Back to Journals » Clinical Ophthalmology » Volume 17
Timing of the Initial Postoperative Care After Cataract Surgery: A Patient’s Perspective
Authors Rush SW, Huseman S, Rush RB ![]()
Received 22 March 2023
Accepted for publication 22 May 2023
Published 25 May 2023 Volume 2023:17 Pages 1475—1479
DOI https://doi.org/10.2147/OPTH.S413602
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Sloan W Rush,1,2 Samuel Huseman,1,2 Ryan B Rush2,3
1Panhandle Eye Group, Amarillo, TX, USA; 2Department of Surgery, Texas Tech University Health Science Center, Amarillo, TX, USA; 3Southwest Retina Specialists, Amarillo, TX, USA
Correspondence: Ryan B Rush, Southwest Retina Specialists, 7411 Wallace Blvd, Amarillo, TX, 79106, USA, Tel +1 806 351-1870, Email [email protected]
Purpose: To evaluate patient preferences in regards to the timing of the initial postoperative examination after undergoing cataract surgery.
Methods: A retrospective, consecutive case series analysis from a single private practice institution was performed using a standardized phone survey on patients who underwent cataract surgery. Subjects were classified into one of two possible study groups according to the timing of their initial postoperative cataract surgery examination: Group A received the initial postoperative cataract surgery examination on the same day as the surgery, whereas Group B received the initial postoperative cataract surgery examination on the day following the operation.
Results: There were 80 subjects contacted for the phone survey of which 70 (35 in each study group) completed the survey and therefore were included in the analysis. Group A subjects responded favorably in regards to preference and realizing reduced time and cost savings compared to Group B (p < 0.0001 for both). There were no subjects in Group A who would have preferred next-day initial postoperative care, whereas 31.4% of subjects in Group B would have preferred same-day care if given the opportunity.
Conclusion: Patients undergoing cataract surgery both prefer and report time and cost savings with same-day initial postoperative care compared to next-day initial postoperative care. Patient preferences regarding their postoperative care should be one of the many factors that a surgeon ought to take into consideration when providing follow-up care after cataract surgery.
Keywords: postoperative cataract surgery care, patient desirability
Introduction
A complicated phacoemulsification cataract surgery may be defined as a surgery in which one or more adverse events occur during the operation,1 and the American Academy of Ophthalmology (AAO) preferred practice patterns advise that such patients should return for a postoperative examination the next day (postoperative day one) following the surgery for initial review.2 Next-day postoperative exams can detect wound leaks, IOP elevations, malpositioned intraocular lenses, and retained lens particles. However, time until first review following routine, uneventful cataract surgery varies according to surgeon preference, but has been reported to occur most frequently either on the same day as the operation or on the following day,3 although there have been some reports suggesting that initial postoperative care may be safely deferred out to 2 weeks.4,5 Nevertheless, the AAO preferred practice patterns recommend that patients who underwent an uncomplicated surgery with a low-risk for postoperative complications should be evaluated in the first 48 hours following surgery.2 Although this provides the physician with helpful guidance when scheduling initial postoperative care, little is known regarding patient preference in the matter. The authors believe that in order to provide a more holistic, patient-centered care, patient preference should be one of the many factors taken into consideration when caring for our patients. In this study, the authors compare same-day versus next-day initial postoperative review following uneventful cataract surgery from a patient’s perspective.
Methods
This retrospective case series was authorized by the Panhandle Eye Group Institutional Review Board (IORG0009239-2) and was conducted on consecutive subjects who underwent routine, uncomplicated cataract surgery at a single private practice institution in Amarillo, TX from January to December 2022. The research was performed according to the principles of the Helsinki Declaration and was compliant with the Health Insurance Portability and Accountability Act of 1996. The need for informed consent was waived because subject data was gathered retrospectively and all identifying subject information was omitted.
All patients included in the study had an initial consultation visit followed by a second biometry visit. Then each patient received separate-day bilateral cataract surgery (within 7 days among the eyes). Subjects were classified into 1 of 2 possible study groups according to the timing of their initial postoperative cataract surgery examination: Group A received the initial postoperative cataract surgery examination on the same day as the operation (+/- 2 to 6 hours postoperatively), whereas Group B received the initial postoperative cataract surgery examination on the day following the operation (+/- 18 to 24 hours postoperatively). All patients received a final visit 3 weeks (+/-1 week) postoperatively from the time of the second eye surgery. Per routine of the clinic, the initial postoperative examination included slit-lamp exam without intraocular pressure measurement unless microcystic edema was detected. Subjects for the study were identified through the practice’s electronic medical record system by billing codes submitted during the time period referenced above. Patients with significant ocular comorbidities that were deemed by clinician to adversely impact the intraoperative/postoperative outcomes were excluded. The postoperative survey was administered by the same examiner (SH) by phone 12 weeks (+/-1 week) after cataract surgery on the second eye. The standardized questions asked to each study subject are displayed in Box 1. Questionnaire responses and all other gathered data were put into a password-protected MS Excel spreadsheet. Google Maps calculated distances from subject addresses to the practice’s surgery center. Relevant baseline and postoperative data were collected from each subject’s electronic medical record. The JMP 7 software (SAS Institute; Cary, NC, USA) was employed to analyze the data. One-way analysis of the variance compared numerical outcomes, and likelihood ratios compared categorical outcomes. Statistical significance was considered at an alpha level of 0.05. Subjects with missing data were expelled from analysis.
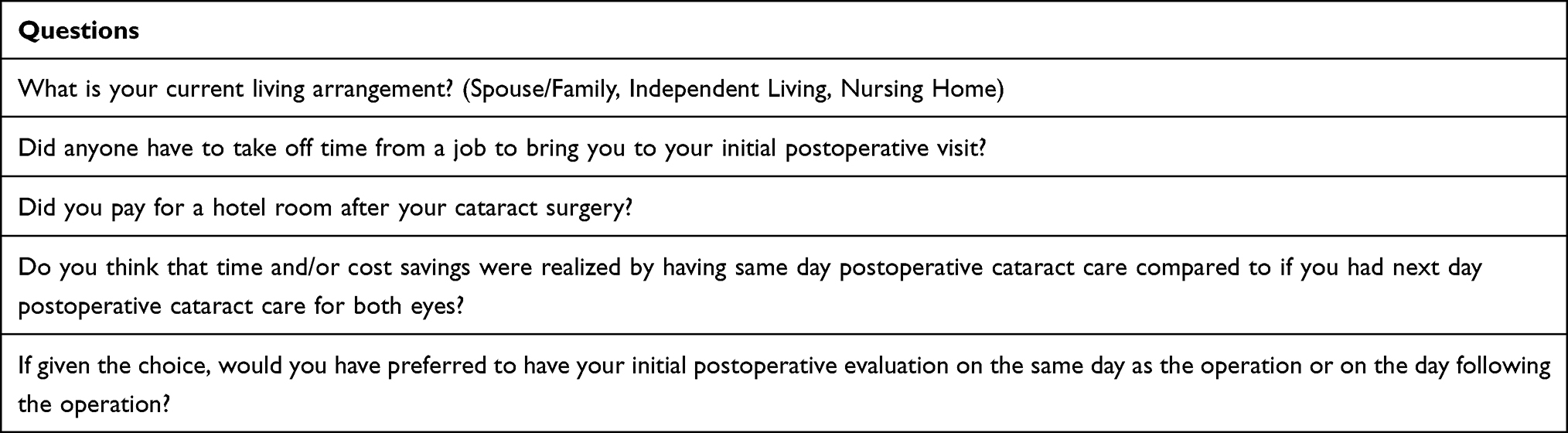 |
Box 1 Same-Day versus Next-Day Postoperative Care. Standardized Phone Survey Questions |
Results
There were 80 consecutive patients who underwent routine, uncomplicated cataract surgery selected for the study. Seventy (35 in each study group) completed the phone survey (87.5% participation rate) and therefore were included in study’s analysis. There were no intraoperative or postoperative surgical complications identified in the medical records review for any of the subjects in either study group prior to the administration of the phone survey.
Table 1 displays the characteristics of the overall study population gathered from the medical records review that potentially could have affected the responses to the survey questions. The average study population age was 69.9 years with 52.9% of the participants being female. There were 35.7% of the respondents that resided >50 miles from the medical facilities, and all patients together traveled an average of 452.4 miles total for bilateral cataract care. There were no statistically significant differences in any of the variables evaluated except for a reduced number of total appointments in favor of Group A (same-day initial postoperative examination). Table 2 displays each study group’s responses to the survey questions. Of note, subjects in Group A (same-day initial postoperative examination) responded favorably in regards to preference and realizing reduced time and cost savings compared to Group B (next-day initial postoperative examination).
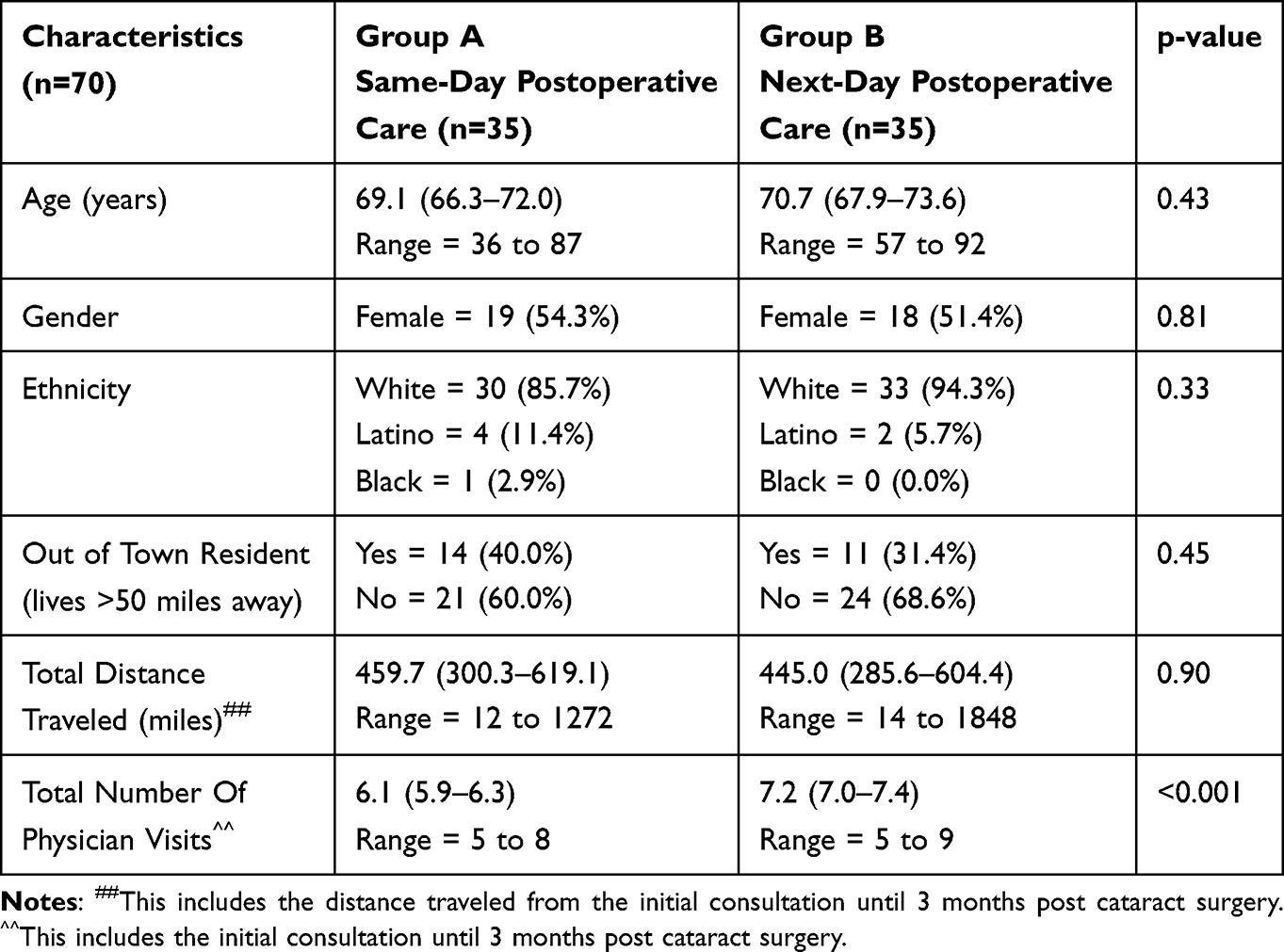 |
Table 1 Same-Day versus Next-Day Postoperative Care. Study Population Characteristics. Means with (95% Confidence Intervals) |
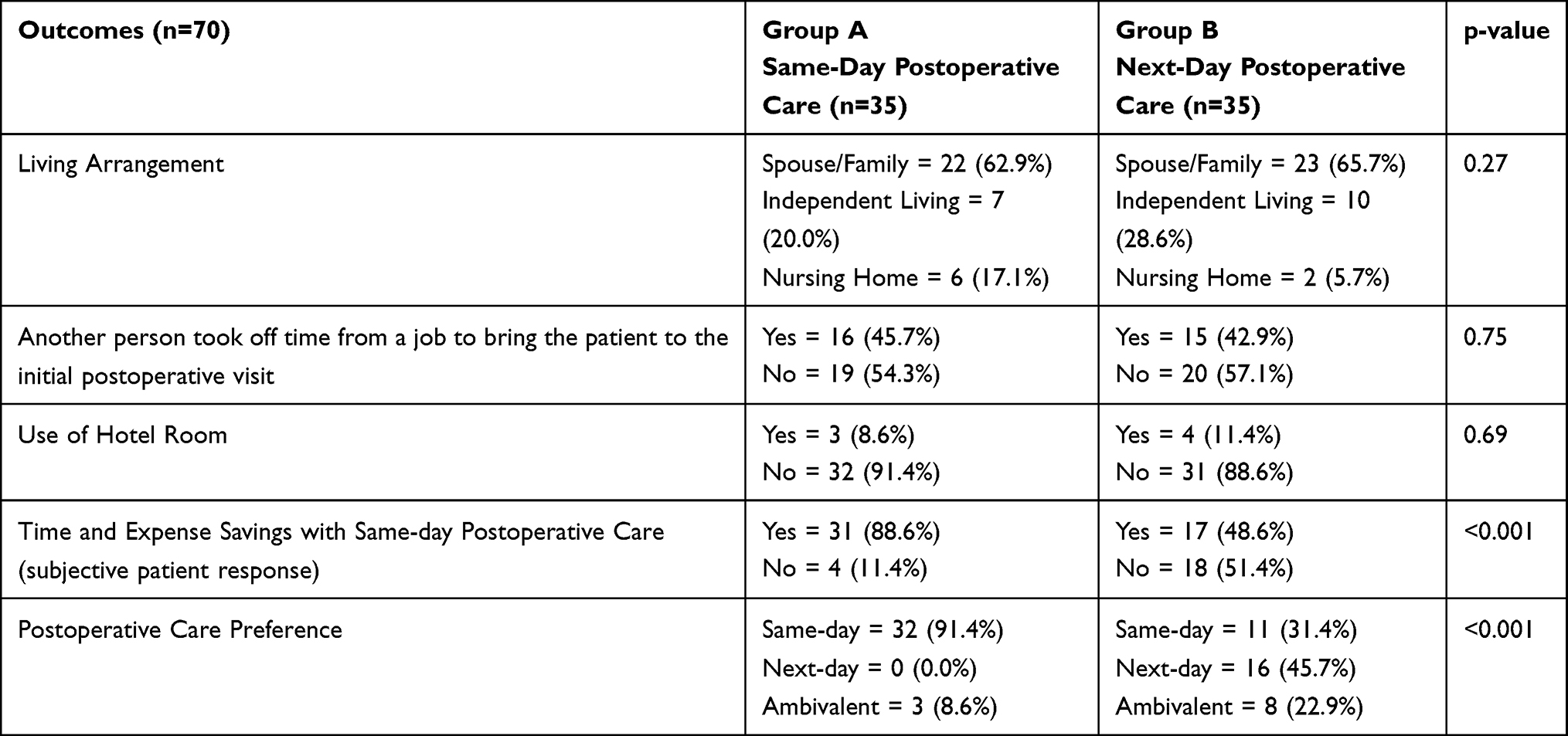 |
Table 2 Same-Day versus Next-Day Postoperative Care. Survey Outcome Measurements |
Discussion
Over the past 20 years, the medical sciences including ophthalmology have taken an increased interest in patient-reported outcomes, and the authors concur that patient-reported outcomes do indeed provide the physician with more ammunition for offering a more holistic approach to the overall care of our patients.6,7 From the perspective of the physician, the postoperative cataract surgery patient must be evaluated initially at some point and whether it is the same-day or on a different day, the authors do not recognize any time or cost savings realized to the physician. And since the AAO preferred practice patterns provide some flexibility in regards to initial postoperative care, the authors believe it is reasonable and appropriate to take into consideration their patient’s preferences on the matter.
The benefits, risks and preferences of cataract surgeons have been published, discussed, and debated during the past 3 decades.1,3–5 As cataract surgery numbers continue to grow throughout the developed world,8 it becomes more and more important for the cataract surgeon to take into consideration the patient’s preferences regarding their postoperative care as well as the overall safety of any such practices. As reported in this study, there were not any identifiable postoperative complications in the medical record review for either the same-day or next-day initial postoperative care groups. However, this study was not powered to detect a difference between study groups in regards to the most serious postoperative complications that might occur (ie endophthalmitis, hypotony, wound leaks, etc.). Moreover, devastating complications such as endophthalmitis rarely show up sooner than 48 hours after cataract surgery and therefore would not be detected by either same-day or next-day initial postoperative care.9 A study would need thousands of cases undergoing same-day versus next-day initial postoperative care to determine safety in subjects receiving cataract surgery, and to the knowledge of the authors, no such sufficiently powered analysis has occurred. A recent retrospective study compared same-day to next-day initial postoperative care but it was woefully underpowered for detecting such postoperative complications known to occur at an incidence of <2%.10 However, our study was powered sufficiently to determine a difference in patient responses to the administered survey regarding the timing of their initial postoperative examinations.
Patient responses to the survey administered in this study shed light on patient preferences regarding their initial postoperative care following cataract surgery. From the medical record review prior to administration of the patient surveys, patients who received same-day initial care did have approximately one fewer appointment during the overall cataract event (from initial consultation until 3 months post-surgery) compared to the patients who received next-day initial care. This difference may contribute to explaining why patients receiving same-day initial care responded favorably in the survey in regards to preferring same-day initial care as well as responding favorably to the overall cataract experience in respect to time and cost savings compared to subjects who received next-day initial care. In fact, no subjects in the same-day initial care group if given the choice would have wanted next-day initial care, whereas over 30% of subjects in the next-day initial care group would have wanted same-day care if given the choice.
Strengths of this study include its balanced study groups and the high participation rate of its respondents. Limitations of this study include its retrospective design, lack of previous validation of the administered patient survey questionnaire, potential for patient bias due to the necessity of having to recall events from the past, the small N which does not allow for inclusion of a significant number of cases that could have intraoperative/postoperative complications (for example, endophthalmitis or IOP elevations), and its inclusion of patients from only one isolated geographic region in the United States. Since about 40% of our study’s overall population had to travel >50 miles to receive cataract surgery, it is unknown if a population residing in a larger metropolitan area in which the high majority of patients only needed to travel a few miles to receive care would respond the same way; this uncertainty may limit our study’s generalizability.
In conclusion, subjects from our geographic area undergoing cataract surgery both prefer and report time and cost savings with same-day initial postoperative care compared to next-day initial postoperative care. Patient’s preferences regarding their postoperative care should be one of the many factors that a cataract surgeon takes into consideration when scheduling postoperative care.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The study was approved by the Panhandle Eye Group Institutional Review Board (IORG0009239-2) in accordance with the Ethical Standards laid down in the Declaration of Helsinki.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Grzybowski A, Kanclerz P. Do we need day-1 postoperative follow-up after cataract surgery? Graefes Arch Clin Exp Ophthalmol. 2019;257:855–861. doi:10.1007/s00417-018-04210-0
2. Olson RJ, Braga-Mele R, Chen SH, et al. Cataract in the adult eye preferred practice pattern®. Ophthalmology. 2017;124:P1–P119. doi:10.1016/j.ophtha.2016.09.027
3. Herbert EN. Low need for intervention at the first day review after uncomplicated phacoemulsification. Eye. 2000;14(Pt 6):923. doi:10.1038/eye.2000.261
4. Saeed A, Guerin M, Khan I. Deferral of first review after uneventful phacoemulsification cataract surgery until 2 weeks: randomized controlled study. J Cataract Refract Surg. 2007;33(9):1591–1596. doi:10.1016/j.jcrs.2007.05.022
5. Kessel L, Andresen J, Erngaard D, et al. Safety of deferring review after uneventful cataract surgery until 2 weeks postoperatively. J Cataract Refract Surg. 2015;41(12):2755–2764. doi:10.1016/j.jcrs.2015.11.010
6. Finger RP, Scholl HPN, Holz FG. Patient reported outcomes. Relevance and application in ophthalmology. Ophthalmologe. 2008;105(8):722–726. doi:10.1007/s00347-008-1804-1
7. Scheibler F, Finger RP, Grosselfinger R, Dintsios CM. Patient-reported and patient-weighted outcomes in ophthalmology. Ophthalmologe. 2010;107(3):235–240. doi:10.1007/s00347-009-2037-7
8. Liu YC, Wilkins M, Kim T, Malyugin B, Mehta JS. Cataracts. Lancet. 2017;390(10094):600–612. doi:10.1016/S0140-6736(17)30544-5
9. Rahmani S, Eliott D. Postoperative endophthalmitis: a review of risk factors, prophylaxis, incidence, microbiology, treatment, and outcomes. Semin Ophthalmol. 2018;33(1):95–101. doi:10.1080/08820538.2017.1353826
10. Patel V, Freedman RL, Das S, et al. Post-operative day zero versus day one follow-up for uncomplicated cataract surgery. Cureus. 2022;14(9):e29286. doi:10.7759/cureus.29286
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.