Back to Journals » Clinical and Experimental Gastroenterology » Volume 19
Toward Integrated Care for Neurogastroenterology and Motility Disorders: A Model for Clinical Practice
Authors Veldman FHC ![]() , Sweerts KWE, Leue C, Brouns J
, Sweerts KWE, Leue C, Brouns J ![]() , Mulkens S, Brans Brabant B, Beckers RCJ, Conchillo JM, Keszthelyi D
, Mulkens S, Brans Brabant B, Beckers RCJ, Conchillo JM, Keszthelyi D
Received 14 November 2025
Accepted for publication 28 February 2026
Published 20 March 2026 Volume 2026:19 581482
DOI https://doi.org/10.2147/CEG.S581482
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Vipul Yagnik
Fleur HC Veldman,1,2,* Kim WE Sweerts,1,3,* Carsten Leue,4,5 Jenny Brouns,6 Sandra Mulkens,7 Bo Brans Brabant,8 Rianne CJ Beckers,1,3 José M Conchillo,1,2 Daniel Keszthelyi1,2
1Department of Gastroenterology-Hepatology, Maastricht University Medical Center, Maastricht, the Netherlands; 2Institute of Nutrition and Translational Research in Metabolism, Faculty of Health Medicine and Life Sciences, Maastricht University, Maastricht, the Netherlands; 3Institute for Oncology and Reproduction, Faculty of Health Medicine and Life Sciences, Maastricht University, Maastricht, the Netherlands; 4Department of Psychiatry, Maastricht University Medical Center, Maastricht, the Netherlands; 5Institute of Mental Health and Neuroscience, Faculty of Health, Medicine, and Life Sciences, Maastricht University, Maastricht, the Netherlands; 6Department of Nutrition and Dietetics, Maastricht University Medical Center, Maastricht, the Netherlands; 7Department of Clinical Psychological Science, Faculty of Psychology and Neuroscience, Maastricht University, Maastricht, the Netherlands; 8Department of Physical Therapy, Maastricht University Medical Center, Maastricht, the Netherlands
*These authors contributed equally to this work
Correspondence: Fleur HC Veldman, Department of Gastroenterology-Hepatology, Maastricht University Medical Center, PO Box 616, Maastricht, 6200 MD, the Netherlands, Tel +31433884051, Email [email protected]
Abstract: Integrated care refers to the coordinated delivery of health services across providers and settings, aimed at ensuring continuous, patient-centered care throughout the course of disease. Models of integrated care have demonstrated particular relevance in the management of gastrointestinal (GI) diseases, such as disorders of gut-brain interaction (DGBI) and inflammatory bowel disease (IBD), due to their multidimensional nature. Integrated care has the potential not only to alleviate symptom burden, but also to improve quality of life and mental health outcomes while reducing healthcare costs. Nevertheless, barriers to implementation persist, and despite growing recognition of its value, integrated care has not yet been systematically adopted for GI motility disorders. These disorders, thought to be multifactorial, exhibit considerable overlap with DGBI, rendering them clinically indistinguishable in some cases. Furthermore, while mental health problems are well recognized in DGBI, they are also commonly observed in individuals with GI motility disorders. In response, Maastricht University Medical Centre+ has developed a multidisciplinary, integrated, patient-centered care model for the diagnosis and management of neurogastroenterology and motility disorders. By presenting this approach, we aim to foster knowledge exchange and support the development of integrated care models adaptable to the specific needs of diverse healthcare settings.
Keywords: integrated care, patient-centered care, GI motility disorders, disorders of gut-brain interaction
Background
Integrated care models, in which multidisciplinary teams work collaboratively, have gained increasing clinical relevance for diagnosing and managing patient outcomes.1,2 Integrated care can be conceptualized as comprising two key elements: first, fragmented aspects of care must be brought together (“integrated”); and second, it must ensure delivery of treatment to individuals in need (“care”).3 Although no single, universally accepted definition exists, from a health system-based perspective, integrated care has been described as
Health services that are managed and delivered so that people receive a continuum of health promotion, disease prevention, diagnosis, treatment, disease management, rehabilitation and palliative care services, coordinated across different levels and sites of care within and beyond the health sector, and according to their needs throughout the life course.4
Multidisciplinary integrated care may therefore yield superior long-term outcomes at both the individual and population levels by reducing outpatient visits, hospital admissions, and associated direct and indirect healthcare costs.1,5–7
Integrated care is particularly relevant in gastroenterology, as gastrointestinal (GI) disorders often involve not only GI symptoms but also contributing factors such as psychological comorbidities, necessitating a multidimensional and integrated approach for effective management.2,6,8,9 In this context, integrated care approaches typically involve allied health professionals, including dedicated dietitians, psychologists, (pelvic) physical therapists, speech therapists, and specialist nurses, working collaboratively with medical doctors such as gastroenterologists and psychiatrists, to provide holistic patient care.6 These models are most extensively described in the management of disorders of gut-brain interaction (DGBI), particularly irritable bowel syndrome (IBS), as they aim to address GI symptoms alongside nutritional factors and brain-gut behavior-targeted therapies.2,10,11
Several benefits of integrated care have been reported, as it may improve not only GI symptoms but also psychological well-being and quality of life, while enhancing patient safety, satisfaction, and resource utilization.1,9,12 Supporting this, an unblinded randomized study by Basnayake et al involving 188 IBS patients demonstrated that multidisciplinary integrated care outperforms gastroenterologist-only care in improving symptoms, quality of life, mental health, and cost-effectiveness.11 Importantly, these advances appear to derive not from the individual interventions (eg, pharmacological, dietary, psychological interventions), but rather from the structured delivery of integrated care itself.8,11 Furthermore, open communication among team members further facilitates shared identification of clinical issues and personalized, collaborative decision-making.2 Taken together, integrated care offers a sustainable model that promotes timely diagnosis, comprehensive management, and improved patient outcomes.
Consequently, integrated care is increasingly recognized as the conventional approach for managing a range of GI disorders, including DGBI, inflammatory bowel disease (IBD), and fecal incontinence.1,5,6,8–10,13 However, a systematic review by Warner et al found that no standardized model currently exists, as integrated care approaches vary in the composition of care teams, therapies provided, and modes of delivery (eg, face-to-face or online).6 Furthermore, several barriers to implementation persist, including limited time for holistic care, predominant resilience on pharmacological treatments, inadequate training of personnel, and restricted access to specialized dietary, psychological, and physical therapies.2 Consequently, significant gaps remain in understanding how integrated care models can be effectively implemented in daily clinical practice.6
These barriers are particularly evident in GI motility disorders, where the implementation of integrated care models remains limited. This gap is of particular concern in gastroparesis, a GI motility disorder increasingly recognized as multifactorial in origin and clinically complex, which imposes substantial symptom and economic burdens, thereby underscoring the need for interdisciplinary management.14–16 Consistent with this, a study by the Gastroparesis Clinical Research Consortium reported that patients with gastroparesis and those with functional dyspepsia, a DGBI, could not be reliable distinguished based on clinical symptoms or pathophysiological features in tertiary care settings.17 Similarly, Huang et al investigated the worldwide prevalence and burden of gastroparesis-like symptoms and reported substantial overlap with DGBI.15 Given this growing recognition of clinical overlap between DGBI and motility disorders, it is therefore logical to develop an integrated care model encompassing both groups of disorders. In addition to the overlapping GI symptoms, mental health problems (eg, anxiety disorders and depression) or comorbid eating disorders (eg, Avoidant/Restrictive Food Intake Disorder) are not exclusive to DGBI but are commonly observed in GI motility disorders as well.18 Indeed, Hasler et al found that comorbid anxiety disorders and depression in gastroparesis are associated with greater symptom severity, although psychological dysfunction appears unrelated to disease etiology or severity of gastric retention19 Likewise, life satisfaction in IBS was independently associated with psychological burden, but not gastrointestinal symptom severity, reinforcing the clinical need to focus on the full extent of the disorder.20
Together, these findings underscore the need for effective diagnostic and treatment strategies, for which integrated care represents a promising approach. At our tertiary neurogastroenterology and motility center, we implemented an integrated care model for GI motility disorders that considers DGBI overlap. This model engages multiple healthcare professionals and incorporates a range of treatment modalities, resulting in a personalized diagnostic and therapeutic pathway for each patient. In this commentary, we present our approach to foster knowledge exchange and support other centers in developing models tailored to their specific care landscapes for neurogastroenterology and motility disorders.
Integrated Care Approach
The Maastricht University Medical Centre+ (MUMC+) is a tertiary referral center, and the Department of Gastroenterology and Hepatology is specialized in neurogastroenterology and motility (NGM) disorders. The integrated care model (Figure 1) illustrates the referral process as well as the subsequent multidisciplinary diagnostic and management steps.
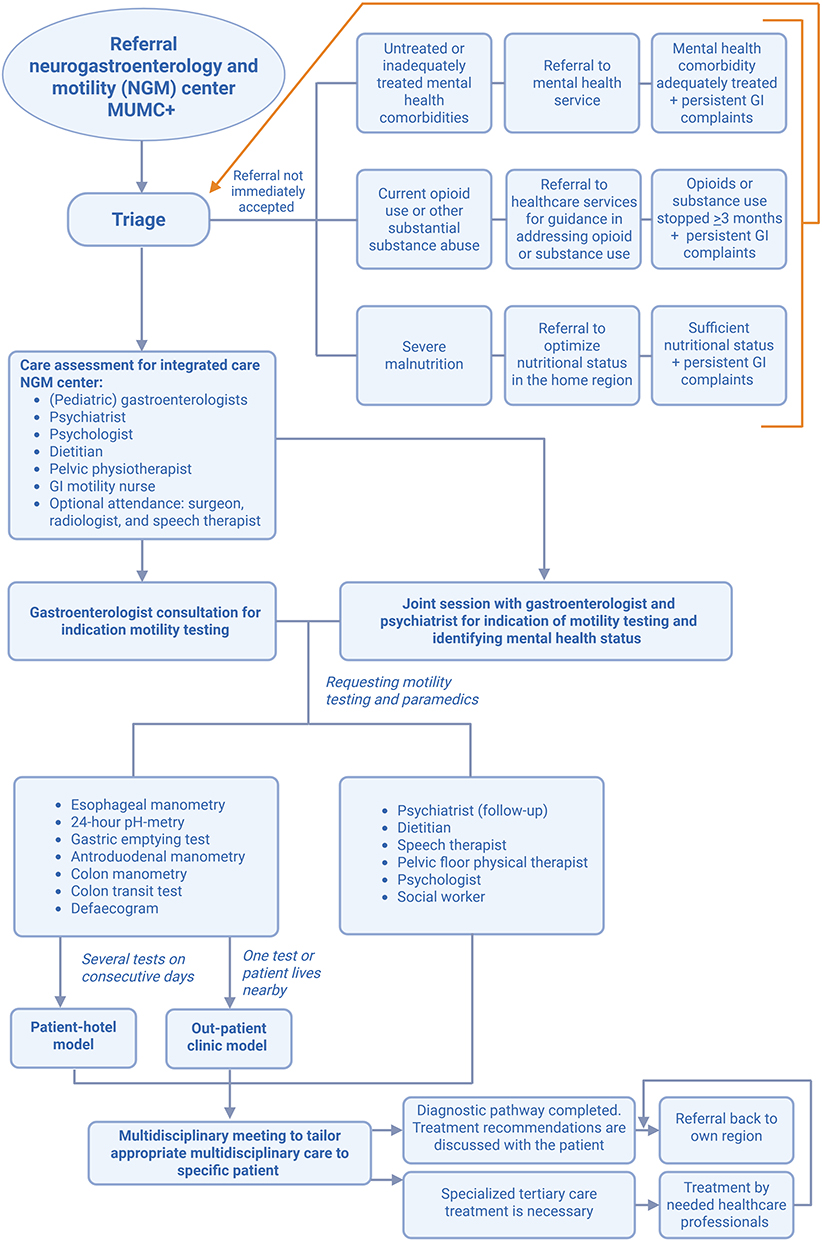 |
Figure 1 Integrated care approach for neurogastroenterology and motility disorders at MUMC+. The model illustrates a structured, multidisciplinary framework in which patients progress through coordinated diagnostic and therapeutic steps. It integrates input from several healthcare professionals and diverse treatment modalities to provide an individualized care pathway. Key steps in the care pathway are highlighted in bold for clarity. Figure created with BioRender.com. |
Referral to the Neurogastroenterology and Motility Center
Patients are referred to our center both nationally (ie, the Netherlands) and internationally. Upon receipt of a referral, a neurogastroenterologist conducts an initial review to determine the most appropriate course of action. Based on this assessment, one of three decisions is made: (1) direct acceptance of the referral to the neurogastroenterology outpatient clinic, (2) further evaluation for potential referral to an upfront integrated consultation, for instance in the case of an extensive past history of mental health problems or a comorbid eating disorder, or (3) temporary rejection of the referral, accompanied by a rationale and, when appropriate, specific advice for the referring physician.
For referrals requiring further review, cases are discussed during the bi-weekly multidisciplinary team meeting, which comprises neurogastroenterologists, a pediatric gastroenterologist, psychiatrist, psychologist, NGM-dedicated dietitian, pelvic physiotherapist, specialized NGM nurse, and a nurse from the GI motility lab; see Figure 2. For selected cases, a radiologist, (pediatric) surgeon, or speech therapist may also be invited. Next, the team collaboratively evaluates whether the patient meets referral criteria, identifies the most appropriate referral pathway, and determines whether any additional information is required prior to acceptance.
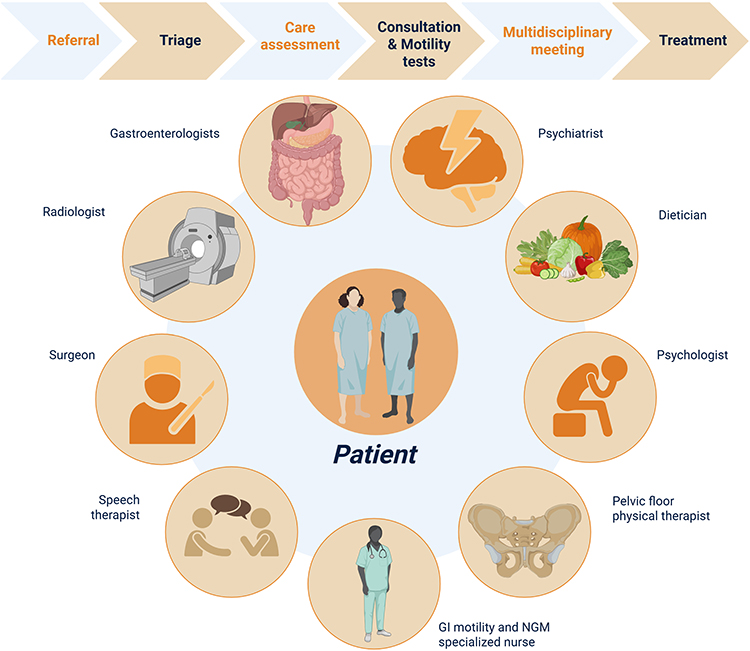 |
Figure 2 Multidisciplinary approach to patient-centered care. The patient is placed at the center of care, supported by a team comprising neurogastroenterologists, a pediatric gastroenterologist, a psychiatrist, a dietitian, a psychologist, a pelvic physiotherapist, a nurse from the GI motility lab and a specialized neurogastroenterology and motility (NGM) nurse. Additional input may be provided by a speech therapist, surgeon, or radiologist. The integrated care pathway is illustrated from referral to treatment: the main steps of this pathway are indicated in bold at the top of the figure. Figure created with BioRender.com. |
Referrals may be temporarily rejected for the following reasons: (a) untreated or inadequately managed mental health comorbidities, (b) ongoing opioid use or other significant substance abuse (eg, cannabinoid use), or (c) severe malnutrition. Once these issues have been appropriately addressed by the referring physician, the referral can be reconsidered. Rejections based on these factors are grounded in clinical evidence: opioid or cannabinoid use, and severe malnutrition can lead to abnormal motility test findings that do not accurately reflect an underlying motility disorder. Opioids may induce symptoms such as abdominal pain and constipation, which often resolve upon discontinuation, thereby obviating the need for further intervention.21 Severe malnutrition can independently alter gastrointestinal motility.22 To ensure that diagnostic testing accurately reflects the underlying disorder rather than nutritional status, patients should first undergo nutritional optimization at their referring center before referral. Similarly, prominent mental health comorbidities or eating disorders may confound symptom interpretation and are most effectively managed by local (mental) healthcare providers.9,23,24 Addressing these factors prior to referral ensures that the patient can derive the greatest benefit from the integrated care approach.
The Diagnostic Process
Following acceptance of the referral, the patient is scheduled for either a 45- to 60-minute consultation with the neurogastroenterologist alone, or for a joint consultation with both the neurogastroenterologist and the psychiatrist, depending on the presenting symptoms and suspected mental health comorbidities. The purpose of this consultation is to assess the patient’s symptoms, discuss expectations, and establish realistic treatment goals. Based on this evaluation, appropriate motility tests can be requested, and referrals to the necessary paramedical professionals are initiated as clinically indicated.
Motility testing is conducted in a specialized motility unit by trained GI motility nurses. For patients requiring multiple tests on consecutive days, testing is performed in a patient-hotel setting.25 Any additional (para)medical consultations are coordinated with the testing schedule to minimize the number of required hospital visits. In this setting, patients are not admitted to the hospital but instead stay in a hotel located within a three-minute walking distance from the hospital. While the hotel provides accommodation, no medical facilities are available on-site, so patients must be fully self-sufficient during their stay. From the patient’s perspective, this setting is generally perceived as more comfortable, offering the privacy of a single room rather than a shared hospital room, and greater freedom of movement between tests, allowing patients to explore the surrounding area. Additionally, the possibility for a relative to stay overnight is appreciated. Economically, the patient-hotel setting reduces hospital costs. A previous study conducted within our NGM center found annual savings between €48,433 and €74,613, corresponding to €613 to €944 per patient.25 Considering both patient satisfaction and cost-efficiency, this approach aligns with a broader vision of patient-centered care and addresses the growing need in healthcare to shorten inpatient stays while maintaining a high-quality patient experience.25
For patients requiring only a single test, or for those living nearby, testing is conducted in the outpatient clinic setting.
The Therapeutic Process
Upon completion of the diagnostic process, each case is reviewed in a multidisciplinary team meeting in order to develop an individualized care plan. The results of the GI motility tests, along with findings from the (para)medical consultations, are discussed. The treatment plan is then tailored to the specific needs identified by the healthcare professionals involved. Based on the discussion, one of two outcomes is determined:
Completion of Diagnostic Process with Regional Follow-Up
The diagnostic process is considered complete and integrated therapeutic recommendations are formulated. These recommendations reflect the collective expertise and observations of the multidisciplinary team and are intended to guide the referring healthcare professional in the patient’s home region. During a final consultation, these recommendations are discussed with the patient, and, if appropriate, initial treatment, such as the initiation of neuromodulatory treatment, may commence at that time. Additionally, the integrated recommendations are communicated to all relevant healthcare providers (eg, gastroenterologist, dietitian, psychologist) involved in the patient’s care within their local region, who can readily contact the NGM center for advice or clarification if needed.
Need for Specialized Tertiary Care
If specialized tertiary care is required before the patient can return to their local healthcare professional, the necessary treatment is provided at MUMC+ by the appropriate healthcare professionals. Upon completion of the required treatment at the MUMC+, responsibility for the patient’s treatment is transferred back to the referring healthcare professional in the patient’s home region. In selected cases of complex motility disorders, the patient’s care may be transferred from the referring center to our NGM center.
Adaptation of the Integrated Care Model
The integrated care model presented here was developed in a well-resourced tertiary care center with access to advanced diagnostics, specialized personnel, comprehensive insurance coverage, and supportive infrastructure. We recognize that full replication in lower-resourced environments may be limited by shortages in these resources, creating access barriers to multidisciplinary interventions. Nonetheless, the core principles of integrated care - coordinated, patient-centered, and multidisciplinary management - can be adapted to diverse settings. The World Health Organization (WHO) emphasizes integrated care, particularly in resource-limited environments, by anchoring service coordination at the primary care level.26 Approaches such as shared-care models, telehealth consultations, and stepped-care strategies may facilitate efficient, patient-centric care while optimizing limited resources.27 Implementation in low-resource settings should consider key contextual factors, including local needs, availability of trained personnel, prioritization of high-need patients, and flexible care delivery. In addition, all expertise need not necessarily to be localized to a single healthcare center. Creating a network of professionals with effective communication and channels for referrals and consultation could offer an alternative solution. Such adaptations can support the development of pragmatic pathways to extend the benefits of multidisciplinary management beyond tertiary centers. While the presented integrated care approach is conceptually robust, future studies are warranted to formally evaluate clinical outcomes, patient-reported outcomes, and cost-effectiveness of the model.
Conclusion
Neurogastroenterology and motility disorders are considered multifactorial in origin and impose substantial symptom and economic burdens, underscoring the need for an integrated care approach. While integrated care models have been successfully implemented in managing DGBI, this paradigm shift has not yet been widely applied to the diagnostic and therapeutic pathways for GI motility disorders. By presenting the integrated care approach implemented at our neurogastroenterology and motility center, we aim to provide a framework that can be adapted to other healthcare settings. Based on our experience, this model has the potential to improve patient satisfaction while fostering better interdisciplinary collaboration among healthcare professionals. Through coordinated, cross-disciplinary efforts, diagnostic and therapeutic pathways can be optimized, providing more personalized care for this complex patient population.
Ethics Approval
Institutional review board approval was not required, as this commentary does not involve research with human subjects or patient-identifiable data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was not supported by any particular form of funding.
Disclosure
S.M: has received royalties from a Dutch handbook about diagnostics and treatment of ARFID and received research funding from Stichting tot Steun (paid to host institute). D.K: has received research funding from Rome Foundation, United European Gastroenterology, Horizon 2020, Horizon Europe, ZonMw, Dutch Foundation for Gastroenterology and has received speaker’s fee from Rome Foundation (paid to host institute). The authors report no other conflicts of interest in this work.
References
1. Rimmer CJ, Gill KA, Greenfield S, Dowswell G. The design and initial patient evaluation of an integrated care pathway for faecal incontinence: a qualitative study. BMC Health Serv Res. 2015;15(1):444. doi:10.1186/s12913-015-1108-5
2. Chey WD, Keefer L, Whelan K, Gibson PR. Behavioral and diet therapies in integrated care for patients with irritable bowel syndrome. Gastroenterology. 2021;160(1):47–8. doi:10.1053/j.gastro.2020.06.099
3. Goodwin N. Understanding integrated care. Int J Integr Care. 2016;16(4):6. doi:10.5334/ijic.2530
4. Contandriopoulos, A.-P. and U.d.M.G.d.r.i.e. santé. The integration of health care: dimensions and implementation. GRIS, Université de Montréal; 2004.
5. Mikocka-Walus AA, Turnbull D, Holtmann G, Andrews JM. An integrated model of care for inflammatory bowel disease sufferers in Australia: development and the effects of its implementation. Inflamm Bowel Dis. 2012;18(8):1573–1581. doi:10.1002/ibd.22850
6. Warner MM, Soliman OM, Crichton M, et al. Systematic review: integrated models of care for managing irritable bowel syndrome. Neurogastroenterol Motil. 2025;37(2):e14989. doi:10.1111/nmo.14989
7. Leue C, Driessen G, Strik JJ, et al. Managing complex patients on a medical psychiatric unit: an observational study of university hospital costs associated with medical service use, length of stay, and psychiatric intervention. J Psychosom Res. 2010;68(3):295–302. doi:10.1016/j.jpsychores.2009.04.010
8. Berry SK, Chey WD. Integrated care for irritable bowel syndrome: the future is now. Gastroenterol Clin North Am. 2021;50(3):713–720. doi:10.1016/j.gtc.2021.04.006
9. Kruimel J, Leue C, Winkens B, et al. Integrated medical–psychiatric outpatient care in functional gastrointestinal disorders improves outcome: a pilot study. Eur J Gastroenterol Hepatol. 2015;27(6):721–727. doi:10.1097/MEG.0000000000000335
10. Staudacher HM, Black CJ, Teasdale SB, et al. Irritable bowel syndrome and mental health comorbidity - approach to multidisciplinary management. Nat Rev Gastroenterol Hepatol. 2023;20(9):582–596. doi:10.1038/s41575-023-00794-z
11. Basnayake C, Kamm MA, Stanley A, et al. Standard gastroenterologist versus multidisciplinary treatment for functional gastrointestinal disorders (MANTRA): an open-label, single-centre, randomised controlled trial. Lancet Gastroenterol Hepatol. 2020;5(10):890–899. doi:10.1016/S2468-1253(20)30215-6
12. Leue C, van Schijndel MA, Keszthelyi D. The multi-disciplinary arena of psychosomatic medicine–time for a transitional network approach. Eur J Psych. 2020;34(2):63–73. doi:10.1016/j.ejpsy.2020.02.003
13. Burgell RE, Hoey L, Norton K, Fitzpatrick J. Treating disorders of brain–gut interaction with multidisciplinary integrated care. Moving towards a new standard of care. JGH Open. 2024;8(5):e13072. doi:10.1002/jgh3.13072
14. Singh R, Zogg H, Ghoshal UC, Ro S. Current treatment options and therapeutic insights for gastrointestinal dysmotility and functional gastrointestinal disorders. Front Pharmacol. 2022;13:808195. doi:10.3389/fphar.2022.808195
15. Huang IH, Schol J, Khatun R, et al. Worldwide prevalence and burden of gastroparesis-like symptoms as defined by the United European gastroenterology (UEG) and European society for neurogastroenterology and motility (ESNM) consensus on gastroparesis. United Eur Gastroenterol J. 2022;10(8):888–897. doi:10.1002/ueg2.12289
16. Chen YJ, Tang W, Ionescu‐Ittu R, et al. Health-care resource use and costs associated with diabetic and idiopathic gastroparesis: a claims analysis of the first 3 years following the diagnosis of gastroparesis. Neurogastroenterol Motil. 2022;34(9):e14366. doi:10.1111/nmo.14366
17. Pasricha PJ, Grover M, Yates KP, et al. Functional dyspepsia and gastroparesis in tertiary care are interchangeable syndromes with common clinical and pathologic features. Gastroenterology. 2021;160(6):2006–2017. doi:10.1053/j.gastro.2021.01.230
18. Murray HB, Kuo B, Eddy KT, et al. Disorders of gut-brain interaction common among outpatients with eating disorders including avoidant/restrictive food intake disorder. Int J Eat Disord. 2021;54(6):952–958. doi:10.1002/eat.23414
19. Hasler WL, Parkman HP, Wilson LA, et al. Psychological dysfunction is associated with symptom severity but not disease etiology or degree of gastric retention in patients with gastroparesis. Am J Gastroenterol. 2010;105(11):2357–2367. doi:10.1038/ajg.2010.253
20. Snijkers JTW, Winkens B, Weerts ZZRM, et al. Satisfaction with life in IBS is associated with psychological burden rather than gastrointestinal symptom severity. Am J Gastroenterol. 2024;119(3):512–520. doi:10.14309/ajg.0000000000002547
21. Patel D, Callaway J, Vaezi M. Opioid-induced foregut dysfunction. Off J Am College Gastroenterol. 2019;114(11):1716–1725. doi:10.14309/ajg.0000000000000354
22. Soni KG, Dike PN, Suh JH, et al. Early-life malnutrition causes gastrointestinal dysmotility that is sexually dimorphic. Neurogastroenterol Motil. 2020;32(12):e13936. doi:10.1111/nmo.13936
23. Wang F, Liu Y-L, Jiang C-H, et al. Association between psychiatric disorders and irritable bowel syndrome: a bidirectional Mendelian randomization study. J Affect Disord. 2025;368:865–871. doi:10.1016/j.jad.2024.09.030
24. Sato Y, Fukudo S. Gastrointestinal symptoms and disorders in patients with eating disorders. Clin J Gastroenterol. 2015;8(5):255–263. doi:10.1007/s12328-015-0611-x
25. Masclee GM, Masclee AA, Kruimel JW, et al. Using a patient hotel: perceptions of the quality of care by patients undergoing analysis for gastrointestinal motility disorders in the Netherlands. J Patient Exp. 2022;9:23743735221089453. doi:10.1177/23743735221089453
26. Vijayasingham L, Ansbro É, Zmeter C, et al. Implementing and evaluating integrated care models for non-communicable diseases in fragile and humanitarian settings. J Migr Health. 2024;9:100228. doi:10.1016/j.jmh.2024.100228
27. Homewood D, Keane KG, Haridy J, et al. Updates in digital shared care: launching into the 21st century. Aust J Gen Pract. 2024;53(11):872–878. doi:10.31128/AJGP-10-23-7005
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Extended Consultations as a Trial Intervention in General Practice: Experiences of Patients with Complex Multimorbidities
Fryd R, Barrett BA, Lundstrøm SL, Frølich A, Aamann IC
Patient Preference and Adherence 2026, 20:580542
Published Date: 26 May 2026