Back to Journals » International Medical Case Reports Journal » Volume 18
Thyroid Tuberculosis: Misdiagnosed as Papillary Thyroid Carcinoma – A Rare Case Report
Authors Tong Y ![]() , Yao J
, Yao J ![]() , Chen Y, Yu Q, Lu Y, Xuan M
, Chen Y, Yu Q, Lu Y, Xuan M
Received 19 July 2025
Accepted for publication 16 October 2025
Published 27 October 2025 Volume 2025:18 Pages 1371—1376
DOI https://doi.org/10.2147/IMCRJ.S553344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Yanhua Tong,1 Jiejie Yao,1,2 Yingzhen Chen,1 Qichun Yu,3 Yu Lu,4 Ming Xuan5
1Department of Ultrasound, Civil Aviation Shanghai Hospital, Shanghai, People’s Republic of China; 2Department of Ultrasound, Ruijin Hospital, Shanghai Jiao Tong University Medical School, Shanghai, People’s Republic of China; 3Department of Pathology, Civil Aviation Shanghai Hospital, Shanghai, People’s Republic of China; 4Department of Radiology, Civil Aviation Shanghai Hospital, Shanghai, People’s Republic of China; 5Department of General Surgery, Civil Aviation Shanghai Hospital, Shanghai, People’s Republic of China
Correspondence: Jiejie Yao, Department of Ultrasound, Ruijin Hospital, Shanghai Jiao Tong University Medical School, 2nd Ruijin Road 197, Shanghai, People’s Republic of China, Tel +8613661812474, Email [email protected]
Background: Thyroid tuberculosis (TTB), either in its primary or secondary form, is a rare occurrence, even in recent years, with a high incidence of tuberculosis in China. Nowadays, with the increasing morbidity of thyroid nodules, it is apt to be misdiagnosed with malignant tumors. In this case, a suspicious malignant lesion was found on thyroid ultrasound (US), but the result after the surgery showed TTB.
Case Presentation: This article reported a 67-year-old woman who was found left thyroid nodules during a physical examination three month ago. Thyroid US showed two suspicious hypoechoic lesions in the left thyroid gland and diagnosed as Chinese Thyroid Imaging Reporting and Data System. (C-TI-RADS) 4A category. The patient underwent US-guided fine needle aspiration of the two lesions, the results of which showed that suspected malignant tumors were not excluded. The patient underwent a left thyroidectomy and central group lymph node dissection. Postoperative pathological examination showed granulomatous inflammation with caseous necrosis in the thyroid gland, and diagnosed as tuberculosis. The patient had nonspecific clinical symptoms, no history of exposition, and no pulmonary involvement. Subsequently, the patient visited the tuberculosis specialist outpatient clinic for treatment.
Conclusion: This case report aims to enhance clinicians’ awareness of TTB. With the increasing detection rate of thyroid nodules in US, it is crucial to distinguish between benign and malignant ones. TTB is often overlooked. Considering the existence of tuberculosis, unnecessary surgical treatment can be avoided.
Keywords: thyroid tuberculosis, misdiagnose, ultrasound, TTB, US
Introduction
It is common knowledge that tuberculosis is one of the most serious public health problems worldwide. According to the World Health Organization's (WHO) Global Tuberculosis Report 2024 it is estimated that there are approximately 10.8 million new cases of tuberculosis worldwide. Among the 30 countries with a high burden of tuberculosis, China ranks third. In 2023, the estimated number of new tuberculosis patients in China was 741,000, with an incidence rate of 52 per 100,000, accounting for 6.8% of the global total.1 However, during the recent Covid-19 pandemic, tuberculosis and Covid-19 have jointly become the main causes of global infectious disease deaths.2 And there is evidence suggesting that the risk of death from Covid-19 combined with tuberculosis is higher than that form a single pathogen.3,4 So the severith of tuberculosis still needs to be taken seriously.
Tuberculosis has been reported in many organs of the body, such as lung, lymph nodes, intestines, kidneys, brain, and bones. However, thyroid tuberculosis (TTB) is an uncommon entity with low incidence rate (0.1–0.4%),5 even in countries where the prevalence of pulmonary tuberculosis is high. The reasons may be explain with the abundant of thyroid colloids, the high supply of blood and oxygen content in thyroid gland, which have strong immunity against tuberculosis. Moreover, a lack of the reticuloendothelial cells in thyroid gland may be another reason of low occurrence of TTB, since reticuloendothelial cells are susceptible to tuberculosis invasion. In clinical practice, it may meet a diagnostic dilemma due to the relative infrequency of occurrence and nonspecific clinical symptoms. It may also present a broad spectrum of manifestations on ultrasound (US), and is hard to be differentiated with thyroiditis, or malignant tumors. A history of tuberculosis at other sites, such as lung or lymph nodes, or a history of TB contact may be help for differential diagnosis. With the development of anti-tuberculosis drugs, TTB can be cured through medical treatment. However, due to the lack of specific signs, it is apt to be misdiagnosed before surgery, which may cause unnecessary surgical trauma.
Case Presentation
A 67-year-old woman was found with left thyroid nodules during a physical examination, and then went to our hospital for further examination. An outpatient physical examination showed the patient with bilateral neck symmetry, soft neck, and centered trachea. The patient had no chronic diseases, had been in good health in the past, had a good nutritional status, had no history of long-term medication, smoking or drinking, and had a body mass index (BMI) within the normal range (BMI = 19.5). The patient had no clinical symptoms of tuberculosis infection such as pain, heat, sweating, heart palpitation and dispositional change, and had no dysphagia, no anorexia, and no weight loss.
Thyroid US indicated that two hypoechoic lesions were found in the left thyroid gland. The size of one lesion was 19.5 (the upper and lower) × 12 (the front and rear) × 16 (the left and right) millimeter (mm), another lesion’s size was 14.9 × 8.4 × 11.3mm. Both lesions had parallel orientations, hypoechogenicity, irregular shapes, unclear boundaries, clustered calcifications, no significant change of the posterior acoustic, high marginal vascularity and low internal blood flow (Figure 1). Several lymph nodes were observed in the side and central regions of left neck. Based on the sonographic features, the two lesions was diagnosed as Chinese Thyroid Imaging Reporting and Data System category 4A (C-TI-RADS 4A),6 subsequently, the patient underwent US-guided FNA of the left thyroid lesions. Due to necrosis absent, the sample cell quantity is small, resulting in Cytological pathological results showed: “Suspected papillary thyroid carcinoma, The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) V category.”
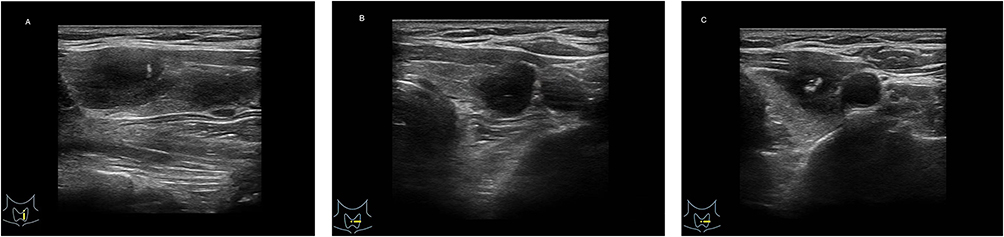 |
Figure 1 Ultrasound features of thyroid tuberculosis. (A) Longitudinal section showed two lesions were found in left thyroid gland; (B) Cross section showed one lesion with low echo and unclear boundary; (C) Cross section showed another lesion with irregular shape, and clumpy calcification. |
The patient was admitted to the department of general surgery for surgery. Preoperative laboratory examinations showed that thyroglobulin (TG) was slightly increased with the value of 78.8ng/mL (standard value: 3.50–77.0ng/mL), other thyroid function indicators including serum triiodothyronine (T3), thyroxine (T4), free triiodomethane (FT3), free thyroxine (FT4) and thyroid stimulating hormone (TSH) were all normal. The Complete Blood Count (CBC) indicated a slightly decreased percentage of neutrophils at 32.7% (standard value: 40–75%), a slightly increased percentage of lymphocytes at 59.3% (standard value: 20–50%), all other blood cell counts were normal. Biochemical tests including blood glucose, blood lipid, liver function, kidney function and electrolytes all showed normal results. Chest CT found minor nodules beside the oblique fissure of the right lung, a little fibrosis in both lungs, and local thickening of pleura on both sides (Figure 2). A left thyroidectomy and central group lymph node dissection were performed. During the operation, two nodules were found on the left thyroid gland. The size of upper pole mass was about 1.5 cm, and the lower polar mass was about 1.2 cm. Both lesions were soft in texture, with no penetration of envelope. The left thyroid gland was completely removed and the left central group lymph nodes were cleared. Postoperative pathological examination indicated that the granulomatous inflammation in the left thyroid gland with locally visible caseous necrosis (Figure 3). The final pathological results were TTB. Immunohistochemical examination showed that cytokeratin 19 negative, (CK19-), galactin 3 antibody positive (Galectin-3+), human bone marrow endothelial cell marker-1 negative (HBME-1-), TG negative (Tg-), thyroid transcription factor-1 negative (TTF-1-), Papillary thyroid carcinoma was ruled out. Also, for the central group, there were different number of granulomatous structures in all 18 lymph nodes.
 |
Figure 2 Chest CT showed no abnormalities. |
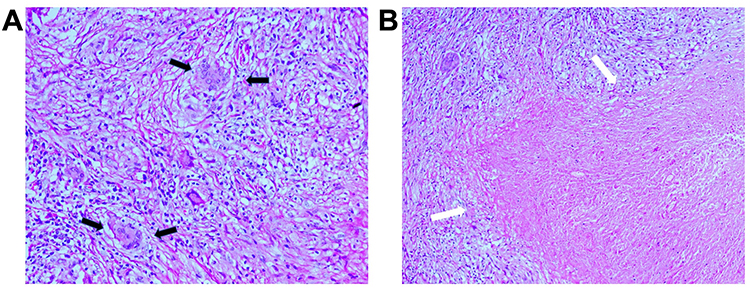 |
Figure 3 Pathological findings of thyroid tuberculosis. (A) Epithelioid granulomas with Langerhans cells were observed in the thyroid gland (black arrows) (hematoxylin-eosin, HE 20X). (B) Caseous necrosis can be seen in the center (white arrows) (hematoxylin-eosin, HE 10X). |
Discussion
With the widespread application of tuberculosis vaccines and the development of effective anti-tuberculous drugs, the morbidity of tuberculosis has been significantly decreased in China. In 2025, the American Thoracic Society (ATS) and the Centers for Disease Control and Prevention (CDC), European Respiratory Society (ERS), and the Infectious Diseases Society of America (IDSA) jointly released an updated version of theTreatment of Drug-Sensitive and Drug-Resistant Tuberculosis, provides new recommendations for the treatment of tuberculosis. The recommended first-line treatment regimen is a 4-month combination of Isoniazid (INH or H), Rifapentine (RFT), Moxifloxacin (MXF or M) and Pyrazinamide (PZA or Z) (2HPZM / 2HPM).7 For patients with drug-resistant tuberculosis (DR-TB), a fully oral short-course regimen containing new drugs such as Bedaquinoline, Primamab and Linezolid is recommended, which significantly improves the success rate and safety of treatment.8
As a rare condition, TTB can be divided into primary and secondary. The former is that after the initial infection with tuberculosis bacilli, the mycobacterium tuberculosis enter the blood and can be latent in the thyroid. The vast majority of infected people have no signs or symptoms of TB and will never develop to TTB. The risk of developing active TB after infection depends on age, the quality of the immune defense mechanisms, and the time elapsed since the infection.9 About 20% of the general population in China has latent TB infection, and the probability of progression to active TB lifetime is about 5%–10%.10,11 When the host immunity is reduced, the dynamic balance between the immune response of the body and the tuberculosis bacterium will broke, the tuberculosis bacterium will be activated from the dormant state, and then further proliferates, spreads, and finally develops into active tuberculosis.9 Secondary TTB often occurs after other parts of tuberculosis, such as pulmonary, cervical lymph nodes etc. Tubercle bacilli spreads through blood or lymph nodes, or directly infects the thyroid gland. Originally, it is difficult to determine the primary or secondary TTB in clinical since the patient has no symptoms of systemic poisoning of tuberculosis, and the chest CT also shows no lesions. Meanwhile, the lack of tuberculosis related clinical manifestations and auxiliary examination evidence makes the diagnosis more difficult. It is generally believed that tuberculous infection spreads to the thyroid by lymphogenous, hematogenous route or directly from adjacent organs. In this case, pathological results indicated that all lymph nodes in central regions of the neck contained granulomatous structures, so the patient most likely had secondary lymphatic infection.
The reasons for the misdiagnosis of this patient were as follows: First, the patient lacked symptoms of systemic intoxication of tuberculosis, such as low fever, night sweats, fatigue, and emasculation. Second, the patient had no local symptoms, such as neck pain and discomfort. Moreover, chest CT showed no imaging manifestations of tuberculosis infection or old tuberculosis. Finally, the US features manifested as lesions with hypoechogenicity, irregular shapes, unclear boundaries and clustered calcifications which were difficult to distinguish from subacute thyroiditis or thyroid malignancy.
Limited published literature has reported TTB. Ozekinci et al12 indicated that the diagnosis of TTB is difficult without histopathological examination of surgical material. Sharma et al13 emphasized the importance of US as the standard imaging method for thyroid nodules evaluation. However, the specific US features of TTB have been rarely evaluated. Nowadays, with the increasing morbidity of thyroid nodules, it is apt to be misdiagnosed with malignant tumors. US-FNAC is of major importance for the differentiation when US shows a suspicious thyroid nodule.14 However, there are still some false negative results due to the extracted limited small samples, making it difficult for clear diagnosis, which increases the probability of patients receiving excessive surgery.
Conclusion
This case report presents a rare and misdiagnosed TTB, which raise the awareness for clinicians to consider this rare disease in the differential diagnosis of thyroid lesions. Moreover, for lesions with malignant US features, the possibility of benign disease such as subacute thyroiditis or TTB should be considered. If FNAC cannot provide a clear diagnosis due to the limited tissue, it can be combined core needle biopsy and other tests, such as molecular biological tests (nucleic acid amplification technology [PCR]; GeneXpert MTB/RIF), immunological tests (tuberculin skin test [TST] and interferon-γ release test [IGRA]), to avoid unnecessary thyroid surgery.
Data Sharing Statement
The data and materials presented in the case report are available on reasonable request from the corresponding author J.J.Y, [email protected].
Ethics Statement
An institution’s ethics committee approval is not required for the case reports.
Informed Consent Statement
This case report has received consent to publish from the patient.
Acknowledgments
We would like to thank the patient and all the staff for their contributions to this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work did not receive any funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organization. Global tuberculosis report 2024. Geneva: World Health Organization; 2024.
2. World Health Organization. Global tuberculosis report 2022. Lancet Microbe. 2022;(1)
3. Zimmer AJ, Klinton JS, Oga-Omenka C, et al. Tuberculosis in Times of Covid-19. J Epidemiol Comm Health. 2021;76:310–316. doi:10.1136/jech-2021-217529
4. Ritacco V, Kantor IN. Tuberculosis and COVID-19: a dangerous relationship. Medicina (B Aires). 2020;80 Suppl 6:117–118.
5. Bansal LK, Gupta S, Gupta AK, Chaudhary P. Thyroid tuberculosis. Indian J Tuberc. 2021;68(2):272–278. doi:10.1016/j.ijtb.2020.09.006
6. Zhou J, Yin L, Wei X, Zhang S, Song Y, Luo B, Superficial Organ and Vascular Ultrasound Group of the Society of Ultrasound in Medicine of the Chinese Medical Association; Chinese Artificial Intelligence Alliance for Thyroid and Breast Ultrasound. 2020 Chinese guidelines for ultrasound malignancy risk stratification of thyroid nodules: the C-TIRADS. Endocrine. 2020;70(2):256–279. doi:10.1007/s12020-020-02441-y
7. Carr W, Kurbatova E, Starks A, et al. Interim guidance:4-month rifapentine-moxifloxacin regimen for the treatment of drugsusceptible pulmonary tuberculosis-United States, 2022[J]. Morb Mortal Wkly Rep. 2022;71(8):285–289. doi:10.15585/mmwr.mm7108a1
8. Guglielmetti L, Khan U, Velásquez GE, et al. oral regimens for rifampin-resistant, fluoroquinolone-susceptible tuberculosis. N Engl J Med. 2025;392(5):468–482. doi:10.1056/NEJMoa2400327
9. Zellweger JP, Sotgiu G, Corradi M, Durando P. The diagnosis of latent tuberculosis infection (LTBI): currently availabletests, future developments, and perspectives to eliminate tuberculosis (TB). Med Lav. 2020;111(3):170–183. doi:10.23749/mdl.v111i3.9983
10. Araújo AN, Matos T, Boavida J, Bugalho MJGM. Thyroid tuberculosis: an unexpected diagnosis. BMJ Case Rep. 2021;14(2):e238795. doi:10.1136/bcr-2020-238795
11. Diel R, Loddenkemper R, Nienhaus A. Predictive value of interferon-gamma release assays and tuberculin skintesting for progression from latent TB infection to disease state: a meta-analysis. Chest. 2012;142(1):63–75. doi:10.1378/chest.11-3157
12. Ozekinci S, Mizrak B, Saruhan G, Senturk S. Histopathologic diagnosis of thyroid tuberculosis. Thyroid. 2009;19:983–986. doi:10.1089/thy.2009.0189
13. Sharma S, Girhotra M, Zafar N, Gupta R. Tuberculosis of the thyroid in a child: a rare cause of thyromegaly. APSP J Case Rep. 2016;7(1):5.
14. Goyal P, Mittal D, Ghosh S, et al. Cytological diagnosis of primary thyroid tuberculosis. JNMA. 2015;53(197):28–30.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.