Back to Journals » Clinical Ophthalmology » Volume 19
Tissue Damage on Ocular Surface After Combined Phacoemulsification with Limbal Relaxing Incision Compared with Standard Phacoemulsification
Authors Wang H ![]() , Yu X, Li Y, Sun L, Liu M, Zhang X, Yang R
, Yu X, Li Y, Sun L, Liu M, Zhang X, Yang R
Received 6 June 2025
Accepted for publication 28 July 2025
Published 13 August 2025 Volume 2025:19 Pages 2743—2750
DOI https://doi.org/10.2147/OPTH.S534006
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Haiyan Wang,1,2 Xinlu Yu,3 Yanan Li,2 Lingjuan Sun,2 Mingqi Liu,2 Xiongwei Zhang,4 Ruibo Yang1
1Tianjin Key Laboratory of Retinal Functions and Diseases, Tianjin Branch of National Clinical Research Center for Ocular Disease, Eye Institute and School of Optometry, Tianjin Medical University Eye Hospital, Tianjin, Tianjin, 300384, People’s Republic of China; 2Department of Ophthalmology, Shijiazhuang People’s Hospital, Shijiazhuang, Hebei, 050000, People’s Republic of China; 3Department of Ophthalmology, Maternal and Child Health Hospital of Qinhuangdao City, Qinhuangdao, Hebei, 066000, People’s Republic of China; 4Department of Nuclear Medicine, Shijiazhuang People’s Hospital, Shijiazhuang, Hebei, 050000, People’s Republic of China
Correspondence: Ruibo Yang, Tianjin Key Laboratory of Retinal Functions and Diseases, Eye Institute and School of Optometry, Tianjin Medical University Eye Hospital, Tianjin, Tianjin, 300384, People’s Republic of China, Email [email protected] Xiongwei Zhang, Department of Nuclear Medicine, Shijiazhuang People’s Hospital, Shijiazhuang, Hebei, 050000, People’s Republic of China, Email [email protected]
Purpose: To investigate the effect of phacoemulsification combined with LRIs on the ocular surface at different postoperative time.
Design: This study was designed as a retrospective analysis. Medical records of patients who had undergone relevant surgeries in the past were reviewed. Patients were divided into two groups based on the surgical procedures they had received: one group was those who had undergone phacoemulsification combined with LRIs (experimental group), and the other was those who had only received phacoemulsification (control group).
Methods: We retrospectively selected 80 patients (80 eyes) who had received cataract treatment. Among them, 41 eyes belonged to the experimental group and 39 eyes to the control group, which were grouped according to the degree of astigmatism as recorded in the medical files. The Tear Film Objective Scatter Index (TF-OSI), tear film break-up time (BUT), Schirmer I test, and Ocular Surface Disease Index (OSDI) scores were utilized to retrospectively evaluate the ocular surface conditions of these patients.
Results: A total of 80 patients (80 eyes) were selected for phacoemulsification treatment with cataract, TF-OSI value of the experimental group was higher than that of the control group at 1 day, 1 week, 6 weeks after surgery (P < 0.05). BUT value was lower than that of the control group at 1 day, 1 week, 6 weeks after surgery (P < 0.05). Schirmer I test value was lower than that of the control group at 1 week and 6 weeks after surgery (P < 0.05). OSDI scores were higher than that of the control group 1 week, 6 weeks and 3 months after surgery (P < 0.05).
Conclusion: Phacoemulsification with LRIs may cause more tissue damage on the ocular surface compared to standard phacoemulsification alone.
Keywords: phacoemulsification, limbal relaxing incisions, corneal astigmatism, ocular surface, tear film objective scatter index
Background
With the advent of the aging population, the number of cataract patients is increasing, cataract is the leading cause of blindness worldwide. With the improvement of surgical equipment and technology, phacoemulsification is currently the preferred treatment for cataract, and cataract surgery has transitioned from simple vision restoration surgery to refractive cataract surgery. Precise refractive cataract surgery requires a refractive power of less than ±0.5D, because more and more patients want to be free from glasses after surgery.
According to the survey,1 approximately 40% of cataract patients have corneal astigmatism ≥ 1.0D, and 20% of patients ≥ 1.5D. In general,2,3 the corneal astigmatism of cataract patients ≥ 0.75D can reduce patient’s visual acuity and contrast sensitivity, affecting daily life and work, which should be actively corrected, and the most commonly used correction methods are implantation of astigmatic intraocular lenses (Toric IOL) and limbal relaxing incisions (LRIs). A large number of reports say that patients with cataract and low-to-moderate astigmatism have comparable corrected effect when use implantation of Toric IOL or LRIs. Rotation of the axis after the implantation of Toric IOL can cause unsatisfactory correction results and optical interference, even require a second surgery to adjust the position of the lens. There are also some patients who are not suitable for Toric IOL implantation, such as: patients with high myopia, large pouches, so Toric IOL rotation is very likely to occur after surgery, instead LRIs have the character of safety, stability and accuracy, it is an ideal correction method for corneal astigmatism.
Phacoemulsification of cataract can cause the damage to the ocular surface, which can cause postoperative dry eye syndrome, but it will gradually improve after surgery.4 Cataract phacoemulsification combined LRIs usually has a unilateral or bilateral release incision on the limbus, the degree of damage to the ocular surface after surgery is theoretically heavier than that of phacoemulsification only, therefore, this study observed the preoperative and postoperative ocular surface conditions of patients undergoing phacoemulsification combined LRIs, in order to further understand the effect on the ocular surface of patients undergoing two different surgical method, better direct patient surgical planning.
Methods
Study Design
This data processing approach fully adheres to the guidelines of the Declaration of Helsinki, since this was a retrospective study using existing medical records, the need for a new ethical approval was waived according to the hospital’s policy and relevant ethical guidelines, and has obtained formal approval for such waiver from the Committee. Although individual patient informed consent was not separately obtained during the subsequent clinical case collection, all identifiable patient information (such as names, medical record numbers, and other personal details) will be strictly de-identified and removed from the dataset to fully protect patient privacy, ensuring that the research is conducted scientifically and in compliance with ethical standards.
Data and Methods
Data
A retrospective review was conducted on the medical records of 80 patients, aged between 50 and 80 years, who had undergone phacoemulsification treatment for cataract in our hospital from December 2022 to August 2023. Among them, 35 were male and 45 were female, with an average age of (68.88 ± 7.99) years. These patients were retrospectively grouped as follows: the experimental group consisted of 41 eyes with regular corneal astigmatism (0.75–2.00D) that had received phacoemulsification and LRIs; the control group comprised 39 eyes with corneal astigmatism (≤0.75D) that had undergone phacoemulsification only. Statistical analysis confirmed that there was no significant difference in age and gender between the two groups (P > 0.05). All patients had been implanted with monofocal aspheric intraocular lenses.
Research Method
TF-OSI
Using optical quality analysis system (OQAS, Visiometrics S.L, Spain) to exam this parameter,5–7 the patient adjust pupils to the natural maximum state in the dark for 5 minutes, require the patient to blink twice and then keep the eyes open for 20 seconds, this test records a two-channel image every 0.5 second until the 20 second, then obtain the mean value of the objective scattering index (Mean OSI) through the image, we calculated the tear film dynamic scattering index (TF-OSI), TF-OSI = MeanOSI-OSI.
Tear Film Break-Up Time (BUT): (Dry Eye Analyzer DED-1L, Kanghua, China)
The patient blinks naturally, and then keep the eyes open at least 20 seconds, and automatically record the time when the reflect ring break, which is a non-invasive tear film break-up time (BUT) test.
Schirmer I Test
Fold the tip of the test strip (Schirmer I Test Strips, Tianjin Jingming, China) and place it at the junction of the middle and outer 1/3 of the lower eyelid, ask the patient to close his eyes lightly, take it off after 5 minutes, and record the results.
International Standard Ocular Surface Disease Index (OSDI) Questionnaire
Before the examination, the patient fills in the OSDI questionnaire8,9 and evaluates the ocular surface condition according to 12 questions. Judging criteria: 0–12 points are normal, 13–100 points have different degrees of dry eye symptoms, the higher the score, the worse the ocular surface condition.
Operation
Experimental group: relaxing incisions design through calculation procedure by online corneal relaxing incisions (www.lricalculator.com), We need to provide the patient’s relevant data as follows, and I will calculate the design results of the corneal relaxing incision based on the information you provide (including the incision axis, arc length, and depth, following the principles of bilateral incisions, each side’s incision length not exceeding 1 quadrant, and the depth being approximately 90% of the peripheral corneal thickness), the main incision position of the cataract was 120°, and the induced astigmatism was 0.3D, the limbal relaxing incisions performed first, followed by phacoemulsification of cataract, the control group underwent phacoemulsification extraction combined with intraocular lens implantation.
Postoperative Medication
Prednisolone Acetate eye drops 4 times/day, Levofloxacin eye drops 4 times/day, diclofenac sodium eye drops 4 times/day after surgery, and last for two weeks.
Follow-Up
Collected TF-OSI, BUT, Schirmer I test and OSDI questionnaires of the time of preoperative data, 1 day, 1 week, 6 weeks, and 3 months after surgery.
Statistical Analysis
The data was analyzed by SPSS25.0 statistical software. The data was correspond to normal distribution was tested by Shapiro–Wilk test (X ± S). Sex comparison between the two groups used the χ²-test, age comparison used two independent samples t-tests, repeated measures variance (ANOVA) was used for comparisons at different time points, multiple comparisons used the Bonferroni test, a and p value less than 0.05 was considered statistically significant.
Results
Baseline Data
The preoperative baseline data of the two groups were compared. There were no statistically significant in preoperative age and gender in the two groups (P > 0.05) (Table 1).
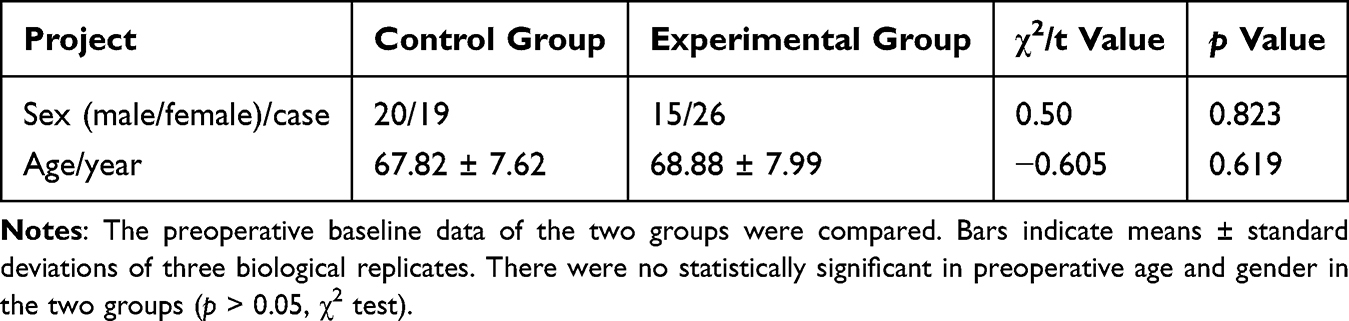 |
Table 1 Comparison of Preoperative Baseline Data Between the Two Groups |
TF-OSI
The TF-OSI value of the experimental group was higher than that of the control group at 1 day, 1 week, 6 weeks after surgery (P < 0.05). TF-OSI value of the two group was higher than before the surgery at 1 day, 1 week, 6 weeks after surgery (P < 0.05), both groups showed a decrease in tear film stability at 1 day, 1 week, and 6 weeks after the surgery (Figure 1).
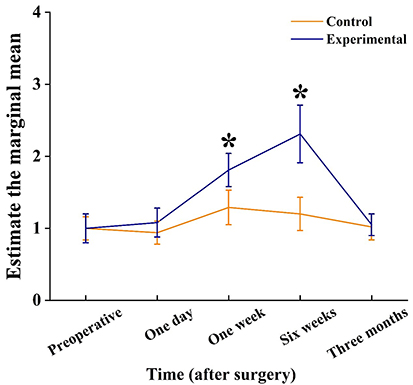 |
Figure 1 Comparison of TF-OSI between control and experimental at different time. The data collection times are preoperative, one day after surgery, one week after surgery, six weeks after surgery and three months after surgery respectively. Bars indicate means ± standard deviations of three biological replicates. Asterisks indicate that the mean values of three replicates are significantly different between control and experimental groups (P < 0.05). |
BUT Value
The BUT value of the experimental group was lower than that of the control group at 1 day, 1 week, 6 weeks after surgery (P < 0.05). BUT value of the experimental group was lower than before the surgery at 1 day, 1 week, 6 weeks after surgery (P < 0.05). BUT value of the control group was lower than before the surgery at 1 week and 6 weeks after surgery (P < 0.05), BUT value was shortened compared with that before the surgery 1 week, and 6 weeks after the surgery, the BUT value of the experimental group is somewhat worse (Figure 2).
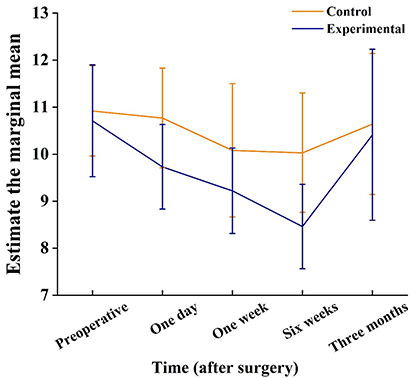 |
Figure 2 Comparison of BUT value between control and experimental at different time. The data collection times are preoperative, one day after surgery, one week after surgery, six weeks after surgery and three months after surgery respectively. Bars indicate means ± standard deviations of three biological replicates. |
The Schirmer I Test Value
The Schirmer I test value of the experimental group was lower than that of the control group at 1 week and 6 weeks after the surgery (P < 0.05), Schirmer I test value of the experimental group was lower than before the surgery at 1 day, 1 week, 6 weeks after surgery (P < 0.05). The Schirmer I test value of the experimental group was significantly shortened after the surgery (Figure 3).
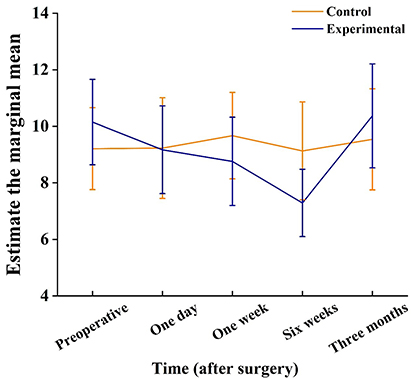 |
Figure 3 Comparison of Schirmer I test between control and experimental at different time. The data collection times are preoperative, one day after surgery, one week after surgery, six weeks after surgery and three months after surgery respectively. Bars indicate means ± standard deviations of three biological replicates. |
OSDI Scores
The OSDI scores of the experimental group were higher than that of the control group 1 week, 6 weeks and 3 months after the surgery (P < 0.05), OSDI scores of the experimental group were higher than before the surgery at 1 week, 6 weeks and 3 months after the surgery (P < 0.05). The OSDI scores of the experimental group were all higher after the surgery, and the dry eye symptoms were relatively obvious (Figure 4).
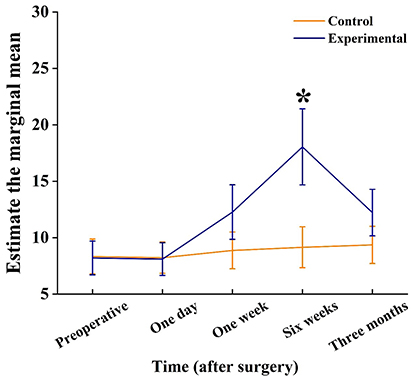 |
Figure 4 Comparison of OSDI scores between control and experimental at different time. The data collection times are preoperative, one day after surgery, one week after surgery, six weeks after surgery and three months after surgery respectively. Bars indicate means ± standard deviations of three biological replicates. Asterisks indicate that the mean values of three replicates are significantly different between control and experimental groups (P < 0.05). |
Discussion
In recent years, with the development of the economic and social society, cataract surgery has already transformed from a vision-restoring surgery to a refractive surgery, so the requirements for the surgery are getting higher and higher. Cataract phacoemulsification combined with LRIs can not only solve the blurred vision caused by cataract but also solve the refractive problem brought by astigmatism, and its safety and effectiveness have been verified, however, there are relatively few studies on the impact of this surgical method on the ocular surface.
In this research, through examination to obtain the TF-OSI value and BUT value, we found that the outcome of the control group are better comparing with the experimental group at 1 day, 1 week and 6 weeks after surgery. In the intragroup comparison, the TF-OSI value and BUT value of both groups became worse at 1 day, 1 week, and 6 weeks after surgery than preoperative. It can be clearly seen that the stability of the tear film of the patients in the experimental group after surgery is poorer than that of in the control group. It has been reported that phacoemulsification can cause a decrease in the stability of the tear film. There are multiple mechanisms by which phacoemulsification reduces the stability of the tear film, including frequent eye drops, mechanical damage, nerve damage around the incision, exposure of the ocular surface to strong light, and repeated irrigation.4,10 The damage to the surrounding nerves to the ocular surface of the two surgical methods is different. An in vivo confocal microscopy study by Misra et al11 reported a decrease in corneal nerve length 1 month after cataract surgery, which was supported by the study by De Cilla et al12 who detected a decline in nerve length at 1 month and 3 months postoperatively and recovery at 8 months postoperatively. Nielsen, Esben et al13 find corneal nerve deterioration 12 months after un-eventful cataract surgery. Although our study failed to collect the changes in the surrounding nerves, the corneal relaxing incisions cause greater damage to the corneal nerve, so the degree of postoperative tear film stability damage of the patients in the experimental group is greater than that of the control group. TF-OSI has high sensitivity to reflect the real situation of the tear film. The experimental results show that the values of TF-OSI in the two groups at 1 week and 6 weeks after surgery have reached the critical value (≥1.2) for dry eye treatment intervention, which is consistent with the research results of many previous scholars.4,14,15
The core mechanism of dry eye disease is the loss of tear film homeostasis. The TF-OSI value and BUT value are direct observation indicators of tear film instability. The Schirmer test is currently a conventional method used in clinical exploration to evaluate the functional state of the lacrimal gland, and it can also indirectly reflect the stability of the tear film. In our study, Schirmer I test value of the experimental group was decreased at 1 day, 1 week, and 6 weeks after surgery compared with before surgery, and the differences were all statistically significant. However, there was no significant difference at each postoperative time point compared with before surgery in the control group. From the results of the Schirmer I test we obtained, it was found that the postoperative tear secretion ability of the patients in the experimental group was lower than that of the control group (there was a statistically significant difference between the two groups at 1 week and 6 weeks after surgery in the intergroup comparison). Less tear secretion leads to a decrease in tear film stability. It was found that the tear film stability of the patients in the experimental group was the worst at 1 week and 6 weeks after surgery. Lambiase et al16 found that the levels of neuropeptide Y and calcitonin gene-related peptide (CGRP) in the tears of patients with dry eye were significantly lower than in healthy individuals. The lower the Schirmer I test results, the lower the CGRP levels in the tears, the shorter the tear film break-up time, the lower the neuropeptide Y levels in the tears. The study17,18 indicated that approximately 50% of patients experience dry eye symptoms within one week after laser in situ keratomileusis (LASIK), and patients who had undergone the procedure for more than 12 months had lower CGRP levels in their tears compared to healthy individuals, with a positive correlation to dry eye symptoms. This is related to the severing of corneal nerve fibers during surgery, which affects the tear secretion reflex arc and disrupts the supply of neurotrophic factors by the nerve fibers. In our experimental group, the increased incisions significantly raised the probability of nerve transection, affecting the regulation of tear secretion.
The OSDI scale is an internationally recognized dry eye questionnaire. It is a self-administered questionnaire that assesses the severity of the self-ocular surface condition. It focuses on the analysis of quality of life, and a score > 12 is considered dry eye. Our research results show that at the time points of 1 week, 6 weeks, and 3 months after surgery, the postoperative scores of patients in the experimental group were all higher than those in the control group, and there was statistical significance. In the results of the OSDI scale, the scores of patients in the experimental group at 1 week and 6 weeks after surgery have reached the dry eye scoring standard, while the scores of patients in the control group at all postoperative time points have not reached the dry eye scoring standard. Some research reports that the OSDI scale is negatively correlated with the amount of tear secretion.8 In our study, the tear secretion in the experimental group decreased after surgery, therefore, the subjective symptoms of dry eye will be more pronounced.
In our study, the ocular surface of the two groups were affected after the surgery, similar to the research results of Ameen et al19 we still aware that dry eye symptoms and ocular surface dysfunction symptoms are very common in elderly.20 In our daily clinical work, we often ignore the attention to the ocular surface before surgery. Previous studies have reported that the subjective symptoms and ocular surface diseases of patients after phacoemulsification are aggravated.21–23 Experts believe that it is very important to optimize the ocular surface before cataract surgery. To sum up, in the preoperative planning of cataract phacoemulsification especially combined with LRIs, optimizing the ocular surface can be appropriately supplemented with artificial tears, during the operation, the movements should be gentle, the light irradiation of the microscope should be reduced, and the operation time should be shortened. After the operation, artificial tears can also be used to assist in the recovery of the tear film.
Of course, our study has certain limitations, such as a small sample size, a short follow-up time after surgery, and no observation and recording of the peripheral corneal nerves and meibomian gland morphology. Another limitation of our study is that the patients used preservative-containing eye drops for treatment after surgery, so the ocular surface may be affected by it, not just the surgery itself.
Conclusion
Phacoemulsification combined with LRIs may cause more tissue damage to ocular surface compared to standard phacoemulsification alone, so it is very important to optimize the ocular surface in the perioperative period.
Data Sharing Statement
The research data used to support the findings of this study are available from the corresponding author upon request.
Ethical Approval
The study protocol was reviewed and approved by the Ethics Committee of Shijiazhuang People’s Hospital. Throughout the study, the principles of the Helsinki Declaration were strictly adhered to and comprehensive measures were taken to protect patient privacy.
Acknowledgment
We sincerely thank the Funds for the Key Project Guidance Program of Medical Science in Hebei Province of China for their financial support. Additionally, we are grateful to the staff responsible for the ocular surface assessments, whose meticulous work and dedication made this study possible.
This research project was supported by the Funds for the Key Project Guidance Program of Medical Science in Hebei Province of China (20191477), National Natural Science Foundation of China (82471049) and Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-037A).
Author Contributions
All authors have made significant contributions to the reported work, whether in the formation of concepts, study design, implementation, data acquisition, analysis and interpretation, or in all of these areas; participated in the drafting, revision, or critical review of the article; given final approval of the version to be published; agreed on the journal to which the article has been submitted; and consented to be accountable for all aspects of the work.
Disclosure
All authors declare that there are no conflicts of interest.
References
1. Mohammadi M, Naderan M, Pahlevani R, Jahanrad A. Prevalence of corneal astigmatism before cataract surgery. Int Ophthalmol. 2016;36:807–817. doi:10.1007/s10792-016-0201-z
2. Schallhorn SC, Hettinger KA, Pelouskova M, et al. Effect of residual astigmatism on uncorrected visual acuity and patient satisfaction in pseudophakic patients. J Cataract Refract Surg. 2021;47:991–998. doi:10.1097/j.jcrs.0000000000000560
3. Wolffsohn JS, Bhogal G, Shah S. Effect of uncorrected astigmatism on vision. J Cataract Refract Surg. 2011;37:454–460. doi:10.1016/j.jcrs.2010.09.022
4. Oh T, Jung Y, Chang D, Kim J, Kim H. Changes in the tear film and ocular surface after cataract surgery. Jpn J Ophthalmol. 2012;56:113–118. doi:10.1007/s10384-012-0117-8
5. Herbaut A, Liang H, Rabut G, et al. Impact of dry eye disease on vision quality: an optical quality analysis system study. Transl Vis Sci Technol. 2018;7(4):5. doi:10.1167/tvst.7.4.5
6. Rush S, Pickett CJ, Rush RB. Patient-reported dry eye outcomes after myopic femtosecond-LASIK: a 6-month prospective analysis. Clin Ophthalmol. 2023;17:2141–2147. doi:10.2147/OPTH.S421369
7. Kang SF, Wang YX, Zhang QC, Wang ZL, Chen GL. Dry eye disease in systemic lupus erythematosus: a cross sectional study. Int J Ophthalmol. 2024;17(7):1255–1261. doi:10.18240/ijo.2024.07.09
8. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
9. Yu K, Bunya V, Maguire M, Asbell P, Ying GS; Dry Eye Assessment and Management Study Research Group. Systemic conditions associated with severity of dry eye signs and symptoms in the dry eye assessment and management study. Ophthalmology. 2021;128(10):1384–1392. doi:10.1016/j.ophtha.2021.03.030
10. Shimabukuro M, Maeda N, Koh S, Abe K, Kobayashi R, Nishida K. Effects of cataract surgery on symptoms and findings of dry eye in subjects with and without preexisting dry eye. Jpn J Ophthalmol. 2020;64:429–436. doi:10.1007/s10384-020-00744-1
11. Misra SL, Goh YW, Patel DV, Riley AF, McGhee CN. Corneal microstructural changes in nerve fiber, endothelial and epithelial density after cataract surgery in patients with diabetes mellitus. Cornea. 2015;34:177–181. doi:10.1097/ICO.0000000000000320
12. De Cillà S, Fogagnolo P, Sacchi M, et al. Corneal involvement in uneventful cataract surgery: an in vivo confocal microscopy study. Ophthalmologica. 2014;231:103–110. doi:10.1159/000355490
13. Nielsen E, Ivarsen A, Hjortdal J. Signs of long-term corneal nerve deterioration after uneventful cataract surgery. J Cataract Refract Surg. 2022;48:372–373. doi:10.1097/j.jcrs.0000000000000792
14. Jiang D, Xiao X, Fu T, Mashaghi A, Liu Q, Hong J. Transient tear film dysfunction after cataract surgery in diabetic patients. PLoS One. 2016;11:e0146752. doi:10.1371/journal.pone.0146752
15. Ishrat S, Nema N, Chandravanshi SCL. Incidence and pattern of dry eye after cataract surgery. Saudi J Ophthalmol. 2019;33:34–40. doi:10.1016/j.sjopt.2018.10.009
16. Lambiase A, Micera A, Sacchetti M, Cortes M, Mantelli F, Bonini S. Alterations of tear neuromediators in dry eye disease. Arch Ophthalmol. 2011;129:981–986. doi:10.1001/archophthalmol.2011.200
17. Savini G, Barboni P, Zanini M. The incidence and risk factors for developing dry eye after myopic LASIK. Am J Ophthalmol. 2006;142:355–356. doi:10.1016/j.ajo.2006.04.040
18. Chao C, Golebiowski B, Zhao X, Chen S, Zhou S, Stapleton F. Long-term effects of LASIK on corneal innervation and tear neuropeptides and the associations with dry eye. J Refract Surg. 2016;32:518–524. doi:10.3928/1081597X-20160603-01
19. El Ameen A, Majzoub S, Vandermeer G, Pisella PJ. [Influence of cataract surgery on Meibomian gland dysfunction (French translation of the article)]. J Fr Ophtalmol. 2018;41:526–535. doi:10.1016/j.jfo.2017.11.021
20. Kato K, Miyake K, Kondo N, et al. Conjunctival goblet cell density following cataract surgery with diclofenac versus diclofenac and rebamipide: a randomized trial. Am J Ophthalmol. 2017;181:26–36. doi:10.1016/j.ajo.2017.06.016
21. Khanal S, Tomlinson A, Esakowitz L, et al. Changes in corneal sensitivity and tear physiology after phacoemulsification. Ophthalmic Physiol Opt. 2008;28:127–134. doi:10.1111/j.1475-1313.2008.00539.x
22. Cho YK, Kim MS. Dry eye after cataract surgery and associated intraoperative risk factors. Korean J Ophthalmol. 2009;23:65–73. doi:10.3341/kjo.2009.23.2.65
23. Kohli P, Arya SK, Raj A, Handa U. Changes in ocular surface status after phacoemulsification in patients with senile cataract. Int Ophthalmol. 2019;39:1345–1353. doi:10.1007/s10792-018-0953-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.