Back to Journals » Clinical Ophthalmology » Volume 16
Tolerability in Glaucoma Patients Switched from Preserved to Preservative-Free Prostaglandin-Timolol Combination: A Prospective Real-Life Study
Authors Jandroković S, Vidas Pauk S ![]() , Lešin Gaćina D
, Lešin Gaćina D ![]() , Skegro I, Tomić M, Masnec S, Kuzman T, Kalauz M
, Skegro I, Tomić M, Masnec S, Kuzman T, Kalauz M
Received 15 July 2022
Accepted for publication 18 August 2022
Published 28 September 2022 Volume 2022:16 Pages 3181—3192
DOI https://doi.org/10.2147/OPTH.S382497
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sonja Jandroković,1,2 Sania Vidas Pauk,1 Dina Lešin Gaćina,1 Ivan Skegro,1,2 Martina Tomić,3 Sanja Masnec,1,2 Tomislav Kuzman,1,2 Miro Kalauz1,2
1Department of Ophthalmology, University Clinical Hospital Center Zagreb, Zagreb, Croatia; 2School of Medicine, University of Zagreb, Zagreb, Croatia; 3Department of Ophthalmology, Vuk Vrhovac University Clinic for Diabetes, Endocrinology and Metabolic Diseases, Merkur University Hospital, Zagreb, Croatia
Correspondence: Sania Vidas Pauk, Department of Ophthalmology, Zagreb University Hospital Center, Kišpatićeva 12, Zagreb, 10000, Croatia, Tel +385989371397, Fax +38512388430, Email [email protected]
Purpose: To evaluate the effect of switching from preserved prostaglandin analog-timolol fixed combinations (PG-timolol FCs) to preservative-free latanoprost-timolol FC (PF-LT) on intraocular pressure (IOP), ocular surface health, and tolerability in glaucoma and ocular hypertension (OH) patients with the concurrent ocular surface disease (OSD).
Methods: This was a longitudinal, prospective, interventional, real-life study among 42 patients. Up to 3 visits were planned, at baseline, 30, and 90 days to assess efficacy on IOP decrease and local tolerance. The severity of OSD symptoms [Ocular Surface Disease Index (OSDI) questionnaire], subjective drug tolerability [visual analog scale (VAS)], conjunctival hyperemia (McMonnies scale), and tear break-up time (TBUT) were the main parameters assessed.
Results: Data from 36 patients were available for statistical analysis. IOP was significantly reduced at day 30 and day 90 compared to baseline (16 vs 14 vs 14 mmHg, p < 0.001). Significant improvement was demonstrated in OSD symptoms, signs, and VAS scores from the baseline to the second and third visits. Median OSDI (27.1 vs 9.6 vs 4.2, p < 0.001), conjunctival hyperemia (2 vs 1 vs 1, p < 0.001), corneal surface staining (p < 0.001), and conjunctival staining scores (p < 0.001), and the percentage of patients with eyelid and periocular hyperemia (61.1 vs 12.5 vs 2.8%, p < 0.001), significantly decreased. TBUT (4 vs 5 vs 6 s, p < 0.001) and VAS score regarding tolerability (5 vs 2 vs 1, p < 0.001) significantly increased.
Conclusion: A switch from preserved PG-timolol FCs to PF-LT improved tolerability and optimized IOP control, providing better adherence with greater chances of treatment success.
Keywords: glaucoma, prostaglandin analogs, preservative, benzalkonium chloride, preservative-free, fixed combinations
Introduction
Glaucoma is a chronic, progressive, potentially blinding, irreversible eye disease causing optic nerve rim and retinal nerve fiber layer damage with consequent visual field loss. It is the second leading cause of blindness in Europe and among the leading causes of blindness worldwide. The global prevalence of primary open-angle glaucoma (POAG) is 3.5% in 40–80-year-olds, with the number of people having glaucoma estimated to be 76 million in 2020, which is expected to increase to 112 million by 2040.1,2 Currently, the usual approach to lower intraocular pressure (IOP) is topical therapy in the first line. Glaucoma requires the continuous long-term engagement of the patient with the recommendation proposed by the doctor and proper self-management to achieve the target IOP and prevent disease progression. Hence, treatment success predominantly lies in patients’ adherence and persistence with therapy, which is related to many drug-related factors, such as side effects, cost, and complexity of the dosing regimen.1
Many prescribed topical glaucoma formulas contain preservatives such as benzalkonium chloride (BAK), polyquaternium-1(PQ), boric acid, and zinc chloride. Their prolonged use causes and exacerbates pre-existing ocular surface disease (OSD), dry eye, and Meibomian gland dysfunction, which already has a high prevalence in the elderly.3–7 BAK is most frequently found in ophthalmic formulations of all preservatives and was shown to significantly contribute to ocular surface damage.4 In vitro, in vivo, and clinical studies extensively investigated its toxic effects and showed that long-term use of BAK causes time and dose-dependent ocular surface cytotoxicity, likely mediated by chronic oxidative stress. That causes inflammation and induction of signals leading to apoptosis and potentially might play a role in trabecular meshwork (TM) dysfunction and cell death, resulting in a vicious cycle.8–12 The more treatments administered, the greater the quantity of toxic compounds and inflammatory cytokines diffusing from the surface to deeper structures, which leads to TM inflammation and higher resistance to aqueous humor outflow, a subsequent increase in IOP, the requirement for more treatments, and eventually surgery, whose prognosis will be negatively influenced by changes within the anterior segment.13 Therefore, cumulative exposure to preservatives might impact patients’ adherence and persistence to treatment and adversely influence the outcomes of glaucoma treatment.
Extensive multicenter epidemiology surveys conducted in Europe and the USA revealed that up to 47.6% and 59% of patients using preserved glaucoma medication reported OSD or dry eye disease (DED) symptoms, whereas 53–70% and 61–78% of patients had signs of OSD or DED.14,15
The invention of prostaglandin analog (PG)-timolol fixed combinations (FCs) offered advances in the treatment of glaucoma, including better efficacy in controlling IOP compared to their separate components, the need for fewer instillations, and the prevention of the previous drug washout.16–21 That resulted in less exposure to preservatives, more effective IOP control, reduced costs, and improved adherence to the treatment regimen. Guven Yilmaz and coworkers showed similar IOP-lowering efficacy of latanoprost, travoprost, and bimatoprost formulations combined with timolol maleate.22
Many clinical studies revealed that using preservative-free (PF) glaucoma formulations significantly reduces OSD signs and symptoms compared to preserved formulations with the same IOP-lowering efficacy.3,4,14,23,24 In various studies, patients tolerated PF glaucoma therapy better, contributing to better treatment persistence and improved patients’ Quality of Life (QoL).10,18,23,25,26 Hence, PF FCs development is considered an important goal in glaucoma management, especially given the prevalence of glaucoma and the number of people suffering from OSD due to the long-term use of preservative-containing therapy.27 Recently, Laboratories Théa, Clermont Ferrand, France, introduced a new PF latanoprost-timolol FC (Fixaprost®, Fixalpost®, Fixapost® according to the country), the first to improve the local tolerability of the most prescribed FC that has so far previously only existed with BAK.28 A Phase III, multicentric, randomized, parallel-group study with 242 patients showed non-inferiority of PF latanoprost-timolol FC (PF-LT) in IOP-lowering efficacy and safety compared to the preserved comparator, with PF-LT showing slight better tolerability.28
The present study’s authors hypothesized that switching the preserved PG-timolol FCs to PF-LT in glaucoma and OH patients with existing OSD would improve their ocular surface health and drug tolerability, with at least the same IOP lowering effect.
This real-life study aimed to evaluate the tolerability and efficacy in glaucoma and OH patients with concurrent OSD who switched from preserved PGs (latanoprost, travoprost, and bimatoprost)-timolol FCs to PF-LT and to evaluate whether this treatment could alleviate OSD symptoms and signs and improve local tolerability.
Patients and Methods
Study Design
This longitudinal, prospective, interventional study of drug tolerability and efficacy was conducted at the Department of Ophthalmology, Zagreb University Hospital Center in Zagreb, Croatia, following the Declaration of Helsinki and approved by the Hospital’s Ethics Committee. The patients included in the study received both written and oral information about the study and signed written informed consent. The study took place between March 2021 and September 2021 and was registered in the two registers; primary: ClinicalTrials.gov Identifier: NCT04891588, and secondary: DRKS German Clinical Trials Register, DRKS-ID: DRKS00024581.
Patients
Forty-two patients were recruited during the authors’ routine clinical work over the three months. Eligible adult subjects (≥18 years) had to have a documented diagnosis of POAG or OH and had been treated and well-controlled for at least three months with preserved PGs (latanoprost, travoprost, and bimatoprost)-timolol 0.5% FC eye drops (any brand) before entering the study. Criteria for inclusion required IOP ≤ 19 mm Hg in both eyes at the inclusion visit, a stable visual field (based on at least two reliable visual field tests performed within the last six months), central corneal thickness within the 500–580 µm range, and presence of at least mild to moderate conjunctival hyperemia [grade 1–5 according to McMonnies-Chapman-Davies’s scale29]. Excluded were patients with best-corrected visual acuity (BCVA) < 0.1 (Snellen decimals), advanced visual field defects (MD ≥ 12 dB), an acute eye infection or severe eye inflammation, those wearing contacts, those who had undergone any intraocular surgery (other than filtration surgery performed at least six months before screening), or those having any ocular surface abnormality preventing accurate IOP measurement.
Methods
On the first baseline visit (V1), the patients were switched from commercially available PGs (latanoprost, travoprost, or bimatoprost)-timolol preserved FCs to a PF-LT (preservative-free fixed combination of latanoprost 0.005% and timolol 0.5% in single-dose units; Laboratoires Théa, Clermont-Ferrand, France). They were instructed to instill one drop of medication daily in the evening.
Two follow-up visits were scheduled for 30±3 days (V2) and 90 ±7 days (V3) after the first visit. At each visit, all the participants underwent the following clinical examinations and investigations: Snellen visual acuity (VA) testing; assessment of the severity of conjunctival hyperemia by using the McMonnies-Chapman-Davies visual analogue scale29 which graduates the hyperemia from 0 (no hyperemia) to 5 (severe hyperemia); assessment of the severity of blepharitis by using Efron’s scale which graduates the blepharitis from 0 (no blepharitis) to 4 (severe blepharitis); TBUT measurement according to TFOS DEWS II Diagnostic guidelines;30 assessment of corneal and conjunctival fluorescein surface staining by using the National Eye Institute/Industry Workshop (NEI) scale;31 Goldman applanation tonometry; assessment of the presence of any papillary/follicular conjunctivitis, eyelid or periocular edema or hyperemia or conjunctival chemosis; assessment of the extent and severity of OSD symptoms and their impact on everyday activities by using Ocular Surface Disease Index (OSDI);30 a Visual Analog Scale (VAS) for the subjective evaluation of drug tolerability, in which 0 indicated very good tolerability and 10 demonstrated very poor tolerability.
IOP was measured using a calibrated Goldman tonometer at 9:00 a.m. (±1 h). Two measurements were taken, and if these differed by >2 mm Hg, a third reading was taken. The average value was used in the analysis.
The Ocular Surface Disease Index (OSDI) questionnaire was used to assess the symptoms, functional limitations, and environmental factors affecting the ocular surface. It contained 12 questions that patients graded on a scale from 0 to 4 (0 – none of the time to 4 – all the time). A total OSDI score was calculated using a particular formula.32 OSDI ranged from 0 to 100, with a higher number indicating a more significant disability. The advantage of this questionnaire is that it can categorize the severity of OSD and has a cut-off value to detect OSD; 0–12 normal ocular surface, 13–22 mild ocular surface disease, 23–32 moderate, and 33–100 severe.
Since the investigator was not blinded, to avoid potential bias, the authors provided three working sheets, one for each visit, where the investigator documented the findings from that visit by not knowing or having insight into the findings from the previous visits. Furthermore, all the measurements were taken twice, first by the second author and then rechecked by the third author. If there were disagreements between the measurements, the first author decided what to accept.
Outcome Measures
Primary outcome measures included the changes in symptoms of ocular surface disease, drug tolerability, signs of ocular surface disease, tear film stability, and visual function.
The secondary outcome measure evaluated the effectiveness of preservative-free latanoprost/timolol FC in controlling the IOP values and safety.
Statistical Analysis
Statistical analysis was performed using StatisticaTM software, package version 14.0 (TIBCO® Inc., USA). The normality of data distribution was tested by the Shapiro–Wilk and Kolmogorov–Smirnov tests, and the homogeneity of variance by Levene’s test. Results of descriptive analyses were expressed as mean ± SD and median (min-max) for continuous data, median (min-max) for ordinal data, and numbers (percentages) for categorical data. Differences in distributions of ordinal and continuous data were evaluated by nonparametric tests (Friedman ANOVA test for dependent variables and Kruskal–Wallis ANOVA for independent variables) since the assumption of homogeneity of variance for tested variables was not met. Cochran’s Q test assessed differences in distributions of categorical data. The Wilcoxon test, Chi-square test, and multiple comparisons were used for post hoc analyses. A p-value of less than 0.05 was considered statistically significant in all analyses.
Results
The authors set the study protocol in the middle of the coronavirus disease 19 pandemics (COVID-19). Six of the 42 recruited patients, who could not participate in follow-up visits due to the COVID-19-related restrictions, were dropped out. Therefore, the data from 36 Caucasian patients, who met all study criteria and attended all scheduled visits, were processed and analyzed. The baseline characteristics of these 36 patients (28 POAG/8 OH) are presented in Table 1. Before entering the study, all patients were treated with preserved PG-timolol FCs for 77.18 ± 41.45 months, among them 14 (38.9%) with latanoprost-timolol FC (Xalacom®, Pfizer, New York, NY, USA), 11 (30.6%) with travoprost-timolol FC (Duotrav®, Alcon, Fort Worth, TX, USA), 7 (19.4%) with bimatoprost-timolol FC (Ganfort®, Allergan, AbbVie Dublin, Ireland), and 4 (11.1%) with latanoprost-timolol FC (Lapovis Plus®, Zentiva, Prague, Czech Republic). According to the OSDI questionnaire scale evaluated at the first visit before switching from preserved PGs-timolol FC, 9 (25%) patients had no OSD symptoms, 9 (25%) had mild, 3 (8.3%) moderate, and 15 (41.7%) of them had severe OSD symptoms.
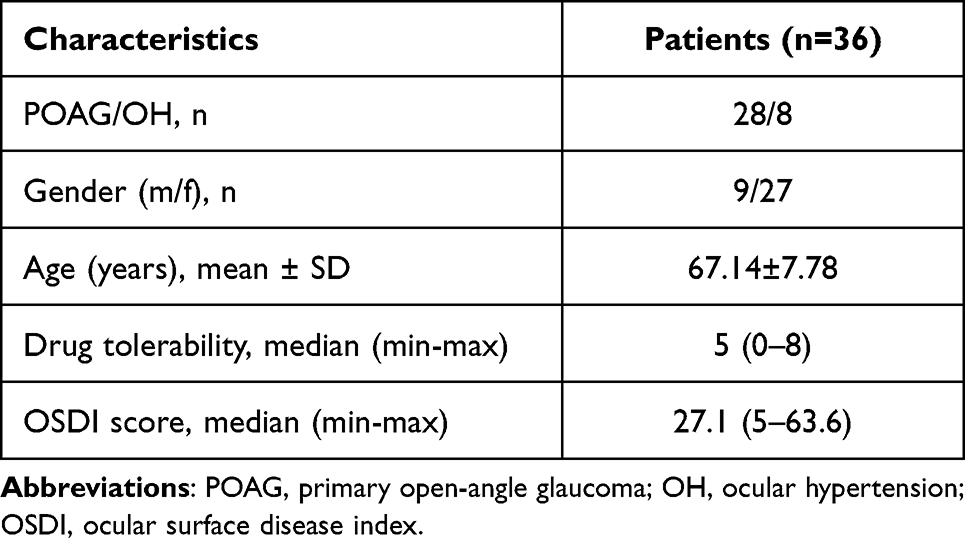 |
Table 1 Baseline Characteristics of 36 Study Patients with POAG and OH |
Table 2 presents baseline characteristics of 72 study eyes with POAG and OH. The most pronounced and severe baseline OSD signs were conjunctival hyperemia, eyelid, or periocular hyperemia, corneal and conjunctival fluorescein surface staining, and short TBUT. The most frequent corneal staining zone was inferior (32.9%), while the most frequent conjunctival staining zones were caruncle (50.6%) and inferior caruncle (35.5%).
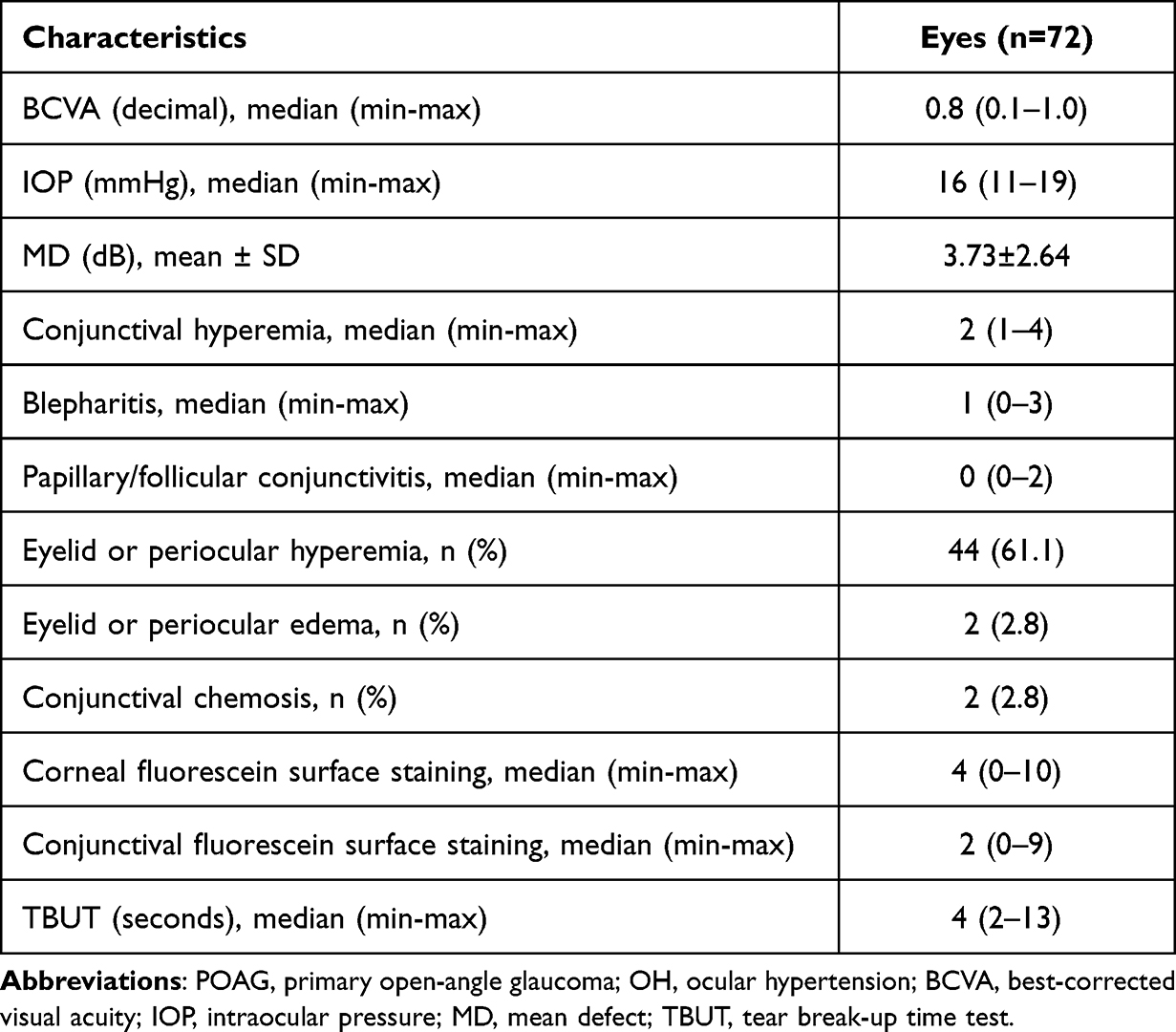 |
Table 2 Baseline Characteristics of 72 Study Eyes with POAG and OH |
When comparing the baseline characteristics of 36 study patients (72 POAG/OH eyes) treated with different preserved PG-timolol FC medications, the only marginal difference was observed in the OSDI score (p = 0.057) (Table 3). Post hoc multiple comparison analyses found a significant difference in the OSDI score only among eyes treated with travoprost-timolol FC and bimatoprost-timolol FC (p = 0.017), while no differences were observed in the OSDI score between the other medications (p > 0.05).
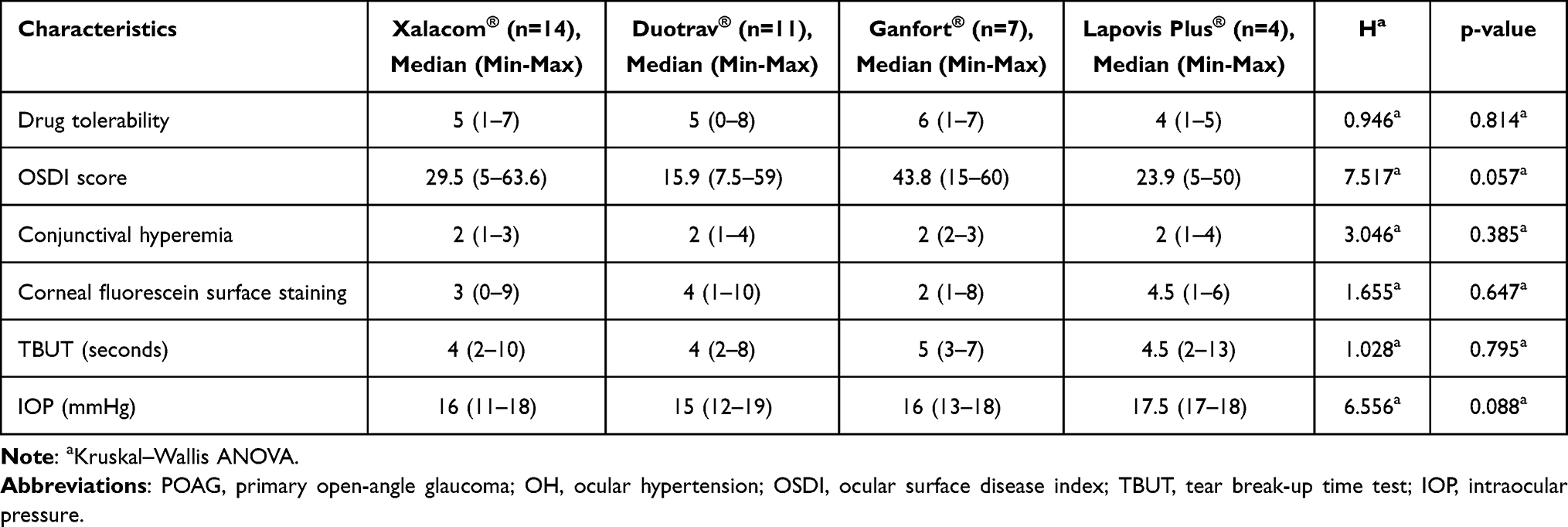 |
Table 3 According to Different Preserved PG-Timolol FC Drugs, the Baseline Clinical Characteristics of 36 Study Patients (72 Eyes) with POAG and OH |
Primary Outcomes
Change of Symptoms of Ocular Surface Disease and Self-Reported Drug Tolerability
The median OSDI score significantly decreased from the baseline on the second and third visits (27.1 vs 9.6 vs 4.2, p < 0.001) (Figure 1A). The post hoc analysis also showed a significant decrease in OSDI from the baseline on the second visit (p < 0.001) and from the second to the third visit (p = 0.003). According to the OSDI scale, from the baseline to second and third visits, the number of patients with no OSD symptoms significantly increased (9 vs 23 vs 27) (p < 0.001), while the number of those with mild (9 vs 7 vs 6), moderate (3 vs 3 vs 0), and severe OSD symptoms (15 vs 3 vs 2) significantly decreased (p < 0.001). Table 4 presents the changes in the score for each OSD question from baseline to study visits (per-protocol set) in 36 study patients with POAG and OH. The most significant improvements were observed for questions of having eyes sensitive to light (p < 0.001), painful or sore eyes (p < 0.001), problems while reading (p < 0.001), and in windy conditions (p < 0.001) during the last week.
 |
Table 4 Changes in the Score for Each OSDI Question from Baseline by Study Visits (Per-Protocol Set) in 36 Study Patients with POAG and OH |
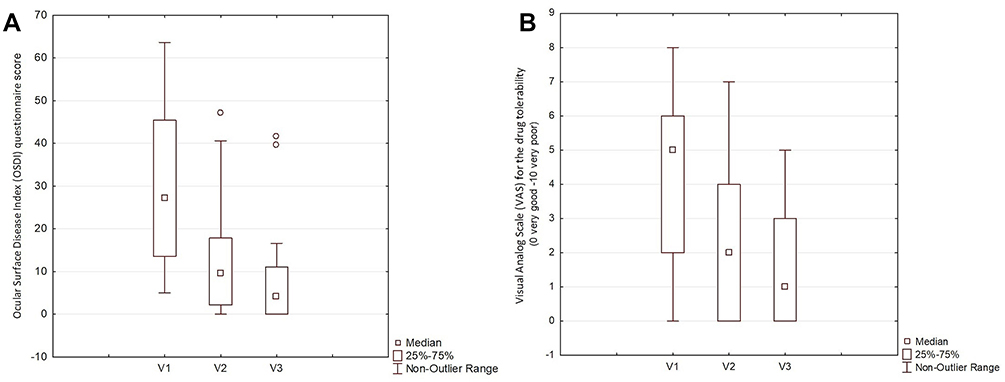 |
Figure 1 Change of OSDI questionnaire score (A) and subjective drug tolerability (B) from baseline by study visits in 36 study patients with POAG and OH. |
The subjective drug tolerability increased from the baseline on the second and third visits (p < 0.001) (Figure 1B). However, post hoc analyses only showed a significant increase in median drug tolerability from the baseline, after switching to PF-LT, on the second visit (5 vs 2, p = 0.001), while it did not change significantly from the second to third visit (2 vs 1, p = 0.079).
Change of Signs of Ocular Surface Disease
Significant changes were noted in most OSD signs from the baseline by the time of the study visits (per-protocol set) in 72 study eyes (Table 5). Among OSD signs, the most decline was observed in conjunctival hyperemia (p < 0.001) (Figure 2A), corneal (p < 0.001) (Figure 2B) and conjunctival fluorescein surface staining (p < 0.001), and eyelid or periocular hyperemia (p < 0.001) (Table 4). From the baseline to the second and third visits, the staining reduced in eyes with corneal inferior (32.9% vs 25% vs 23%), central and inferior (14.5% vs 13.2% vs 12.8%), and superior, nasal, inferior, and central fluorescein surface zones (19.7% vs 1.3% vs 0%). Conjunctival fluorescein surface staining reduced in caruncle (50.6% vs 42.1% vs 40.8%) and inferior-caruncle zones (35.5% vs 14.5% vs 10.5%) from the baseline to the study visits (data not shown). No significant differences were found in the eyelid or periocular edema and conjunctival chemosis from baseline to study visits (p = 0.135) (Table 4). TBUT significantly increased from baseline to study visits (per-protocol set) in 72 study eyes with POAG and OH (p < 0.001) (Figure 2C). However, post hoc analyses found that TBUT was significantly improved only from the baseline to the second visit (p < 0.001), while no significant difference in TBUT was found from the second to the third visit (p = 0.151).
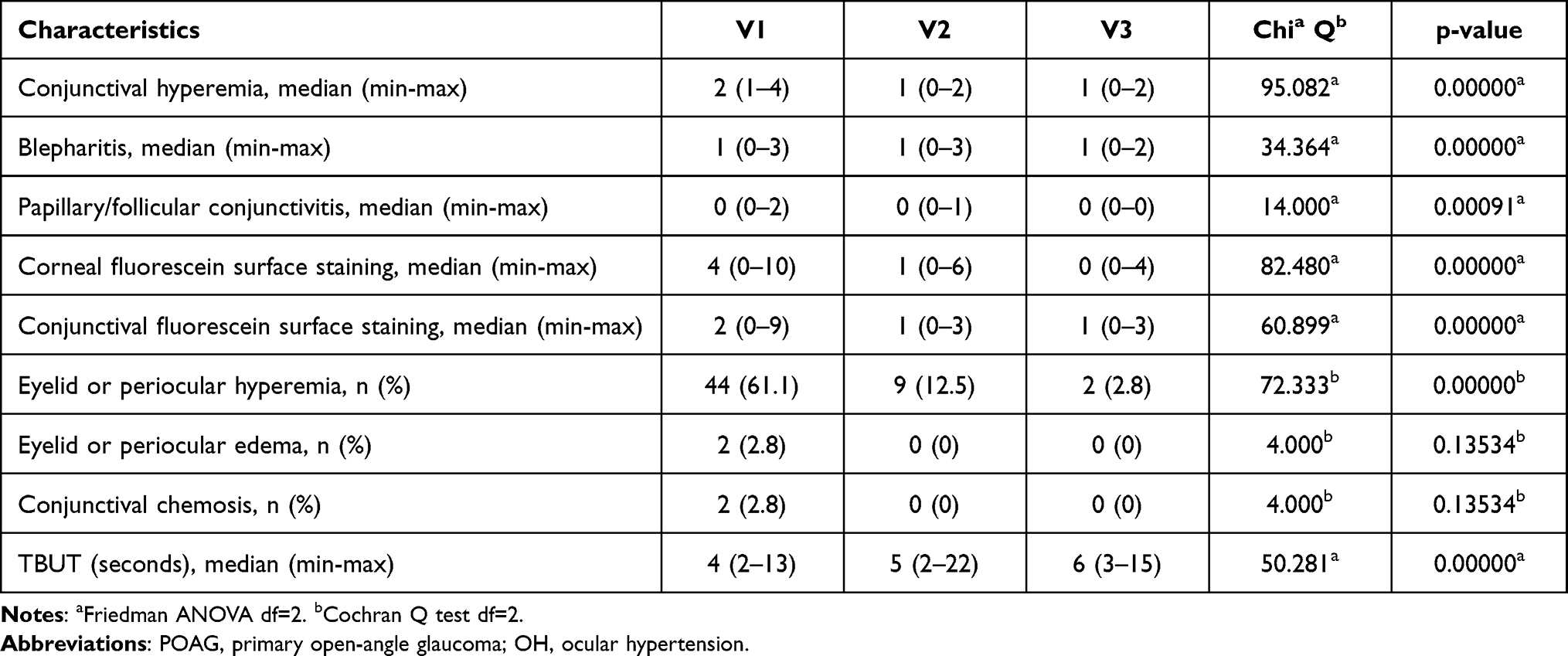 |
Table 5 Changes of Ocular Surface Disease Signs from Baseline by Study Visits (Per-Protocol Set) in 72 Study Eyes with POAG and OH |
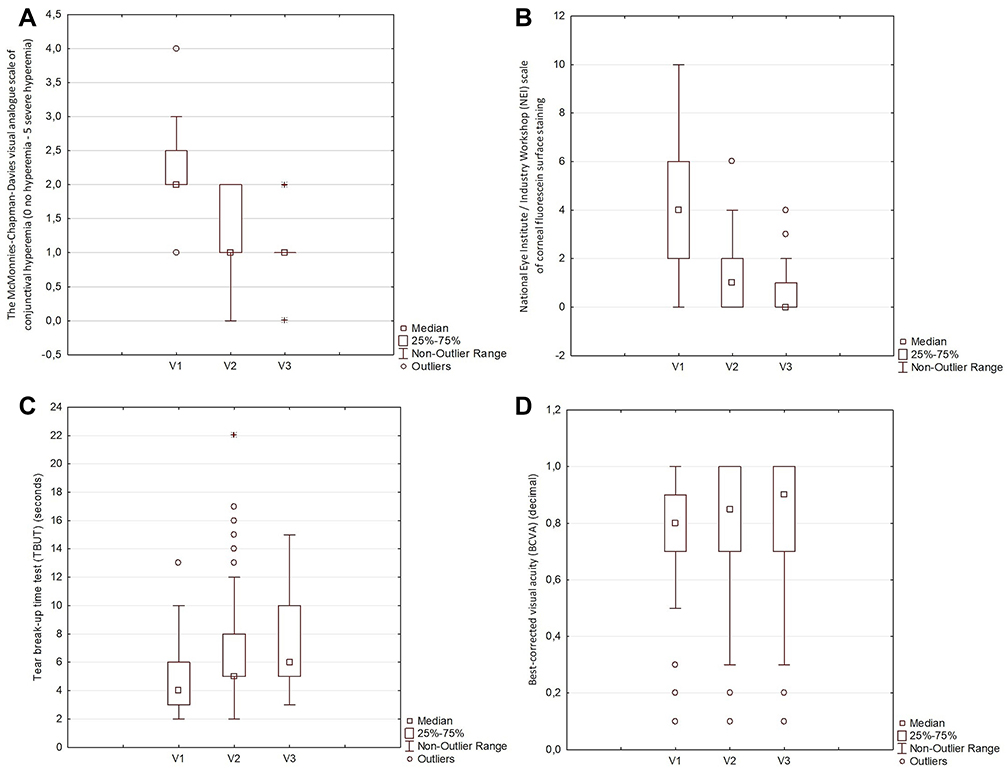 |
Figure 2 Change of the severity of conjunctival hyperemia (A), the severity of corneal fluorescein surface staining (B), TBUT (C), and BCVA (D), from baseline by study visits in 72 study eyes with POAG and OH. |
Change of Visual Function
A significant improvement was observed in visual function from the baseline by study visits (per-protocol set) in 72 study eyes with POAG and OH (p = 0.030) (Figure 2D). Post hoc analyses found a significant increase in the median BCVA from the baseline to the third visit (0.8 vs 0.9, p = 0.025). In contrast, no substantial changes in the median BCVA were observed from the baseline on the second visit (0.8 vs 0.85, p = 0.073) and from the second to the third visit (0.85 vs 0.9, p = 0.167).
Secondary Outcome
A significant decrease in IOP was seen from baseline to study visits (per-protocol set) in 72 study eyes with POAG and OH (p < 0.001). However, according to the post hoc analyses, the median IOP decreased significantly only from the baseline to the second visit (16 vs 14 mmHg, p < 0.001), while no significant difference in the median IOP was observed from the second to the third visit (14 vs 14 mmHg, p = 0.073).
Adverse Events
No local or systemic adverse events (AE) were reported during the study.
Discussion
Due to its high efficacy, good overall tolerability profile, and the need for once-daily administration, latanoprost-timolol FC is one of the most prescribed fixed formulations in glaucoma treatment, which until recently, existed only preserved with BAK.33 Fixalpost® is the first, and until now, the only PF-latanoprost-timolol FC (PF-LT) developed to eliminate dose-dependent and time-dependent undesired and detrimental effects of BAK on the ocular surface in patients who use the medication on a daily and lifelong basis.28 To our knowledge, the present study is the first prospective study in which POAG and OH patients with concurrent OSD were switched from preserved PG-timolol FCs, of any brand, to PF-LT. The authors investigated the effect of that switch on symptoms and signs of OSD, local drug tolerability, and QoL using the OSDI questionnaire, self-reported drug tolerability, and objective measurements. More than 75% of patients reported OSD symptoms at the baseline visit that impacted their daily functioning. Overall, 42% of patients reported their symptoms as severe, with a tremendous impact on everyday living and QoL. Overall subjective evaluation of drug tolerability was moderate to poor. Upon examination, most patients had moderate conjunctival hyperemia, mild to moderate blepharitis, TBUT lower than 5 seconds, and 61.1% had eyelid or periocular hyperemia. Conjunctival and corneal surface staining were present in almost all subjects. There were no significant differences in OSD severity and ocular tolerability regarding the initial drug. However, there was borderline significance for OSDI, with bimatoprost-timolol FC scoring worse than the other drugs. Therefore, despite adequate control of IOP in patients with their initial preserved therapy, they were experiencing clinical signs and symptoms of OSD and tolerated it poorly. Thirty days after switching the therapy, the authors noticed a significant improvement in the overall OSDI score and the self-reported drug tolerability (p < 0.001), which increased patient satisfaction with therapy. The findings were further improved after 90 days. In the end, only six patients reported moderate OSD, and none had severe OSD symptoms. The subjective evaluation of drug tolerability was excellent. Subjects felt the most significant improvement in light sensitivity, ocular pain, and ocular dryness. A significant improvement was noticed in the incidence and severity of all OSD signs from the initial visit to the second and third visits. The most significant improvements were observed in conjunctival hyperemia, eyelid and periocular hyperemia, and fluorescein ocular surface staining. According to the results, the authors suggested that a switch to PF-LT, regardless of the initial drug, ameliorated the ocular surface health, alleviated OSD symptoms, and significantly improved local drug tolerability.
The clinical Phase III study that investigated the efficacy and safety of T2347 [preservative-free fixed combination of latanoprost 0.005% and timolol 0.5 (PF-LT)] was published in 2019 by the T2347 Study Group. It was conducted in ten countries on 122 patients receiving T2347 and 110 remaining on BAK–latanoprost-timolol FC. The study met the co-primary endpoints showing non-inferiority in terms of IOP-lowering efficiency and safety of T2347 compared to a preserved comparator. AEs were similar in both treatment groups, with no reported severe local or systemic AE. Regarding ocular tolerability, the total severity score of ocular symptoms upon administration was lower for the T2347 group, but there were no differences in symptoms throughout the day. Patients subjectively tolerated PF-LT better, but there were no differences in objective ocular parameters. In conclusion, PF-LT (T2347) and the BAK-containing comparator showed similar efficacy and safety, while T2347 showed slightly better subjective, but not objective ocular tolerance.28 The present, real-life switch study results in drug tolerability and efficacy in IOP decrease were more in favor of PF-LT compared to those obtained in the phase III T2347 study.28 A possible explanation is a difference between the study population and the prescribed initial drug. In the T2347 phase III study, patients were previously treated successfully and were mainly satisfied with the initial preserved therapy. On the other hand, the present study’s population was older (67.14±7.78 vs 65.8 ± 10.8 years). All the patients had OSD to various extents and therefore experienced a significant improvement in the OSD signs and symptoms and drug tolerability after switching to PF-LT therapy. Second, in this study, patients initially received different PG-timolol FCs. It has been shown that latanoprost-timolol FC causes less conjunctival hyperemia.33 In contrast, bimatoprost-timolol causes more redness than other PG-timolol FCs. Thus, reduced redness and better tolerability may be due to switching to another PG-timolol FC, not only the elimination of BAK or PQ.
So far, PF-latanoprost (PF-L) was the most investigated PF PG formulation available on the market. The initial preclinical study showed a significant reduction in viability of the human corneal epithelial cells and significant toxic and inflammatory responses in the animal model (rabbit ocular surface epithelium) of BAK-latanoprost (BAK-L) versus PF-L.11 Based on those findings, the PF-L T2345 (Monoprost® Laboratoires Théa, Clermont-Ferrand, France) phase III study on the efficacy and safety and the Relief study of the local tolerability of PF-L (T2345) in humans revealed a better ocular safety profile, local tolerability, and non-inferior IOP-lowering efficacy of PF-L vs BAK-L.10,34 Another two studies, a meta-analysis on 20 randomized controlled trials (RCTs) and a recent study published by El Ameen and coworkers, showed a better ocular tolerance of PF-L (T2345) compared to all other preserved PGs (latanoprost, bimatoprost, travoprost, and tafluprost) with no statistically significant differences in mean IOP for all drugs, except for BAK-tafluprost which was inferior to PF-L.35,36
Many studies demonstrated improved drug tolerability after switching from preserved to unpreserved therapy.10,24,25,34,36 However, a recently published meta-analysis that investigated the safety and efficacy of BAK-preserved, alternatively preserved, and PF glaucoma medications were inconsistent with these findings. This meta-analysis included sixteen, only RCTs and no real-life study. It showed no conclusive evidence of differences in effectiveness or safety between these three preservative formulations on glaucoma and OH patients.37 Furthermore, the included studies did not focus on treatment tolerance in patients with OSD, while the real-life studies generally tend to do so.
It was long thought that preservatives, like BAK, enhance the penetration of drugs into the anterior chamber through disruption of the hydrophobic barrier of the corneal epithelium, making BAK-containing drugs more efficient.38 However, many authors refuted that.4,10,35 Two studies demonstrated non-inferiority of preserved latanoprost and bimatoprost-timolol FCs compared to their unpreserved comparators in IOP lowering efficiency.28,39 The present study showed no differences in median baseline IOP regarding the initial drug. However, the authors found a significant reduction in overall median IOP on the second visit, which remained stable until the third visit. The authors can explain this in several ways. First, optimizing the ocular surface in patients with glaucoma and OSD might improve IOP control.28,40 Second, the patients probably adhered more to a treatment schedule due to fewer ocular symptoms and signs and better drug tolerability, which was demonstrated as treatment facilitators in various studies.10,25,26,28 Third, the patients probably adhered more due to the Hawthorne effect, a type of reactivity in which individuals modify an aspect of their behavior in response to their awareness of being observed, which resulted in better adherence in a clinical trial setting.41 Fourth, the authors measured IOP only three times during the study, at the baseline, second and third visits, and the study had no parallel-group design. Twenty-four hours of IOP observation in an RCT would be a better solution to investigate this more objectively.
The authors must declare the limitations and potential biases of the present research. The study was not a parallel group, randomized comparative study. That might have resulted in selection bias. Moreover, a direct comparison of the drugs might show more objective results. However, the parallel-group study design was considered unethical in this case, as patients in our study already had OSD, so continued use of the same drug would worsen the ocular surface parameters. The open-label study design could not be avoided since preservative or PF drugs had different packages, impacting the researchers’ objectivity in assessing OSD signs and IOP measurements, and patients’ subjective assessments. Patients probably adhered more to treatment due to the Hawthorne effect, so this may not be the best example of real-life patient behavior.41 Investigators would be more likely to include patients who complained about medication problems, which might result in regression-to-the-mean bias. Given the fluctuating nature of OSD symptoms (and signs) in this setting, some patients might improve without any medication change, which remains undetected in an uncontrolled study. Further, the study was conducted on a relatively small number of participants of different ethnicity, predominantly females, so the results may not be generalizable to other populations, and it lasted only three months. Therefore, to strengthen the value of our research, more studies are needed with more subjects and longer follow-ups.
Conclusion
The present real-life study confirmed that a switch from preserved prostaglandin analog-timolol fixed combinations (FCs) to preservative-free latanoprost-timolol FC significantly reduced symptoms and signs of OSD, improved ocular drug tolerability, and consequently the persistence and effective reduction of intraocular pressure. The beneficial effects of switching to unpreserved medication might affect patient adherence and persistence with therapy and impact therapy outcomes, and therefore suitable for all glaucoma patients.
Abbreviations
BAK, benzalkonium chloride; BCVA, best-corrected visual acuity; DED, dry eye disease; FC, fixed combination; IOP, intraocular pressure; MD, mean defect; NEI, National Eye Institute/Industry Workshop; OH, ocular hypertension; OSD, ocular surface disease; OSDI, ocular surface disease index; PF, preservative-free; PF-L, preservative-free latanoprost; PF-LT, preservative-free latanoprost timolol fixed combination; PG, prostaglandin analog; POAG, primary open-angle glaucoma; PQ, polyquaternium-1; QOL, quality of life; RCT, randomized controlled trial; TBUT, tear break-up time; TFOS DEWS, Tear Film and Ocular Surface Society, Dry Eye Workshop; TM, trabecular meshwork; VAS, visual analog scale.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available but from the corresponding author at reasonable request.
Ethics Statement and Informed Consent
All present research procedures were conducted according to the 1964 Declaration of Helsinki and its later amendments. Before conducting this study, the proposals and ethical standards were reviewed and approved by the Hospital’s Ethics Committee of University Clinical Hospital Center Zagreb (class: 8.1.-21/18-4, number: 02/21 JG). Moreover, we formally introduced to all participants important information about this study and obtained their consent before participating in the research. Finally, all participant information is anonymous and confidential.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of the data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
This study has been funded by an unrestricted grant from Laboratoires Théa (Clermont-Ferrand, France).
Disclosure
Sonja Jandroković, Sania Vidas Pauk, Dina Lešin Gaćina, Ivan Skegro, Sanja Masnec and Tomislav Kuzman reports grants from Laboratoires Théa affiliate Inspharma, during the conduct of the study. The authors report no conflicts of interest regarding this work.
References
1. EGS. European Glaucoma Society Terminology and guidelines for glaucoma, 5th Edition. Br J Ophthalmol. 2021;105(Suppl1):1–169. doi:10.1136/bjophthalmol-2021-egsguidelines
2. Quigley HA. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262–267. doi:10.1136/bjo.2005.081224
3. Baudouin C, Labbé A, Liang H, Pauly A, Brignole-Baudouin F. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312–334. doi:10.1016/j.preteyeres.2010.03.001
4. Holló G, Katsanos A, Boboridis KG, Irkec M, Konstas AGP. Preservative-free prostaglandin analogs and prostaglandin/Timolol fixed combinations in the treatment of glaucoma: efficacy, safety and potential advantages. Drugs. 2018;78(1):39–64. doi:10.1007/s40265-017-0843-9
5. Pisella PJ, Pouliquen P, Baudouin C. Prevalence of ocular symptoms and signs with preserved and preservative free glaucoma medication. Br J Ophthalmol. 2002;86(4):418–423. doi:10.1136/bjo.86.4.418
6. Steven DW, Alaghband P, Lim KS. Preservatives in glaucoma medication. Br J Ophthalmol. 2018;102(11):1497–1503. doi:10.1136/bjophthalmol-2017-311544
7. Wilson LA. To preserve or not to preserve, is that the question? Br J Ophthalmol. 1996;80(7):583–584. doi:10.1136/bjo.80.7.583
8. Baudouin C, Riancho L, Warnet JM, Brignole F. In vitro studies of antiglaucomatous prostaglandin analogues: travoprost with and without benzalkonium chloride and preserved latanoprost. Invest Ophthalmol Vis Sci. 2007;48(9):4123–4128. doi:10.1167/iovs.07-0266
9. Baudouin C, Denoyer A, Desbenoit N, Hamm G, Grise A. In vitro and in vivo experimental studies on trabecular meshwork degeneration induced by benzalkonium chloride (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc. 2012;110:40–63.
10. Misiuk-Hojlo M, Pomorska M, Mulak M, et al. The RELIEF study: tolerability and efficacy of preservative-free latanoprost in the treatment of glaucoma or ocular hypertension. Eur J Ophthalmol. 2019;29(2):210–215. doi:10.1177/1120672118785280
11. Pauly A, Roubeix C, Liang H, Brignole-Baudouin F, Baudouin C. In vitro and in vivo comparative toxicological study of a new preservative-free latanoprost formulation. Invest Ophthalmol Vis Sci. 2012;53(13):8172–8180. doi:10.1167/iovs.12-10766
12. Janson BJ, Alward WL, Kwon YH, et al. Glaucoma-associated corneal endothelial cell damage: a review. Surv Ophthalmol. 2018;63(4):500–506. doi:10.1016/j.survophthal.2017.11.002
13. Baudouin C, Kolko M, Melik-Parsadaniantz S, Messmer EM. Inflammation in Glaucoma: from the back to the front of the eye, and beyond. Prog Retin Eye Res. 2021;83:100916. doi:10.1016/j.preteyeres.2020.100916
14. Jaenen N, Baudouin C, Pouliquen P, Manni G, Figueiredo A, Zeyen T. Ocular symptoms and signs with preserved and preservative-free glaucoma medications. Eur J Ophthalmol. 2007;17(3):341–349. doi:10.1177/112067210701700311
15. Leung EW, Medeiros FA, Weinreb RN. Prevalence of ocular surface disease in glaucoma patients. J Glaucoma. 2008;17(5):350–355. doi:10.1097/IJG.0b013e31815c5f4f
16. Aptel F, Cucherat M, Denis P. Efficacy and tolerability of prostaglandin-timolol fixed combinations: a meta-analysis of randomized clinical trials. Eur J Ophthalmol. 2012;22(1):5–18. doi:10.5301/ejo.5000009
17. Bangalore S, Kamalakkannan G, Parkar S, Messerli FH. Fixed-dose combinations improve medication compliance: a meta-analysis. Am J Med. 2007;120(8):713–719. doi:10.1016/j.amjmed.2006.08.033
18. Cheng JW, Cheng SW, Gao LD, Lu GC, Wei RL. Intraocular pressure-lowering effects of commonly used fixed-combination drugs with timolol: a systematic review and meta-analysis. PLoS One. 2012;7(9):e45079. doi:10.1371/journal.pone.0045079
19. Inoue K, Okayama R, Higa R, Sawada H, Wakakura M, Tomita G. Ocular hypotensive effects and safety over 3 months of switching from an unfixed combination to latanoprost 0.005%/timolol maleate 0.5% fixed combination. J Ocul Pharmacol Ther. 2011;27(6):581–587. doi:10.1089/jop.2011.0057
20. Pfeiffer N; European Latanoprost Fixed Combination Study Group. A comparison of the fixed combination of latanoprost and timolol with its individual components. Graefes Arch Clin Exp Ophthalmol. 2002;240(11):893–899. doi:10.1007/s00417-002-0553-0
21. Higginbotham EJ. Considerations in glaucoma therapy: fixed combinations versus their component medications. Clin Ophthalmol. 2010;4:1–9.
22. Guven Yilmaz S, Degirmenci C, Karakoyun YE, Yusifov E, Ates H. The efficacy and safety of bimatoprost/timolol maleate, latanoprost/timolol maleate, and travoprost/timolol maleate fixed combinations on 24-h IOP. Int Ophthalmol. 2018;38(4):1425–1431. doi:10.1007/s10792-017-0601-8
23. Bhagat P, Sodimalla K, Paul C, et al. Efficacy and safety of benzalkonium chloride-free fixed-dose combination of latanoprost and timolol in patients with open-angle glaucoma or ocular hypertension. Clin Ophthalmol. 2014;8:1241–1252. doi:10.2147/OPTH.S64584
24. Uusitalo H, Chen E, Pfeiffer N, et al. Switching from a preserved to a preservative-free prostaglandin preparation in topical glaucoma medication. Acta Ophthalmol. 2010;88(3):329–336. doi:10.1111/j.1755-3768.2010.01907.x
25. Erb C, Stalmans I, Iliev M, Muñoz-Negrete FJ. Real-world study on patient satisfaction and tolerability after switching to preservative-free latanoprost. Clin Ophthalmol. 2021;15:931–938. doi:10.2147/OPTH.S295821
26. Wong TT, Aung T, Ho CL. Ocular surface status in glaucoma and ocular hypertension patients with existing corneal disorders switched from latanoprost 0.005% to tafluprost 0.0015%: comparison of two prostaglandin analogues with different concentrations of benzalkonium chloride. Clin Exp Ophthalmol. 2018;46(9):1028–1034. doi:10.1111/ceo.13329
27. European Medicines Agency. EMEA public statement on antimicrobial preservatives in ophthalmic preparations for human use; 2009.
28. Aptel F, Pfeiffer N, Schmickler S, et al. Noninferiority of preservative-free versus BAK-preserved latanoprost-timolol fixed combination eye drops in patients with open-angle glaucoma or ocular hypertension. J Glaucoma. 2019;28(6):498–506. doi:10.1097/IJG.0000000000001248
29. McMonnies CW, Chapman-Davies A. Assessment of conjunctival hyperemia in contact lens wearers. Part I. Am J Optom Physiol Opt. 1987;64(4):246–250. doi:10.1097/00006324-198704000-00003
30. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
31. Lemp MA. Report of the National Eye Institute/Industry workshop on clinical trials in dry eyes. CLAO J. 1995;21(4):221–232.
32. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the Ocular Surface Disease Index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
33. Lou H, Wang H, Zong Y, Cheng JW, Wei RL. Efficacy and tolerability of prostaglandin-timolol fixed combinations: an updated systematic review and meta-analysis. Curr Med Res Opin. 2015;31(6):1139–1147. doi:10.1185/03007995.2015.1039504
34. Rouland JF, Traverso CE, Stalmans I, et al. Efficacy and safety of preservative-free latanoprost eyedrops, compared with BAK-preserved latanoprost in patients with ocular hypertension or glaucoma. Br J Ophthalmol. 2013;97(2):196–200. doi:10.1136/bjophthalmol-2012-302121
35. Cucherat M, Stalmans I, Rouland JF. Relative efficacy and safety of preservative-free latanoprost (T2345) for the treatment of open-angle glaucoma and ocular hypertension: an adjusted Indirect comparison meta-analysis of randomized clinical trials. J Glaucoma. 2014;23(1):e69–75. doi:10.1097/IJG.0b013e3182a075e6
36. El Ameen A, Vandermeer G, Khanna RK, Pisella PJ. Objective ocular surface tolerance in patients with glaucoma treated with topical preserved or unpreserved prostaglandin analogues. Eur J Ophthalmol. 2019;29(6):645–653. doi:10.1177/1120672118805877
37. Hedengran A, Steensberg AT, Virgili G, Azuara-Blanco A, Kolko M. Efficacy and safety evaluation of benzalkonium chloride preserved eye-drops compared with alternatively preserved and preservative-free eye-drops in the treatment of glaucoma: a systematic review and meta-analysis. Br J Ophthalmol. 2020;104(11):1512–1518. doi:10.1136/bjophthalmol-2019-315623
38. Majumdar S, Hippalgaonkar K, Repka MA. Effect of chitosan, benzalkonium chloride and ethylenediaminetetraacetic acid on permeation of Acyclovir across isolated rabbit cornea. Int J Pharm. 2008;348(1–2):175–178. doi:10.1016/j.ijpharm.2007.08.017
39. Bourne RRA, Kaarniranta K, Lorenz K, Traverso CE, Vuorinen J, Ropo A. Changes in ocular signs and symptoms in patients switching from bimatoprost-timolol to tafluprost-timolol eye drops: an open-label Phase IV study. BMJ Open. 2019;9(4):e024129. doi:10.1136/bmjopen-2018-024129
40. Batra R, Tailor R, Mohamed S. Ocular surface disease exacerbated glaucoma: optimizing the ocular surface improves intraocular pressure control. J Glaucoma. 2014;23(1):56–60. doi:10.1097/IJG.0b013e318264cd68
41. Sedgwick P, Greenwood N. Understanding the Hawthorne effect. BMJ. 2015;351:h4672. doi:10.1136/bmj.h4672
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bimatoprost Intracameral Implant (Durysta®): A New Era in Glaucoma Management Through Sustained-Release Innovation
Vagiakis I, Papadopoulou EP, Amaxilati E, Tsiropoulos GN, Konstas AG, Panos GD
Drug Design, Development and Therapy 2025, 19:703-714
Published Date: 31 January 2025
Efficacy and Safety of Preservative-Free Bimatoprost 0.01% Gel in Patients with Open-Angle Glaucoma and Ocular Hypertension: Results from Two Phase III Randomized Trials
Bacharach J, Miller-Ellis E, Harasymowycz P, Peace JH, Nissle S, Day DG, Stalmans I
Clinical Ophthalmology 2026, 20:571715
Published Date: 12 April 2026