Back to Journals » Clinical Ophthalmology » Volume 20
To Evaluate the Agreement and Repeatability of the Eyerobo VS Portable Autorefractor Cycloplegic Refraction in Children and Adolescents
Authors Cui M, Zhou Y, He X, Hu L, Chen J, Yan C, He W, Qin G, Yu S
Received 31 December 2025
Accepted for publication 5 February 2026
Published 19 February 2026 Volume 2026:20 588537
DOI https://doi.org/10.2147/OPTH.S588537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Man Cui,1,2,* Yibing Zhou,2,3,* Xingru He,4 Lan Hu,2 Jiayan Chen,2 Chunhong Yan,4 Wei He,2 Guanghao Qin,2 Sile Yu4
1School of Visual Sciences, He University, Shenyang, People’s Republic of China; 2Department of Clinical Research, He Eye Specialist Hospital, Shenyang, People’s Republic of China; 3School of Public Health, Dalian Medical University, Dalian, People’s Republic of China; 4School of Public Health, He University, Shenyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guanghao Qin, Department of Clinical Research, He Eye Specialist Hospital, Shenyang, People’s Republic of China, Email [email protected] Sile Yu, School of Public Health, He University, Shenyang, People’s Republic of China, Email [email protected]
Purpose: To assess the agreement of the Eyerobo VS with the ARK-1 and subjective refraction (SR) and repeatability of the Eyerobo VS three measurements cycloplegic refraction in children and adolescents.
Patients and Methods: This study included 158 participants (316 eyes) aged 10.33 ± 2.10. All participants underwent eye examinations, including the ARK-1, the Eyerobo VS, and SR. The refractive error-related parameters included Sphere, spherical equivalent (SE), J0, and J45. Bland-Altman analysis was used to assess the agreement between the Eyerobo VS and the ARK-1 and the agreement between the Eyerobo VS and SR. The intraclass correlation coefficient (ICC) was used to evaluate the repeatability of the Eyerobo VS three measurements.
Results: The Eyerobo VS showed agreement with the ARK-1 within 0.5 D of 81.0% (Sphere), 79.4% (SE), 96.8% (J0), and 99.7% (J45). The Eyerobo VS showed agreement with SR within 0.5 D of 82.9% (Sphere), 79.4% (SE), 96.2% (J0), and 100.0% (J45). The ICC for the three measurements of the Eyerobo VS was 0.97 for Sphere and 0.95 for SE, respectively.
Conclusion: The refractive measurement cycloplegic refraction of the Eyerobo VS showed high reliability and good agreement with the ARK-1 and SR on Sphere, SE, J0, and J45. The Eyerobo VS portable autorefractor could facilitate large-scale vision screening in schools and remote areas.
Keywords: refractive error, subjective refraction, autorefractor, Eyerobo VS, ARK-1
Introduction
Globally, at least 2.2 billion people have a vision impairment or blindness, of which over 1 billion cases could have been prevented or have yet to be addressed, according to the first World report on vision issued by the WHO.1 Uncorrected refractive error was the major cause of visual impairment (43%)2 and the second most common cause of blindness globally.3 Astigmatism, hyperopia, and myopia are common refractive errors that impact a sizable fraction of the global population. In particular, the number of people with myopia is increasing every year, reaching half of the world population by 2050.4 The global productivity loss associated with vision impairment from uncorrected myopia in adults was estimated at US$244 billion.5 Addressing uncorrected refractive error could yield a net economic impact of over US$250 billion annually.6
The reasons for this serious public health problem include barriers to availability and access to quality services, major shortages and maldistribution of well-trained personnel, and lack of suitable, well-maintained equipment and consumables.7 Due to the fact that many eye problems may be asymptomatic, vision screening plays a crucial role in detecting visual disorders in children and adolescents without signs of visual impairment.8 Effective vision screening facilitates early diagnosis and treatment, and reduces adverse effects on children and adolescents. Currently, the primary methods for measuring refractive error include subjective refraction (SR) and objective refraction (OR). As the gold standard for patient acceptance, SR is a clinically accepted and frequently performed procedure in optometric practice.9,10 The accuracy of SR relies on the response of the person being examined and the examiner’s skills.11 Thus, SR may be limited in vision screening. The autorefractor, such as the ARK-1 (Nidek, Japan), is commonly used by eye care practitioners worldwide and can quickly and conveniently measure refractive error in clinical practice.12,13 However, most autorefractors are relatively large, requiring that the instruments be mounted on a table.14 Therefore, the autorefractor is not convenient to move and use in large-scale vision screening. Thus, among children and adolescents, a convenient and easy-to-use method of vision screening is required.
The Eyerobo VS (Eyerobo, China) is a portable autorefractor (2WIN-S, Adaptica, Italy) that combines a photorefractometer with an occlude tube that blocks ambient light, allowing the exam to be performed in any lighting condition.15,16 It can measure the refraction, corneal reflex, pupil size and interpupillary distance simultaneously. This is especially important for children’s vision screening, as it allows greater relaxation of accommodation and better simulation of normal viewing conditions, leading to more accurate refractive results.17 The Eyerobo VS has advantages in vision screening.
A previous study15 has validated the effectiveness of the Eyerobo VS for vision screening in the presence of non-cycloplegia. However, to our knowledge, no studies have examined cycloplegic refraction in the Eyerobo VS vision screening in children and adolescents. However, cycloplegic refraction is the gold standard for epidemiological assessment of refractive error in the pediatric population.18–20 In ocular examinations of children under non-cycloplegic conditions, the influence of accommodation cannot be disregarded.21 Therefore, this study aimed to evaluate the repeatability and agreement of the Eyerobo VS with the ARK-1 and SR cycloplegic refraction in children and adolescents.
Materials and Methods
Study Participants
This cross-sectional study was approved by the Ethics Committee of He Eye Specialist Hospital (IRB (2023) K026.01). It was registered at ClinicalTrails.gov (NCT06346626) on March 26, 2024. All procedures were reviewed and approved by the local institutional ethical review board in accordance with the Declaration of Helsinki principles. Written informed consent was obtained from the participants and parents.
Patients who visited the Pediatric Ophthalmology Clinic at Shenyang He Eye Specialist Hospital were invited to participate in this study from August 2023 to April 2024. Inclusion criteria: (i) Ages 6–18 years; (ii) Best corrected visual acuity better than 0.1 logMAR (logarithm of the minimum angle of resolution) (6/7.5); (iii) Patients who visited the clinic and volunteered to participate in this study. Exclusion criteria: (i) Participants who could not cooperate in completing the examination; (ii) Suffering from other ocular diseases (such as closed-angle glaucoma, shallow anterior, etc.) that do not allow dilated pupil examination; (iii) Suffering from eye diseases such as strabismus and previous ocular surgeries; (iv) Non-compliant to dilated pupil examination; (v) Other medical conditions in the opinion of the principal investigator were not suitable to participates in the study.
Refractive Error-Related Parameters
Refraction measurements were compared using Sphere and spherical equivalent (SE = sphere + cylinder/2). Vector analysis was also used to compare the measurements. Since vector analysis considers both the direction and magnitude of the astigmatic cylinder when calculating refractive error statistically, it is a well-established technique for analyzing refractive error data. The following formulas, proposed by Thibos et al,22 were used to perform vector analysis: J0 denotes the horizontal cylindrical vector, and J45 denotes the oblique cylindrical vector.


Examination Procedures
One drop of Proparacaine Hydrochloride Eye Drops (Alcon Laboratories, Inc., USA) was administered five minutes later, followed by three drops of 1% cyclopentolate (Alcon Laboratories, Inc., USA) at ten-minute intervals to induce ciliary muscle paralysis. Refractive error tests were taken after 30 minutes. Each participant underwent one ARK-1 examination, three consecutive Eyerobo VS examinations, and one SR examination. The order of the ARK-1 and the Eyerobo VS examinations was randomized in a 1:1 ratio. Since SR required further adjustment and confirmation based on OR results, it was performed last. Tests were taken at least 15 minutes apart for each method. The autorefractor was calibrated before each test was conducted. All participants employed an identical autorefractor during the study. And SR was performed by the same trained ophthalmologist.
Statistical Analysis
The data were analyzed using SPSS statistics software (version 25.0; SPSS Inc., United States). Data were expressed as mean ± standard deviation (SD). Accounting for inter-eye correlation, the mixed-effects models were used to compare the Eyerobo VS with the ARK-1 and with SR.23 The intraclass correlation coefficient (ICC) was calculated for the repeatability of the Eyerobo VS three measurements, with values below 0.5 regarded as poor repeatability, 0.5–0.75 as moderate, 0.75–0.9 as good, and over 0.9 as outstanding.24 The Bland-Altman analysis with 95% limits of agreement (LoA) was used to assess the agreement between the Eyerobo VS and the ARK-1 and the agreement between the Eyerobo VS and SR. The percentage of the difference between the Eyerobo VS and the ARK-1 and between the Eyerobo VS and SR within 0.5 D was also calculated. It was deemed a clinically acceptable range when the difference between measurements from different methods was within thresholds of 0.5 D.10,25 Bland-Altman graphs were plotted using MedCalc statistical software (version 9.0.4, Ostend, Belgium). P value of <0.05 was considered to show statistical significance.
The G*Power 3.1.9.2 (Heinrich Heine Universität, Düsseldorf, Germany) program was utilized in this investigation to determine the paired t-test sample size. To reach the 90% power effect, at least 44 subjects were required, assuming that the α was 5% and the effect size of the two devices was 0.5.26,27 Simultaneously, McAlinden et al28 suggested that at least 100 subjects should be included in the sample size to assess the degree of agreement between the two approaches. Increasing the sample size allows for a more accurate assessment of the agreement range and provides tighter confidence intervals. Finally, 316 eyes of 158 participants were included in this study.
Results
Characteristics of Measurements by the Eyerobo VS, the ARK-1, and SR
The study included 316 eyes from 158 participants (72 males, 45.6%; 84 females, 54.4%), with a mean age of 10.33 ± 2.10 years. The characteristics of Sphere, SE, J0, and J45 measured by the Eyerobo VS, the ARK-1, and SR are shown in Table 1.
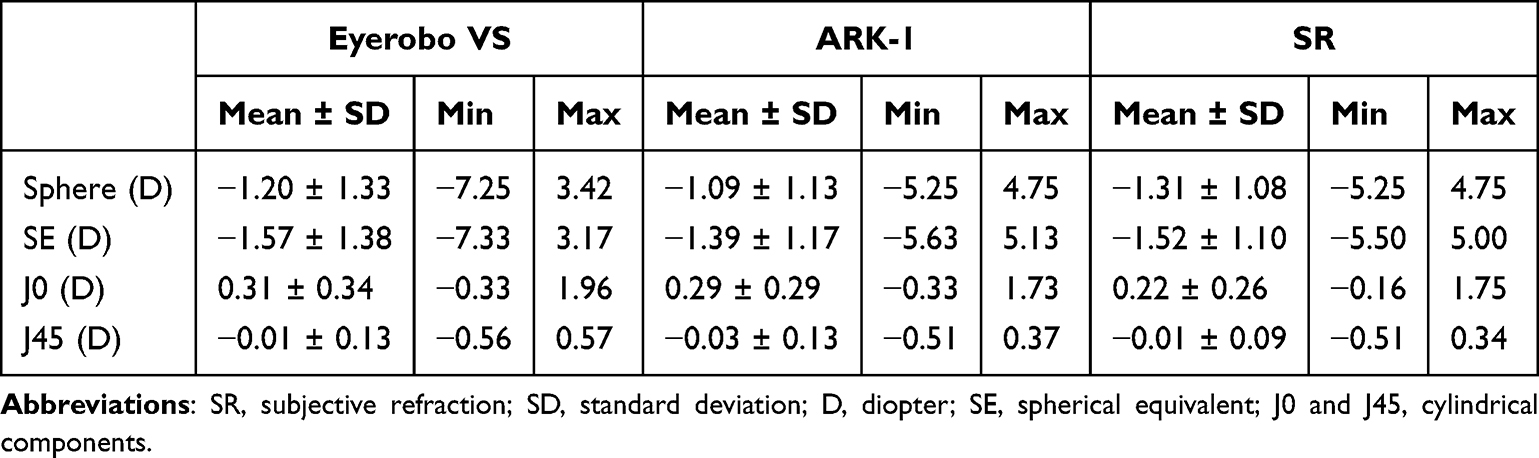 |
Table 1 Characteristics of Measurements by the Eyerobo VS, the ARK-1, and SR |
Comparison and Agreement of Measurements by the Eyerobo VS, the ARK-1, and SR
The difference and agreement of Sphere, SE, J0, and J45 measured by the Eyerobo VS, the ARK-1 and SR are shown in Table 2. Bland-Altman plots present the 95% LoA of Sphere, SE, J0, and J45 between the Eyerobo VS and the ARK-1 and between the Eyerobo VS and SR (Figures 1 and 2).
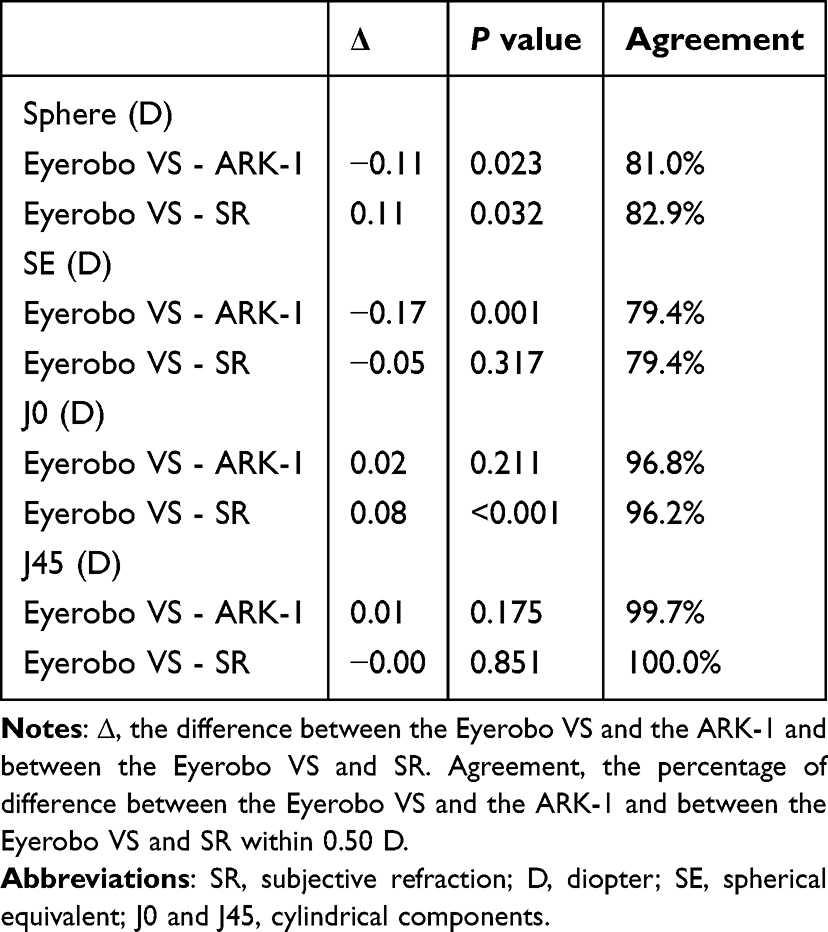 |
Table 2 Comparison and Agreement of Measurements by the Eyerobo VS, the ARK-1, and SR |
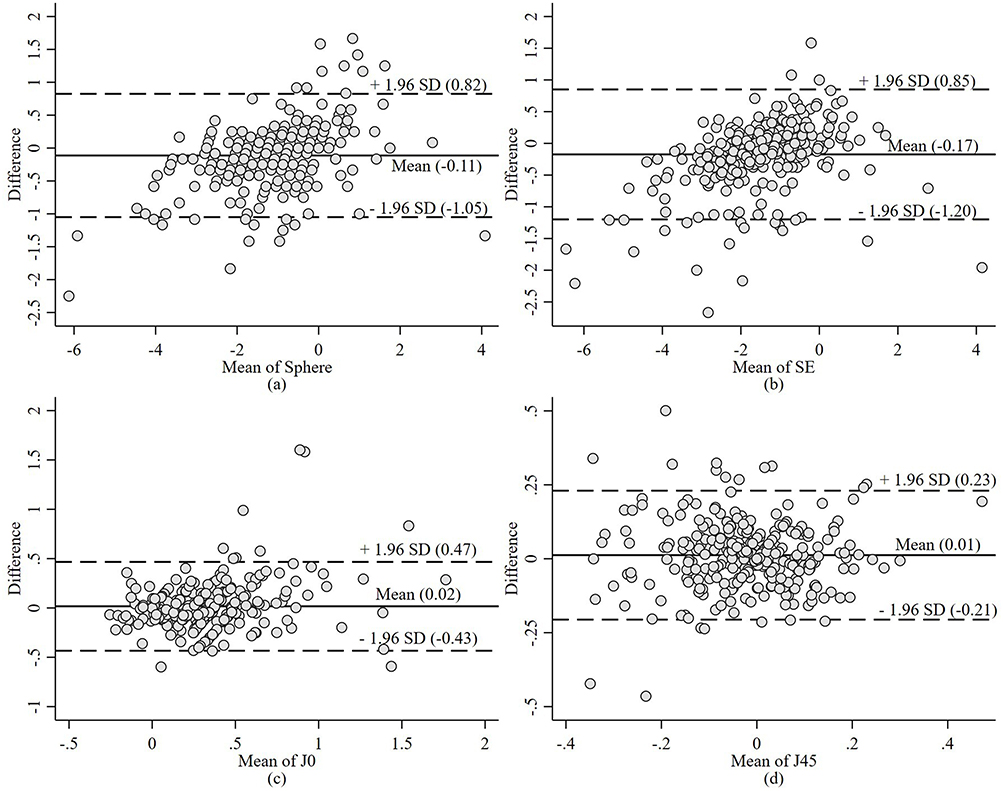 |
Figure 1 Plots of Bland-Altman comparing the Eyerobo VS and the ARK-1 for (a) Sphere, (b) SE, (c) J0, and (d) J45. Abbreviations: SD, standard deviation; SE, spherical equivalent; J0 and J45, cylindrical components. |
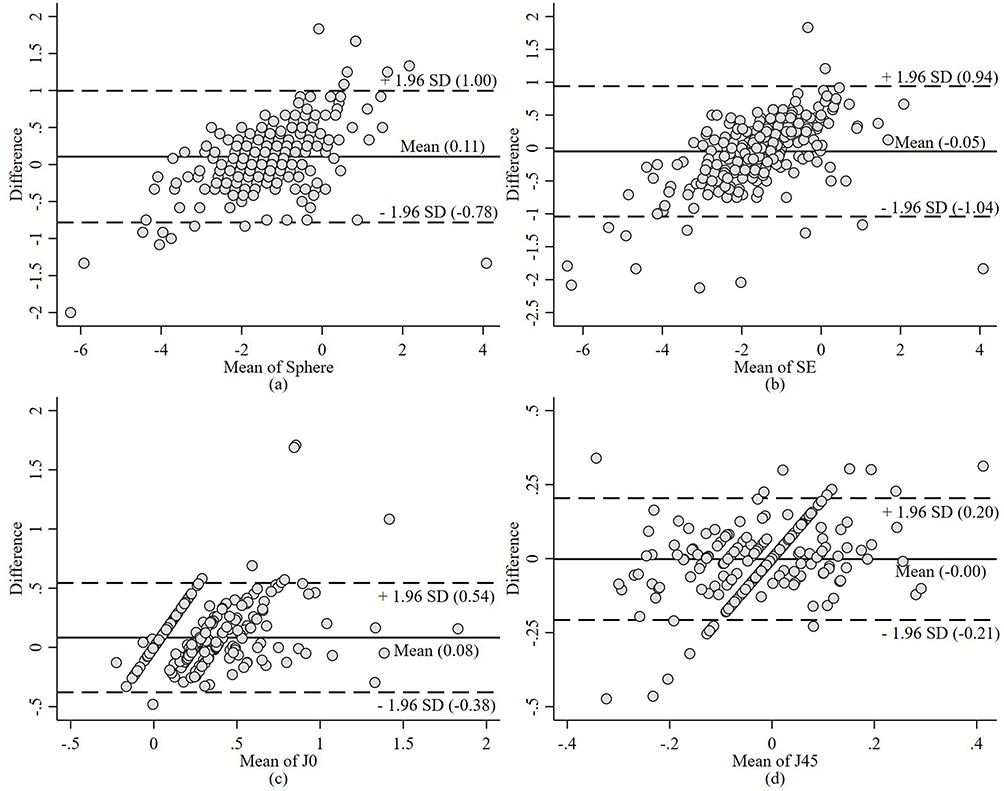 |
Figure 2 Plots of Bland-Altman comparing the Eyerobo VS and SR for (a) Sphere, (b) SE, (c) J0, and (d) J45. Abbreviations: SR, subjective refraction; SD, standard deviation; SE, spherical equivalent; J0 and J45, cylindrical components. |
The Eyerobo VS vs the ARK-1
Compared with the ARK-1, the Eyerobo VS showed significant differences in Sphere and SE. However, there were no significant differences in J0 and J45. The J0 and J45 differences between the Eyerobo VS and the ARK-1 were 0.02 (0.31 ± 0.34 D vs 0.29 ± 0.29 D, P = 0.211) and 0.01 (−0.01 ± 0.13 D vs −0.03 ± 0.13 D, P = 0.175), respectively. The Eyerobo VS showed agreement with the ARK-1 within 0.5 D of 81.0% (Sphere), 79.4% (SE), 96.8% (J0) and 99.7% (J45).
The Bland-Altman analysis of the data indicated 95% LoA between the Eyerobo VS and the ARK-1 of Sphere (−1.05 D, 0.82 D), SE (−1.20 D, 0.85 D), J0 (−0.43 D, 0.47 D), and J45 (−0.21 D, 0.23 D).
The Eyerobo VS vs SR
Compared with SR, the Eyerobo VS showed significant differences in Sphere and J0, but no significant differences in SE and J45. The SE and J45 differences between the Eyerobo VS and SR were −0.05 (−1.57 ± 1.38 D vs −1.52 ± 1.10 D, P = 0.317) and −0.00 (−0.01 ± 0.13 D vs −0.01 ± 0.09 D, P = 0.851), respectively. The Eyerobo VS showed agreement with SR within 0.5 D of 82.9% (Sphere), 79.4% (SE), 96.2% (J0) and 100.0% (J45).
The Bland-Altman analyses of the data indicated 95% LoA between the Eyerobo VS and SR of Sphere (−0.78 D, 1.00 D), SE (−1.04 D, 0.94 D), J0 (−0.38 D, 0.54 D), and J45 (−0.21 D, 0.20 D).
Repeatability of the Eyerobo VS
The repeatability of the Eyerobo VS three measurements is shown in Table 3. The ICC demonstrated outstanding repeatability for Sphere (0.97) and SE (0.95), respectively. The ICC demonstrated moderate repeatability for J0 (0.57) and J45 (0.64), respectively. The repeated measures ANOVA showed that within-subject differences for Sphere, SE, J0, and J45 were not statistically significant (P > 0.05).
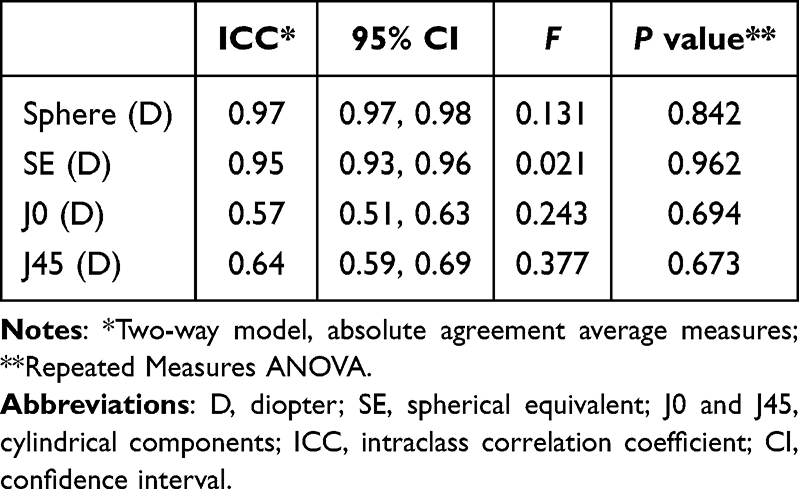 |
Table 3 Repeatability of the Eyerobo VS |
Discussion
The laborious manual retinoscopy process can be avoided using a portable autorefractor. A quick, accurate, and dependable instrument for objective measurement can serve as a foundation for SR. The study evaluated the agreement of the Eyerobo VS with the ARK-1 and SR and repeatability of the Eyerobo VS three measurements of cycloplegic refraction in children and adolescents. This study demonstrates that, compared to the ARK-1 and SR, Sphere, SE, J0, and J45 of the Eyerobo VS portable autorefractor exhibit good agreement (79.4%–100.0%). Numerous studies have been conducted on children to test the validity and reproducibility of autorefractor instruments installed on tables to measure refractive error.29–32 The Eyerobo VS three measurements demonstrated an outstanding repeatability for Sphere and SE, respectively.
Autorefractors are especially important in large-scale vision screening of children and remote areas. The agreement of Sphere, SE, J0, and J45 between the Eyerobo VS and the ARK-1 were 79.4%–99.7%. A recent study comparing the 2WIN with the ARK-1 showed the difference of cycloplegic SE was −0.37 D (95% LoA: −2.74 D, 2.00 D).33 The difference of SE was 0.46 D (95% LoA: −1.32 D, 2.24 D) observed among children aged 4–14 years, as determined by Liu et al15 when they compared the Eyerobo VS with cycloplegic retinoscopy. Compared with the study by Liu et al15 (software version 5.3), the Eyerobo VS (software version 5.6) in this study achieved better results and more accurate measurements. The differences of Sphere, SE, and J0 were smaller, and the difference of J45 was equal. The Eyerobo VS three measurements demonstrated an outstanding repeatability for Sphere and SE, respectively. The Eyerobo VS three measurements demonstrated a moderate repeatability for J0 and J45, respectively. The repeatability of three measurements by the Eyerobo VS in the present study showed that the repeatability of SE was better, J0 was worse, and J45 was close to the values in Liu et al,15 which may be inconsistencies in children and adolescents’ cooperation, alignment, and fixation, leading to different measurement results. In addition, the use of these devices in children without cycloplegia has been shown in the study to understate hyperopia and overestimate myopia.30 This may be due to children’s accommodation, which can affect the diagnostic accuracy of latent refractive defects.34
In practical lens fitting, SR is commonly used as the gold standard. During fitting, SR integrates the patient’s subjective experience with prescription strength. Most studies also frequently employ SR as the benchmark for comparing the accuracy of different autorefractors.10,15,17 Therefore, this study likewise used SR as the standard for comparison. The agreement of Sphere, SE, J0, and J45 between the Eyerobo VS and SR were 79.4%–100.0%. According to these preliminary findings, most pediatric patients may benefit from the Eyerobo VS for prescription glasses. A related study showed that the SE refraction obtained by open-view binocular handheld aberrometer wavefront autorefractor agreed within 0.5 D of the SR in 70% of the cases.17 A study showed that wavefront aberrometry-based autorefractor agreed within 0.5 D of SR values in 84% for SE.10 The agreement of SE between the Eyerobo VS and SR was 79.4% in this study. The results supported that the Eyerobo VS portable autorefractor can be used as the basis of the SR. So the Eyerobo VS can be applied to large-scale vision screening, especially in the optometrist’s inadequate health services and remote areas. The Eyerobo VS could be a valuable complement to the clinic for screening refractive error, as non-specialists can also use the Eyerobo VS with short-term training.
Some limitations in this study need to be taken into account. A limitation of this study is that no comparison of optometric measurements was made between professionals and non-professionals. Future studies comparing professionals and laypersons are therefore needed to demonstrate their use in large-scale vision screening for nonprofessionals. Another drawback is that there were few participants in the hyperopes study, making it challenging to reach firm findings. Finally, this study did not provide a cost-effectiveness analysis, which would be necessary if this device were to become available for large-scale vision screening.
Conclusion
In this study, the refractive measurement cycloplegic refraction of the Eyerobo VS showed high reliability and good agreement with the ARK-1 and SR on Sphere, SE, J0, and J45. The Eyerobo VS portable autorefractor could facilitate large-scale vision screening in schools and remote areas. As a complementary tool, the Eyerobo VS measurements can serve as a foundation for SR and reduce the global burden of visual impairment in children due to undetected and uncorrected refractive error.
Data Sharing Statement
Anonymized datasets generated and analyzed during the current study will be made available on reasonable request by the corresponding author (Guanghao Qin, [email protected]).
Ethics Approval and Informed Consent
This cross-sectional study was approved by the Ethics Committee of He Eye Specialist Hospital (IRB (2023) K026.01). It was registered at ClinicalTrails.gov (NCT06346626) on March 26, 2024. All procedures were reviewed and approved by the local institutional ethical review board in accordance with the Declaration of Helsinki principles. Written informed consent was obtained from the participants and parents.
Acknowledgments
We thank the participants in this study. The authors have no proprietary interest in any of the products mentioned in this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Foundation of Liaoning Educational Committee (Grant No. LJKZ1387).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO launches first world report on vision. 2019. Available from: https://www.who.int/news-room/detail/08-10-2019-who-launches-first-world-report-on-vision.
2. Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–9. doi:10.1136/BJOPHTHALMOL-2011-300539
3. Bourne RRA, Stevens GA, White RA, et al. Causes of vision loss worldwide, 1990-2010: a systematic analysis. Lancet Glob Health. 2013;1(6). doi:10.1016/S2214-109X(13)70113-X
4. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
5. Naidoo KS, Fricke TR, Frick KD, et al. Potential lost productivity resulting from the global burden of myopia: systematic review, meta-analysis, and modeling. Ophthalmology. 2019;126(3):338–346. doi:10.1016/j.ophtha.2018.10.029
6. World Health Organization. Eye care, vision impairment and blindness: refractive errors. 2024. Available from: https://www.who.int/news-room/questions-and-answers/item/blindness-and-vision-impairment-refractive-errors.
7. Burton MJ, Ramke J, Marques AP, et al. The lancet global health commission on global eye health: vision beyond 2020. Lancet Glob Health. 2021;9(4):e489–e551. doi:10.1016/S2214-109X(20)30488-5
8. Ambrosino C, Dai X, Antonio Aguirre B, Collins ME. Pediatric and school-age vision screening in the United States: rationale, components, and future directions. Children. 2023;10(3). doi:10.3390/CHILDREN10030490
9. Carpena-Torres C, Batres L, Serramito M, Carracedo G. Repeatability of subjective refraction in different age groups. Photonics. 2024;11(7):634. doi:10.3390/PHOTONICS11070634
10. Rao DP, Negiloni K, Gurunathan S, et al. Validation of a simple-to-use, affordable, portable, wavefront aberrometry-based auto refractometer in the adult population: a prospective study. BMC Ophthalmol. 2022;22(1). doi:10.1186/S12886-022-02684-5
11. Otero C, Aldaba M, Pujol J. Clinical evaluation of an automated subjective refraction method implemented in a computer-controlled motorized phoropter. J Optom. 2018;12(2):74. doi:10.1016/J.OPTOM.2018.09.001
12. Paudel N, Adhikari S, Thakur A, Shrestha B, Loughman J. Clinical accuracy of the nidek ARK-1 autorefractor. Optom Vis Sci. 2019;96(6):407–413. doi:10.1097/OPX.0000000000001386
13. Jin C, Wang S, Ye H, Wei R, Dong Y, Zhao P. Effects and related factors of short-time accommodation training on measuring consistency of InnovEyes sitemap, autorefraction, and subjective refraction. J Refract Surg. 2024;40(12):e941–e955. doi:10.3928/1081597X-20241022-01
14. Wesemann W, Dick B. Accuracy and accommodation capability of a handheld autorefractor. J Cataract Refract Surg. 2000;26(1):62–70. doi:10.1016/S0886-3350(99)00325-9
15. Liu Z, Pazo EE, Ye H, Yu C, Xu L, He W. Comparing school-aged refraction measurements using the 2WIN-S portable refractor in relation to cycloplegic retinoscopy: a cross-sectional study. J Ophthalmol. 2021;2021:1–8. doi:10.1155/2021/6612476
16. Zhou Y, He X, Liu Z, et al. Agreement and repeatability of scotopic pupil size measurement with the 2WIN-S portable refractor in Chinese adults. Sci Rep. 2024;14(1). doi:10.1038/S41598-024-66540-W
17. Gil A, Hernández CS, Pérez-Merino P, et al. Assessment of the QuickSee wavefront autorefractor for characterizing refractive errors in school-age children. PLoS One. 2020;15(10):e0240933. doi:10.1371/JOURNAL.PONE.0240933
18. Wilson LB, Melia M, Kraker RT, et al. Accuracy of autorefraction in children: a report by the American academy of ophthalmology. Ophthalmology. 2020;127(9):1259–1267. doi:10.1016/j.ophtha.2020.03.004
19. Paff T, Oudesluys-Murphy AM, Wolterbeek R, et al. Screening for refractive errors in children: the plusoptiX S08 and the Retinomax K-plus2 performed by a lay screener compared to cycloplegic retinoscopy. J AAPOS. 2010;14(6):478–483. doi:10.1016/j.jaapos.2010.09.015
20. Morgan IG, Iribarren R, Fotouhi A, Grzybowski A. Cycloplegic refraction is the gold standard for epidemiological studies. Acta Ophthalmol. 2015;93(6):581–585. doi:10.1111/AOS.12642
21. Magome K, Morishige N, Ueno A, Matsui TA, Uchio E. Prediction of cycloplegic refraction for noninvasive screening of children for refractive error. PLoS One. 2021;16(3):e0248494. doi:10.1371/JOURNAL.PONE.0248494
22. Thibos LN, Wheeler W, Horner D. Power vectors: an application of Fourier analysis to the description and statistical analysis of refractive error. Optom Vis Sci. 1997;74(6):367–375. doi:10.1097/00006324-199706000-00019
23. Ying GS, Maguire MG, Glynn R, Rosner B. Tutorial on biostatistics: linear regression analysis of continuous correlated eye data. Ophthalmic Epidemiol. 2017;24(2):130. doi:10.1080/09286586.2016.1259636
24. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
25. van der Zee C, Muijzer MB, Claessens JLJ, Wisse RPL. Determining the variability associated with visual acuity and refractive error measurements: a systematic review. Ophthalmology. 2025;132(9):1020–1032. doi:10.1016/J.OPHTHA.2025.04.021
26. Prajapati B, Dunne M, Armstrong R. Sample size estimation and statistical power analyses.
27. Mcginnigle S, Naroo SA, Eperjesi F. Evaluation of the auto-refraction function of the Nidek OPD-Scan III. Clin Exp Optom. 2014;97(2):160–163. doi:10.1111/CXO.12109
28. McAlinden C, Khadka J, Pesudovs K. Statistical methods for conducting agreement (comparison of clinical tests) and precision (repeatability or reproducibility) studies in optometry and ophthalmology. Ophthalmic Physiol Opt. 2011;31(4):330–338. doi:10.1111/J.1475-1313.2011.00851.X
29. Calvo-Maroto AM, Llorente-González S, Bezunartea-Bezunartea J, et al. Comparative study of refraction between wave front-based refraction and autorefraction without and with cycloplegia in children and adolescents. Children. 2022;9(1). doi:10.3390/CHILDREN9010088
30. Hashemi H, Khabazkhoob M, Asharlous A, Yekta A, Emamian MH, Fotouhi A. Overestimation of hyperopia with autorefraction compared with retinoscopy under cycloplegia in school-age children. Br J Ophthalmol. 2018;102(12):1717–1722. doi:10.1136/BJOPHTHALMOL-2017-311594
31. Guha S, Shah S, Shah K, Hurakadli P, Majee D, Gandhi S. A comparison of cycloplegic autorefraction and retinoscopy in Indian children. Clin Exp Optom. 2017;100(1):73–78. doi:10.1111/CXO.12375
32. Kulp MT, Ying GS, Huang J, et al. Accuracy of noncycloplegic retinoscopy, retinomax autorefractor, and SureSight vision screener for detecting significant refractive errors. Invest Ophthalmol Vis Sci. 2014;55(3):1378–1385. doi:10.1167/IOVS.13-13433
33. Kanclerz P, Przewłócka K, Arnold RW. Agreement in non-cycloplegic and cycloplegic refraction between a photoscreener and a calibrated autorefractor. BMC Ophthalmol. 2024;24(1):130. doi:10.1186/S12886-024-03375-Z
34. Krishnacharya PS. Study on accommodation by autorefraction and dynamic refraction in children. J Optom. 2014;7(4):193–202. doi:10.1016/J.OPTOM.2014.07.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.