbers (p< 0.02) across treatment groups when compared to the negative control group. Platelets were significantly elevated in the 100ng/kg treatment groups as compared to the negative control and other treatment groups. Liver and kidney tissue sections for animals that received 500ng/kg of recombinant IL-10 were comparable to those of the negative control and at 1000 and 2000ng/kg, a dose-dependent increase in organ damage was evident.
Conclusion: We demonstrate that systemic administration of recombinant IL-6 at concentrations ranging between 500– 1000ng/kg is well tolerated, above this concentration, dose-dependent toxicities and adverse side effects becoming evident. It would be interesting to explore long-term toxicities associated with the systemic administration of IL-6.
Keywords: interleukin-6, hepatotoxicity, nephrotoxicity, Wistar albino rats, immunotherapy
Introduction
Interleukin-6 is a glycoprotein expressed by the interleukin-6 gene and acts as a pro-inflammatory cytokine by mediating fever and acute-phase response.1–3 Interleukin-6 enhances and increases blast cell colony formation, and hematopoiesis, and is important in megakaryocytic differentiation and associated with higher platelet production.4,5 In infectious diseases like human African trypanosomiasis, interleukin-6 is upregulated in late-stage patients and recommended as a therapeutic target.6,7 In this regard, several studies have demonstrated the therapeutic potential of Interleukin-6. In one study, IL-6 was shown to facilitate hepatocyte regeneration in liver toxicity.8 Interleukin-6 was demonstrated to promote megakaryocyte maturation and increase platelet recovery in cancer chemotherapy patients.9 Interleukin-6 has been shown as a prognostic indicator and provides a clinical perspective on Interleukin-6 blocking therapies in renal disease.10 Anti-interleukin-6 therapeutics can neutralize Interleukin-6 production in vivo and are safe and useful in inflammatory diseases, such as Castleman disease.1,11
Despite their use and recommendations as therapeutic agents, cytokine toxicities have been reported. Interferon-α is associated with fever fatigue, headache, gastrointestinal symptoms, and myalgia as well as the increase in hepatic enzymes, thrombocytopenia, leukopenia, and neutropenia12 including neuropsychiatric issues that include, confusion, depression, and mania13,14 and it may cause a permanent change of the immune system with the development of vitiligo and hypothyroidism.11,15 Interleukin-2 has been associated with capillary leak syndrome, which involves cardiac arrhythmias, myocarditis, reversible renal and hepatic dysfunction, hypotension, tachycardia, and pulmonary, peripheral edema secondary to third-space fluid accumulation. Interleukin-2 also causes fever, chills, fatigue, and gastrointestinal side effects such as vomiting, anorexia, transaminase elevation, cholestasis, electrolyte abnormalities, and diarrhea.13
High levels of IL-6 in serum have shown poor prognosis of tumor types like breast, renal, prostate, ovarian, and especially myeloma cells which start excreting high volumes of Interleukin-6 to act as an autocrine growth factor that promotes the growth of these cancer cells but this can be overcome by use of corticosteroids because they inhibit Interleukin-6.13 However, studies investigating the therapeutic and chemical properties of interleukin-6 have recommended Interleukin-6 as a therapeutic agent because Interleukin-6 plays a great role in the pathogenesis of various cancers, including prostate, breast, ovarian, and renal, in addition to B-malignancies, mostly myeloma. As a result of these observations, there have been ongoing clinical trials about Interleukin-6 like; Interleukin-6 with ovarian cancer therapy,16 Effects of Interleukin-6 on fetal hematopoietic progenitors,17,18 in vivo effects of recombinant human Interleukin-6 in primates; stimulated production of platelets,11 Administration of Interleukin-6 stimulates multilineage hematopoiesis and accelerates recovery from radiation-induced hematopoietic depression,19 Phase 1 trial of subcutaneous interleukin-6 in patients with advanced malignancies.20 In this study, we investigated the toxicities associated with systemic administration of interleukin-6 in Wistar albino rats.
Methodology
Experimental Design
We carried out an experimental study to investigate the effect of systemic administration of Interleukin-6 on hematological indices and liver and kidney function over 21 days. We utilized both male and female randomly selected Wistar albino rats that were acquired from the animal handling facility at the College of Veterinary Medicine, Animal Resources, and Biosecurity at Makerere University. A total of 24 rats of approximately 8 weeks of age and an average weight of 300 ± 5 g were housed in standard rat cages (Alibaba, China) for two (2) weeks to allow acclimatization in a controlled environment. The sample size of 24 rats was calculated using GitHub software as that giving a difference between means of 0.621 at a significant level alpha of 0.05, and power of 83%. Rats were housed under standard laboratory conditions of light, temperature (28±2°C), and relative humidity (55±5%) with an alternating light and dark cycle. The animals were fed on commercially available pelleted rat chow (Nuvita, Uganda), and water was provided ad-lib.
Rats were randomly divided into 4 groups, each with 6 animals, and treated with different drugs. The randomization was done with the help of the RandoMice randomization software.22 Briefly, group 1 worked as the negative control and received 0.3mls of normal saline (Sigma, USA). Group 2 received 500ng/kg recommended human dose23 of recombinant murine IL-6 (Biomatik, USA). Group 3 received 1000ng/kg of IL-6 while Group 4 received 2000ng/kg of recombinant Interleukin-6. Recombinant Interleukin-6 was administered intramuscularly (0.3mL) to all animals once daily for 21 days. On day 22 post-treatment, rats were euthanized by administering 100% carbon dioxide (CO2) as previously described.24 A 5mL blood sample was collected by cardiac puncture and serum was utilized for liver and kidney function biochemical assays. Total blood counts for white blood cell indices, red blood cell indices, and platelet counts were carried out. Liver and kidney tissues were collected and fixed in 10% formaldehyde for histological analysis.
Laboratory Procedures
Hematology Parameters
Haematological parameters like packed cell volume and complete blood count were performed on the blood samples. Complete blood count (CBC) is a blood test used to evaluate overall health and investigate various blood disorders, including anaemia, infection, and leukaemia. This test involves all blood parameters like red blood cell count for carrying oxygen in the body, white blood cell count fighting infection. We used this test to detect the effect of interleukin-6 on red blood cells and white blood cells as well and platelets. This test was performed by putting a well-mixed whole blood sample below the Sysmex machine to suck 1µL of blood that is analyzed and the results were printed out.
Clinical Chemistry Parameters (Liver Function Tests and Renal Function Tests)
Clinical chemistry is the measurement of chemical component of body fluids (urine and blood). Liver function tests included enzymes (AST, GGT, ALP, ALT), Proteins, and bilirubin, while renal function tests included urea, creatinine, creatinine clearance, microalbumin, sodium ions, potassium ions, and chloride ions. The blood sample was centrifuged to attain serum, and 4µL of serum was put into an Integra cup that was inserted into the COBAS Integra 400 machine. The machine sucks the serum as reagents interact with the serum and reactions are read as results and printed out at the end of the analysis. Therefore, the LFTs and RFTs were done to assess the effect of interleukin-6 on liver and kidney function.
Histopathological Analysis
After surgical removal, liver and kidney tissues were fixed in 10% formalin (Alibaba, China) for 2 days before analysis. Tissues were trimmed and loaded in cassettes and processed using a Histokinette (Leica, Germany) as previously described by.25 The processed tissues were embedded in molten paraffin wax, blocked on wooden blocks, trimmed, and sectioned using a Rotary Microtome (Baired and Tatlock, London), at 5µm thickness. The sections were later floated out on warm water in a water bath (Leica, Germany 1210) set at 44°C, dried and fixed on a glass slide in an oven set at 52°C for 48 hours. After which the sections were deparaffinized, stained with hematoxylin and eosin and then mounted using DPX (Distrene, plasticizer and xylene). Prepared slides were coded using numbers without showing the treatment groups and were analyzed by a Senior Pathologist at the College of Veterinary Medicine, Animal Resource and Biosecurity at Makerere University. Representative slides were later observed using a Carl Zeiss light microscope (Axiostar, Germany) for alterations in normal liver and kidney architecture. Photomicrographs were taken using a mounted digital camera (PowerShot, China) with ZoomBrowser EX version 2 imaging software.
Data Analysis
Data analysis was performed using GraphPad version 7 statistical software. We used the D’Agostino-Pearson normality test, as the data were normally distributed, parametric tests were used for group comparisons. Values for each group were expressed as mean ± SEM. The effect of the treatment on renal, liver, and haematology parameters among different groups was analyzed using a one-way ANOVA at a significant level α = 0.05. For groups where the one-way ANOVA results were significant, the Tukey Kramer Multiple Comparison test, set at a significance level α = 0.05 was used to compare every mean with every other mean.
Ethical Consideration
Ethical approval for this study was sought from the Institutional Review Board for the use of laboratory animals at the College of Veterinary Medicine, Animal Resources and Biosecurity at Makerere University (SBLS.CKD.2017). The Organization for Economic Co-operation and Development Environment Directorate guidelines for testing of chemicals in laboratory animals were strictly adhered to (OECD, 2001).
Results
Animal Characteristics After Treatment
Following the treatment, Interleukin-6 was generally well tolerated. No side effect was dose-limiting. Systemic symptoms such as fever, lethargy, fatigue, muscle wastage, tachycardia, and myalgias were the main side effects as these were observed in the 2000ng/kg group and 1000ng/kg. Additionally, cutaneous side effects consisting of a local reaction at the injection site of Interleukin-6 were observed.
Effect of Systemic Administration of Interleukin-6 on Liver Function
To determine the effect of administering Interleukin-6 systemically over 21 days, liver functional tests were assayed. Results showed that, Interleukin-6 treatment had no significant effect (p = 0.86, F (3, 20) = 1.9, Table 1) on Serum Total Bilirubin levels, serum direct bilirubin (p = 0.16, F (3, 20) = 0.6), Serum Glutamic Pyruvic Transaminase (p = 0.6, F (3, 20) = 0.7414), serum glutamic Oxaloacetic transaminase (p = 0.53, F (3, 20) = 0.7721), Alkaline phosphatase (p = 0.52, F (3, 20) = 1.285), Total protein (p = 0.31, F (3, 20) = 0.5824), Albumin (p = 0.63, F (3, 20) = 0.7225) and the Gamma-Glutamyl Transferase.
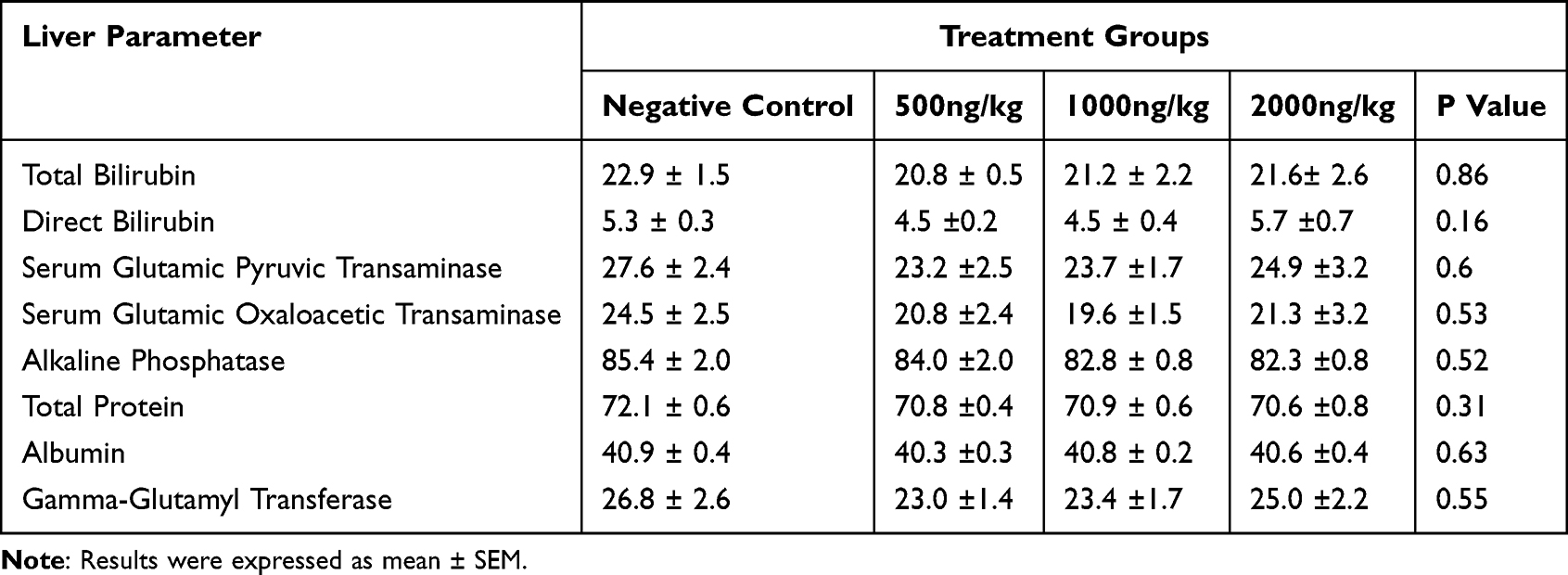 |
Table 1 Effect of Systemic Administration of Interleukin-6 on Liver Function |
Effect of Systemic Administration of Interleukin-6 on Kidney Function
To determine the effect of administering Interleukin-6 systematically over a 21-day period, kidney functional tests were assayed. The results revealed that Interleukin-6 treatment had a significant effect (p =0.0001, F (3, 20) = 11.8, Table 2) on serum creatinine levels and serum urea (p = 0.01, F (3, 20) = 4.8). On comparison between groups, serum creatinine levels showed a significant dose dependent reduction. The group receiving the highest dose of Interleukin-6 (2000ng/kg) showed significantly (P = 0.05) lower Serum Creatinine levels (70.8 ± 1.0µmol/l) as compared to the negative control (81.00 ± 1.8 µmol/l) and 500ng/l (79.2 ± 1.3 µmol/l) group. No significant difference was observed in Serum Creatinine levels between the negative control and the group receiving 500ng/kg of Interleukin-6.
 |
Table 2 Effect of Systemic Administration of Interleukin-6 on Kidney Function |
When serum urea levels were compared across treatment groups, similar dose-dependent reductions were observed. Serum urea levels were significantly (P = 0.05) reduced in the 200ng/l group (5.8 ± 0.4µmol/l) as compared to the negative control (8.1 ± 0.4µmol/l), 500ng/l (7.4 ± 0.5µmol/l) and 1000ng/l (6.6 ± 0.5µmol/l) groups. No significant differences were noted between the negative control group and the Interleukin-6 treatment groups at 500ng/kg and 1000ng/kg. The Interleukin-6 treatment did not have a significant effect on electrolyte levels, sodium levels (p = 0.13, F (3, 20) = 2.152), potassium levels (p = 0.13, F (3, 20) = 2.088), and chloride levels (p = 0.7, F (3, 20) = 0.4733).
Effect of Systemic Administration of Interleukin-6 on Haematological Indices
To determine the haematological effect of administering IL-6 systemically over 21 days, both white and red blood cell indices were measured (Table 3). Results from this study showed that systemic administration of IL-6 significantly affected lymphocyte numbers (p = 0.018, F (3, 20) = 4.2) and platelets (p = 0.01, F (3, 20) = 4.9). Comparison between groups showed significantly lower lymphocyte numbers in the 1000ng/kg (2.73 ± 1.18µmol/L) group compared to the negative control (6.95 ± 0.75µmol/L) group. Lymphocyte numbers did not significantly differ across other groups. Comparisons between platelet counts across the different groups revealed significantly (p = 0.05) higher numbers in the 1000ng/kg (545.7 ± 29.84µmol/L) group as compared to other groups. Platelet counts did not differ significantly across other groups. For other white and red blood cell haematological parameters, IL-6 administration did not have a significant effect.
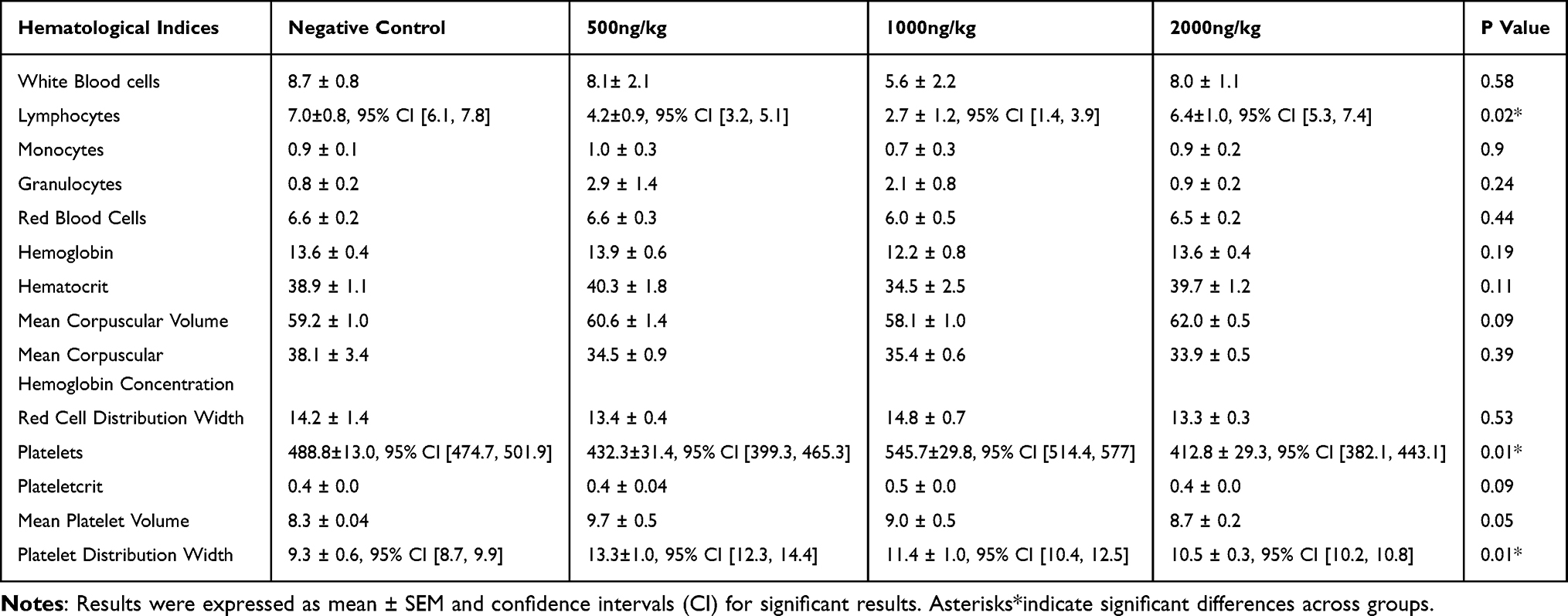 |
Table 3 Effect of Systemic Administration of Interleukin-6 on Hematological Indices |
Effect of Systemic Administration of Interleukin-6 on Kidney Histology
Histological examination of sections from the kidney cortex in the negative control group revealed the normal kidney architecture with visible renal corpuscles and convoluted tubules (Figure 1, plate 1) that were comparable to that of the 500ng/kg Interleukin-6 group (Figure 1, plate 2). A mild Interleukin-6 dose-dependent nephrotoxicity was observed in the 1000ng/kg (Plate 3), and 2000ng/kg (Plate 4) treatment groups. Nephrotoxicity was evidenced by mild proximal tubular necrosis, glomerular, and renal tubular degeneration tending with evidence of necrosis.
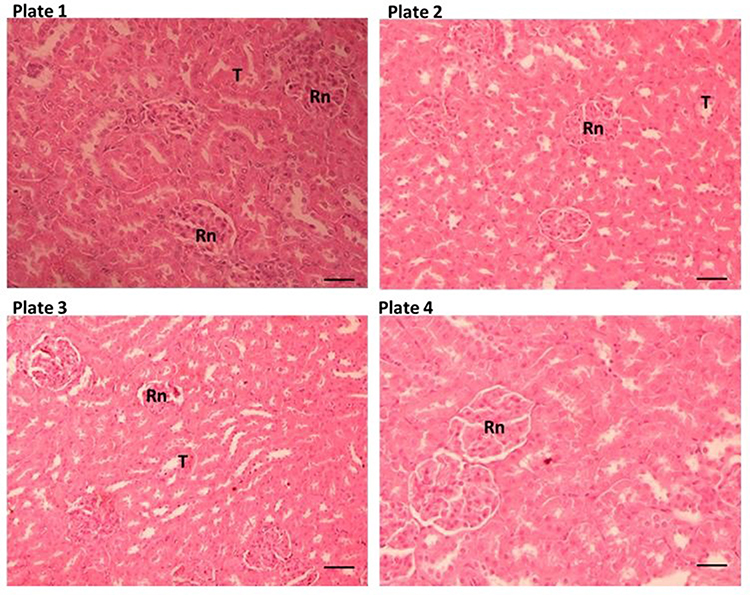 |
Figure 1 Transverse section through the kidney showing histopathological changes. Plate 1 (normal control group) shows a normal kidney architecture, note the renal corpuscle (Rn) deep in the cortex, the proximal convoluted tubules (T) are also clearly discernible and similar in plate 2 (500ng/kg group). Note the mild nephrotoxicity with mild disintegration of the renal tubules in the 1000ng/kg and 2000ng/kg groups. The scale bar is 25µm. |
Effects of Systemic Administration of Interleukin-6 on Liver Histology
Histology examination of the liver sections from the negative control group revealed the central vein with radiating hepatic cords, indicating normal liver lobular architecture (Figure 2, plate 1). The liver architecture of the 500ng/kg group Interleukin-6 was comparable to that of the negative control (Figure 2, plate 2). Liver sections from the 1000ng/kg (plate 3) and 2000ng/kg (plate 4) showed a mild dose-dependent deterioration in the liver architecture. The hallmark of this damage was indicated as hepatocyte degeneration, enlarged hepatocytes, and disintegration of hepatic cords.
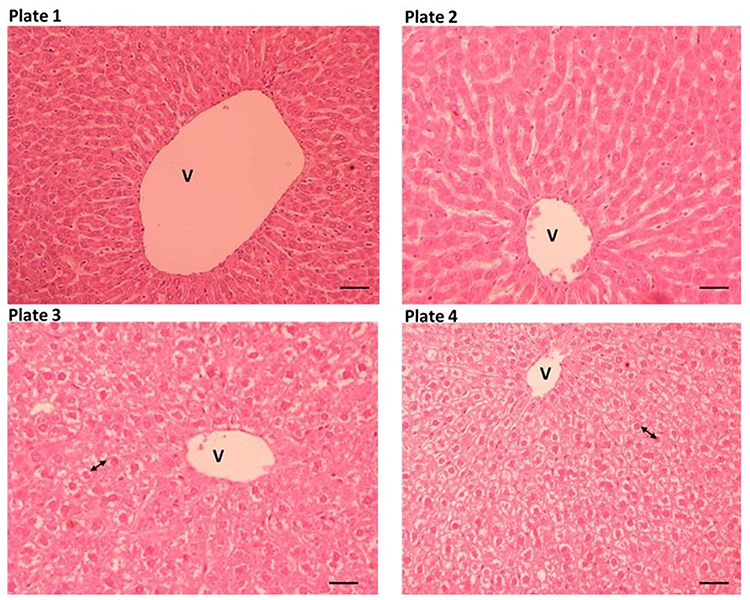 |
Figure 2 Transverse section through the liver showing histopathological changes. Plate 1 (normal control group) shows normal liver lobular architecture, note the central vein (V) with radiating hepatic cords that are very discernible and similar to plate 2 (500ng/kg group). Plate 3 (1000ng/kg group) and plate 4 (2000ng/kg group) showed mild disintegration of hepatic cords, enlarged and degenerating hepatocytes (arrowheads). The scale bar is 25µm. |
Discussion
Clinical trials have come up identifying Interleukin-6 as a therapeutic agent because Interleukin-6 plays a great function in the pathogenesis of various cancers, including prostate, breast, ovarian, and renal, in addition to B-malignancies, mostly myeloma; Interleukin-6 with ovarian cancer therapy,26,27 Effects of Interleukin-6 on fetal hematopoietic progenitors,17 in vivo effects of recombinant human Interleukin-6 in primates; stimulated production of platelets,11 Administration of Interleukin-6 stimulates multilineage hematopoiesis and accelerates recovery from radiation-induced hematopoietic depression,19 Use of interleukin-6 in treatment of severe COVID-19.28,29 Before a drug comes to market, its safety is very important. Our experiment was focused on determining the toxicity effect of systemic administration of recombinant interleukin-6 on clinical chemistry parameters, hematology parameters, and histology of the liver and the kidney.
Toxicity was dose-limiting at 2000ng/kg recombinant interleukin-6 because of a combination of headache, fever, myalgia, and chills.20 At low doses of 500ng/kg and 1000ng/kg, these signs were tolerated and are attributed to immune and acute phase responses, which are characterized by fever to Interleukin-6. Muscle wastage has been previously associated with Interleukin-6 due to its ability to stimulate protein breakdown at a high concentration of 2000ng/kg, thus the fever and accelerating peripheral lymphocytes and their precursors.30,31 Fatigue and lethargy have been associated with interleukin-6 secretion by the body cells,32 as well as tachycardia because interleukin-6 demonstrates the ability to stimulate the Hypothalamic-pituitary-adrenal axis, stimulating adrenocorticotropic hormone and corticosterone production that increase blood pressure.33 Similarly, infusion reactions have been observed with the intravenous administration of infliximab, a TNF-α antagonist.34 Among individuals receiving interferon alpha, flu-like symptoms with headache, nausea, fever, and chills have been reported.35 As described, there was no significant effect of Interleukin-6 on liver function tests in the results for the experiment even though there was an acute phase protein characterized by the fever that was seen in the animals albeit in this case, it was a positive acute phase protein thus the increase in the lymphocyte count in the 1000ng/kg IL-6 group.36,37 Though the liver tissue histopathology exhibited mild liver damage, which is supported by previous studies.38 Chronic exposure of IL-6 has been associated with impaired hepatic lipid metabolism,39 and recently in SARS-COV-2 patients, IL-6 has been associated with inducing liver inflammation and liver injury.40 Administration of IFN has been associated with glomerulonephritis, tubulo-interstitial nephritis, systemic lupus erythematosus-like syndrome, and in some cases, thrombotic microangiopathy.41 In acute renal failure, IL-10 has been shown to dysregulate monocytes, leading to a poor outcome among patients with acute renal failure.42 In our study, no renal toxicity was observed as determined by serum sodium, potassium, and chloride in line with previous studies43 though there was a significant decrease in serum creatinine and urea thus exhibited no effect on the kidney because low levels of urea in blood are not a cause for concern and not used to diagnose or monitor renal function. The low creatinine and urea levels observed in this case might have different causes. A urea reduction might be associated with the liver’s inability to metabolize ammonia, as the liver is critical in processing proteins and managing waste products. Inadequate protein intake might fail to provide the required substrates for urea production, thus lowering its levels.43 In this study, animals were fed on commercial feeds, and we did not confirm the protein levels in the feeds. Furthermore, overhydration has been shown to reduce urea levels.43 Low creatinine levels are also not for the diagnosis of renal function but in this case, it is might have resulted from muscular dystrophy or muscle wastage44,45
Interleukin-6, being a pleiotropic cytokine, was administered for three weeks in Wistar albino rats and increased platelet and lymphocyte counts in the 2000ng/kg treatment group. Megakaryocytopoiesis stimulation occurs at both an early and a late stage of differentiation. In the early steps of hematopoietic differentiation, several growth factors, including Interleukin-3 and GM-CSF, can induce proliferation and differentiation of the committed progenitor but are not specific to the megakaryocytic lineage. Interleukin-6 is one of the main stimulators at the late stages of megakaryocytic differentiation. In vitro, Interleukin-6 increases the ploidy and size of individual megakaryocytes.46 Moreover, at high dose levels, Interleukin-6 acts synergistically with Interleukin-3 in vitro to stimulate megakaryocytic proliferation and differentiation at early steps and Interleukin-6 alone does not affect megakaryocyte development. Preclinical studies in healthy primates have shown that in vivo administration of Interleukin-6 increased platelet production and induced a right shift in megakaryocytic DNA ploidy. The time to obtain a maximal effect on platelet production may reflect the time necessary to increase megakaryocytic ploidy and size in response to Interleukin-6, which in turn causes an increased efflux of platelets from the marrow. The shift of megakaryocyte ploidy appeared 1 week before maximal peripheral platelet counts. This delay is like that observed in primates47 in patients with advanced malignancies. Nevertheless, there is no definitive explanation for this delay in IL-6-induced increases in platelet counts. In our study, Interleukin-6 did not affect white blood cells and red blood cells as well as haemoglobin, which is in line with other previous animal studies.48
Our study has clinical implications that might guide subsequent clinical trials and IL-6 therapy. Several side effects have been observed during cytokine therapy that include hematologic, psychiatric, endocrine, neurologic, pulmonary, and dermatological.49 Interferon alpha administration has been associated with altered sleep patterns, anorexia, and fatigue.50 In this study, IL-6 therapy was associated with fever, fatigue, muscle wasting, and lethargy. The diverse nature of these side effects and toxicities would need to be weighed against the potential benefits of using IL-6 in therapy in a benefit-to-risk ratio. Furthermore, we show that a dose of 1000ng/kg and below seems to be well tolerated and could be explored in clinical trials and clinical settings. In addition, some of the reported side effects could be clinically managed through symptomatic treatment.
Our study has limitations. Firstly, we did not analyze for gender specific differences in cytokine levels across the study groups due to the uneven distribution of animals by gender across the study groups, yet gender has previously been shown to affect cytokine levels.51,52 We thus recommend that future studies explore the variations in toxicities across gender comprehensively. Secondly, we only considered subacute toxicities, and IL-6 administration might likely have chronic toxicities. Chronic IL-6 exposure has been associated with a disruption in normal CNS function,53 and aggravates fatty liver diseases by increasing lipogenesis.54
Conclusion
Our results have shown that recombinant interleukin-6 can be safely administered up to 1000ng/kg above which dose-limiting side effects are evident. As we did not investigate the efficacy of IL-6, it is likely that there might be potential benefits of high doses that might outweigh the observed side effects, and this necessitates further studies. To use IL-6 at higher doses, the benefit-to-risk ratio needs to be ascertained with concurrent symptomatic management of arising side effects. As we did not investigate the chronic toxicity associated with IL-6 administration, it is likely that either the toxicities might revert or that low doses might also prove to have serious effects. Therefore, future studies to explore the chronic toxicity associated with IL-6 administration in light of its efficacy are paramount.
Abbreviations
AST, Aspartate Aminotransferase; ALP, Alkaline phosphatase; ALT, Alanine Aminotransferase; CBC, Complete Blood Count; GGT, Gamma-glutamyl transferase; IL, Interleukin; LFTs, Liver Function Tests; PAMPs, Pathogen Associated Molecular Patterns; PRRs, Pattern Recognition Receptors; RFTs, Renal Function Tests.
Data Sharing Statement
Data associated with this study has been incorporated in this manuscript.
Ethical Approval and Consent to Publish
Ethical approval for this study was obtained from the Institutional Review Board for the use of laboratory animals at the College of Veterinary Medicine, Animal Resources and Biosecurity at Makerere University (SBLS.CKD.2017). The Organization for Economic Co-operation and Development Environment Directorate guidelines for testing of chemicals in laboratory animals were strictly adhered to (OECD, 2001).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no competing interests in this work.
References
1. Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. 2014;6(10):a016295. doi:10.1101/cshperspect.a016295
2. Kang S, Tanaka T, Narazaki M, Kishimoto T. Targeting interleukin-6 signaling in clinic. Immunity. 2019;50(4):1007–1023. doi:10.1016/j.immuni.2019.03.026
3. Le RQ, Li L, Yuan W, et al. FDA approval summary: tocilizumab for treatment of chimeric antigen receptor t cell-induced severe or life-threatening cytokine release syndrome. oncologist. 2018;23(8):943–947. doi:10.1634/theoncologist.2018-0028
4. Malara A, Abbonante V, Di Buduo CA, Tozzi L, Currao M, Balduini A. The secret life of a megakaryocyte: emerging roles in bone marrow homeostasis control. Cell Mol Life Sci CMLS. 2015;72(8):1517–1536. doi:10.1007/s00018-014-1813-y
5. Reems J-A, Pineault N, Sun S. In vitro megakaryocyte production and platelet biogenesis: state of the art. Transfus Med Rev. 2010;24(1):33–43. doi:10.1016/j.tmrv.2009.09.003
6. Nyawira Maranga D, Kagira JM, Kinyanjui CK, Muturi Karanja S, Wangari Maina N, Ngotho M. IL-6 is upregulated in late-stage disease in monkeys experimentally infected with Trypanosoma brucei rhodesiense. Clin Dev Immunol. 2013;2013:320509. doi:10.1155/2013/320509
7. Kato CD, Alibu VP, Nanteza A, Mugasa CM, Matovu E. Interleukin (IL)-6 and IL-10 are up regulated in late stage Trypanosoma brucei rhodesiense sleeping sickness. PLoS Negl Trop Dis. 2015;9(6):e0003835. doi:10.1371/journal.pntd.0003835
8. Widjaja AA, Chothani SP, Cook SA. Different roles of interleukin 6 and interleukin 11 in the liver: implications for therapy. Hum Vaccines Immunother. 2020;16(10):2357–2362. doi:10.1080/21645515.2020.1761203
9. Kuter DJ. Treatment of chemotherapy-induced thrombocytopenia in patients with non-hematologic malignancies. Haematologica. 2022;107(6):1243–1263. doi:10.3324/haematol.2021.279512
10. Jones SA, Fraser DJ, Fielding CA, Jones GW. Interleukin-6 in renal disease and therapy. Nephrol Dial Transplant off Publ Eur Dial Transpl Assoc. 2015;30(4):564–574. doi:10.1093/ndt/gfu233
11. Rossi J-F, Chiang H-C, Lu Z-Y, et al. Optimisation of anti-interleukin-6 therapy: precision medicine through mathematical modelling. Front Immunol. 2022;13:919489. doi:10.3389/fimmu.2022.919489
12. Conlon KC, Miljkovic MD, Waldmann TA. Cytokines in the Treatment of Cancer. J Interferon Cytokine Res. 2019;39(1):6–21. doi:10.1089/jir.2018.0019
13. Lee S, Margolin K. Cytokines in cancer immunotherapy. Cancers. 2011;3(4):3856–3893. doi:10.3390/cancers3043856
14. Potere N, Batticciotto A, Vecchié A, Porreca E, Cappelli A, Abbate A. The role of IL-6 and IL-6 blockade in COVID-19: expert review of clinical immunology: vol 17, no 6 - get access. Available from: https://www.tandfonline.com/doi/full/10.1080/1744666X.2021.1919086?scroll=top&needAccess=true.
15. Custurone P, Di Bartolomeo L, Irrera N, et al. Role of cytokines in vitiligo: pathogenesis and possible targets for old and new treatments. Int J Mol Sci. 2021;22(21):11429. doi:10.3390/ijms222111429
16. Nenu I, Toadere TM, Topor I, et al. Interleukin-6 in hepatocellular carcinoma: a dualistic point of view. Biomedicines. 2023;11(10):2623. doi:10.3390/biomedicines11102623
17. Bernad A, Kopf M, Kulbacki R, Weich N, Koehler G, Gutierrez-Ramos JC. Interleukin-6 is required in vivo for the regulation of stem cells and committed progenitors of the hematopoietic system. Immunity. 1994;1(9):725–731. doi:10.1016/s1074-7613(94)80014-6
18. Gardner JD, Liechty KW, Christensen RD. Effects of interleukin-6 on fetal hematopoietic progenitors. Blood. 1990;75(11):2150–2155. doi:10.1182/blood.V75.11.2150.2150
19. Patchen ML, MacVittie TJ, Williams JL, Schwartz GN, Souza LM. Administration of interleukin-6 stimulates multilineage hematopoiesis and accelerates recovery from radiation-induced hematopoietic depression. Blood. 1991;77(3):472–480. doi:10.1182/blood.V77.3.472.472
20. Weber J, Yang JC, Topalian SL, et al. Phase I trial of subcutaneous interleukin-6 in patients with advanced malignancies. J Clin Oncol off J Am Soc Clin Oncol. 1993;11(3):499–506. doi:10.1200/JCO.1993.11.3.499
21. Hailemichael Y, Johnson DH, Abdel-Wahab N, et al. Interleukin-6 blockade abrogates immunotherapy toxicity and promotes tumor immunity. Cancer Cell. 2022;40(5):509–523. doi:10.1016/j.ccell.2022.04.004
22. van Eenige R, Verhave PS, Koemans PJ, Tiebosch IA, Rensen PC, Kooijman S. RandoMice, a novel, user-friendly randomization tool in animal research. PLoS One. 2020;15(8):e0237096. doi:10.1371/journal.pone.0237096
23. Jacobs K, Godwin J, Foster M, et al. Lead-in dose optimization to mitigate cytokine release syndrome in aml and mds patients treated with flotetuzumab, a CD123 x CD3 dart® molecule for T-cell redirected therapy. Blood. 2017;130:3856. doi:10.1182/blood.V130.Suppl_1.3856.3856
24. Hickman DL, Fitz SD, Bernabe CS, et al. Evaluation of low versus high volume per minute displacement CO2 methods of euthanasia in the induction and duration of panic-associated behavior and physiology. Anim Open Access J MDPI. 2016;6(8):45. doi:10.3390/ani6080045
25. tissue processing overview: steps & techniques for histopathology. Available from: https://www.leicabiosystems.com/knowledge-pathway/an-introduction-to-specimen-processing/.
26. Masjedi A, Hashemi V, Hojjat-Farsangi M, et al. The significant role of interleukin-6 and its signaling pathway in the immunopathogenesis and treatment of breast cancer. Biomed Pharmacother. 2018;108:1415–1424. doi:10.1016/j.biopha.2018.09.177
27. Soler MF, Abaurrea A, Azcoaga P, Araujo AM, Caffarel MM. New perspectives in cancer immunotherapy: targeting IL-6 cytokine family. J Immunother Cancer. 2023;11(11):e007530. doi:10.1136/jitc-2023-007530
28. Aziz M, Fatima R, Assaly R. Elevated interleukin‐6 and severe COVID‐19: a meta‐analysis. J Med Virol. 2020;92(11):2283–2285. doi:10.1002/jmv.25948
29. Lagunas‐Rangel FA, Chávez‐Valencia V. High IL‐6/IFN‐γ ratio could be associated with severe disease in COVID‐19 patients. J Med Virol. 2020;92(10):1789–1790. doi:10.1002/jmv.25900
30. Muñoz‐Cánoves P, Scheele C, Pedersen BK, Serrano AL. Interleukin‐6 myokine signaling in skeletal muscle: a double‐edged sword? Febs J. 2013;280(17):4131–4148. doi:10.1111/febs.12338
31. Pedersen BK, Steensberg A, Schjerling P. Muscle-derived interleukin-6: possible biological effects. J Physiol. 2001;536(Pt 2):329. doi:10.1111/j.1469-7793.2001.0329c.xd
32. Grygiel-Górniak B, Puszczewicz M. Fatigue and interleukin-6 - a multi-faceted relationship. Reumatologia. 2015;53(4):207–212. doi:10.5114/reum.2015.53998
33. Drummond JB, Soares BS, Vieira EL, Pedrosa W, Teixeira AL, Ribeiro-Oliveira A Jr. Interleukin-6 response to insulin-induced hypoglycemia is associated with hypothalamic-pituitary-adrenal axis activation. Journal of Neuroimmunology. 2021;350:577446. doi:10.1016/j.jneuroim.2020.577446
34. Jang DI, Lee AH, Shin HY, et al. The role of tumor necrosis factor alpha (TNF-α) in autoimmune disease and current TNF-α inhibitors in therapeutics. Int J Mol Sci. 2021;22(5):2719. doi:10.3390/ijms22052719
35. Sleijfer S, Bannink M, Van Gool AR, Kruit WH, Stoter G. Side effects of interferon-alpha therapy. Pharm World Sci. 2005;27(6):423–431. PMID: 16341948. doi:10.1007/s11096-005-1319-7
36. Cray C. Acute Phase Proteins in Animals. Prog Mol Biol Transl Sci. 2012;105:113–150. doi:10.1016/B978-0-12-394596-9.00005-6
37. Anaya J-M, Castiblanco J, Rojas-Villarraga A, et al. The multiple autoimmune syndromes. A clue for the autoimmune tautology. Clin Rev Allergy Immunol. 2012;43(3):256–264. doi:10.1007/s12016-012-8317-z
38. D’Hondt V, Humblet Y, Guillaume T, et al. Thrombopoietic effects and toxicity of interleukin-6 in patients with ovarian cancer before and after chemotherapy: a multicentric placebo-controlled, randomized phase ib study. Blood. 1995;85(9):2347–2353. doi:10.1182/blood.V85.9.2347.bloodjournal8592347
39. Li H, Liu NN, Li JR, et al. Bicyclol ameliorates advanced liver diseases in murine models via inhibiting the IL-6/STAT3 signaling pathway. Biomed Pharmacother. 2022;150:113083. doi:10.1016/j.biopha.2022.113083
40. McConnell MJ, Kawaguchi N, Kondo R, et al. Liver injury in COVID-19 and IL-6 trans-signaling-induced endotheliopathy. J Hepatol. 2021;75:647–658. doi:10.1016/j.jhep.2021.04.050
41. Gianassi I, Allinovi M, Caroti L, Cirami LC. Broad spectrum of interferon-related nephropathies-glomerulonephritis, systemic lupus erythematosus-like syndrome and thrombotic microangiopathy: a case report and review of literature. World J Nephrol. 2019;8(7):109. doi:10.5527/wjn.v8.i7.109
42. Roth K, Strickland J, Pant A, et al. Interleukin-10 disrupts liver repair in acetaminophen-induced acute liver failure. Front Immunol. 2023;14:1303921. doi:10.3389/fimmu.2023.1303921
43. Hosten AO. BUN and creatinine. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations.
44. Kreiner FF, Kraaijenhof JM, von Herrath M, Hovingh GKK, von Scholten BJ. Interleukin 6 in diabetes, chronic kidney disease, and cardiovascular disease: mechanisms and therapeutic perspectives. Expert Rev Clin Immunol. 2022;18(4):377–389. doi:10.1080/1744666X.2022.2045952
45. Stephens C. low creatinine: causes, symptoms, treatments. available from: https://www.healthline.com/health/low-creatinine#causes-and-symptoms.
46. Shahbaz H, Rout P, Gupta M. Creatinine Clearance. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024. Available from http://www.ncbi.nlm.nih.gov/books/NBK544228/.
47. Velazquez-Salinas L, Verdugo-Rodriguez A, Rodriguez LL, Borca MV. The role of interleukin 6 during viral infections. Front Microbiol. 2019;10. doi:10.3389/fmicb.2019.01057
48. Laterveer L, van Damme J, Willemze R, Fibbe WE. Continuous infusion of interleukin-6 in sublethally irradiated mice accelerates platelet reconstitution and the recovery of myeloid but not of megakaryocytic progenitor cells in bone marrow. Exp Hematol. 1993;21(13):1621–1627. PMID: 8243564.
49. Baldo BA. Side effects of cytokines approved for therapy. Drug Safety. 2014;37(11):921–943. doi:10.1007/s40264-014-0226-z
50. Hauser P, Khosla J, Aurora H, et al. A prospective study of the incidence and open-label treatment of interferon-induced major depressive disorder in patients with hepatitis C. Mol Psychiatry. 2002;7(9):942–947. doi:10.1038/sj.mp.4001119
51. Marusich JA, Gay EA, Stewart DA, Blough BE. Sex differences in inflammatory cytokine levels following synthetic cathinone self-administration in rats. Neurotoxicology. 2022;88:65–78. doi:10.1016/j.neuro.2021.11.002
52. Wegner A, Benson S, Rebernik L, et al. Sex differences in the pro-inflammatory cytokine response to endotoxin unfold in vivo but not ex vivo in healthy humans. Innate Immunity. 2017;23(5):432–439. doi:10.1177/1753425917707026
53. Nelson TE, Ur CL, Gruol DL. Chronic interleukin-6 exposure alters electrophysiological properties and calcium signaling in developing cerebellar purkinje neurons in culture. J Neurophysiol. 2002;88(1):475–486. doi:10.1152/jn.2002.88.1.475
54. Vida M, Gavito AL, Pavón FJ, et al. Chronic administration of recombinant IL-6 upregulates lipogenic enzyme expression and aggravates high-fat-diet-induced steatosis in IL-6-deficient mice. Dis Models Mech. 2015;8(7):721–731.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Simultaneous Determination of Unbound Plasma Concentration of Methotrexate and 7-Hydroxymethotrexate in Children Patients Receiving High-Dose Methotrexate Therapy

Dong WC, Gao SS, Shi B, Li HR, Jiang Y, Guo JL, Zhang ZQ, Zhang YZ
Drug Design, Development and Therapy 2025, 19:4383-4396
Published Date: 26 May 2025