Back to Journals » Journal of Blood Medicine » Volume 15
Thrombotic Risk Assessment, P-Selectin, and Thromboprophylaxis Use Among, Cancer Patients at the University of Calabar Teaching Hospital, Calabar
Authors Akaba K ![]() , Akaba E, Oshatuyi O
, Akaba E, Oshatuyi O ![]() , Ssenkumba B
, Ssenkumba B ![]()
Received 14 May 2024
Accepted for publication 11 December 2024
Published 14 December 2024 Volume 2024:15 Pages 501—512
DOI https://doi.org/10.2147/JBM.S478192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Kingsley Akaba,1 Edakabasi Akaba,2 Olukayode Oshatuyi,2 Brian Ssenkumba3
1Department of Haematology, University of Calabar, Calabar, Cross River State, Nigeria; 2Department of Pathology, University of Calabar Teaching Hospital, Calabar, Cross River State, Nigeria; 3Department of Pathology, Kampala International University Western Campus, Ishaka, Uganda
Correspondence: Kingsley Akaba, Department of Haematology, University of Calabar, Calabar, Cross-River State, Nigeria, Email [email protected]
Background: Venous thromboembolism is the second leading cause of mortality among cancer patients. The Khorana Risk Assessment Score (KRAS) is widely acknowledged as the most validated tool in this context.
Aim: To assess the thrombotic risk in cancer patients using the modified Khorana Risk Assessment Score, examine the association between modified KRAS and soluble P-selectin levels, and document the utilization of thromboprophylaxis among cancer patients at the University of Calabar Teaching Hospital.
Methods: This was a cross-sectional hospital-based recruiting 100 cancer patients. Seven millilitres of blood were collected for complete blood count and P-selectin assay. Continuous variables were expressed as mean and standard deviation, while categorical variables were summarized using frequencies. Chi-square was employed to compare VTE risk status across genders, different cancer types, and guideline compliance. The significance level was set at 0.05.
Results: Participants age ranged from 19 to 87 years, with a male-to-female ratio of 1:1.6. The most common female cancer was Breast at 40.32% and prostate cancer at 65.79% was the most common in males. Seventy nine percent and 21% of participants had intermediate and high-risk modified KRAS scores respectively. The median level of soluble P-selectin among cancer patients was 23.00 within the interquartile range. Significant associations were observed between cancer types and sex, VTE risk assessment and cancer types, and cancer types and risk score.
Conclusion: The risk of VTE among cancer patients ranges from intermediate to high, going by the modified Khorana risk score irrespective of the P selectin level, with underutilization of thromboprophylaxis. There is little adherence to the Khorana score in our setting, hence the need for greater application and knowledge of this predictive score in clinical practice to improve outcomes and quality of life.
Keywords: thrombosis, cancer, P-selectin
Introduction
The incidence of cancer is rising significantly with a global estimate of 18.1 million and 9.6 million deaths. Over 600,000 deaths occur annually in Africa.1 It was estimated that by the end of 2020, the incidence of cancer in Africa will rise to about 15 million.2 The prevalence of cancer in Nigeria is estimated at 211,052 with about 70,327 deaths and 115,950 new cases.1 In Cross River State, Ebughe et al reported a total of 941 cancer patients at the University of Calabar in a ten years study.3 Venous thromboembolism (VTE) which is comprised of pulmonary embolism (PE) and deep vein thrombosis (DVT), is one of the leading causes of mortality among cancer patients. The prognostic implications of VTE in cancer have been studied in different types of cancer.4–7 Available data suggests that VTE in malignancies is associated with tumour aggressiveness and can adversely impact the survival of patients.5,8 Cancer is known as a hypercoagulable and prothrombotic disease associated with significant alteration of the haemostatic system. This is due to the release of tissue factor and procoagulant molecules by the neoplasm.5 There is also increased expression of activated factor X, increased expression of TF, plasminogen activator inhibitor-1 (PAI- 1), urokinase plasminogen, and tissue-type plasminogen activator with prothrombotic potential. Cancer cells secrete a lot of cytokines TNF-α and IL-1β, which causes expression of TF and down-regulates thrombomodulin predisposes to hypercoagulability and risk of VTE.4–7 Other reported mechanisms for hypercoagulability include angiogenesis, the mechanical effect exerted by the tumours, and increased endothelial cell activation among others.9 Besides cancer, other VTE-associated risk factors include surgery, trauma, hospitalization, cancer with or without chemotherapy, and also the use of central nervous catheters. Risk assessment models (RAM) such as the Khorana score can be used to predict the risk of VTE in cancer patients. The Khorana Risk Score (KRS) is a tool that was introduced in 2008 and was designed to predict the risk of VTE in cancer patients based on the type of cancer, body mass index, and haematological parameters of the patient. It stratifies patients into no risk, low and high risk of VTE, and therefore forms the basis for recommending the use of anticoagulants (either thromboprophylaxis or antithrombotic therapy). KRS score is endorsed by the American Society of Clinical Oncology (ASCO), the International Society for Thrombosis and Haemostasis (ISTH), and the National Comprehensive Cancer Network (NCCN). KRS assigns points to five clinical and pre-chemotherapy laboratory parameters. The parameters include; primary tumour site, platelet count, haemoglobin concentration, or use of erythropoiesis-stimulating agents, leukocytes count, and body mass index. Patients with a KRS of greater than 3 are considered at high risk for developing blood clots and may benefit from prophylactic anticoagulation. In addition to the use of risk assessment models, the use of biomarkers has been suggested to increase the sensitivity of predicting VTE in at-risk patient groups10 One such molecule is P-selectin. P-selectin is a transmembrane protein present in the α granules of platelets and the Weibel-Palade bodies of endothelial cells, during activation, it is rapidly translocated to the cell surface. P-selectin mediates the rolling of platelets and leukocytes on activated endothelial cells as well as interactions of platelets with leukocytes11 The aim of this study is to assess the risk pattern of VTE, practice of thromboprophylaxis and correlate the level of P-selectin as a biomarker for thrombosis and VTE risk score using KRS among cancer patients.
Methods
Study Area
The study was carried out in Cross River State specifically at the University of Calabar Teaching Hospital (UCTH). UCTH is a Federal Government-owned tertiary institution, situated in Calabar Municipality LGA, Calabar, and Cross River State. The facility receives referrals from neighbouring states such as Akwa Ibom, Bayelsa, Ebonyi, and Rivers States.
Study Design
This was a cross-sectional study. This was deemed appropriate for this research because it was an observational study involving cancer patients seen at the University of Calabar Teaching Hospital and clinicians who manage cancer patients. The vegetation ranges from mangrove swamps, through rainforest, to derived savannah, and montane parkland.
Study Population
This study involved all cancer patients seen at the University of Calabar Teaching Hospital and clinicians who manage cancer patients.
Inclusion Criteria
The study population consisted of
- Adult cancer patients (≥18 years) receiving care at the University of Calabar Teaching Hospital who met the study inclusion criteria;
- Primary or relapsing cancer patients;
- Planned initiation of cancer therapy (chemotherapy, hormone therapy, molecular targeted therapy, immunotherapy, radiation therapy, or surgery); or
- Planned first-line therapy for patients with relapsed cancer; provision of informed consent.
Exclusion Criteria
- Patients with only intramucosal cancer,
- Brain cancer,
- Bleeding disorders, other
- Contrary indication for thromboprophylaxis, and
- Those judged as inappropriate for inclusion or difficult to follow up by the investigators were excluded.
Sample Size Estimation
The sample size of 100 after factoring in 10% attrition was calculated using the Kish Leslie formula with a reference proportion of 6.4% from a study by Ay (Ay et al, 2008)
Sampling Technique
The researchers employed a purposive sampling technique, a non-probability sampling method used when the researcher aims to study a specific group of individuals or phenomena based on their unique characteristics and relevance to the research. Target patients with histological evidence of cancer were recruited from various clinics (Surgical, Medical, and Haematology Clinics) involved in the care of cancer patients.
Study Tools
A workshop on thrombotic risk assessment was carried out in all the clinical units involved in the management of cancer patients to educate them on the guidelines for thrombotic risk assessment in cancer patients and how to use the Khorana Risk Score. The patient information leaflet was also designed to educate cancer patients on their risk of thrombosis and the benefits of thromboprophylaxis. Recruited subjects were evaluated for thrombotic risk using the Khorana risk scoring tool (Table 1) and a blood sample collected for evaluation of p selectin levels.
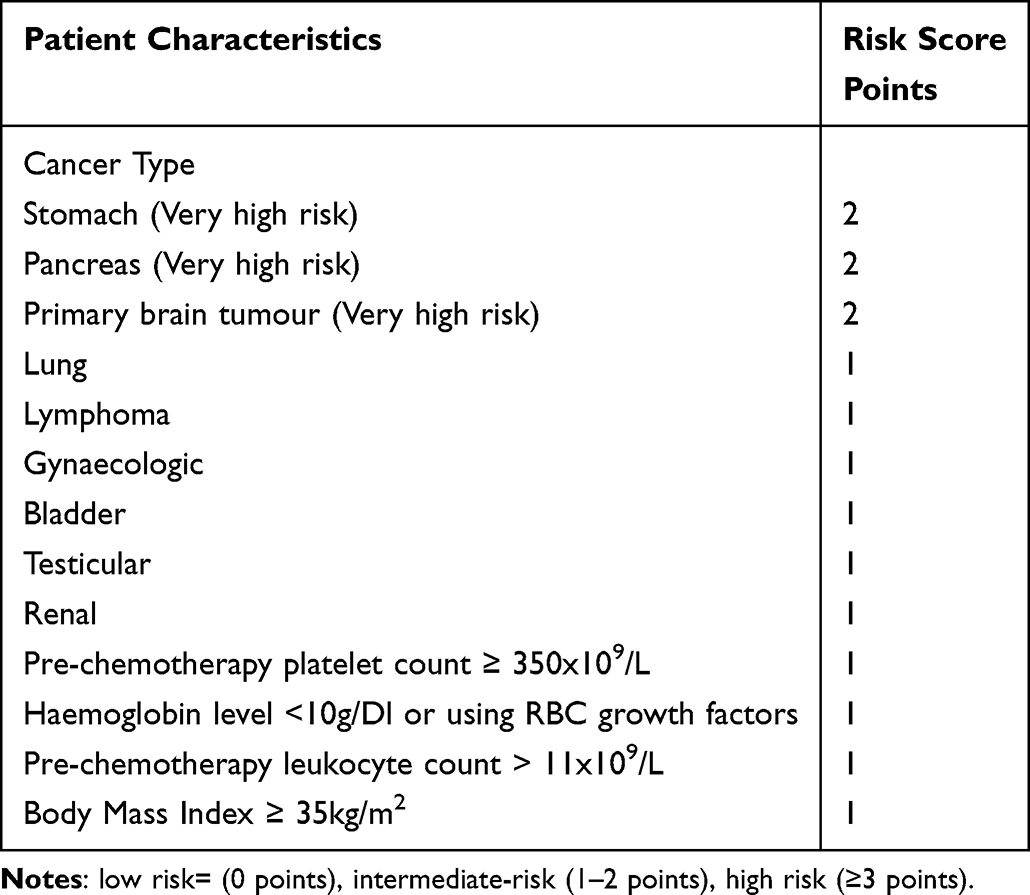 |
Table 1 Khorana Risk Scoring Model Table |
Pre-Testing
Basic Haematological Parameters involved using full blood count which includes haematocrit, haemoglobin concentration, and total white cell and platelet counts were obtained from the EDTA sample, using an automated blood cell counter (Sysmex Haematology Auto- analyser model KN21, Texas, USA). The basic principles underlying this technique are electronic impedance and light scattering. This was done in the main Haematology Laboratory, UCTH. In the P-selectin assay, the samples of patients with suspected DVT were screened further using the P-selectin assay. An immunological assay based on an enzyme-linked immunoassay was used.
Statistical Analysis
The data was collected and analyzed using the Statistical Package for Social Sciences version 26. Data of continuous variables were expressed as mean, standard deviation and categorical variables will be summarized using frequencies. Chi-square was used to compare VTE risk status between males and females, across different cancer types, and between those who complied with guidelines. P-value was set at ≤ 0.05.
Ethical Approval
The study obtained ethical clearance from the University of Calabar Teaching Hospital, Nigeria under number HREC 41285 and all participants provided informed consent. The study complies with the Declaration of Helsinki.
Results
Description of Sociodemographic Characteristics
The sample population consisted of 100 subjects, spanning various age groups. The largest age group, comprising 44% of the subjects, was individuals aged 40–59, followed by those aged 60–79 (30%). Participants aged 20–39 made up 21%, while those aged 0–19 and 80+ represented 1% and 4%, respectively.
For gender distribution, females constituted 62% of the sample, with males making up 38%. Most participants were married (73%), with single individuals accounting for 21%. A smaller proportion were widowed (5%) or separated (1%).
Educational backgrounds varied, with the largest segment having completed secondary education (39%), followed by those with tertiary education (37%). Primary education holders accounted for 15%, and 9% were uneducated.
The majority of participants (72%) had experienced their illness for 0–2 years, while 22% had been ill for 3–5 years. Only 6% had a duration of illness exceeding five years. A comprehensive overview of the socio-demographic characteristics of the patients is provided in Table 2.
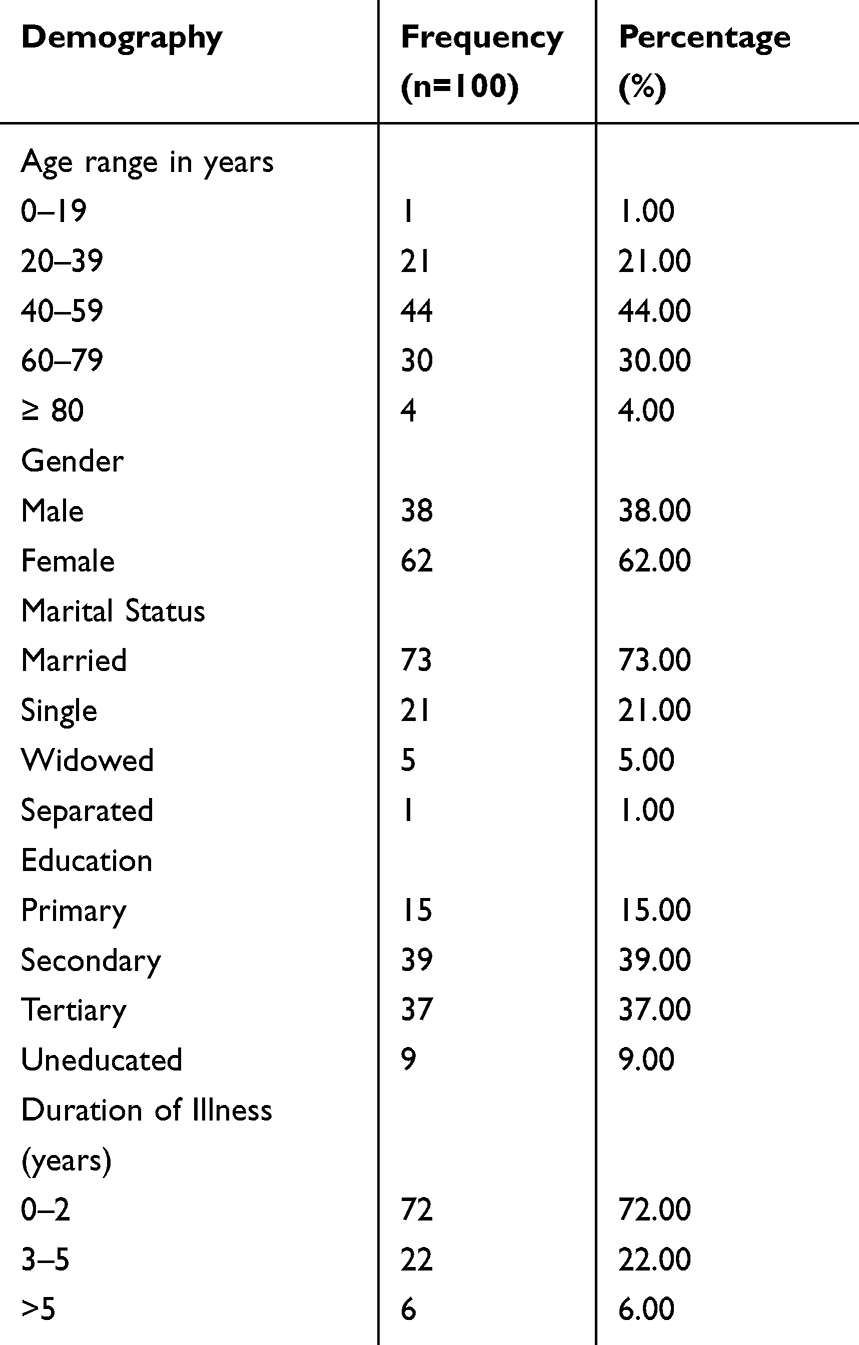 |
Table 2 Demographic Characteristics |
Cancer Types
Figure 1 displays the distribution of cancer types among the participants. The most prevalent types were breast and prostate cancers, each with 25 cases, accounting for 25% of the total. Ovarian cancer followed, with 13 cases (13%), and lymphoma, with 12 cases (12%). Leukemia was found in 6 cases (6%), while cervical cancer appeared in 3 cases (3%) and vulvar cancer in another 3 cases (3%). Bladder, endometrial, lung, Meigs syndrome, and pancreatic cancers each had 2 cases (2%). Less frequent types, each representing 1% of the sample, included gastric cancer, glioblastoma, and osteosarcoma.
 |
Figure 1 Different Cancers of the subjects. |
Year of Diagnosis
Figure 2 details the distribution of cancer diagnoses by year. Diagnoses were minimal from 2007 to 2016, with just one case per year (1% each). Diagnoses began to rise in 2017 and 2018, with five (5%) and seven cases (7%), respectively. This trend continued in 2019 (5%) and 2020 (8%). The number of diagnoses peaked in 2021, with 13 cases (13%), and surged in 2022, when 59 cases were recorded, accounting for 59% of the total sample.
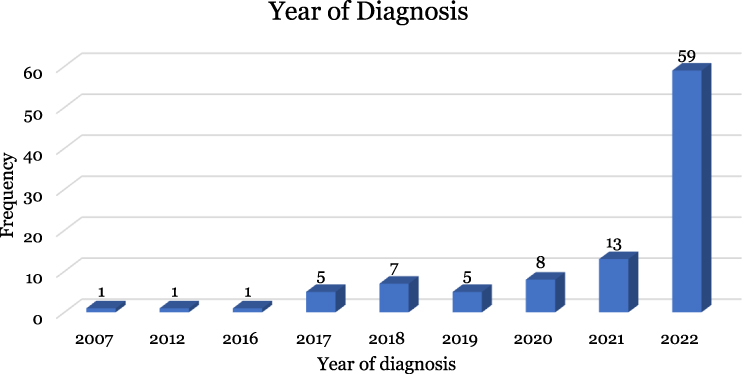 |
Figure 2 Years of Disease Diagnosis. |
Treatment Plan
Table 3 summarizes the treatment modalities used within the sample population. Chemotherapy was administered to 28% of participants, while 72% did not receive it. Surgery was performed on 45% of the sample, with 55% not undergoing surgery. Radiation therapy was utilized by 49% of participants, while 51% did not receive it. Only 4% of the sample received anticoagulant prophylaxis, with the remaining 96% not receiving this treatment option.
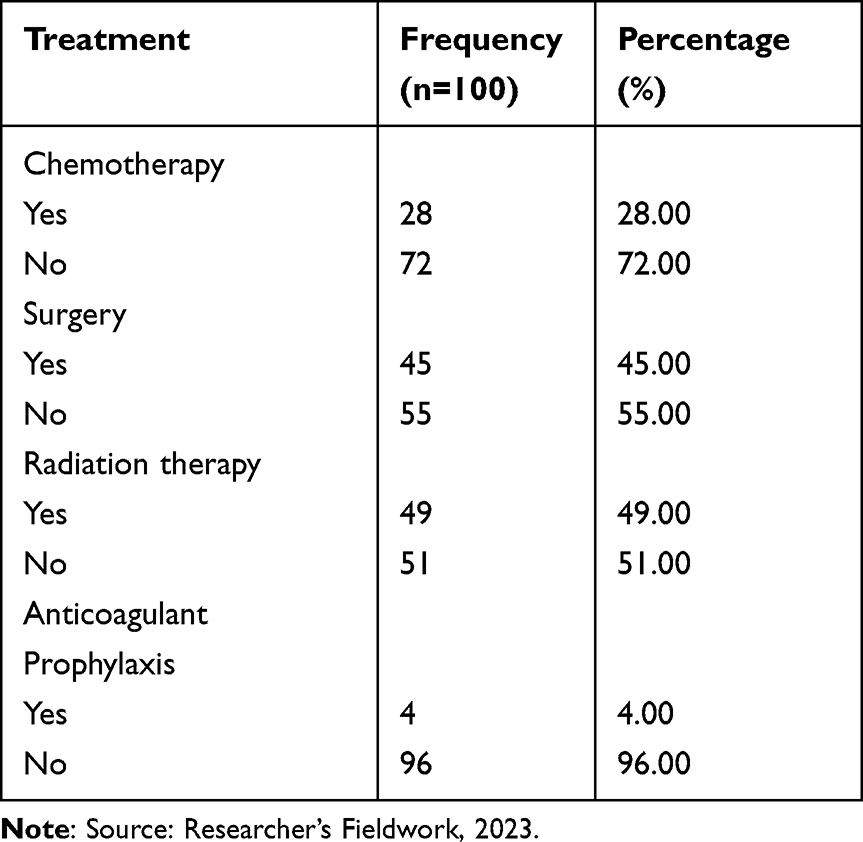 |
Table 3 Treatment Plan |
Association Between Type of Cancer and Sex Distribution
As shown in Table 4; among males, prostate cancer was the most common, comprising 65.79% of male cases, followed by lymphoma (13.16%) and smaller percentages of leukaemia, bladder, gastric, glioblastoma, and lung cancers. In females, breast cancer had the highest frequency at 40.32%, with ovarian cancer at 24.19%, followed by lymphoma, cervical cancer, and leukaemia. A Chi-square test showed a significant association between gender and cancer type (X² = 79.131, p < 0.001), indicating gender-specific cancer distribution (Table 4).
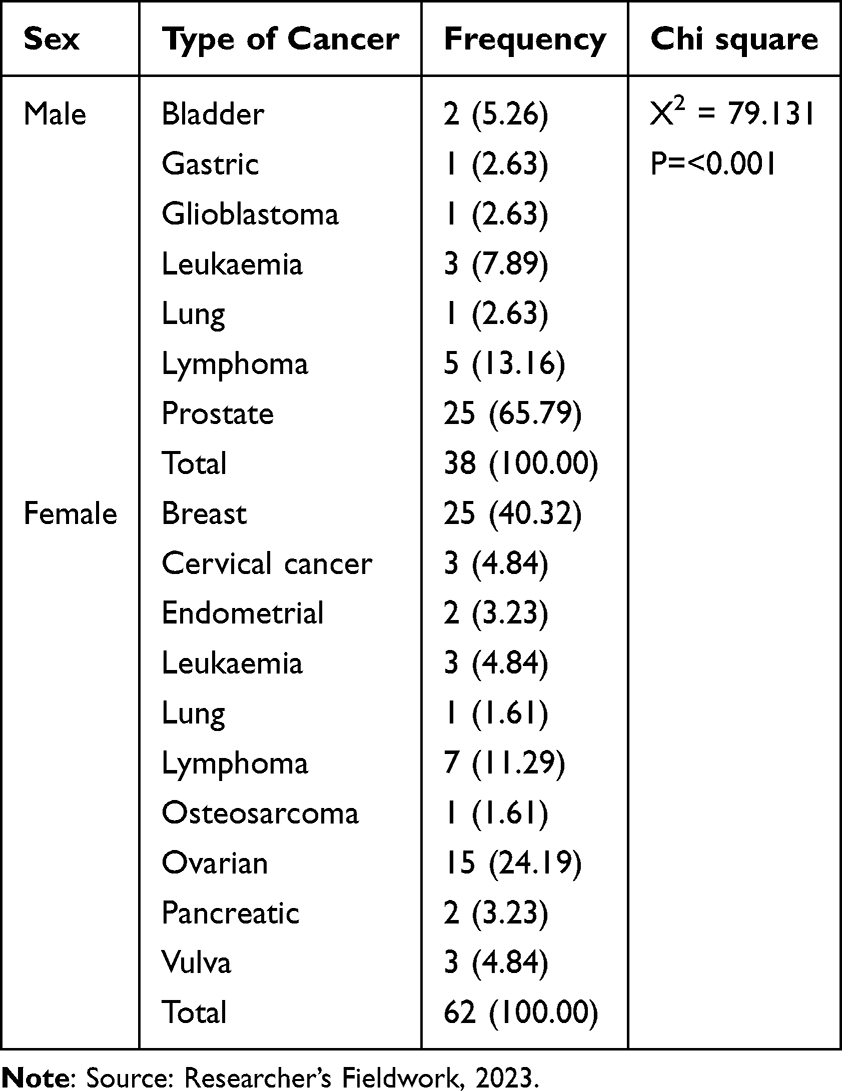 |
Table 4 Association Between Type of Cancer and Sex Distribution |
Blood Count Parameters in the Study Population
Table 5 outlines haematological parameters for the study population, including haemoglobin, white blood cell, and platelet counts. The average haemoglobin level was 11.13 g/dL (SD = 5.74), ranging from 3.80 to 27.20 g/dL, showing considerable variation. The mean white blood cell count was 11.05 x 10^9/L (SD = 21.75), with a broad range from 1.00 to 129.00 x 10^9/L. Platelet counts averaged 189.51 x 10^9/L (SD = 137.87), ranging from 8.00 to 578.00 x 10^9/L, indicating substantial diversity in blood count parameters among participants.
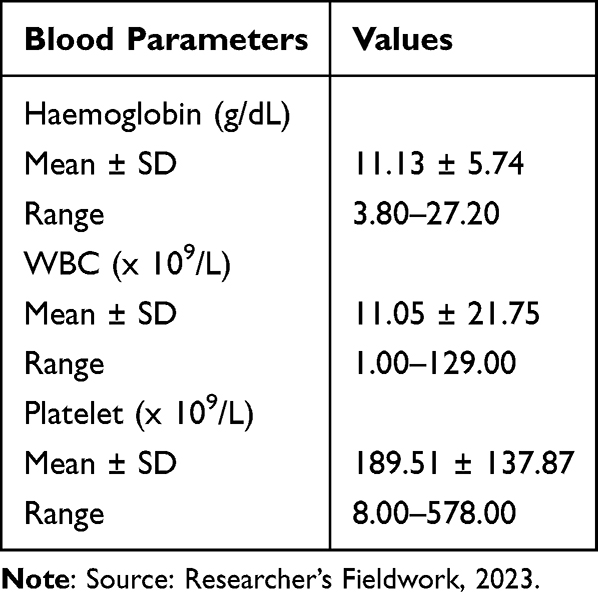 |
Table 5 Blood Count Parameters in the Study Population |
Body Mass Index
Table 6 indicates that the majority of the study population (54%) had a BMI within the “Normal weight” range. An additional 38% were classified as “Overweight”, while a smaller proportion (8%) fell into the “Obesity” category, reflecting a predominantly normal to slightly elevated BMI distribution within the sample.
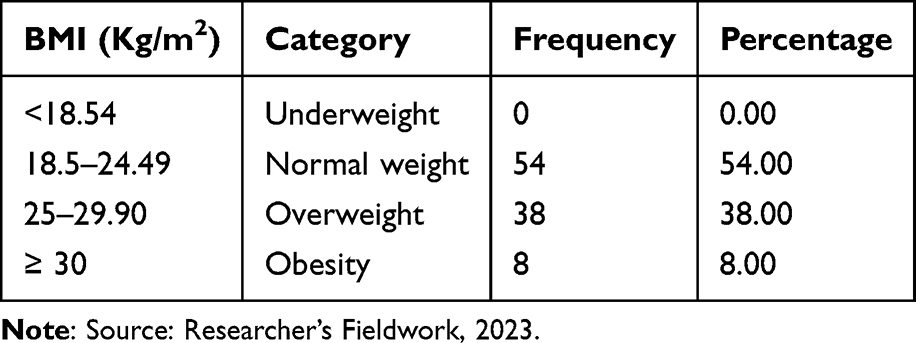 |
Table 6 Body Mass Index |
P-Selectin Levels (Ng/Ml)
The average P-selectin level among study participants was 23.54 ng/mL (SD = 13.29), with a median of 23.00 ng/mL. The interquartile range (IQR) for P-selectin was 13.00 to 23.00 ng/mL. Presented in Table 7 and Table 8 respectively.
 |
Table 7 P-Selectin Levels in Study Subjects |
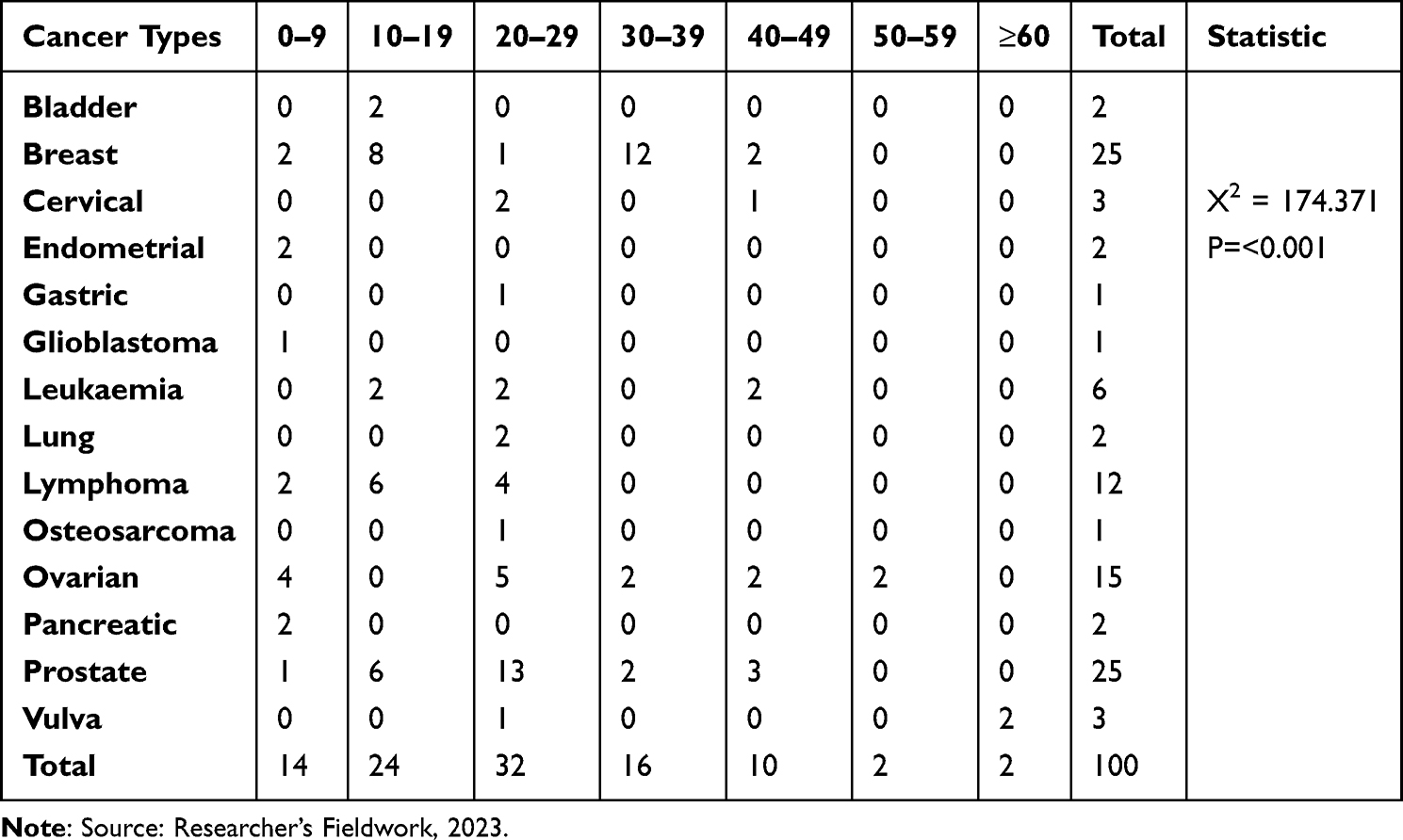 |
Table 8 Association Between Cancer Types and P-Selectin |
Khorana Scoring System
In the study, VTE risk scores varied, with the majority (41%) of individuals scoring 1.0, indicating a moderate VTE risk. Another 32% had a score of 2.0, also suggesting moderate risk. Higher risk scores included 3.0 (15% of participants) and 4.0 (5%), associated with elevated VTE risk. Seven individuals had a 0.0 score (7%), representing the lowest risk. The average Khorana risk score was 1.84 (SD = 0.95), with an interquartile range of 1.00 to 2.00, covering moderate risk levels. The findings are presented in Table 9
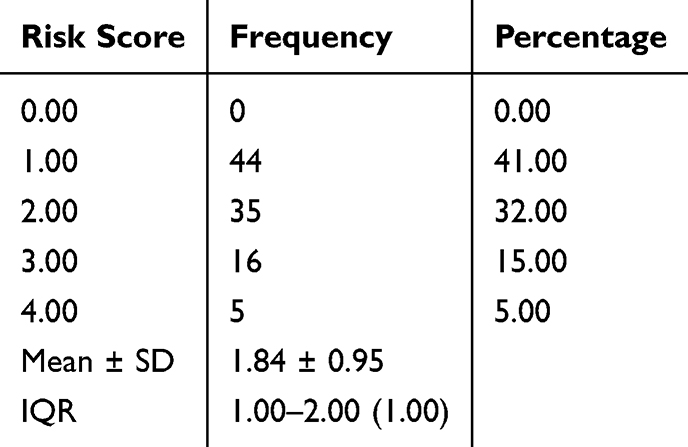 |
Table 9 Khorana Scoring System |
VTE Risk Assessment
Table 10 reveals that most of the study population (79%) were classified as “Intermediate Risk” for Venous Thromboembolism (VTE), indicating a moderate risk level. A smaller group, representing 21% of participants, fell into the “High Risk” category, suggesting a heightened susceptibility to VTE in this subset.
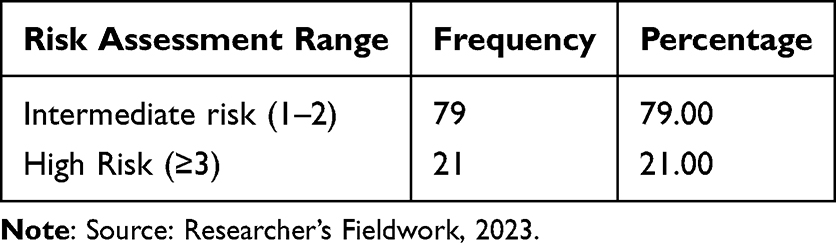 |
Table 10 VTE Risk Assessment |
Association Between VTE Risk and Sex
Table 11 provides a comprehensive analysis of the association between VTE (Venous Thromboembolism) risk assessment and sex within the study population. The independent sample t-test was conducted to assess the association between VTE risk assessments and sex. No observable statistical difference was seen in the association between VTE risk and the sex of the patients (t= −0.717, p=0.475).
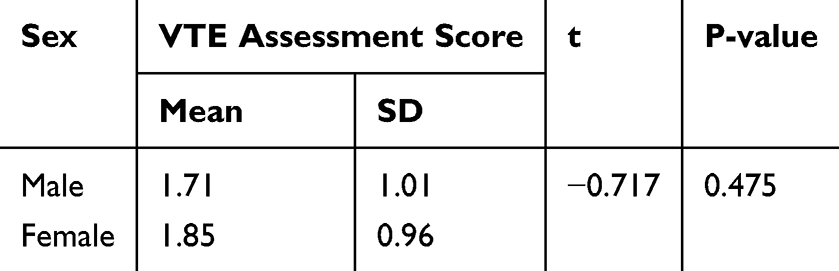 |
Table 11 Association Between VTE Risk and Sex |
Correlation Between P-Selectin and VTE Risk
Correlation between P-selectin and KRS showed a weak negative association (r =−0.08) and the p-value indicates insignificance (p=0.404) as shown in Figure 3.
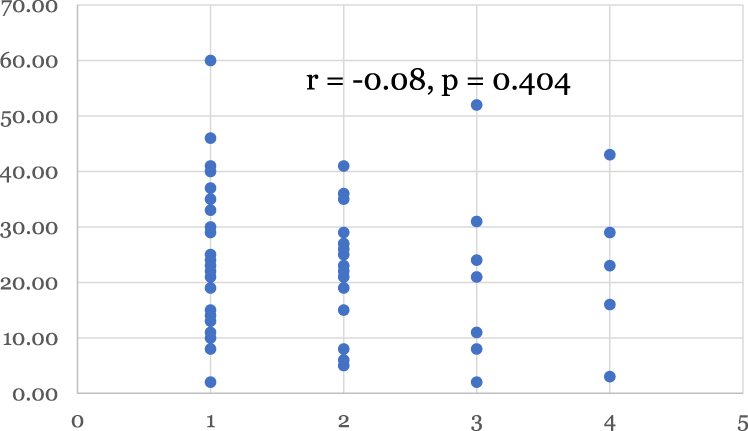 |
Figure 3 Correlation between P-selectin and KRS. |
Discussion
Cancer is a hypercoagulable and prothrombotic disease associated with significant alterations in the haemostatic system. In this study, subjects with cancer were predominantly middle-aged females, with a peak age range of 40–59 years. Most were married, had tertiary education, and had a duration of illness of approximately two years. This demographic trend may be attributed to the health-seeking behaviours of married women and their educational backgrounds. Additionally, a significant portion of our subjects were gynaecological cancer patients, a finding also reported by Omosun et al in Lagos, Southwest Nigeria.12
In our study, breast and ovarian cancers were the predominant cancers among females, while prostate cancer was most prevalent among males. This aligns with the findings of Agba et al in North Central Nigeria,13 who reported a higher prevalence of 66.4% of breast and prostate cancers among females and males, respectively. A similar trend was noted in a study by Uchendu in the South-South region of Nigeria, which found a predominance of breast cancer in females and colorectal cancer in males.14 In contrast, Omosun et al found a predominance of cervical cancer in the Southwest of Nigeria. These discrepancies may be attributed to variations in study design.12
Our study demonstrated that surgery was the most common treatment option, followed by radiation and chemotherapy, with anticoagulant use recorded at 4%. This finding is consistent with the work of Cai et al, who investigated thromboprophylaxis for inpatients with advanced cancer in a palliative care setting.15 Additionally, Mahan et al reported a thromboprophylaxis rate of 3.9% among medically ill patients, which mirrors our findings.16
The haematological parameters varied significantly in our study; haemoglobin levels ranged from severe anaemia to polycythaemia, while white blood cell counts varied from severe leukopenia to marked leucocytosis. Platelet counts also exhibited a range from severe thrombocytopenia to moderate thrombocytosis. These variations can be attributed to the effects of chemotherapy and the different stages of cancer, as well as the potential impact of systemic inflammation related to cancer.17,18
Our findings indicate that most subjects had a normal BMI, with few classified as overweight and even fewer as obese. This is in line with the findings of Fadelu et al, who also reported normal BMI in a study of body mass index, chemotherapy-related weight changes, and disease-free survival in Haitian women. This similarity may be due to the predominance of breast cancer among our subjects and the chronicity of the diseases.19 In contrast, Pati’s study indicated an association between obesity and breast, endometrial, and pancreatic cancers.20
The soluble P-selectin levels in our subjects were found to be within the median interquartile range. Soluble P-selectin, which is released by activated platelets, is associated with thrombosis risk. This finding aligns with Ayc et al,21 who noted no change in soluble P-selectin levels in newly diagnosed cancer patients, though these levels were associated with venous thromboembolism risk. Similarly, Castellon et al reported normal P-selectin levels in non-small cell lung cancer patients,22 while Setiawan et al found no change in soluble P-selectin values among cancer patients undergoing chemotherapy.23 Comparable findings were also reported by Haznedaroglu et al and Blann et al.24,25
Those with breast and prostate cancer exhibited the highest levels of soluble P-selectin, followed by lung cancer patients. This finding is consistent with research by Cihan Ay et al21, which showed that high plasma levels of soluble P-selectin are predictive of venous thromboembolism in cancer patients. Additionally, Omunakwe identified higher levels of P-selectin among prostate cancer patients.26
In our study, the Khorana risk score (KRS) for most subjects ranged from 1 to 2 (73%), indicating intermediate risk, while approximately 20% were classified as high risk. This suggests that the risk of a thrombotic event within six months is approximately 6.6% for the intermediate-risk group and 11% for the high-risk group, as reported by Mulder et al.27 Similar findings were noted by Nishimura in a literature review on predicting venous thromboembolism using the Khorana score.28 Furthermore, a study conducted by Overvad et al29 in Denmark indicated that cancer patients with a high KRS have a heightened six-month risk of both arterial thrombosis and other thromboembolic events.
Our study also revealed a significant association between KRS and cancer types, which contrasts with the findings of a meta-analysis by Nick Van et al that noted an association of the risk score predominantly with pancreatic cancer.30 This discrepancy may result from our study being cross-sectional with a broader range of cancers compared to the smaller sample sizes typically used in retrospective studies.
Nevertheless, our findings are similar to those of Keziah et al31 in a retrospective cohort study of venous thromboembolism rates in ambulatory cancer patients, as well as Ayane Oba Aonuma’s research on cancer-associated thromboembolism incidence in Japanese populations.32 Ellen Marcus also reported a strong association between the Khorana score and venous thromboembolism among ovarian cancer patients.33
Lastly, the correlation between P-selectin and the Khorana risk score showed a weak negative association (r = −0.08) with a p-value indicating insignificance (p = 0.404). This implies no statistically significant association between P-selectin values and the KRS, consistent with the findings of Ay Chan et al.21
Conclusion
This study has shown that the risk of VTE among cancer patients ranges from intermediate to high, going by the modified Khorana risk score irrespective of the P selectin level. There is little adherence to Khorana score in our setting, hence the need for greater application and knowledge of this predictive score in clinical practice to improve outcome and quality of life. Furthermore, there is underutilization of thromboprophylaxis among cancer patients and mainly patients at high risk of VTE.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
No conflict of interest.
References
1. Bray F, Ferlay J, Soerjomatara I, Siegel RL, Torre LA, Jemal A. Global cancer statistics:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Vorobiof DA, Abratt RP. The cancer burden in Africa. S Afr Med J. 2007;1–3.
3. Ebughe GA, Ugbem TI, Ushie DE, Effewongbe S. Cancer in Cross River State. J Adv Med Med Res. 2019;1–8. doi:10.9734/jammr/2019/v30i130163
4. Diaz ES, Walts AE, Karlan BY, Walsh CS. Venous thromboembolism during primary treatment of ovarian clear cell carcinoma is associated with decreased survival. Gynecol Oncol. 2013;131(3):541–545. doi:10.1016/j.ygyno.2013.09.005
5. Enrik H, Oft T, Sorensen S, et al. Prognosis of cancers associated with venous thromboembolism. New Engl J Med. 2000;343(25):1946.
6. Matsuura Y, Robertson G, Marsden DE, Kim SN, Gebski V, Hacker NF. Thromboembolic complications in patients with clear cell carcinoma of the ovary. Gynecol Oncol. 2007;104(2):406–410. doi:10.1016/j.ygyno.2006.08.026
7. Rodriguez AO, Wun T, Chew H, Zhou H, Harvey D, White RH. Venous thromboembolism in ovarian cancer. Gynecol Oncol. 2007;105(3):784–790. doi:10.1016/j.ygyno.2007.02.024
8. Sandhu R, Pan CX, Wun T, et al. The incidence of venous thromboembolism and its effect on survival among patients with primary bladder cancer. Cancer. 2010;116(11):2596–2603. doi:10.1002/cncr.25004
9. Ohashi Y, Ikeda M, Kunitoh H, et al. Venous thromboembolism in patients with cancer: design and rationale of a multicentre, prospective registry (Cancer-VTE Registry). BMJ Open. 2018;8(5):e018910. doi:10.1136/bmjopen-2017-018910
10. Cohen AT, Katholing A, Rietbrock S, Bamber L, Martinez C. Epidemiology of first and recurrent venous thromboembolism in patients with active cancer: a population-based cohort study. Thromb and Haemost. 2017;117(1):57–65. doi:10.1160/TH15-08-0686
11. Purdy M, Obi A, Myers D, Wakefield T. P- and E- selectin in venous thrombosis and non-venous pathologies. J Thromb Haemost. 2022;20(5):1056–1066. doi:10.1111/jth.15689
12. Omosun A, Abayomi A, Ogboye O, et al. Distribution of cancer and cancer screening and treatment services in Lagos: a 10-year review of hospital records. JCO Global Oncol. 2022;8:e2200107. doi:10.1200/GO.22
13. Jedy-Agba E, Curado MP, Ogunbiyi O, et al. Cancer incidence in Nigeria: a report from population-based cancer registries. Cancer Epidemiol. 2012;36(5):271–278. doi:10.1016/j.canep.2012.04.007
14. Uchendu OJ. Cancer incidence in Nigeria: a tertiary hospital experience. Asian Pac J Cancer Care. 2019;5(1):27–32. doi:10.31557/apjcc.2020.5.1.27-32
15. Cai R, Zimmermann C, Krzyzanowska M, Granton J, Hannon B. Thromboprophylaxis for inpatients with advanced cancer in palliative care settings: a systematic review and narrative synthesis. Palliative Med. 2019;33(5):486–499. doi:10.1177/0269216319830860
16. Mahan CE, Fisher MD, Mills RM, et al. Thromboprophylaxis patterns, risk factors, and outcomes of care in the medically ill patient population. Thromb Res. 2013;132(5):520–526. doi:10.1016/j.thromres.2013.08.013
17. Aynalem M, Adem N, Wendesson F, et al. Hematological abnormalities before and after initiation of cancer treatment among breast cancer patients attending at the University of Gondar comprehensive specialized hospital cancer treatment center. PLoS One. 2022;17(8 August):e0271895. doi:10.1371/journal.pone.0271895
18. Shilpa MD, Kalyani R, Sreeramulu PN. Prognostic value of pre-treatment routine hematological parameters in breast carcinoma: advantageous or deleterious? Biomed Res Ther. 2021;7(8):3916–3920. doi:10.15419/bmrat.v7i8.621
19. Fadelu T, Damuse R, Lormil J, et al. Body mass index, chemotherapy related weight changes and disease free survival in Haitian women with nonmetastatic breast cancer. JCO Global Oncol. 2020;6:1656–1665. doi:10.1200/GO.20.00307
20. Pati S, Irfan W, Jameel A, Ahmed S, Shahid RK. Obesity and cancer: a current overview of epidemiology, pathogenesis, outcomes, and management. Cancers. 2023;15(2):485. doi:10.3390/cancers15020485
21. Ay C, Simane R, Vormittag R, et al. High plasma levels of soluble P-selectin are predictive of venous thromboembolism in cancer patients: results from the Vienna Cancer and Thrombosis Study (CATS). Blood. 2018;112(7):2703–2708. doi:10.1182/blood-2008-02-142422
22. Castellón Rubio VE, Segura PP, Muñoz A, Farré AL, Ruiz LC, Lorente JA. High plasma levels of soluble P-selectin and factor VIII predict venous thromboembolism in non-small cell lung cancer patients: the Thrombo-NSCLC risk score. Thromb Res. 2020;196:349–354. doi:10.1016/j.thromres.2020.09.021
23. Setiawan B, Permatadewi CO, de Samakto B, et al. Von Willebrand factor: antigen and ADAMTS-13 level, but not soluble P-selectin, are risk factors for the first asymptomatic deep vein thrombosis in cancer patients undergoing chemotherapy. Thromb J. 2020;18(1). doi:10.1186/s12959-020-00247-6
24. Haznedaroğlu IC, Dündar SV, Ozcebe O, et al. Serum L-selectin and P-selectin levels in lymphomas. Haematologia. 2000;30(1):27–30. doi:10.1163/15685590051129841
25. Blann AD, Dunmore S. Arterial and venous thrombosis in cancer patients. Cardiol Res Pract. 2011;1(1). doi:10.4061/2011/394740
26. Omunakwe HN, Ekeke OC, Obiorah C. P-selectin as a marker of platelet activation in Africans with prostate cancer: a cross-sectional study. IOSR J Dental Med Sci. 2016;15(09):67–70. doi:10.9790/0853-1509036770
27. Mulder FI, Candeloro M, Kamphuisen PW, et al. The khorana score for prediction of venous thromboembolism in cancer patients: a systematic review and meta-analysis. Haematologica. 2019;104(6):1277–1287. doi:10.3324/haematol.2018.209114
28. Nishimura A, Ikeda Y. Predicting the incidence of venous thromboembolism using the Khorana score: a literature review. Yakugaku Zasshi. 2021;141(4):611–622. doi:10.1248/yakushi.20-00228
29. Overvad TF, Ording AG, Nielsen PB, et al. Validation of the Khorana score for predicting venous thromboembolism in 40 218 patients with cancer initiating chemotherapy. Blood Advances. 2022;6(10):2967–2976. doi:10.1182/bloodadvances.2021006484
30. Nick V, Ventresca M, Di Nisio M, et al. The Khorana score for prediction of venous thromboembolism in cancer patients: an individual patient data meta-analysis. Journal of Thrombosis and Haemostasis. 2020;18(8):1940–1951. doi:10.1111/jth.14824
31. Keziah A, George J, Robinson EJ, Scully M, Thomas MR. Retrospective cohort study of venous thromboembolism rates in ambulatory cancer patients: association With Khorana score and other risk factors. Journal of Hematology. 2019;8(1):17–25. doi:10.14740/jh471
32. Aonuma AO, Nakamura M, Sakamaki K, et al. Incidence of cancer-associated thromboembolism in Japanese gastric and colorectal cancer patients receiving chemotherapy: a single-institutional retrospective cohort analysis (Sapporo CAT study). BMJ Open. 2019;9(8):e028563. doi:10.1136/bmjopen-2018-028563
33. Marcus E, Kuo DY-S, Nevadunsky NS, Gressel GM. Association of the Khorana score with development of venous thromboembolism in ovarian cancer. Journal of Clinical Oncology. 2021;39(15_suppl):5555. doi:10.1200/JCO.2021.39.15_suppl.5555
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.