Back to Journals » Journal of Asthma and Allergy » Volume 19
Thunderstorm-Associated Asthma in Shenzhen, China: A Retrospective Case-Control Study of Risk Factors, Clinical Characteristics, and Management Approaches
Authors Shang X, Yang Y, Deng W
Received 26 November 2025
Accepted for publication 17 March 2026
Published 1 April 2026 Volume 2026:19 584545
DOI https://doi.org/10.2147/JAA.S584545
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Xubin Shang, Yonggang Yang, Wangsheng Deng
Department of Emergency Medicine, People’s Hospital of Longhua, Shenzhen, Guangdong Province, 518109, People’s Republic of China
Correspondence: Wangsheng Deng, Department of Emergency Medicine, People’s Hospital of Longhua, NO. 38 Jinglong Construction Road, Shenzhen, Guangdong Province, 518109, People’s Republic of China, Tel +8615361681772, Email [email protected]
Objective: To identify risk factors, clinical characteristics, and management approaches associated with thunderstorm-associated asthma (TA) in Shenzhen, China, comparing it with general asthma (GA).
Methods: A retrospective case-control study was conducted, including 42 patients with TA who presented with asthma exacerbations following thunderstorms and 361 patients with GA. Demographic variables and inflammatory biomarkers, including absolute eosinophil count (AEC), absolute neutrophil count, and C-reactive protein were evaluated. Logistic regression and receiver operating characteristic analyses were applied to determine discriminative factors.
Results: Patients with TA were younger than those with GA (median 49 vs 57 years, p = 0.003) and demonstrated a higher prevalence of allergic rhinitis (73.8% vs 41.0%, p < 0.001). Eosinophil counts were significantly elevated among patients with TA (0.74× 109/L vs 0.42× 109/L, p < 0.001). An AEC ≥ 0.71× 109/L effectively differentiated TA from GA (area under the curve [AUC] = 0.843). The combined model incorporating age, allergic rhinitis history, and AEC yielded improved diagnostic performance (AUC = 0.880). Hospitalization rates were lower in the TA group (16.7% vs 68.4%, p = 0.041), although all individuals received oxygen therapy.
Conclusion: TA in Shenzhen affects younger atopic individuals with eosinophilic inflammation. AEC ≥ 0.71× 109/L may aid screening during meteorological alerts, guiding acute management with oxygen, bronchodilators, and corticosteroids while avoiding unnecessary antibiotics.
Keywords: absolute eosinophil count, allergic rhinitis, biomarker diagnosis, emergency management, eosinophilic inflammation, risk factors, retrospective case-control study, Shenzhen, thunderstorm asthma, united airway disease
Introduction
Asthma is a chronic inflammatory disorder of the airways that results from complex and incompletely elucidated interactions between genetic predisposition and environmental exposures.1,2 Thunderstorm asthma (TA) represents a phenotype of asthma precipitated by the concurrence of elevated aeroallergen concentrations, commonly pollen during late spring and early summer, and thunderstorm activity. In sensitized individuals, exposure to allergenic particles dispersed can precipitate acute bronchospasm within minutes. The initial asthmatic response is characterized by immunoglobulin E (IgE)-mediated mast cell degranulation, resulting in airway smooth muscle constriction, mucosal edema, and increased mucus secretion.3 This early response may be followed by sustained activation of T-helper type 2 (Th2) lymphocytes, upregulation of inflammatory cytokine signaling, and eosinophilic infiltration of the airway mucosa, thereby perpetuating airway inflammation and bronchial hyperresponsiveness.4 Although inhaled bronchodilator therapy was generally effective, hypoxia and respiratory failure can occasionally develop, and mortality, though rare, remains a possible outcome.5 TA affected not only individuals but also multiple persons located near the storm front, representing a significant and emerging global public health concern characterized by rapidly occurring epidemic asthma exacerbations.
The TA epidemic of 21 November 2016 in Melbourne, Australia, served as a sentinel event, revealing critical vulnerabilities within emergency healthcare systems. During this event, respiratory-related emergency department presentations increased by 672% within 30 hours (an estimated 3365 excess cases), resulting in ten fatalities and overwhelming critical care resources throughout Victoria.5 Pathophysiologically, TA is primarily mediated by eosinophilic airway inflammation, a defining feature of corticosteroid-responsive asthma, in which quantification of eosinophils serves as a key indicator for therapeutic guidance. Despite these insights, substantial gaps in understanding remain, particularly concerning region-specific risk profiles such as those in Asian populations, rapid diagnostic biomarkers for differentiating TA from general asthma (GA), and evidence-based strategies for acute management during meteorological surges. TA requires a critical alignment of factors: high concentrations of specific pollen, storm-driven meteorological forces, and a susceptible population. Melbourne exemplifies this risk: its temperate climate promotes intense seasonal grass pollen release, which coincides with spring and summer thunderstorms. These storms can rupture pollen grains into respirable allergenic particles, triggering population-wide outbreaks. Shenzhen, in contrast, presents a divergent profile. Its subtropical climate features different pollen types and seasonal patterns, with dominant aeroallergens being dust mites and mold spores. Crucially, Shenzhen’s peak thunderstorm season occurs in summer, largely dissociated from its primary pollen peaks. This temporal disconnect likely mitigates the risk of large-scale thunderstorm asthma events locally.
Eosinophils and the type 2 inflammatory response they mediate play a central role in asthma pathophysiology, particularly in the eosinophilic phenotype. By releasing cytotoxic proteins and pro-inflammatory cytokines, eosinophils contribute to airway hyperresponsiveness, mucus hypersecretion, and airway remodeling.6 Peripheral blood eosinophil count is a practical and reliable biomarker that supports phenotype identification and guides anti-inflammatory and biologic therapies, which have been shown to reduce exacerbations and improve disease control.7 These observations underscore the clinical importance of inflammatory heterogeneity in asthma. Despite growing recognition of asthma phenotypes, localized evidence on TA in Asia, especially in rapidly urbanizing subtropical regions, remains scarce. Most authoritative data originate from temperate countries, leaving uncertainty regarding how regional climate, aerobiology, and population susceptibility influence TA epidemiology in settings such as China. This knowledge gap increases the risk of misclassification in emergency settings, where TA may resemble general asthma exacerbations, and highlights the absence of locally validated early-warning systems and coordinated public health response strategies.
Methods
Study Design and Participants
A retrospective case-control study was conducted in the Emergency Department of the People’s Hospital of Longhua, Shenzhen, a regional tertiary care institution located in southeastern China. The study protocol was approved by the institutional Human Research Ethics Committee.
Case and Control Definitions
Case Group (TA)
The case group comprised adults aged 18 years or older residing in Shenzhen who presented to the emergency department with acute asthma exacerbations occurring within 10 hours following a documented thunderstorm event (20:00 April 30, 2024 to 08:00 May 1, 2024). This thunderstorm was a typical seasonal convective storm with heavy rainfall, characteristic of springtime weather in the region, and did not constitute a rare extreme meteorological disaster. Temporal case distribution peaked at 17 patients within 2 hours post-event, with 8 cases occurring in the first hour and subsequent gradual decline.
Control Group (GA)
The control group included consecutive adults aged 18 years or older who presented with asthma exacerbations to the same emergency department during the two-month observation period (April 1 to 29 and from May 2 to 31, 2024) without exposure to thunderstorm-related meteorological triggers.
Inclusion and Exclusion Criteria
Participants were eligible for inclusion if all of the following criteria were met: (1) a physician-confirmed diagnosis of asthma consistent with the Global Initiative for Asthma (GINA) 2019 guidelines;8 (2) adults (≥ 18 years old); (3) availability of a complete blood count (CBC) results; and (4) access to comprehensive electronic medical record data, including detailed treatment documentation.
The following exclusion criteria were applied to reduce potential confounding factors: (a) Individuals with non-allergic rhinitis (eg, vasomotor or infectious rhinitis) or other non-asthmatic chronic respiratory diseases (eg, COPD, bronchiectasis). (b) Those with symptoms of acute upper or lower respiratory infection (eg, fever, sore throat, cough, sputum, nasal congestion/rhinorrhea) within 4 weeks prior to the target thunderstorm event. This criterion aimed to exclude recent clinically evident infections, such as viral illnesses, as common triggers of asthma exacerbation. (c) Use of systemic corticosteroids within 1 week or long-term use of immunosuppressants/biologics. (d) History of significant exposure to occupational asthmagens. (e) Coexisting other systemic allergic diseases (eg, severe atopic dermatitis, allergic bronchopulmonary aspergillosis). (f) Pregnant or lactating women. (g) Inability to comply with follow-up or unavailability of key clinical data.
Oxygen Therapy Criteria
Upon arrival at the emergency department, all patients underwent peripheral oxygen saturation (SpO2) measurement using a pulse oximeter. Supplemental oxygen was administered to patients with severe asthma symptoms (eg, respiratory distress, use of accessory muscles, inability to speak full sentences) and/or SpO2 < 94% on room air. Oxygen was delivered via nasal cannula (1–4 L/min) for most patients, or via simple face mask for those with SpO2 < 92% or poor response to initial treatment. The detailed nebulization procedure is available in Supplementary Material 1.
Data Collection Methodology
Data were abstracted from the hospital’s electronic medical record system and included the following variables: (1) demographic characteristics and clinical history; (2) laboratory parameters, including absolute eosinophil count (AEC), absolute neutrophil count (ANC), and C-reactive protein (CRP) levels; (3) therapeutic interventions, such as antibiotics, oxygen therapy, short-acting β2-agonists (SABA), short-acting muscarinic antagonists (SAMA), inhaled corticosteroids, intravenous corticosteroids; (4) clinical outcomes, including hospitalization status, length of hospital stay, and chest computed tomography (CT) utilization; and (5) outpatient visit and inpatient records retrievable through the institution’s electronic medical record database. Binary variables, such as antibiotic use, were coded as dichotomous responses (yes/no).
Statistical Analysis
All statistical analyses were performed using R software (version 4.3.1; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables with a normal distribution were expressed as mean ± standard deviation (±s), and intergroup comparisons were conducted using the independent-samples t-test. Continuous variables that did not conform to a normal distribution were expressed as median with interquartile range [M (P25, P75)], and intergroup comparisons were performed using the Mann–Whitney U-test (rank-sum test). Categorical variables were presented as counts and percentages [(n) %], with comparisons between groups conducted using the chi-squared test or Fisher’s exact test, as appropriate.
Univariate and multivariate logistic regression analyses were performed to evaluate factors associated with TA. Receiver operating characteristic (ROC) curve analysis was used to assess the diagnostic performance of identified predictors. For modeling the association between inflammatory biomarkers (AEC, ANC, and CRP) and length of hospital stay, Poisson regression was employed when the assumption of equidispersion was satisfied; otherwise, a negative binomial regression analysis was used.
Results
The demographic and clinical characteristics of the study population are presented in Table 1. Comparison between the TA group (n = 42) and the GA group (n = 361) demonstrated that the patients in the TA group were younger (median age: 49 years vs 57 years, p = 0.003), with no statistically significant difference in sex distribution (p = 0.258). The proportion of patients with a documented history of asthma was significantly lower in the TA group than in the GA group (26.2% vs 58.4%, p < 0.001), whereas the prevalence of a history of allergic rhinitis was higher among patients with TA (73.8% vs 41.0%, p < 0.001).
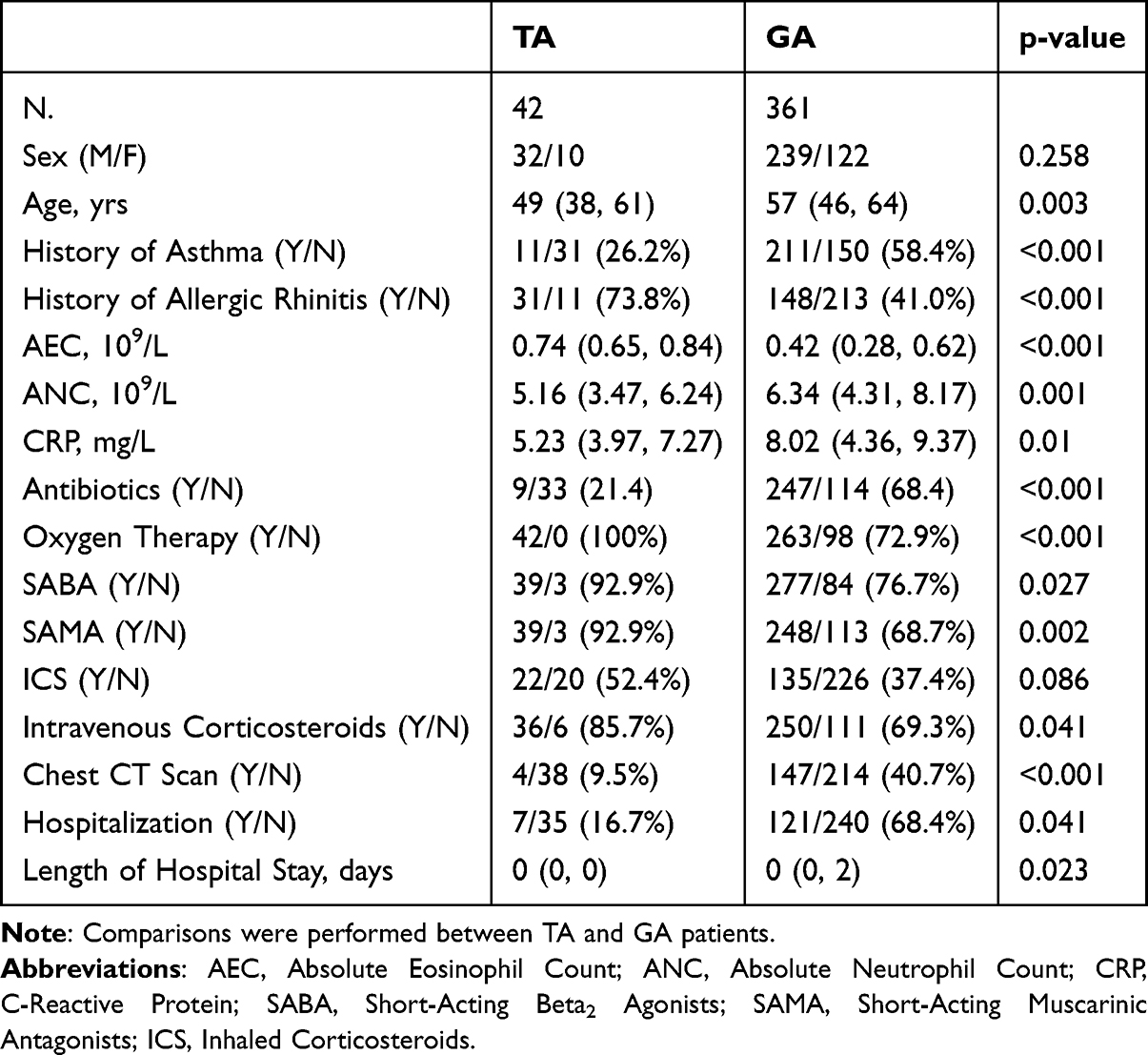 |
Table 1 Comparison of Demographics, Medical History, Treatment and Prognosis |
Laboratory analysis showed that the AEC level was elevated in the TA group compared with the GA group (0.74 × 109/L vs 0.42 × 109/L, p < 0.001), while the ANC (5.16 × 109/L vs 6.34 × 109/L, p = 0.001) and CRP levels (5.23 mg/L vs 8.02 mg/L, p = 0.01) were lower.
Regarding therapeutic interventions, the proportion of patients receiving antibiotic treatment was significantly lower in the TA group (21.4% vs 68.4%, p < 0.001). All TA patients received supplemental oxygen (100%), guided by SpO2 measurement and clinical assessment, whereas 72.9% of GA patients received oxygen (p < 0.001). The rates of chest CT utilization (9.5% vs 40.7%, p < 0.001) and hospitalization (16.7% vs 68.4%, p = 0.041) were also significantly lower in the TA group than in the GA group.
Multivariate logistic regression analysis demonstrated that age (odds ratio [OR] = 0.964; 95% CI: 0.94–0.987, p = 0.003), history of allergic rhinitis (OR = 4.056; 95% CI: 2.033–8.68, p < 0.001), and AEC level (OR = 379.054; 95% CI: 69.409–2588.544, p < 0.001) were independent predictors of TA (Table 2). Each additional year of age was associated with a 3.6% reduction in the likelihood of TA occurrence, whereas a history of allergic rhinitis and elevated AEC values increased the likelihood by approximately 4.06-fold and 379-fold, respectively.
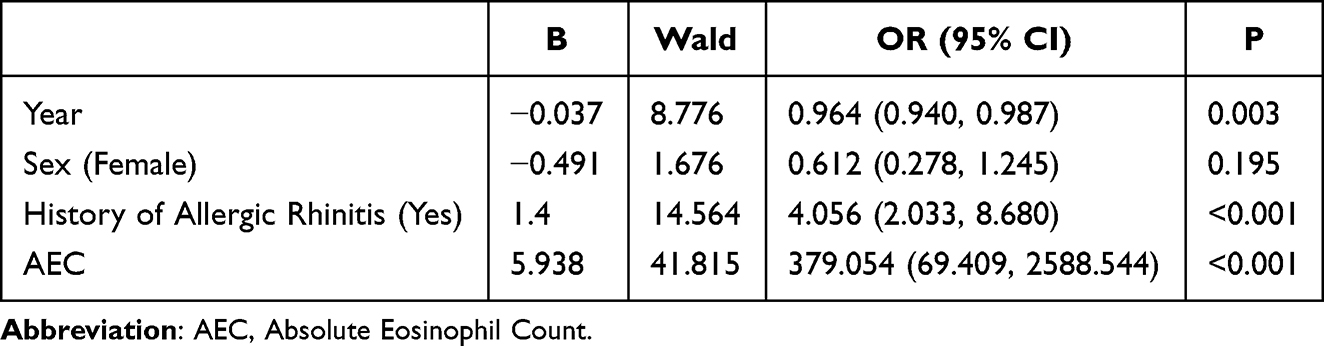 |
Table 2 Univariate Regression Analysis of TA Occurrence |
Regression analysis assessing hospitalization duration revealed that elevated ANC (rate ratio [RR] = 2.087; 95% CI: 1.225–3.557, p = 0.007) and higher CRP (RR = 1.110; 95% CI: 1.044–1.181, p = 0.001) were significantly associated with prolonged length of stay. Although AEC did not reach statistical significance (p = 0.134), a negative association trend was observed (RR = 0.008) (Table 3).
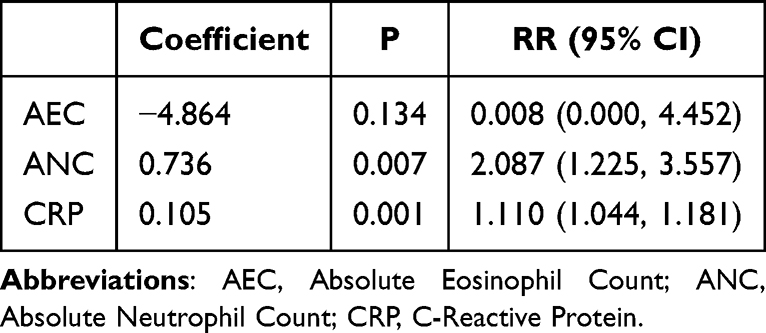 |
Table 3 Risk Factors Analysis for Prolonged Hospital Stay in TA Patients (Negative Binomial Regression) |
The ROC analysis demonstrated an area under the curve (AUC) of 0.843 for AEC. At the optimal cut-off value of 0.71×109/L, the sensitivity was 92.9% and the specificity was 66.2%, indicating that AEC had substantial value as a screening indicator for TA, although its specificity was relatively limited (Figure 1).
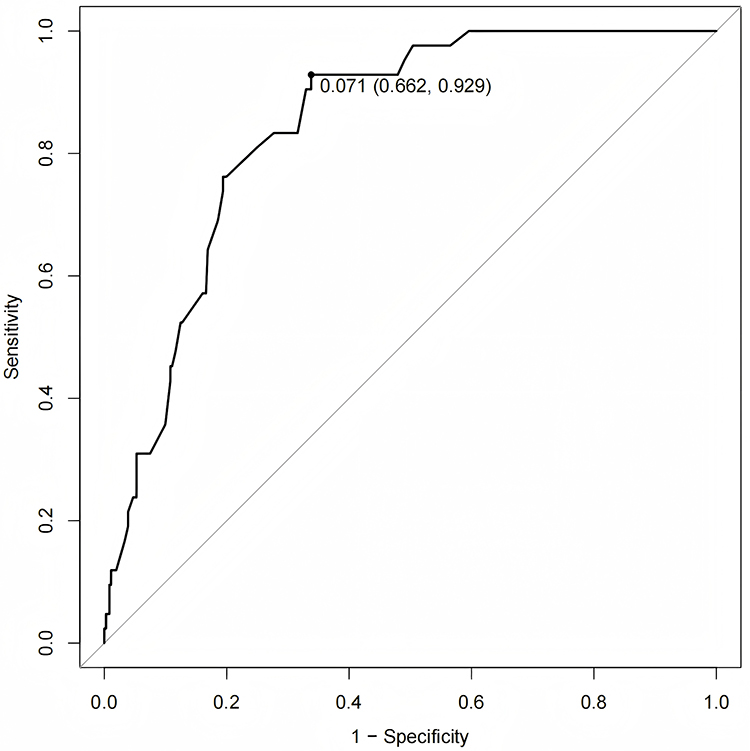 |
Figure 1 ROC curve of AEC for differentiating TA from GA. The area under the curve (AUC) was 0.843. At the optimal cutoff threshold of 0.71 (dashed vertical line), the test achieved a sensitivity of 92.9% and specificity of 66.2%. |
When multiple predictive variables were combined, the AUC increased to 0.880, representing a statistically significant improvement over the single-variable model (Figure 1). Using an optimal cut-off probability of 0.104, the combined model achieved a sensitivity of 85.7% and a specificity of 78.4%, demonstrating enhanced discriminative accuracy for differentiating TA from GA (Figure 2).
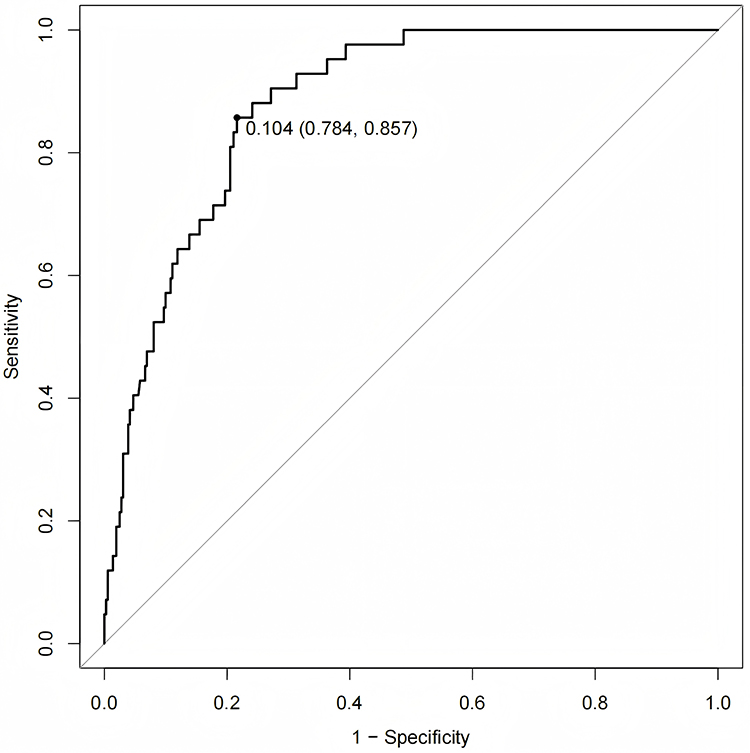 |
Figure 2 ROC curve of the multivariate model (age + history of allergic rhinitis +AEC). The area under the curve (AUC) was 0.880. At the optimal probability cutoff of 0.104 (dashed vertical line), the model achieved a sensitivity of 85.7% and specificity of 78.4%. |
Discussion
TA represents a distinct clinical phenomenon characterized by acute exacerbations of asthma triggered by the synergistic interaction between elevated pollen concentrations and thunderstorm activity. The ongoing effects of climate change have contributed to increased thunderstorm frequency and higher pollen production, thereby heightening the risk of severe TA episodes. These changes have also led to the expansion of TA beyond its traditional geographical and seasonal boundaries, with occurrences now reported in previously unaffected regions and during atypical periods.9,10
The present study characterized the demographic, inflammatory, and management characteristics of TA in Shenzhen, China, and compared them with those observed in GA. The results were consistent with international epidemiological findings while emphasizing regional variations that underscore the importance of localized public health interventions.
The largest documented TA outbreak occurred during the 2016 Melbourne epidemic, which remains a pivotal reference point in the global understanding of this phenomenon.5,11 Among the 1435 patients who presented to emergency departments and participated in a subsequent survey, the mean age was 32 years, 56% were male, and 28% had a physician-confirmed diagnosis of asthma. Notably, 87% of those affected were diagnosed with allergic rhinitis, a condition recognized as a major predisposing factor for TA. The findings from Shenzhen revealed notable differences compared to the seminal 2016 Melbourne thunderstorm asthma epidemic, underscoring how geographic and environmental contexts may shape TA presentation. Demographically, the Melbourne cohort was younger (mean age 32 years) with a male predominance (56%), whereas our TA patients were older (median 49 years) with no gender predominance, a discrepancy possibly due to our adult-only inclusion and distinct population exposure patterns in subtropical Shenzhen. A similarly low proportion of prior asthma diagnosis was observed in both settings (28% in Melbourne vs 26% here), reinforcing that TA often represents a first acute asthmatic event in atopic individuals. However, the prevalence of allergic rhinitis was higher in Melbourne (87%) than in our cohort (74%), which may reflect differences in local aerobiology, pollen sensitization profiles, or genetic susceptibility. Most strikingly, the scale of healthcare impact diverged substantially: the Melbourne event overwhelmed emergency services with a 672% surge in respiratory presentations and multiple fatalities, whereas our TA cases were largely managed without hospitalization (17%) or advanced imaging (10% chest CT rate), suggesting a milder collective severity and no systemic crisis. This contrast may be attributed to the smaller magnitude of the thunderstorm event, generally less severe clinical presentations, differences in emergency response protocols, or distinct bioclimatic interactions in a subtropical megacity. These findings highlight that while eosinophilic inflammation and allergic rhinitis remain central to TA pathophysiology globally, regional manifestations and healthcare burdens can vary significantly. Consequently, preparedness strategies and diagnostic frameworks must be adapted to local epidemiological patterns and healthcare realities in rapidly urbanizing subtropical regions.
The observed age disparity, where patients with TA exhibited a younger median age (49 years) compared with their GA counterparts (57 years), was consistent with patterns reported in previous investigations, such as the 2016 Melbourne epidemic. The comparatively older age distribution observed in the Shenzhen cohort may be attributable to the exclusion of pediatric populations from the present analysis. Another possible explanation is that patients with milder TA symptoms, particularly younger adults, may not have sought medical attention.
The upper and lower airways are recognized as a unified anatomical and functional system, with substantial evidence supporting asthma and allergic rhinitis as interrelated manifestations of a single inflammatory disorder commonly referred to as “united airway disease”.12,13 In the current cohort, 73.8% of patients with TA had allergic rhinitis, whereas only 26.2% had a prior diagnosis of asthma. This pattern suggests that TA frequently represents the initial manifestation of asthma among atopic individuals, underscoring allergic rhinitis as a critical predisposing factor. These findings reinforce the united airway disease paradigm, highlighting the interplay between upper and lower airway inflammation.
Previous studies have demonstrated that a prior asthma diagnosis is not a consistent characteristic of TA, with approximately 36–56% of affected patients lacking a definitive asthma history. However, the most of these individuals exhibited clinical features consistent with hay fever, indicative of sensitization to pollen or fungal spores.5 In contrast, individuals with established asthma are at greater risk of experiencing severe or life-threatening TA episodes.14
From a clinical perspective, these observations emphasize the importance of integrated management strategies for allergic rhinitis and asthma to mitigate TA susceptibility, particularly in regions experiencing increased thunderstorm frequency. Optimizing asthma control through appropriate pharmacologic interventions is a key preventive measure for reducing the risk of TA-related exacerbations.15
Multiple factors have been associated with increased susceptibility to TA at both the individual and population levels. Among these, a history of allergic rhinitis appears to represent the most significant individual risk factor, reflecting clinical evidence of sensitization to environmental aeroallergens. Data from previously reported TA outbreaks indicate that more than 90% of affected patients exhibited allergic rhinitis and/or positive skin prick test results, a prevalence substantially higher than that observed in the general population.4 Furthermore, the age distribution of patients affected by TA typically falls within the 20–50 year range, closely paralleling the epidemiological profile of allergic rhinitis.16
The strong association between allergic rhinitis and TA (OR = 4.06) reinforces the “united airway disease” paradigm, emphasizing the need for integrated upper/lower airway management. Notably, the clinical presentation of rhinitis in TA may not always align with classic systemic atopy. The emerging concept of local allergic rhinitis, characterized by a localized nasal allergic response in the absence of systemic IgE sensitization, offers a plausible framework for understanding some of these cases.17 It is conceivable that a subset of TA patients with prominent upper airway symptoms, but negative conventional allergy testing may have underlain local allergic rhinitis, where the thunderstorm event triggers a localized inflammatory cascade. This hypothesis warrants further investigation, as it could refine risk stratification and personalize prophylactic measures for susceptible individuals. Comprehensive therapeutic strategies encompassing pharmacologic treatment of allergic rhinitis and asthma, along with allergen immunotherapy, constitute key components of primary and secondary prevention efforts aimed at reducing individual susceptibility to TA. The development of individualized treatment plans addressing both airway components is therefore recommended. However, current evidence does not support the efficacy of intranasal corticosteroid therapy for allergic rhinitis in preventing TA onset.18
Characterization of the inflammatory phenotype of asthma is essential not only for accurate diagnosis but also for assessing clinical severity and disease burden, risk of exacerbation, bronchial hyper-reactivity, and airway remodeling.19 Peripheral blood eosinophil count has been shown to correlate with eosinophil levels in bronchoalveolar lavage fluid and serves as a reliable biomarker for predicting response to conventional anti-inflammatory treatment, including inhaled and systemic corticosteroids. Although a universally accepted threshold for eosinophilic asthma has not been established, clinical trials have generally employed peripheral blood eosinophil counts of ≥ 150 cells/µL, ≥ 300 cells/µL, or ≥ 400 cells/µL to define eosinophilic phenotypes.20–22
The pronounced elevation in AEC observed in TA compared with GA (0.74 ×109/L vs 0.42 × 109/L, respectively) supports eosinophilic inflammation as a key pathophysiological mechanism in TA and underscores its potential diagnostic value. ROC analysis showed strong discriminative performance for AEC alone (AUC = 0.843) and further enhancement in the combined model incorporating age, allergic rhinitis history, and AEC (AUC = 0.880). An AEC threshold of ≥ 0.71×109/L effectively discriminated between TA and GA. However, the moderate specificity (66.2%) indicates that additional biomarkers, such as IgE and IL-5, or clinical parameters, including temporal proximity to thunderstorm exposure, may be required to achieve a more definitive diagnosis. The improved diagnostic performance of the combined model (sensitivity 85.7%, specificity 78.4%) supports the implementation of a multimodal diagnostic framework, particularly in emergency department settings with limited resources. While our findings highlight the diagnostic utility of AEC, with a cutoff of ≥ 0.71×109/L showing high sensitivity for distinguishing TA from GA, it is important to frame this as a promising screening tool rather than a definitive diagnostic criterion. The proposed threshold and its associated clinical management implications, such as prioritising oxygen, systemic corticosteroids, and avoiding unnecessary antibiotics, derive from a retrospective, single-center study. Therefore, these recommendations should be validated in larger, prospective, multicentre cohorts before being widely integrated into routine clinical pathways. Such studies would further clarify the precision of this biomarker in diverse populations and settings, ensuring its reliability for guiding real-time emergency decisions during thunderstorm alerts.
Treatment patterns in TA highlighted its acute yet transient clinical profile. The markedly lower hospitalization rate (16.7% vs 68.4%) and reduced CT utilization (9.5% vs 40.7%) in the TA cohort suggested fewer structural pulmonary complications compared with GA. However, the universal administration of oxygen therapy among patients with TA (100% vs 72.9% in GA) reflected compliance with established acute management protocols. The lower frequency of antibiotic administration (21.4% vs 68.4%) was consistent with TA’s non-infectious etiology. The higher use of SABA, SAMA, and corticosteroids in TA likely reflected standardized emergency management strategies aimed at achieving rapid bronchodilation and effective inflammation control during high-demand respiratory surge events.
Limitations
This study has several notable limitations. First, its single-center design may have limited the generalizability of the findings to populations in regions with distinct climatic conditions or environmental exposures, or healthcare system capacities. Second, the retrospective study design introduced a potential risk of documentation bias, as patients with mild TA who did not seek medical attention may not have been captured in the electronic health records. Third, we lacked systematic virological screening data, such as polymerase chain reaction testing of nasopharyngeal swabs. Although individuals with clinically apparent respiratory infections within four weeks before the thunderstorm event were excluded, asymptomatic or mild, unreported viral infections could not be ruled out. Given that respiratory viral infections are well-established triggers of asthma exacerbations and may seasonally coincide with periods of elevated pollen levels and thunderstorm activity, residual confounding from unrecognized viral infections may have led to an overestimation of the observed association between thunderstorm exposure and asthma onset. Additionally, the control cohort was restricted to the period between April and May 2024, which may have obscured potential seasonal variations in GA presentation during other months. Moreover, the absence of environmental and behavioral variables such as contemporaneous pollen concentrations, air quality metrics, and adherence to preventive pharmacotherapies constituted unmeasured confounders that could have influenced respiratory outcomes and the observed associations. Lastly, all participants in this study were recruited from the population of Shenzhen, China, and thus were exclusively of Asian ethnicity. This homogeneity limits the generalizability of our findings regarding risk profiles, biomarker thresholds, and clinical management implications to other racial or ethnic groups. Consequently, our results should be interpreted as primarily applicable to populations with similar genetic backgrounds and environmental exposures. Future multi-center studies including diverse populations are necessary to validate and refine these observations across different demographic and geographic settings.
Conclusion
Our study provides key observations: a significant proportion of TA patients presented with elevated AEC (median 0.74×109/L), and a threshold of ≥ 0.71×109/L demonstrated high sensitivity (92.9%) for differentiating TA from GA in our cohort. Management patterns were also observed: TA cases universally received oxygen therapy, had higher rates of systemic corticosteroid use, and lower rates of antibiotic administration and hospitalization compared to GA. Based on these observations, we infer that AEC may serve as a practical screening indicator in emergency settings during thunderstorm alerts, and that acute management might be optimized by emphasizing oxygen and systemic corticosteroids while de-escalating antibiotics. However, these interpretations and the derived clinical and public health implications, including the precise cutoff value and the generalizability of the management pattern, require validation in larger, prospective, multicenter studies. Future research should prioritize multicenter studies across diverse geographical and climatic zones to validate and generalize our findings beyond the subtropical context of Shenzhen. Prospective studies integrating real-time aerobiological and meteorological data are needed to establish causality and refine predictive models. Finally, the mechanisms underlying the upper-lower airway link in TA, including the role of local allergic responses, warrant further exploration to advance personalized prevention.
Abbreviations
AEC, absolute eosinophil count; ANC, Absolute Neutrophil Count; AUC, The area under the curve; CRP, C-Reactive Protein; CBC, complete blood count; GINA, Global Initiative for Asthma; ED, emergency department; TA, thunderstorm-associated asthma; GA, general asthma; SABA, short-acting β2-agonists; SAMA, short-acting muscarinic antagonists; ICS, Inhaled Corticosteroids; ROC, receiver operating characteristic.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The retrospective study was approved by ethics committee of the People’s Hospital of Longhua (No. 2025078). This study was conducted in accordance with the declaration of Helsinki. Informed consent was waived due to the retrospective nature of the study, which involved the analysis of existing clinical data with no direct patient contact or intervention.
Acknowledgments
We thank the staff for their dedicated work in implementing the study’s intervention and evaluation.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Popović-Grle S, Štajduhar A, Lampalo M, Rnjak D. Biomarkers in different asthma phenotypes. Genes. 2021;12(6):801. doi:10.3390/genes12060801
2. Mao YZ, Li CZ, Bu WQ, et al. Pudilan Anti-inflammatory oral liquid and organic acid component from taraxaci herba attenuate allergic asthma in young mice through toll-like receptor 2/toll-like receptor 4 signaling pathway. World J Tradit Chin Med. 2024;10(3):294–11. doi:10.4103/wjtcm.wjtcm_64_24
3. Cockcroft DW, Davis BE, Blais CM. Thunderstorm asthma: an allergen-induced early asthmatic response. Ann Allergy Asthma Immunol. 2018;120(2):120–123. doi:10.1016/j.anai.2017.12.002
4. Harun N, Lachapelle P, Douglass J. Thunderstorm-triggered asthma: what we know so far. J Asthma Allergy. 2019;12:101–108. doi:10.2147/JAA.S175155
5. Thien F, Beggs PJ, Csutoros D, et al. The Melbourne epidemic thunderstorm asthma event 2016: an investigation of environmental triggers, effect on health services, and patient risk factors. Lancet Planet Health. 2018;2(6):e255–e263. doi:10.1016/S2542-5196(18)30120-7
6. McBrien CN, Menzies-Gow A. The biology of eosinophils and their role in asthma. Front Med. 2017;4:93. doi:10.3389/fmed.2017.00093
7. Schleich FN, Manise M, Sele J, et al. Distribution of sputum cellular phenotype in a large asthma cohort: predicting factors for eosinophilic vs neutrophilic inflammation. BMC Pulm Med. 2013;13(1):11. doi:10.1186/1471-2466-13-11
8. Reddel HK, FitzGerald JM, Bateman ED; Global Initiative for Asthma (GINA). GINA 2019: a fundamental change in asthma management: treatment of asthma with short-acting bronchodilators alone is no longer recommended for adults and adolescents. Eur Respir J. 2019;53(6):1901046. doi:10.1183/13993003.01046-2019
9. D’Amato G, Vitale C, Lanza M, Molino A, D’Amato M. Climate change, air pollution, and allergic respiratory diseases: an update. Curr Opin Allergy Clin Immunol. 2016;16(5):434–440. doi:10.1097/ACI.0000000000000301
10. Allen JT. Climate change and severe thunderstorms. In: Oxford Research Encyclopedia of Climate Science. Oxford University Press; 2018.
11. Lee J, Kronborg C, O’Hehir RE, et al. Who’s at risk of thunderstorm asthma? The ryegrass pollen trifecta and lessons learnt from the Melbourne thunderstorm epidemic. Respir Med. 2017;132:146–148. doi:10.1016/j.rmed.2017.10.012
12. Bousquet J, Bedbrook A, Czarlewski W, et al. Guidance to 2018 good practice: ARIA digitally-enabled, integrated, person-centred care for rhinitis and asthma. Clin Transl Allergy. 2019;9(1):16. doi:10.1186/s13601-019-0252-0
13. Bousquet J, Schunemann HJ, Togias A, et al. Next-generation Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines for allergic rhinitis based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and real-world evidence. J Allergy Clin Immunol. 2020;145(1):70–80.e3. doi:10.1016/j.jaci.2019.06.049
14. Queensland University of Technology. Literature Review on Thunderstorm Asthma and Its Implications for Public Health Advice. Department of Health and Human Services; 2017.
15. Silver JD, Sutherland MF, Johnston FH, et al. Seasonal asthma in Melbourne, Australia, and some observations on the occurrence of thunderstorm asthma and its predictability. PLoS One. 2018;13(4):e0194929. doi:10.1371/journal.pone.0194929
16. Australian Institute of Health and Welfare. Allergic rhinitis (Vol. 25); 2019. Avaiable from: https://www.aihw.gov.au/reports/chronic-respiratory-conditions/allergic-rhinitishay-fever/contents/allergic-rhinitis.
17. Berghi O, Dumitru M, Cergan R, et al. Local allergic rhinitis—a challenge for allergology and otorhinolaryngology cooperation (scoping review). Life. 2024;14(8):965. doi:10.3390/life14080965
18. National Asthma Council Australia. Thunderstorm asthma. National Asthma Council Australia; 2022. Avaiable from: https://www.nationalasthma.org.au/.
19. Saglani S, Lloyd CM. Novel concepts in airway inflammation and remodelling in asthma. Eur Respir J. 2015;46(6):1796–1804. doi:10.1183/13993003.01196-2014
20. Levy ML, Bacharier LB, Bateman E, et al. Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Primary Care Respir Med. 2023;33(1):7. doi:10.1038/s41533-023-00330-1
21. Skolnik NS, Carnahan SP. Primary care of asthma: new options for severe eosinophilic asthma. Curr Med Res Opin. 2019;35(7):1309–1318. doi:10.1080/03007995.2019.1595966
22. Corren J, Du E, Gubbi A, Vanlandingham R. Variability in blood eosinophil counts in patients with eosinophilic asthma. J Allergy Clin Immunol. 2021;9(3):1224–1231.e9.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.