Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Time to Switch to Second-Line Anti-Retroviral Treatment and Its Predictors Among HIV Infected Adults with Virological Failure in Northwest Ethiopia: A Retrospective Follow-Up Study
Authors Demeke Alemu K ![]() , Abebe Moges N
, Abebe Moges N ![]() , Jara Boneya D, Assemu Asrade A
, Jara Boneya D, Assemu Asrade A ![]() , Degu Tsega T
, Degu Tsega T ![]() , Shitaw Tewachew A
, Shitaw Tewachew A ![]()
Received 15 November 2021
Accepted for publication 28 January 2022
Published 5 March 2022 Volume 2022:14 Pages 87—100
DOI https://doi.org/10.2147/HIV.S348076
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Kasaye Demeke Alemu,1 Nurilign Abebe Moges,2 Dube Jara Boneya,2 Abaynew Assemu Asrade,1 Tilahun Degu Tsega,2 Abrham Shitaw Tewachew1,3
1Department of HIV/AIDS Prevention Care and Treatment, International Center for AIDS Care Program/ICAP, Bahir Dar, Ethiopia; 2Departments of Public Health College of Health Sciences, Debre Markos University, Debre Markos, Ethiopia; 3College of Medicine, Debre Berhan University, Debre Berhan, Ethiopia
Correspondence: Kasaye Demeke Alemu, Tel +251921668185, Email [email protected]
Background: HIV treatment failure is a devastating public health challenge worldwide. Low rates and delays in switching are associated with increased death and second-line failure. But the time to switch and predictors are not well studied in Ethiopia. Therefore, this study assessed the time to switch to second-line ART and its predictors among HIV-infected adults with virological failure in Northwest Ethiopia.
Methods: An institution-based retrospective follow-up study was conducted from Oct 1/2016 to Feb 28/2020 in Northwest Ethiopia. Secondary data were extracted through a predefined extraction tool from 427 HIV-infected adults, which were selected by systematic random sampling. Kaplan–Meier with log rank test was done to identify the survival time and compare survival time among different categorical independent variables. The Cox proportional hazard model was fitted and variables having a p-value of less than 0.05 with a 95% confidence level were identified as a predictor of time to switch to second-line ART and interpreted accordingly.
Results: A total of 288 (67.45%) HIV-infected adults were switched to second-line ART with a median time of 162 days (IQR: 35,682). The risk of switching is higher among HIV infected adults with viral RNA of 60,000 copies/mL or more at failure (AHR=1.80, 95% CI: 1.31– 2.48), ≥ 8 years duration on first-line ART (AHR: 2.31, 95% CI: 1.62, 3.29) and enhanced adherence counseling of 4 to 6 sessions (AHR: 1.28, 95% CI: 1.01, 1.63), and lower with 4 or more missed appointments (AHR: 0.49, 95% CI; 0.28, 0.84) and no history of 1st line regimen change (AHR: 0.53: 95% CI: 0.41,0.69).
Conclusion: The median time to switch to second-line ART following 1st line virological failure is about 162 days, higher than other related studies. But switching was higher in patients with high viral RNA copies, missed appointments, longer duration on first-line ART, and the number of enhanced adherence counseling. So, intervention strategies that aid patients to have timely switch without due delays as soon as virologic failure should be prioritized.
Keywords: virological failure, switch, second-line ART, Northwest Ethiopia, Ethiopia
Background
Despite antiretroviral treatment (ART) having significantly improved the survival of patients who suffer from HIV (Human Immune Deficiency Syndrome), still, people are dying prematurely while they are on treatment due to several factors. Among these factors, treatment failure is a giant challenge.1–3 The World Health Organization’s (WHO) definition of treatment failure for deciding to switch ART regimens can be virological, immunological or clinical.4 A virological failure (VF) is when two consecutive plasma viral load measurements of above 1000 copies/mL are done 3 to 6-months intervals, with enhanced adherence counseling (EAC) support between measurements after at least 6 months of starting a new ART regimen. The value of viral load (VL) testing as a more sensitive and earlier indicator of treatment failure is increasingly recognized. Thus, it is the gold standard for monitoring the response to anti-retro viral (ARV) drugs, so health care providers are using it as the final evidence for making a decision to switch ART regimen.4,5
Highly active anti-retro viral therapy (HAART) regimens commonly require changes to overcome treatment failure, which often involve switching multiple medications simultaneously. Switching from first-line to second-line ART should occur immediately after confirmed VF without any delay.4–8 But rates of switching to second-line ART are low and concerns have been raised that people on ART may be experiencing long periods taking the failed first-line regimen.9,10 While late switching, with complex resistance, appears to have minimal effect on early second-line outcomes, the role of virological monitoring in determining long-term outcomes is yet to be determined.9,11,12
HIV treatment failure has to become the overwhelming challenge that the world faced in the present day despite growing enormous investments against it.13 In Africa, 9% of adults taking ART were developing VF14 and, also in Ethiopia, the prevalence of first-line ART failure was 21%.15 With these and more prevalence, the time to switch varies across different studies. For example, in Uganda, 43% and 66.1% of adult patients with first-line ART treatment failure were switched to second-line ART regimens with the median time of 180 and 243 days respectively.16,17 In South Africa also 74.3% of patients were switched to second-line ART with a median time of 84 days after confirmed VF.18
Yet a growing number of patients are expected to experience treatment failure over time, with a subsequent escalating need for second-line regimens, longer time to switch leads to elevated hazards of death, the possibility of a poor response to the new therapy, and increases non-nucleotide reverse transcriptase inhibitor resistance mutations, which could also be detrimental to second-line regimen activity.17,19 Mortality in patients with first-line VF and not switched to second-line ART was 11.9%, compared to 1.2% for those who switched.17 The relative benefit of the earlier switch is based on the assumption of a linear relationship between the timing of switch and probability of death; the longer the time, the higher probability of death.20
Despite all global and local efforts, rates of switching to second-line ART are low and concerns have been raised that patients may be experiencing long periods with VF.9 Previous studies showed that age of the patient, disclosure HIV status, WHO clinical staging, baseline regimen, had caretaker, viral RNA copies at failure, missing visits on first-line ART, and longer duration on the first-line regimen were significant factors associated with switching to second-line ART after first-line regime failure.17–19,21–24
Although patients who switch to second-line treatment after failure have improved outcomes compared to patients who do not switch, a low proportion of patients were switched, and failing to second-line ART remains become high.25 To the best of researchers’ knowledge, there is limited study regarding time to switch to second-line ART among patients with first-line VF in Ethiopia where there is a significant number of patients encountered treatment failure with no scientific evidence whether switched or not and its predictors.15 Therefore, understanding the time between treatment failure and switching and its predictors is very crucial to combat treatment failure and improve clinical care outcomes of patients taking ART by preparing and implementing actual data-driven quality improvement projects. So, this study was intended to assess the time to switch to second-line ART and its predictors among HIV-infected adults with first-line VF in Northwest Ethiopia.
Methods
Study Setting
This study was conducted in Northwest Ethiopia including 12 high caseload ART public health facilities.26 An institution-based retrospective follow-up study was conducted from October 1/2016-September 30/2020 among HIV-infected adults who had confirmed VF from October 1/2016 to February 28/2020 to the first-line ART drugs. Then secondary data were extracted from October 10 to November 10/2020.
All HIV-infected adults with first-line VF at high load public health facilities in Northwest Ethiopia from October 1/2016 to February 28/2020 were the study population. Among these, those who had incomplete data of date of switch and VF were excluded from this study.
Sample Size and Sampling Procedures
Sample size was calculated by time to event data formula using Stata 14.1 by taking into account the duration on first-line ART (less than 1 year on ART before failure) as the major exposure variable, (in this regard, a 5% level of significance [two-sided], a power of 80% and a ratio of unexposed to exposed of 1:1, crude hazard ratio 1.46, and withdrawal of 10%18 were considered). Then, using the command of Stata 14.1, power log-rank 0.5, Schoenfeld wd prob (0.1), and the total sample size required for this study was calculated and gave 440. Among 870 HIV-infected adults with confirmed VF to the first line ART-taking individuals in 12 facilities, 440 were selected proportionally from each facility using a systematic random sampling technique in which different K was used for each facility. The high viral load management register was used as a source document at which all ART-taking individuals with the first high viral load were listed and followed through.
Study Variables
Dependent Variable
Time to switch to second-line ART since virological treatment failure to first-line ART.
Independent Variables
Socio-demographic factors (age at failure, sex, religion, marital status, educational status, occupation, residence, having telephone), baseline clinical, laboratory and ART information (baseline WHO stage, baseline ART regimen, baseline functional status, and baseline BMI), adherence barriers before failure (use a condom, take alcohol/Khat, disclosed HIV status and has caregiver) and ART follow up, laboratory and clinical information before failure (recent adherence level, Tuberculosis Preventive Therapy [TPT] provision status, Cotrimoxazole Prophylactic Therapy [CPT] provision status, latest BMI at failure, duration on first-line treatment, missed appointment, recent functional status, first-line regimen change, enrolled to appointment spacing model and numbers of EAC follow up time between first HVL and confirmatory viral load test) are potential predictors of time to switch to second-line ART.
Operational Definition
Switch: A discontinuation of a failed first-line ART regimen and the start of a protease inhibitor (PI) based second-line ART regimen.5
Event: A switch or shift to PI-based second-line ART regimen from a failing first-line ART regimen only due to VF evidenced by the record from the patient’s chart.
Censored: Includes lost to follow up, transferred out, and dead before switched to second-line ART within the follow-up period and,those patients who did not switch at the end of follow up.
Survival time: Time from confirmed VF to switch to second-line ART or censored measured in days till the end of follow-up.
Virological Failure: Two consecutive measurements of HIV viral RNA greater than 1000 copies/mL 3 to 6 months apart with optimum adherence support after the patient was provided with new first-line ART for at least 6 months.5 The date of failure was ascertained by the date at which the viral load test was done and received at the ART clinic evidenced by the record at the high viral load register.
High load Facility: ART providing facility having greater than 500 ART users.5
First high viral load: The initial viral load counts greater than 1000 copies/mL done 3 or more months immediately before 2nd high viral load.
Second high viral load: The confirmatory viral load greater than 1000 copies/mL was done after 3 to 6 completed enhanced adherence sessions.
First-line regimen change: a switch or substitution of at least one drug from the original HAART regimen.5
Data Collection Procedures and Tools
Data abstraction format was developed to capture secondary data from ART entry and follow-up sheet used in the ART clinics. This format was adapted from previous works of literature17,18,22,25,27 and modified from ART follow up templates, to collect socio-demographic, baseline clinical, laboratory, and ART information, Patient-related adherence barriers, and ART follow up, laboratory and clinical Information from high viral load management registry, patient chart, and facility electronic-based smart care. For this purpose, one-degree clinical nurse or health officer experienced in the area who had extracted the required data from chart and register and one card room worker who draw the chart were assigned for the entire data collection period to each facility. Besides, two BSc. holder public health officers who have been managing and facilitating the overall data collection were deployed. The overall course was taken a month cascaded by the principal investigator.
Data Quality Control
The training was given to data collectors and supervisors for a day on how to extract the data, the use of source documents, and the scope of the research. The abstraction tool was reviewed and commented on by senior experts in the area, and a pretest was done on 5% of the total sample size at Debre Markos health center from October 5–9/2020 to check for tool consistency and relevance. Strict follow-up and supervision were carried out during data collection. The principal investigator and supervisors have been conducting day-to-day follow-up during the whole period of data collection. Each abstraction form was reviewed and checked for completeness by the supervisor and the PI daily and the necessary corrective feedback was given to data collectors.
Statistical Data Management and Analysis
The data extracted from the chart were entered into Epi-data version 3.1 and checked for completeness, cleaned to check for frequencies, accuracy, consistencies, outliers, missed values, and variables. The data was exported to Stata 14.1 for analysis, and then categorized and sorted to facilitate its analysis.
Descriptive statistics were used to describe the characteristics of the cohort. Kaplan–Meier (KM) was used to estimate survival time in days, day intervals between dates at which Virological failure was confirmed and switched to second-line ART or censored. KM with Log rank test was done to compare the survival time among groups of different categorical independent variables and proportional hazard Cox regression was done to estimate hazard ratio. The presence of multicollinearity and interaction effect was checked for each variable. Schoenfeld residuals statistical test, presence of time-dependent covariate, and graphical methods were used to check the Cox Proportional Hazard (PH) assumption. Multivariable Cox regression was computed for all variables that have less than 0.2 with bi-variable analysis. The final model was built through a stepwise regression procedure after being checked and meeting the PH assumption. The fitness of the final model was also checked using the cox-Snell test graphically and the global test statistically.
Hazard ratios with 95% confidence intervals (CI), incidence rate, and median time to switch were estimated and interpreted accordingly. Statistical significance was declared for explanatory variables with a p-value of less than 0.05.
Results
Study Participants’ Characteristics
In this study, a total of 427 (97.04%) HIV-infected adults who had confirmed first-line VF were included with an overall response rate of 97%, and 13 were excluded due to chart loss.
Among all participants, 243 (56.9%) were females and 183 (42.8%) were married. The mean (±SD) age of people at treatment failure of first-line ART was 38.5 (± 9) years. A total of 278 (65.1%) and 337 (78.9%) were from urban and out of the catchment areas respectively as shown from socio-demographic characteristics of respondents in Table 1.
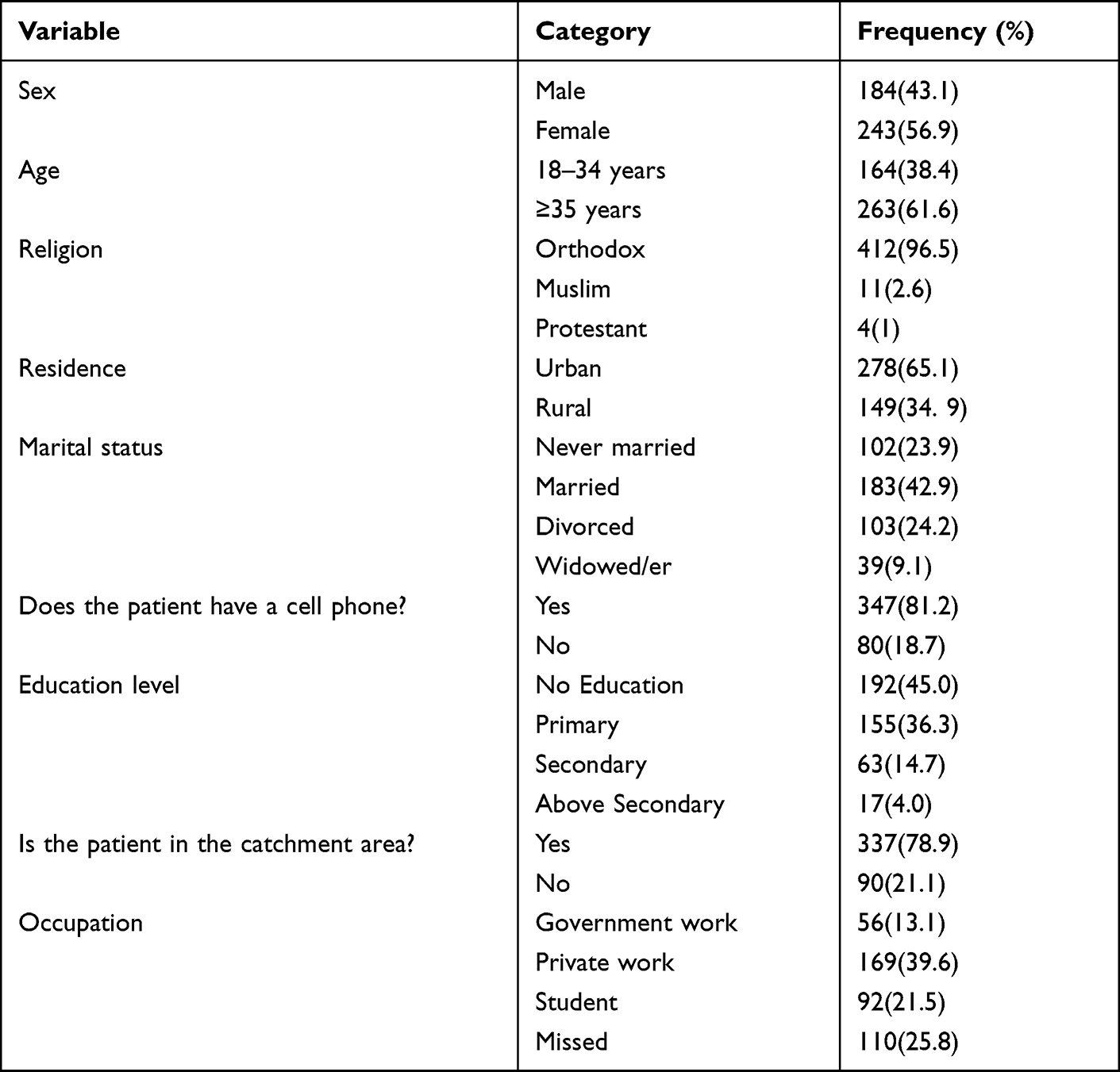 |
Table 1 Socio-Demographic Characteristics of HIV Infected Adults with 1st Line Virological Failure at High Load Public Health Facilities in Northwest Ethiopia, from 2016 to 2020 (n=427) |
The mean (±SD) of the baseline BMI of study participants was found to be 19.8 (±2.6) kg/m2. A total of 236 (55%) of HIV-infected adults have started with a Nevirapine-based first-line ART regimen and 358 (84%) had working functional status (Table 2).
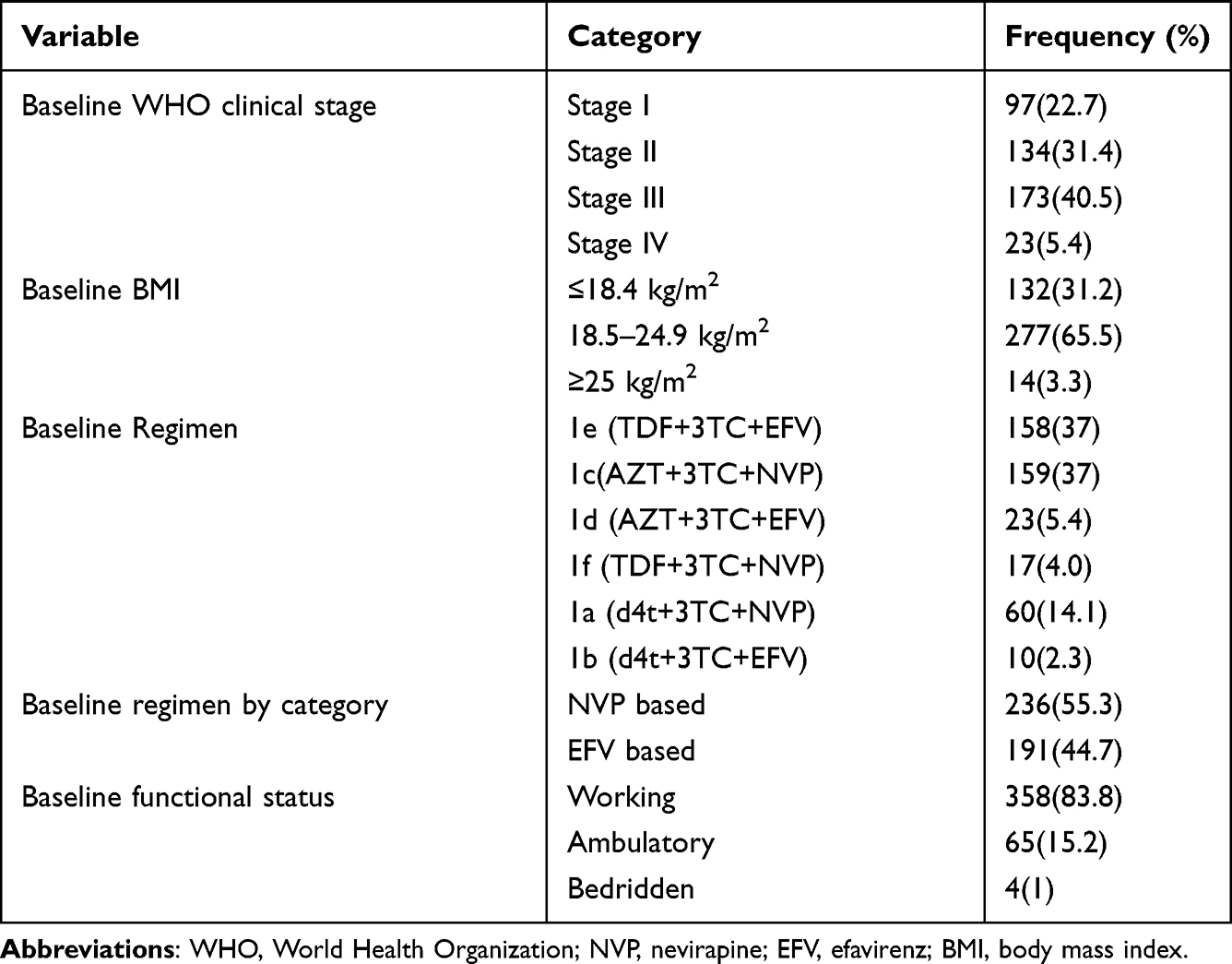 |
Table 2 Baseline Clinical, Laboratory, and ART Information of HIV Infected Adults with Virological Failure at High Load Public Health Facilities in Northwest Ethiopia, from 2016 to 2020 (n=427) |
One hundred one (23.7%) and 193 (45.1%) of HIV-infected adults reported using a condom and disclosed their HIV status to their family members respectively. Taking alcohol/Khat was reported by 105 (24.6%) HIV-infected adults. A total of 368 (86.4%) of HIV-infected adults had caregivers (Table 3).
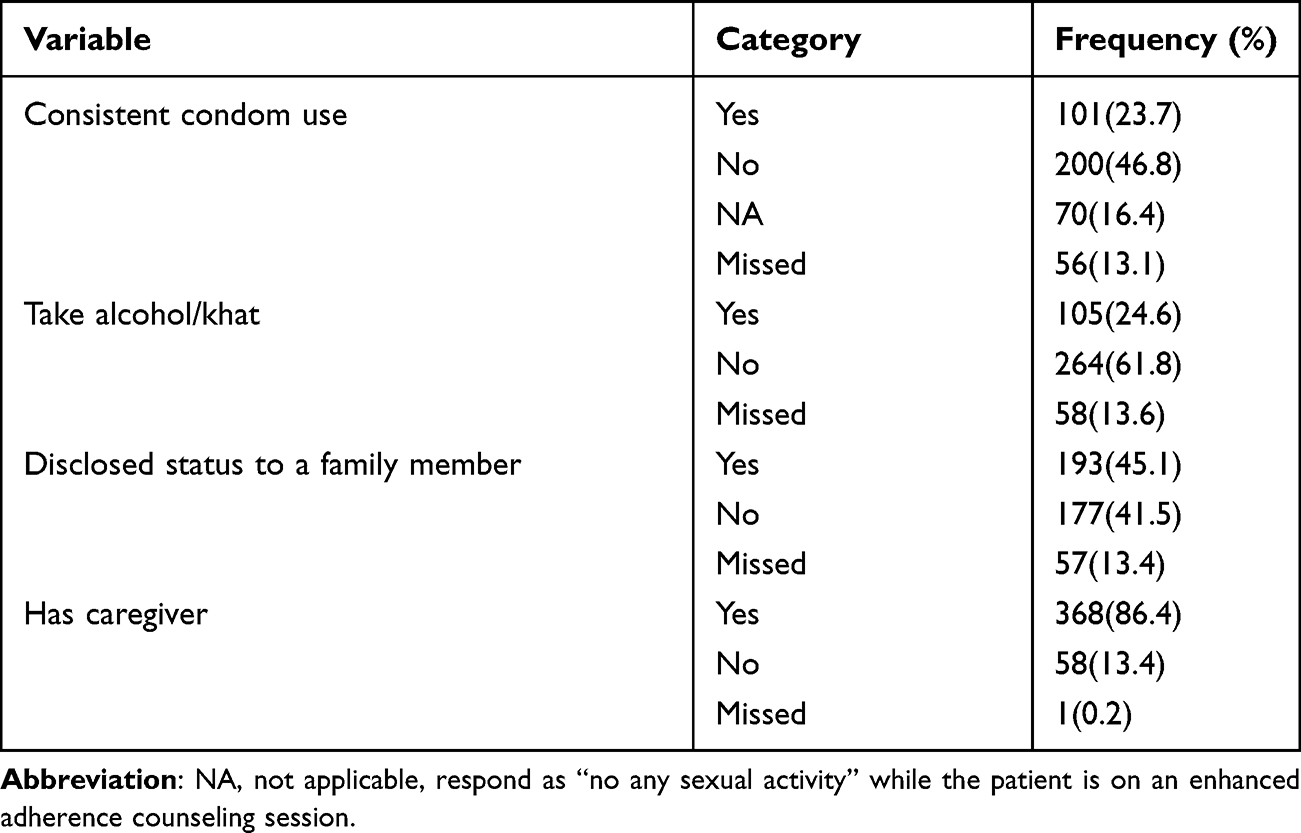 |
Table 3 ART Adherence Barriers of HIV Infected Adults with the First-Line Virological Failure at High Load Public Health Facilities in Northwest Ethiopia from 2016 to 2020 (n=427) |
The mean (±SD) duration on first-line ART was 6.9 (±3.2) years. A total of 390 (91.3%) HIV-infected adults had good adherence at the latest visit. Of all participants, 75 (17.6%) were found to be underweight by BMI, and 162 (37.9%) had a history of first-line regimen change at least once. Three hundred ten (72.6%) and 164 (39%) participants were provided with TPT and CPT respectively and only 31 (7.3%) participants were enrolled in a 6-month Appointment Spacing Model (ASM) before confirmed first line VF. Among all, 182 (42.6) had taken first-line ART for 5 to 8 years, 239 (55.7%) had completed EAC only with 3 sessions and the mean (±SD) time between 1st and 2nd HVL test was 11.0 months ± (5.2–13.6 IQR) months (Table 4).
 |
Table 4 ART Follow-Up, Laboratory and Clinical Information of Adult HIV Infected Patients with Virological Failure at High Load Public Health Facilities in Northwest Ethiopia, from 2016 to 2020 (n=427) |
Survival Status on First Line Regimen
The cumulative survival probability of HIV infected adults to take the failed first-line ART regimen at the end of follow up was 9.83% (95% CI: 4.96, 16.66) and the cumulative survival probability by 90, 180 and 360 days were 59%, 47%, and 36% respectively.
The Kaplan–Meier survival curve showed a steeper decrease during the initial follow-up periods, with a 0.50 cumulative estimated survival probability at 162 days. Thereafter, the percentage of people who survived showed a slower decrease over time, almost becoming flat at the end (Figure 1). A significant difference in survival probability of HIV-infected adults with first-line VF was observed among HIV infected adults with and without a history of first-line ART regimen change (Figure 2).
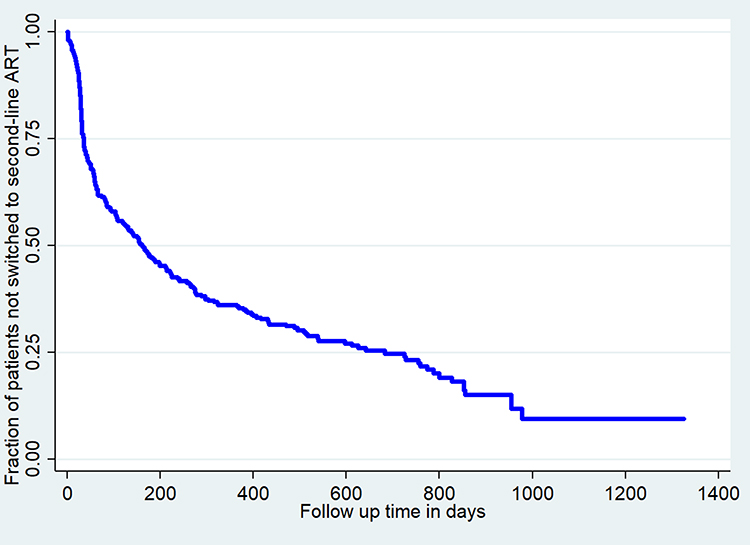 |
Figure 1 The Kaplan–Meier survival curve of time to switch to 2nd line anti-retroviral therapy (ART) and its predictors among HIV-infected adults at high load public health facilities in Northwest Ethiopia, from 2016 to 2020 (n=427). |
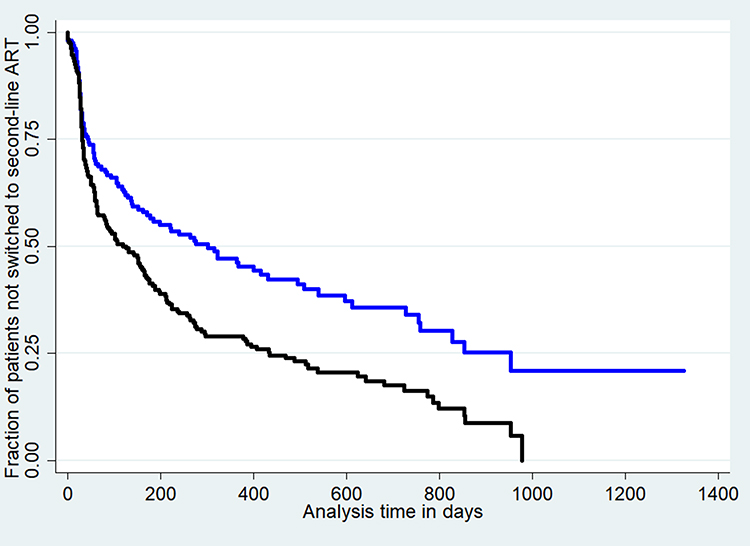 |
Figure 2 The Kaplan–Meier survival curve by regimen change for time to switch to 2nd line Anti-Retroviral Therapy (ART) and its predictors among HIV-infected adults at high load public health facilities Northwest Ethiopia, from 2016 to 2020 (n=427). (Blue line=survival curve of patients with 1st line regimen change, Black line = survival curve of patients with 1st line regimen change). |
Time to Switch to Second Line ART
Among 427 participants, 288 (67.4%) were switched to second-line ART and 139 were censored, contributing a total of 95,763 observation days under analysis with the median follow up time of 109 (31–332 IQR) days having 1 day and 1326 days of minimum and maximum follow up days respectively.
The estimated median time to switch is 162 days (95% Cl: 122, 211) (35–682 IQR). The median time varies across different explanatory variables such as first-line regimen change; those without and with regimen change, 127 had 303 days respectively.
As shown in Figure 3, 213 (74%) of HIV-infected adults are switched to second-line ART within the first 6 months since confirmed treatment failure (Figure 3). Among HIV-infected adults who were not switched to second-line ART, 82 (59%) were active and taking the first-line ART regimen (Figure 4).
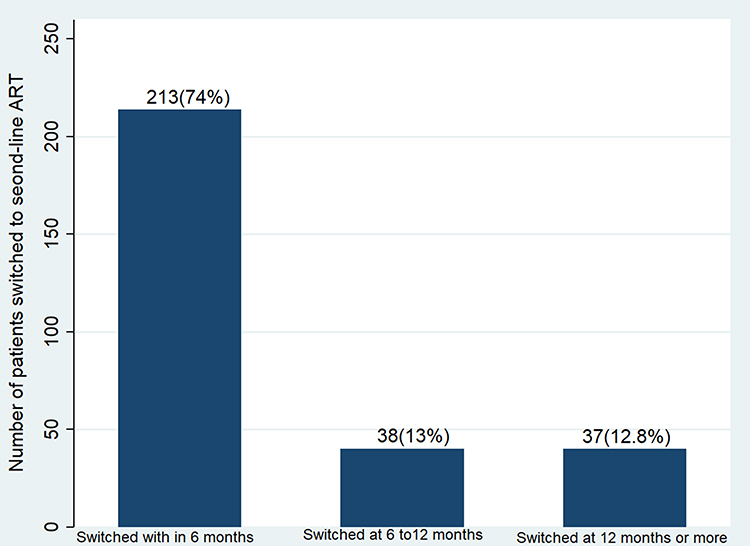 |
Figure 3 The bar graph of the proportion of switching by time to switch to the 2nd line Anti-Retroviral Therapy (ART) among HIV-infected adults at high load public health facilities in Northwest Ethiopia, from 2016 to 2020 (n=427). |
 |
Figure 4 The pie chart of the proportion of patients by final status among HIV-infected adults at high load public health facilities in Northwest Ethiopia, from 2016 to 2020 (n=427), (Blue=active, Orange=transferred out to other facility, Red=Lost to follow up, Green=dead). |
The overall incidence rate of switching was 3/1000 person-days (95% CI: 2.6, 3.3). The cumulative incidence of the switch by 3 and 6 months after failure was 6.1% and 4.6% respectively. Besides, the incidence of switching among those HIV-infected adults with and without regimen change was 2/1000-person day and 3/1000-person day.
Predictors of Time to Switch
From the bi-variable analysis, ten variables namely, first-line regimen change before failure, viral RNA copies at failure, duration on first-line ART, missed appointment, baseline WHO stage, duration of between first and second viral load test, number of EAC session, whether enrolled to ASM or not, latest BMI and residence with a p-value of ≤ 0.2 were statistically significant and then included for multivariable analysis. Thus, in multivariable analysis five variables namely history of first-line regimen change, viral RNA copies at failure, duration on first-line ART before failure, missed appointments, and the number of EAC sessions were significantly associated with time to switch to second-line ART with 95% confidence level and p-value of less than 0.05 (Table 5).
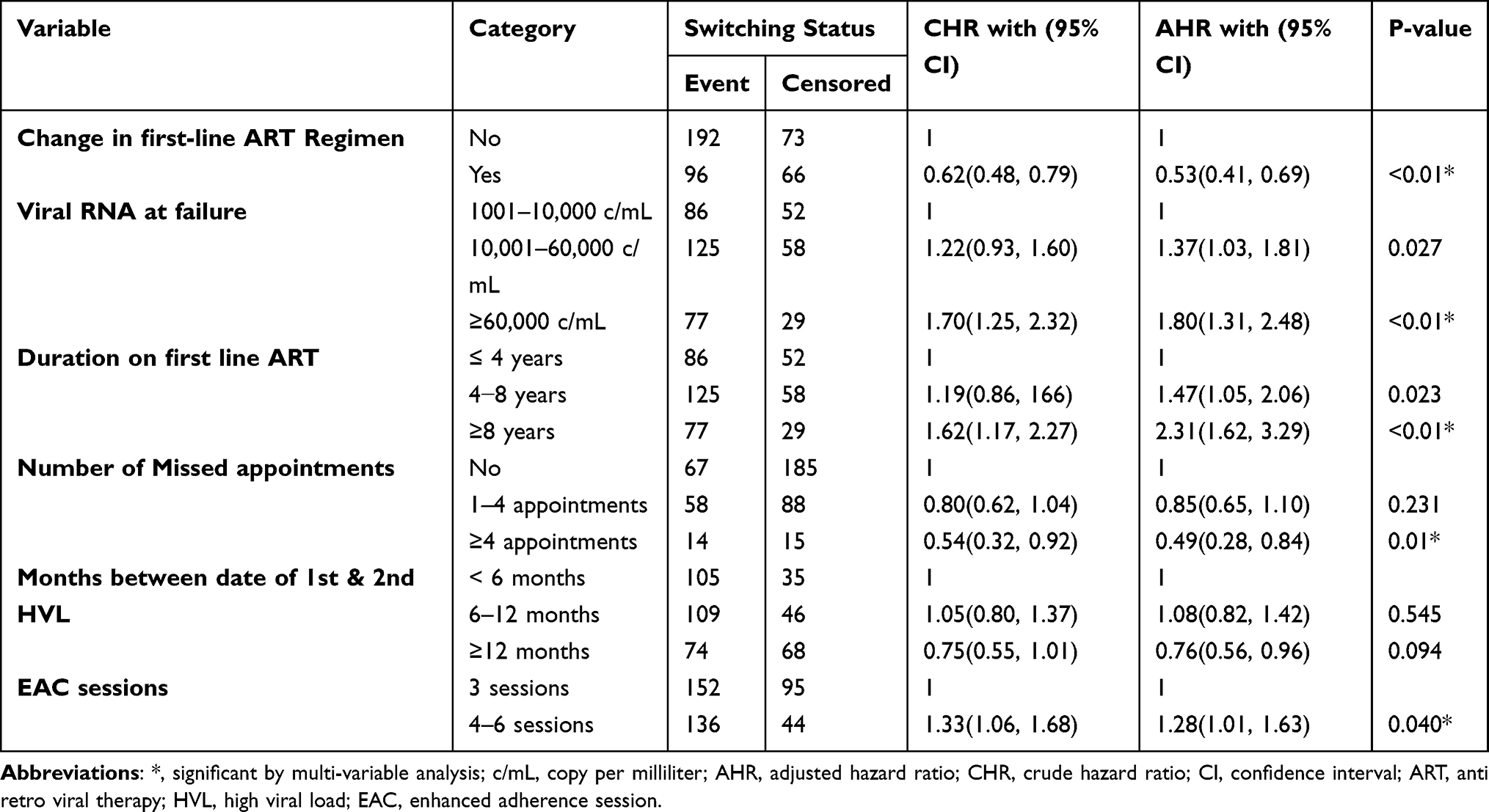 |
Table 5 Bi-Variable and Multivariable Analysis of Predictors of Time to Switch to 2nd Line ART Among HIV-Infected Adults at High Load Public Health Facilities in Northwest Ethiopia, from 2016 to 2020 (n=427) |
In this study, the risk of switching to second-line ART among HIV-infected adults with first-line regimen change was lower by 47% compared to their counterparts (AHR: 0.53, 95% CI: 0.41, 0.69). Similarly, the risk of switching to a second-line ART regimen among HIV infected adults with viral RNA of 60,000 copies/mL or more during failure was 1.8 times higher than those HIV infected adults with viral RNA of fewer than 10,000 copies/mL during failure (AHR: 1.8, 95 CI: 1.31, 2.48). It is also true that the risk among HIV infected adults with viral RNA of 10,001 to 60,000 copies/mL was 1.37 times higher than those HIV infected adults with viral RNA of 1001 to 10,000 copies/mL during failure (AHR: 1.37, 95% CI 1.03, 1.81) (Table 5).
The duration on first-line ART is significantly associated with the switching to a second-line regimen, in which those HIV-infected adults who were on first-line ART for 8 years or more had a 2.31 times higher risk of switching to second-line ART compared to those who were taking for less than 4 years (AHR: 2.31, 95% CI: 1.62, 3.29). It is also true that taking first-line ART for 4 to 8 years had a 1.47 times higher risk of switching than those who were taking it for less than 4 years (AHR: 1.47, 95% CI: 1.05, 2.06). This study also indicated that the risk of switching to a second-line ART among HIV infected adults with a history of 4 or more missed appointments 1 year before VF decreased by 51% compared to those who had a history of no missed appointment (AHR: 0.49, 95% CI: 0.28, 0.84). Besides, the risk of switching to a second-line ART among HIV-infected adults who completed EAC by 4 to 6 sessions was 1.28 times higher compared with HIV-infected adults who completed EAC by 3 sessions (AHR: 1.29, 95% CI:1.01, 1.63) (Table 5).
Discussion
This study followed 427 HIV-infected adults for a total of 95,763 observation days under analysis with the median follow-up time of 109 days having 1 day and 1326 days of minimum and maximum follow-up days respectively. The cumulative incidence of switching to second-line ART among HIV-infected adults with first-line virological failure was 67.4% over 4 years follow-up period with the overall incidence rate of switching 3/1000 person-days observation.
The finding of this study showed that the median time to switch was 162 days in which half of the HIV infected adults were taking the already failed first-line ART up to 162 days despite the Ethiopian national guideline recommendation to switch to second-line ART immediately after virological first-line treatment failure.5,7 This finding is greater than the findings of the study in South Africa (102 days),19 Uganda and South Africa (116 days),16 and another study in South Africa (121 days). The delay in switching might be due to resource-limited settings where second-line treatment options are limited, HIV-infected adult’s behavior-related factor-like missed appointments that could delay the decision making by the clinical switching team to switch the regimen. In South Africa, all community clinics were led by doctors which might have contributed to the timely decision to switch to second-line ART.17 However in Ethiopia, no medical doctors were available at health centers during the study period. In addition, in Ethiopia, because the third-line ART option is available only in a few hospitals, clinicians’ reservation to not narrowing patients’ treatment options might be the potential reason for delaying switching compared to other countries having a shorter time to switch.
Differing from that, the median time to switch in this study was lower than the median time of switch in the studies done at South Africa (public hospital in eThekwini, KwaZulu-Natal; 192 days)28 and Uganda (243 days).17 The delays in switching might be because the ART service was being scaled up to many facilities in South Africa and that allowed too many patients were offloaded before knowing their final switching status.
The risk of switching to second-line ART among HIV-infected adults who had a history of first-line regimen change was lower compared with their counterparts. This is in line with the study conducted in Myanmar,27 which probably might be due to providers’ motivation to evaluate clinical outcomes of the newly modified better regimen that include Dolutegravir by following for more periods against the standard and to preserve the chance of the patient’s treatment options. As Ethiopia has adopted the Dolutegravir rollout campaign since Feb 2019, ART providers might be motivated to evaluate its effectiveness for more periods.
HIV-infected adults with viral RNA of 60,000 copies/mL or more were 1.8 times higher risk for switching to second-line ART which is consistent with the study done in South Africa.19 The same is true for the studies done in Uganda17 and South Africa.29 An increasing viral load count shows the degree of the severity of uncontrolled viral replication which in turn tells us impaired functionality of the first-line regimen. Virological treatment failure later leads to worsening immunologic and clinical conditions. Due to that, health care providers might have perceived those patients with worse health conditions need to be switched early. It is also suggestive that clinicians may delay switch to optimize adherence and preserve first-line ART for patients with lower viral load count. In addition, the risk of HIV transmission is higher among people with higher viral RNA copies.4,5 Therefore providers might consider that switching people with VF to second-line ART as a prevention strategy. But the finding of this study is conflicting with the finding of the study done in South Africa which is lower viral RNA copy was the risk for the switch to second-line ART. The possible reason for the difference could be that in the previous study increased drug resistance and being non-adherent was common among people with higher viral RNA copies. Due to this, providers focused on resolving the adherence problem before switching. It could also be because of difference in study setting that includes categorization of viral RNA copies, sample size, the health system factor, and the health care provider’s motivation.22
This study yields that, the risk of switching among HIV-infected adults with a history of 4 or more missed appointments was lower than those with no missed appointments. It is supported by studies done in South Africa.18,19,22 Healthcare providers indeed require repeated visits and exhaustive counseling to rule out causes of viremia other than treatment failure through intensive adherence counseling. So, a lower risk of switching among HIV-infected adults with a history of 4 or more missed appointments might be because healthcare providers had no repeated opportunity to assess possible causes and decide to take action.
This study also evidenced that the risk of switching to second-line ART among HIV-infected adults with the duration of 8 or more years taking on the first-line treatment was 2.31 times higher compared with those with less than 4 years taking on first-line ART. This finding is in agreement with the study done in sub-Saharan African countries21 and low-income countries.24 This might reflect that the advancement in first-line regimens to a more effective drug in people who started ART in the recent years, including improved expertise in managing treatment-related complications, as well as more cautious management towards treatment failure, which required an additional adherence check and not to narrowing the treatment options for HIV infected adults where there is limited access to a third-line regimen. Opposing to that, studies done in South Africa stated that, starting ART in recent years had an increased risk of switch relative to starting ART in remote years.18 The difference might be due to the study setting and period.
The current study also showed that EAC of 4–6 sessions was also found to be an important independent predictor of time to switch, in which EAC of 4–6 sessions had a 1.28 risk of switch compared with EAC of 3 sessions. This is probably because frequent visits and counseling support help the provider to be certain that adherence problems are resolved and decide to switch early. Effective EAC improves patients’ compliance to the ART by resolving adherence barriers working on patients’ behavioral, cognitive, emotional, and social factors. Therefore, it results in up to 70% of viral re-suppression in patients with first HVL. It reflects the importance of repeated EAC in improving the care as well to support the certainty of the cause of viremia, which eases the decision to continue on the first-line regimen or to switch to second-line ART.5,30
Conclusion
This study reflects time to switch to second-line ART following first-line Virological failure is 162 days, higher than other related studies. But the rate of switching was higher among HIV infected adults with viral RNA 60000 copies/mL or more, eight years or more duration on first-line ART and EAC of 4 to 6 sessions, and lower among HIV infected adults with a history of first-line regimen change and four or more missed appointments. So, intervention strategies that support patients to have timely switch without due delays as soon as virologic failure should be prioritized.
Abbreviations
AHR, adjusted hazard ratio; AIDS, acquired immune deficiency syndrome; ART, anti-retroviral therapy; ARV, anti-retroviral; BMI, body mass; CPT, cotrimoxazole prophylactic therapy index; EAC, enhanced adherence counseling; EAS, enhanced adherence support; HAART, highly active ant-retroviral therapy; HIV, human immune deficiency virus; KM, Kaplan–Meier; TPT, tuberculosis preventive therapy; PI, protease inhibitor; VF, virological failure; VL, viral load.
Data Sharing Statement
All materials and data are available from the corresponding author without any restriction.
Ethical Approval and Consent to Participate
The use of routinely collected anonymous clinical data was approved for this research project by “Debre Markos University, college of health Science Research Review and Ethical Committee” by the reference number HSC/R/C/Scr/CO/41/11/13. Permission was approved from selected public health facilities to use an anonymous medical registration number only for each individual as an identifier, and confidentiality was assured. The recorded had been kept confidential and not accessed by a third person except the PI.
Acknowledgments
We would like to acknowledge Debre Markos University, Health Science College, department of public health for facilitating all the requirements from beginning to the completion of this work. We are also equally indebted to all health facilities included in this work for all the cooperation they paid for this study to be completed. Finally, we are grateful to data collectors, supervisors, and data clerks of respective health facilities for their honest cooperation in obtaining the data for this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work had no funds except that the cost was covered by the principal investigator.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Federal Ministry of Health (FMOH) Ethiopia Ethiopian national comprehensive HIV care guideline 2018.pdf. 2018.
2. UNAIDS. Ethiopia UNAIDS.pdf; 2019. Available from: https://www.unaids.org/sites/default/files/media_asset/2019-UNAIDS-data_en.pdf.
3. Schwartländer B, Stover J, Hallett T, et al. Towards an improved investment approach for an effective response to HIV/AIDS. Lancet. 2011;377(9782):2031–2041. doi:10.1016/S0140-6736(11)60702-2
4. World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach.
5. Federal Ministry of Health (FMOH) Ethiopia. National consolidated guidelines for comprehensive HIV prevention, care and treatment. 2018.
6. WHO. What’s new in treatment monitoring: viral load and CD4 testing; 2017. Available from: https://www.who.int/hiv/pub/arv/treatment-monitoring-info-2017/en/.
7. World Health Organization. Update of recommendations on first-and second-line antiretroviral regimens. World Health Organization; 2019. Available from: https://www.who.int/hiv/pub/arv/arv-update-2019-policy/en/.
8. Madec Y, Leroy S, Rey-Cuille MA, Huber F, Calmy A. Persistent difficulties in switching to second-line ART in sub-Saharan Africa—a systematic review and meta-analysis. PLoS One. 2013;8(12):e82724.
9. Zhou J, Li P, Kumarasamy N, et al. Deferred modification of antiretroviral regimen following documented treatment failure in Asia: results from the TREAT Asia HIV Observational Database (TAHOD). HIV Med. 2010;11(1):31–39. doi:10.1111/j.1468-1293.2009.00738.x
10. Niguse H. Reasons for Antiretroviral Drug Switch Among Patients Attending at the Antiretroviral Therapy clinic of Tikur Anbesa Specialized Hospital. Addis Ababa, Ethiopia: Addis Ababa University; 2016.
11. Ajose O, Mookerjee S, Mills EJ, Boulle A, Ford N. Treatment outcomes of patients on second-line antiretroviral therapy in resource-limited settings: a systematic review and meta-analysis. AIDS (London, England). 2012;26(8):929–938. doi:10.1097/QAD.0b013e328351f5b2
12. Shroufi A, Van Cutsem G, Cambiano V, et al.Simplifying switch to second-line antiretroviral therapy: predicted effect of defining failure of first-line efavirenz-based regimens in sub-Saharan Africa by a single viral load more than 1000 copies/mL. AIDS (London, England). 2019;500:18–01168.
13. WHO. Global Action Plan on HIV Drug Resistance 2017–2021. WHO; 2017.
14. Kiweewa F, Esber A, Musingye E, et al. HIV virologic failure and its predictors among HIV-infected adults on antiretroviral therapy in the African Cohort Study. PLoS One. 2019;14(2):e0211344.
15. Feleke R, Geda B, Teji Roba K, Weldegebreal F. Magnitude of antiretroviral treatment failure and associated factors among adult HIV-positive patients in Harar public hospitals, Eastern Ethiopia. SAGE Open Med. 2020;8:1–7.
16. Petersen ML, Tran L, Geng EH, et al.Delayed switch of antiretroviral therapy after virologic failure associated with elevated mortality among HIV-infected adults in Africa. AIDS. 2014;28(14):2097.
17. Victor Ssempijja GN, Chang L, Gray R, et al. Rates of switching to second-line antiretroviral therapy and impact of delayed switching on immunologic, virologic, and mortality outcomes among HIV-infected adults with virologic failure in Rakai, Uganda. BMC Infect Dis. 2017;17:1.
18. Rohr J, Ive P, Berhanu R, et al. Predictors of time to switch to second line ART after first line failure in Johannesburg, South Africa. Age. 2014;37:
19. Rohr JK, Ive P, Horsburgh CR, et al. Marginal structural models to assess delays in second-line HIV treatment initiation in South Africa. PLoS One. 2016;11(8):e0161469. doi:10.1371/journal.pone.0161469
20. Petersen ML, Tran L, Geng EH, et al. Delayed switch of antiretroviral therapy after virologic failure associated with elevated mortality among HIV-infected adults in Africa. AIDS (London, England). 2014;28(14):2097. doi:10.1097/QAD.0000000000000349
21. Palombi L, Marazzi MC, Guidotti G, et al. Incidence and predictors of death, retention, and switch to second-line regimens in antiretroviral-treated patients in sub-Saharan African Sites with comprehensive monitoring availability. Clin Infect Dis. 2009;48(1):115–122. doi:10.1086/593312
22. Johnston V, Fielding KL, Charalambous S, Churchyard G, Phillips A, Grant A. Outcomes following virological failure and predictors of switching to second-line antiretroviral therapy in a South African treatment program. J Acquir Immune Defic Syndr. 1999;2012:370–380.
23. Johnston V, Fielding K, Charalambous S, et al. Second-line antiretroviral therapy in a workplace and community-based treatment programme in South Africa: determinants of virological outcome. PLoS One. 2012;7(5):e36997. doi:10.1371/journal.pone.0036997
24. Keiser O, Tweya H, Boulle A, et al. Switching to second-line antiretroviral therapy in resource-limited settings: comparison of programmes with and without viral load monitoring. AIDS (London, England). 2009;23(14):1867.
25. Rohr JK. First Line Antiretroviral Treatment Failure and Second Line Treatment Outcomes Among HIV Patients in Southern Africa. Boston University Theses & Dissertations; 2015.
26. East Gojjam Zone Health Department. HIV Program 4th Quarter Report. Debre Markos: East Gojjam Zone Health Department; 2020.
27. Kyaw NTT, Harries AD, Kumar AM, et al. High rate of virological failure and low rate of switching to second-line treatment among adolescents and adults living with HIV on first-line ART in Myanmar, 2005–2015. PLoS One. 2017;12(2):e0171780. doi:10.1371/journal.pone.0171780
28. Narainsamy D, Mahomed S. Delays in switching patients onto second-line antiretroviral treatment at a public hospital in eThekwini, KwaZulu-Natal. South Afr J HIV Med. 2017;18:1–5.
29. Bell-Gorrod H, Fox MP, Boulle A, et al.The impact of delayed switch to second-line antiretroviral therapy on mortality, depending on failure time definition and CD4 count at failure. Am J Epidemiol. 2019;189(8):811–819.
30. Haas AD, Keiser O, Balestre E, et al. Monitoring and switching of first-line antiretroviral therapy in adult treatment cohorts in sub-Saharan Africa: collaborative analysis. Lancet HIV. 2015;2(7):e271–e8. doi:10.1016/S2352-3018(15)00087-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.