Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Toad Poisoning: Clinical Characteristics and Outcomes
Authors Trakulsrichai S ![]() , Chumvanichaya K
, Chumvanichaya K ![]() , Sriapha C
, Sriapha C ![]() , Tongpoo A, Wananukul W
, Tongpoo A, Wananukul W
Received 19 July 2020
Accepted for publication 8 September 2020
Published 16 December 2020 Volume 2020:16 Pages 1235—1241
DOI https://doi.org/10.2147/TCRM.S272863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Satariya Trakulsrichai,1,2 Kritsada Chumvanichaya,1,3 Charuwan Sriapha,2 Achara Tongpoo,2 Winai Wananukul2,4
1Department of Emergency Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand; 2Ramathibodi Poison Center, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand; 3Emergency Department, Somdech Phra Pinklao Hospital, Bangkok 10600, Thailand; 4Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand
Correspondence: Satariya Trakulsrichai
Department of Emergency Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand
Tel +66-2-2011484
Fax +66-2-2012404
Email [email protected]
Objective: This study was performed to describe the clinical characteristics and outcomes of patients with toad poisoning in Thailand.
Methods: We carried out a retrospective study of patients with toad poisoning from the Ramathibodi Poison Center Toxic Exposure Surveillance System during a 5-year period (2012– 2016).
Results: We studied 36 patients poisoned by toad toxin. The median age was 31 years. Most patients were male (66.7%) and had ingested toad meat (50%). The most common presentation was gastrointestinal (GI) symptoms with a median onset of 2 h after ingestion. Twelve patients presented with bradycardia; seven presented with shock and one with cardiac arrest. In the initial EKGs of all patients, the most common abnormality was sinus bradycardia.Two patients developed cardiac arrest early during management in the emergency room (within 15 minutes after ER arrival or within 4.5 h after ingestion). During admission, one patient developed sinus bradycardia, and two developed bradyarrhythmia; however, all three were stable. No tachyarrhythmias such as ventricular tachycardia were detected in any patient. Some patients (11.1%) presented with hyperkalemia. Serum digoxin was detected in five of seven patients tested, ranging from 0.43 to > 8 ng/mL. Most patients (75%) were admitted to the hospital; the median duration of hospitalization was 2 d (range 0.5– 5 d). The overall mortality rate was 8.3%, and all three patients that died ate toad meat and/or eggs and developed cardiac arrest. All patients received supportive with/without symptomatic care including GI decontamination, inotropic drugs, cardiac pacing, and management of hyperkalemia. One patient received intravenous calcium for hyperkalemia but did not develop dysrhythmia after calcium administration. One patient received digoxin-specific antibody fragments (DsFab), after which he clinically improved and was discharged.
Conclusion: Toad poisoning commonly caused GI symptoms and bradycardia. However, in severe cases, death occurred. Tachyarrhythmia was not observed. Supportive, symptomatic care might be the main therapies for this poisoning, especially if DsFab is not available.
Keywords: toads, bufotoxin, bufadienolide, cardioactive steroids, cardiac glycosides, digoxin-specific antibody fragments
Introduction
Cardioactive steroids (CAS) are naturally occurring compounds that consist of a steroid nucleus and an unsaturated 5- or 6-membered lactone ring.1–3 CAS are classified as a cardenolide or a bufadienolide and can be found in plants and animals.1–3 Most bufadienolides, such as bufalin, are derived from mammals and amphibians including some species of toads (in the genus Bufo in the family Bufonidae).1–5 Cardiac glycosides refer to cardioactive steroids that also contain sugar residues such as digoxin.2
CAS inhibit sodium–potassium ATPase, mainly in cardiac tissue.3 The predominant features of acute CAS poisoning include gastrointestinal (GI) symptoms, hyperkalemia, cardiotoxicity including bradycardia, varying degrees of heart block, and dysrhythmias.3
Toad toxin is present in the secretions of the skin, parotid glands, and eggs of some toads.2–7 The toxin is likely resistant to destruction by heating or cooking.8–10
Currently, there are several reports of toad poisoning in humans;6–15 the clinical features resemble digoxin toxicity and testing for serum digoxin may yield positive results. Toad poisoning was commonly reported from the ingestion of toad meat or eggs, aphrodisiac pills (such as “Love Stone”), and herbal or traditional medicines (such as Chan Su).6–15 However, intravenous injection of toad extract is also reported and contributed to the death of one young male patient.16 Toad poisoning is associated with high mortality.1
Every year, patients with toad poisoning are referred and consulted to the Ramathibodi Poison Center (RPC). The present study was performed to describe and clarify the clinical characteristics and outcomes of patients with toad poisoning in Thailand.
Materials and Methods
Study Design
We performed a 5-year retrospective study (January 2012–December 2016) using data collected from the RPC Toxic Exposure Surveillance System, which is the database of our poison center. The primary objective was to describe the clinical characteristics and outcomes in patients with toad poisoning in Thailand during the 5-year period.
Study Setting and Population
The study setting was a poison center of a tertiary teaching hospital in Thailand. Most queries to the RPC are from medical personnel; the RPC responds to approximately 15,000–20,000 consultation requests/year. Follow-up telephone calls are periodically made to collect data and monitor patient progress, to provide ongoing treatment recommendations, and to determine the patients’ medical outcomes. All cases are recorded in the RPC Toxic Exposure Surveillance System database and are verified by a team of information scientists and medical toxicologists. The diagnosis of toad poisoning was primarily based on a history of toad ingestion with the clinical presentation of poisoning at the hospital. Patients who coingested other cardiac glycoside drugs or illicit drugs or herbal medicine or overdose of pharmaceutical drugs with toads were excluded from the study.
Study Protocol
For patients who met the inclusion criteria, we collected the following data: demographics, medical history, clinical features, laboratory results, treatments, follow-up details, final diagnosis, and outcome.
Hyperkalemia and hypokalemia were defined as measured serum potassium >5.5 mEq/L and <3.5 mEq/L, respectively.17 Acute kidney injury was diagnosed based on clinical history and laboratory data using the Kidney Disease: Improving Global Outcomes clinical practice guideline.18 We assumed that all patients without known underlying disease were healthy and previously had normal kidney function. Hypotension was defined as systolic blood pressure <90 mmHg.19 A heart rate greater than 100 beats per minute was defined as tachycardia, and a heart rate fewer than 60 beats per minute was defined as bradycardia.20 The normal vital signs in pediatric patients were based on the normal values for each age.21
We used Excel (Microsoft Corp., Redmond, WA, USA) to collect and analyze the data. The mean and standard deviation were used for continuous data with normal distribution; otherwise, the median with minimum and maximum were used. The frequency and percentage were used for categorical data analysis.
Results
A total of 36 patients from 24 RPC telephone consultations were included; patient characteristics are summarized in Table 1. No patients were excluded from the study; that is, none of the patients had coingested other drugs or substances with toads. Thirteen patients were younger than 15 years old. All patients had ingested toads as food, except four patients; one child accidentally ingested toad skin secretion when she caught an alive toad, another child caught an alive toad and then bit the toad. For the other 2 patients, one ingested dried meat of one toad as a health supplement, and the other patient deliberately ingested toad pickled eggs after arguing with her spouse as the intentional ingestion. Twenty-six patients cooked toads before eating, 3 patients did not cook and 7 patients did not have the detail of cooking noted in their records. Two patients reported that they had underlying diseases (one with schizophrenia and the other with an unspecified psychiatric condition).
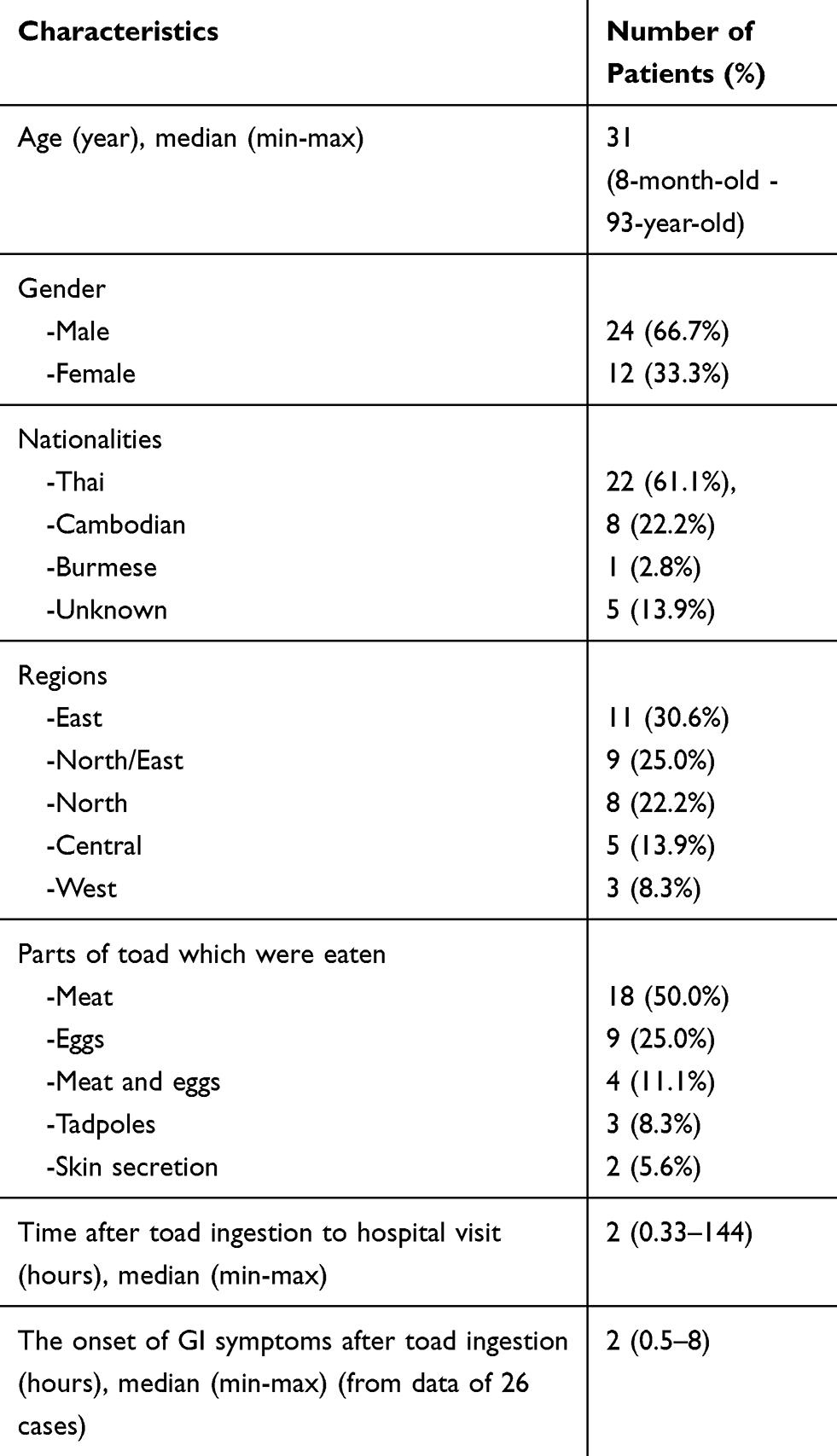 |
Table 1 The Clinical Characteristics of the Patients (36 Patients) |
At the first presentation, 34 patients reported GI symptoms including nausea, vomiting, and abdominal pain -after ingestion. The other two patients did not have GI symptoms noted in their records; one presented with cardiac arrest and the other had agitation with severe bradycardia and developed cardiac arrest shortly after arrival in the emergency room (ER). None of the patients complained of visual abnormalities. Abnormal vital signs recorded at the hospital arrival in our data included bradycardia in 12 patients (33.3%), tachycardia in one (2.8%), and hypotension in seven (19.4%). All patients presented to the hospital with normal consciousness except three patients; one was drowsy, another was comatose, and the third patient was agitated. One patient presented with cardiac arrest and eventually died in the ER.
From the 29 initial EKGs recorded, the abnormal findings showed sinus bradycardia (12 patients), atrial fibrillation with slow ventricular response (one patient), complete heart block (one patient), and normal sinus rhythm with occasional premature ventricular contractions (one patient).
During observation and management in the ER, two patients developed cardiac arrest approximately 10–15 minutes after presenting to the ER (at 2 h and 4.5 h after toad ingestion). The EKG during cardiac arrest noted in the records showed pulseless electrical activity in two patients.
For the initial laboratory results, the mean of the initial potassium recorded in 27 patients was 4.2 mEq/L. From the data of 32 patients, four and five had hyperkalemia (range 5.5–7.7 mEq/L) and hypokalemia (range 2.8–3.48 mEq/L), respectively. Results for the initial serum calcium and magnesium concentrations were only noted for some patients. Two of five patients whose serum calcium concentration was recorded had hypercalcemia. Three of seven patients whose serum magnesium concentration was recorded had abnormal results.
The median initial serum creatinine concentration was 0.83 mg/dL (range 0.3–2.8 mg/dL). Four patients had an elevated serum creatinine concentration (range 1.37–2.8 mg/dL). Serum digoxin concentrations were measured and recorded for seven patients. The laboratory methods for serum digoxin testing in each hospital were not described. Serum digoxin concentration was detected and determined in five patients (range 0.43 to >8 ng/mL), measured at 1–24 h after toad consumption. The highest concentration (>8 ng/mL) was detected in one patient who died.
Most patients (75%) admitted to the hospital had a median stay of 2 d (range 0.5–5 d). During the admission evaluation, one patient developed sinus bradycardia of 30–50 beats/minute, two developed bradyarrhythmia (specific type not recorded); however, all three patients were stable. No ventricular tachycardia or ventricular fibrillation were detected in any of the patients.
The management is summarized in Table 2. Three patients were intubated with an endotracheal tube during the cardiac arrest resuscitation. None received cardioversion or defibrillation during admission. All patients received supportive with/without symptomatic care.
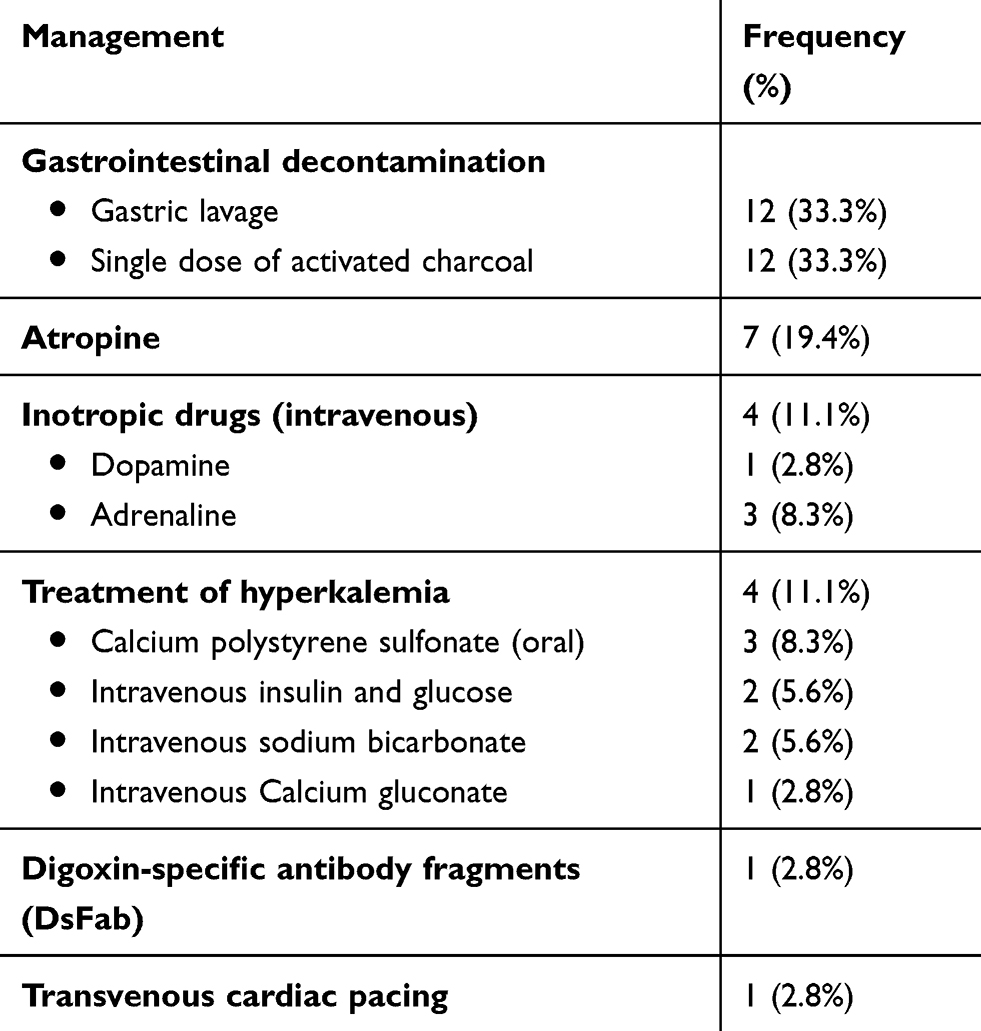 |
Table 2 The Management of All Patients During the Hospitalization |
One 51-year-old male patient with no definite underlying illness received digoxin-specific antibody fragments (DsFab) as digoxin immune Fab (DigiFab®, BTG International Inc., Conshohocken, PA, USA) at 1 d after eating toad meat. He had hypotension (blood pressure 80/40 mmHg), complete heart block with pulse rate 37 beats/minute, hyperkalemia (serum potassium concentration 7.7 mEq/L), and elevated creatinine concentration (1.6 mg/dL) at presentation to the hospital. He was on inotropic drugs and transvenous cardiac pacing. He was given 10 vials of DsFab approximately 1 d after ingestion. The complete heart block turned to second-degree AV block Mobitz type 1 for approximately 1–2 h after DsFab treatment. His initial serum digoxin concentration was 0.62 ng/mL at approximately 6–7 h after ingesting the toad meat, increased to >4 ng/mL after DsFab treatment and decreased to 1.76 ng/mL on day 5. He was discharged 5 d after admission.
In this study, the mortality rate was 8.3%. The data of three dead patients are shown in Table 3.
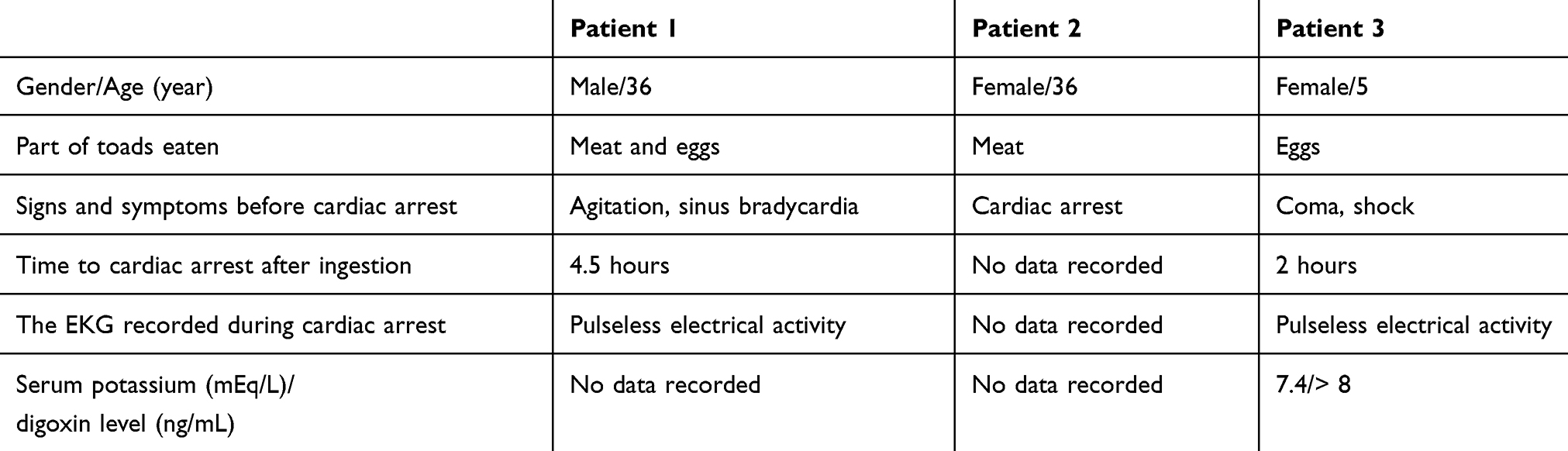 |
Table 3 The Clinical Features of 3 Fatal Patients |
Discussion
With 36 patients studied over a 5-year period, including patients ranging from infants to older individuals, this is one of the largest studies of toad poisoning cases reported to date.
Bufo melanostictus is distributed widely across south and southeast Asia,8,22,23 and is found throughout Thailand.22,23 We therefore postulated that this toad species was responsible for causing the poisoning in our patients.
Most of our patients ate toads; therefore, toad consumption might be a local tradition for some people—not only Thai but also other people of Asian ethnicity in Thailand. Therefore, toad poisoning is an important health problem in Thailand, also causing fatalities. Public education on the awareness and seriousness of toad toxins could be a useful public health measure and might play an important role in the prevention of this kind of poisoning.
GI symptoms were the most common clinical presentation and occurred very early in our patients (within 8 h) after ingestion. This finding was consistent with other reports.8,13,15 Therefore, GI symptoms could represent the early manifestation of this poisoning and alert physicians to admit and observe these patients.
The abnormal EKGs at presentation showed sinus bradycardia in most patients with bradyarrhythmia in a few patients. Together with EKG results during hospitalization or EKG during cardiopulmonary resuscitation (CPR) in three patients who died, the common finding was sinus bradycardia and rarely bradyarrhythmia. Moreover, no tachyarrhythmia was detected in any of our patients. Our finding was different from the other reports in which tachyarrhythmia was noted in some patients who had severe toad poisoning.10,13–15 In one study of yellow oleander (a plant that contains CAS) poisoning from Sri Lanka.24 The authors found that few patients developed atrial or ventricular tachyarrhythmias or ventricular ectopic beats. However, because of the retrospective nature of our study, we might have missed some transient events such as ventricular tachyarrhythmia during CPR or hospitalization.
Some patients had hyperkalemia that was consistent with acute CAS poisoning. One case report found that the serum potassium concentration had prognostic implications in toad intoxication9 In our study, two patients with serum potassium >7 mEq/L presented with severe initial symptoms; one with cardiac arrest at presentation and the other one with complete heart block. Nonetheless, some patients presented with hypokalemia that might relate to their GI symptoms. Taken together, we concluded that toad poisoning from ingestion of toads as food commonly present with GI symptoms, bradycardia, and occasionally hyperkalemia—symptoms that resemble acute digoxin poisoning.
Serum digoxin concentrations were measured within 1 d after ingestion and could be detected in five patients. Because digoxin concentrations were measured in different hospitals (not our hospital), we assumed that the measurement methods for digoxin concentration were immunoassay methods that are commonly used in clinical laboratories to determine serum or plasma digoxin concentrations in therapeutic drug monitoring.25 Our study helps confirm that the digoxin concentration can be detected and measured by nonspecific digoxin assays in patients with toad intoxication, consistent with other studies.8,13,15
In our study, three patients died, which resulted in the high mortality rate. This finding supported those of a systematic review of 27 patients with bufadienolide poisoning that showed a mortality rate as high as 29.6%.1 These three patients died very early after toad ingestion. This was consistent with the findings reported by others, in which the majority of deaths occurred within 24 h after ingestion.8,13,15
Because severe clinical sequelae, including death, occurred early in the first day after ingestion, close observation and monitoring should be implemented in all patients, particularly early in the course of poisoning.
Most patients in our study had a mild clinical course and could be discharged within 2 d; therefore, supportive and symptomatic treatment could be the main management in all patients with this type of poisoning and contribute to a good clinical outcome in most patients, even those who did not receive the antidote.
One patient received calcium for hyperkalemia but survived without subsequent cardiac dysrhythmia; this observation supports the finding from another study that intravenous calcium does not seem to cause malignant dysrhythmias.26
DsFab are reportedly effective in the treatment and reversal of the clinical manifestations of toad poisoning resulting from ingestion of a purported topical aphrodisiac.13 DsFab as DigiFab® used to be included in our national antidote program, but it is no longer included in the antidote list.27 In Thailand, the decision for DsFab treatment might depend on and/or be complicated by multiple factors such as the treating physician’s decisions, DsFab availability at that time, the transport time to access the antidote, and changes in the signs and symptoms as the clinical course improves or progresses after supportive care. These factors might partially explain why only one patient received this antidote.
Some experts include poisoning with a nondigoxin cardioactive steroid as an indication for administering DsFab.28 By that criterion, all of our patients should have received the antidote. In the setting of digoxin-related life-threatening dysrhythmias or high serum potassium concentration, if we excluded three patients who developed cardiac arrest very early, we could identify two indications for treating with DsFab. Those indications are any digoxin-related life-threatening dysrhythmia or serum potassium concentration >5 mEq/L in the setting of acute digoxin poisoning.28 By those criteria, seven patients should have received this antidote; however, only one such patient received DsFab. The other six patients survived with supportive and symptomatic treatment. If we used serum potassium concentration >6 mEq/L.29,30 As an indication, instead of >5 mEq/L, six patients should have received the antidote; however, again, only one patient received DsFab. The other five patients survived with supportive and symptomatic treatment.
Accordingly, from our findings together with the high price31 and limited availability of the antidote, the specific antidote (DsFab) should be considered as antidote therapy and administered appropriately and early in severe cases (life-threatening dysrhythmia, hyperkalemia, or hemodynamic instability). However, the antidote might not be required in all instances of toad poisoning, especially for ingesting the animal itself rather than the processed or dried toxin. Further study and more patient data are needed to determine the specific indications for and doses of DsFab for toad poisoning.
Our study has some limitations. First, the study was retrospective and based on data obtained from telephone consultations; therefore, some data might be incomplete. The medical history was obtained from patients as reported to medical personnel; therefore, sometimes this information might not be clear or completely accurate. Second, a small number of patients were included in this study. Finally, no laboratory test was performed to confirm the identity of the specific toad toxin.
Conclusion
GI symptoms and bradycardia were commonly seen in patients with toad poisoning; severe cases can be fatal. None of the patients we studied developed tachyarrhythmia. The main therapies for this type of poisoning might be supportive and symptomatic care, especially if DsFab is unavailable. DsFab should be considered and administered appropriately and early in severe cases. Further study is needed to determine the specific indications for and doses of DsFab for toad poisoning.
Data Sharing Statement
The data are not available for public access because of patient privacy concerns but are available from the corresponding author upon reasonable request.
Ethical Approval
This study was approved by the Institutional Ethics Committee Board of Ramathibodi Hospital Faculty of Medicine, Mahidol University. The Ethics Approval Reference Number is COA. MURA2020/575. Because this is a retrospective study that used the pre-existing confidential database from the poison center, in which data were previously recorded, patient consent was not required by our hospital’s ethics committee board. The results of this study have been reported anonymously.
Funding
We declare no funding for this study.
Disclosure
The authors report no conflict of interest.
References
1. Barrueto F
2. Roberts DM, Gallapatthy G, Dunuwille A, Chan BS. Pharmacological treatment of cardiac glycoside poisoning. Br J Clin Pharmacol. 2016;81(3):488–495. doi:10.1111/bcp.12814
3. Qi J, Zulfiker AHM, Li C, Good D, Wei MQ. The development of toad toxins as potential therapeutic agents. Toxins (Basel). 2018;10(8):336. doi:10.3390/toxins10080336
4. Radford DJ, Gillies AD, Hinds JA, Duffy P. Naturally occurring cardiac glycosides. Med J Aust. 1986;144(10):540–544. doi:10.5694/j.1326-5377.1986.tb112283.x
5. Gao H, Zehl M, Leitner A, Wu X, Wang Z, Kopp B. Comparison of toad venoms from different Bufo species by HPLC and LC–DAD–MS/MS. J Ethnopharmacol. 2010;131(2):368–376. doi:10.1016/j.jep.2010.07.017
6. Cha K, So BH, Jeong WJ. Bufotoxin poisoning that showed the sign of acute digitalis overdose in the patient of Kyushin® intoxication. Hong Kong J Emerg Med. 2020;27(3):180–184. doi:10.1177/1024907918807526
7. Isoardi K, Lee S, Burren JM, George J, Goggin A, Chan BS. Bufadienolide toxicity in a child following cane toad egg ingestion. Emerg Med Australas. 2018;30(5):728–729. doi:10.1111/1742-6723.13150
8. Keomany S, Mayxay M, Souvannasing P, et al. Toad poisoning in Laos. Am J Trop Med Hyg. 2007;77(5):850–853. doi:10.4269/ajtmh.2007.77.850
9. Chi HT, Hung DZ, Hu WH, Yang DY. Prognostic implications of hyperkalemia in toad toxin intoxication. Hum Exp Toxicol. 1998;17(6):343–346. doi:10.1177/096032719801700610
10. Jan SL, Chen FL, Hung DZ, Chi CS. Intoxication after ingestion of toad soup: report of two cases. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi. 1997;38(6):477–480.
11. Ramkumar AG, Sakunthala SR, Rajasekaran D. An interesting case of cardiotoxicity due to bufotoxin (toad toxin). J Assoc Physicians India. 2011;59:737–738.
12. Kuo HY, Hsu CW, Chen JH, Wu YL, Shen YS. Life-threatening episode after ingestion of toad eggs: a case report with literature review. Emerg Med J. 2007;24(3):215–216. doi:10.1136/emj.2006.044602
13. Brubacher JR, Ravikumar PR, Bania T, Heller MB, Hoffman RS. Treatment of toad venom poisoning with digoxin-specific Fab fragments. Chest. 1996;110(5):1282–1288. doi:10.1378/chest.110.5.1282
14. Yei CC, Deng JF. [Toad or toad cake intoxication in Taiwan: report of four cases]. J Formos Med Assoc. 1993;92(Suppl 3):S135–S139. Chinese.
15. Gowda RM, Cohen RA, Khan IA. Toad venom poisoning: resemblance to digoxin toxicity and therapeutic implications. Heart. 2003;89(4):e14. doi:10.1136/heart.89.4.e14
16. Kostakis C, Byard RW. Sudden death associated with intravenous injection of toad extract. Forensic Sci Int. 2009;188(1–3):e1–e5. doi:10.1016/j.forsciint.2009.02.006
17. Petrino R, Marino R. Fluids and electrolytes. In: Tintinalli JE, editor. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide.
18. KDIGO. Clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2(1):6.
19. Nicks BA, Gaillard JP. Approach to nontraumatic shock. In: Tintinalli JE, editor. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide.
20. Michaud GF, Stevenson WG. Physiologic and non-physiologic sinus tachycardia. In: Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine.
21. Nelson LS, Howland MA, Lewin NA, et al. Initial evaluation of the patient: vital signs and toxic syndromes. In: Nelson LS, Howland MA, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS, editors. Goldfrank’s Toxicologic Emergencies,
22. U.S. Fish and Wildlife Service. Southeast Asian toad (Duttaphrynus melanostictus) ecological risk screening summary; 2018. Available from: https://www.fws.gov/fisheries/ANS/erss/highrisk/ERSS_Duttaphrynus_melanostictus_Final.pdf.
23. van Dijk PP, Iskandar D, Lau MWN, et al. 2004. Duttaphrynus melanostictus. The IUCN Red List of Threatened Species 2004. e.T54707A86445591. Available from: http://www.iucnredlist.org/details/full/54707/0.
24. Eddleston M, Ariaratnam CA, Sjöström L, et al. Acute yellow oleander (Thevetia peruviana) poisoning: cardiac arrhythmias, electrolyte disturbances, and serum cardiac glycoside concentrations on presentation to hospital. Heart. 2000;83(3):301–306. doi:10.1136/heart.83.3.301
25. Dasgupta A. Therapeutic drug monitoring of digoxin: impact of endogenous and exogenous digoxin-like immunoreactive substances. Toxicol Rev. 2006;25(4):273–281. doi:10.2165/00139709-200625040-00007
26. Levine M, Nikkanen H, Pallin DJ. The effects of intravenous calcium in patients with digoxin toxicity. J Emerg Med. 2011;40(1):41–46. doi:10.1016/j.jemermed.2008.09.027
27. Suchonwanich N, Wananukul W. Improving access to antidotes and antivenoms, Thailand. Bull World Health Organ. 2018;96(12):853–857. doi:10.2471/BLT.18.217075
28. Hack JB. Cardioactive steroids. In: Nelson LS, Howland MA, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS, editors. Goldfrank’s Toxicologic Emergencies.
29. Chan BSH, Buckley NA. Digoxin-specific antibody fragments in the treatment of digoxin toxicity. Clin Toxicol (Phila). 2014;52(8):824–836. doi:10.3109/15563650.2014.943907
30. Dawson AH, Buckley NA. Digoxin. Medicine. 2016;44:158–159. doi:10.1016/j.mpmed.2015.12.006
31. Johnson AR, Crouch B, Horowitz BZ. Discrepancies in reported US pricing information for digoxin-Fab. Clin Toxicol (Phila). 2015;53(1):71. doi:10.3109/15563650.2014.994065
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.